Clinical History: A 41-year-old right-handed man presents with 3 years of radial-sided right wrist pain. The patient does not recall a specific injury, but he began having severe wrist pain while training for the marines. He was initially treated conservatively with rest, which resulted in improved symptoms. The symptoms were subsequently aggravated while working out with kettlebells and performing pull ups. The patient also reports symptoms of clicking/clunking and decreased grip strength. Axial (1a), coronal (1b), and sagittal (1c) fat-suppressed T1 VIBE images are provided from an MR arthrogram after radiocarpal injection. What are your findings? What is the diagnosis?

1a

1b

1c
Figure 1
Findings

2a

2b

2c
Figure 2:
Axial and coronal images (2a and 2b) show tearing involving the volar, membranous, and dorsal components of the scapholunate interosseous ligament (arrows). The axial image (2a) also demonstrates additional tearing of the dorsal intercarpal ligament with mild widening of the scapholunate interosseous space. The sagittal image (2c) shows tearing of the dorsal capsulo-scapholunate septum (DCSS) with dorsal tilting of the lunate (arrowhead).
Diagnosis
Grade 4 scapholunate instability with dorsal intercalated segmental instability (DISI).
Introduction
Scapholunate dissociation is the most common form of wrist instability, defined as “the loss of synchronous motion or normal alignment between the scaphoid and the lunate”.1 The mechanism of injury is typically a fall with the wrist extended and in ulnar deviation. Reported symptoms include swelling, dorsal tenderness, decreased grip strength, and reduced range of motion.2 The initial diagnosis can be challenging due to a number of factors. Foremost, isolated scapholunate interosseous (SLI) ligament injury is often missed due to normal alignment on initial radiographs. In addition, with severe trauma, other injuries such as fractures of the distal radius or scaphoid can cause diagnostic difficulty. Furthermore, patients often do not seek immediate treatment and may present in the subacute or chronic phase after the symptoms become aggravated by strenuous work or repetitive activities.2 With delayed presentation, derangement is more likely to be evident on imaging due to progressive destabilization of the wrist. Patients who are underdiagnosed, misdiagnosed, or untreated may suffer from chronic wrist dysfunction, which can result in lost time at work and interference with everyday activities.3
Please refer to Table 1 below for a full list of abbreviations used throughout this article.
| Table 1 – Abbreviations | |
| Term | Term |
| DCSS | Dorsal capsulo-scapholunate septum |
| DIC ligament | Dorsal intercarpal ligament |
| DISI | Dorsal intercalated segmental instability |
| DRC ligament | Dorsal radiocarpal ligament |
| EWAS | European Wrist Arthroscopy Society |
| LR ligament | Long radiolunate ligament |
| LTI ligament | Lunotriquetral interosseous ligament |
| PARC | Proximal avulsion of the radiocarpal capsule |
| RL angle | Radiolunate angle |
| RSC ligament | Radioscaphocapitate ligament |
| SL angle | Scapholunate angle |
| SLAC | Scapholunate advanced collapse |
| SLI ligament | Scapholunate interosseous ligament |
| STT ligament | Scaphotrapeziotrapezoid ligament |
Scapholunate Stabilization
A scapholunate stabilizer can be defined as any structure that helps prevent abnormal motion or abnormal alignment between the scaphoid and lunate bones. Scapholunate stabilizers are characterized as primary or secondary. The SLI ligament serves as the sole primary stabilizer. Secondary scapholunate stabilization is a complicated and debated subject, with contributions from muscles and tendons, volar and dorsal intrinsic and extrinsic ligaments, and a structure that has recently received a great deal of attention, the dorsal capsulo-scapholunate septum (DCSS).
The SLI ligament is an intrinsic wrist ligament. Intrinsic wrists ligament are defined as originating and inserting within the carpus, whereas extrinsic ligaments are defined as connecting the forearm with the carpus.2 Although typically referred to as one unit, the SLI ligament is actually composed of dorsal and volar ligaments that connect the scaphoid and lunate bones, joined by a central fibrocartilaginous membrane proximally (figure 4). The dorsal ligament is widely regarded as the strongest and most important component of the SLI ligament with a tensile strength of 260 newtons, compared to a tensile strength of 118 newtons for the volar ligament, and 63 newtons for the central membrane.4 Injury involving the entirety of the SLI ligament results in dynamic changes of the wrist and, therefore represents a critical step that may lead to progressive carpal instability.2 However, multiple studies have demonstrated that no static malalignment occurs between or among the carpal bones after isolated injury to the SLI ligament and that at least one secondary stabilizer must also be injured before there is imaging-detectable widening of the scapholunate interosseous space.5,6

3a
Figure 3:
3D graphic representation of the scapholunate interosseous ligament with the scaphoid removed demonstrates the dorsal ligament (red), central fibrocartilage membrane (yellow), and volar ligament (blue).

4a
Figure 4:
The mechanism of injury for tearing of the SLI ligament is a fall onto an outstretched hand with the wrist extended and in ulnar deviation. With the scaphoid closely tethered to the distal carpal row via intrinsic ligaments (red ligaments) and the lunate tethered to the radius via extrinsic ligaments (blue ligaments), progressive torque is placed on the SLI ligament (top images) resulting in tearing progressing from the volar SLI ligament (bottom left), to the central fibrocartilage membrane (bottom middle), and finally to the dorsal SLI ligament (bottom right).
Muscles and tendons are an important line of defense as secondary stabilizers when it comes to secondary stabilization of the scaphoid and lunate. Mechanoreceptors within wrist ligaments deliver proprioceptive information to the sensorimotor system, which ideally results in a protective muscle response. In general, muscles that prevent scaphoid flexion are considered protective, such as the extensor carpi radialis longus and abductor pollicis longus muscles.2
Volar wrist ligaments contributing to secondary scapholunate stability include two extrinsic ligaments and one intrinsic ligament: the radioscaphocapitate (RSC) ligament (extrinsic), the long radiolunate (LR) ligament (extrinsic), and the scaphotrapeziotrapezoid (STT) ligament (intrinsic) (figure 5). Short et al. sequentially sectioned the SLI, STT, and RSC ligaments in cadaveric wrists. After sectioning the STT ligament, ulnar deviation of the scaphoid and extension of the lunate increased, which was not observed when only the SLI ligament was sectioned.7
In addition, there was a significant increase in scaphoid flexion after sectioning all three ligaments, suggesting that the STT and RSC ligaments are important contributors to scaphoid stability.7 Linscheid also showed that there must be injuries to the SLI and RSC ligaments before scaphoid subluxation or widening of the scapholunate interosseous space occurs.6 Pérez et al. demonstrated increased lunate extension when the STT or LR ligament, in addition to the SLI ligament, was sectioned.1 Overstraeten et al. identified a significant association between the severity of SLI ligament injuries and LR ligament injuries.8 These findings confirm the importance of the integrity of these volar ligaments in providing stability to the scaphoid and lunate.

5a
Figure 5:
3D graphic representation of the volar ligaments of the wrist highlights the long radiolunate (LR), radioscaphocapitate (RSC), and the scaphotrapeziotrapezoid (STT) ligaments, which contribute to secondary scapholunate stability.
There are two important ligaments at the dorsal aspect of the wrist that together form a lateral “V” shaped structure: the intrinsic dorsal intercarpal (DIC) ligament and the extrinsic dorsal radiocarpal (DRC) ligament (figure 6). Recent investigations have mainly focused on the secondary role that the DIC ligament plays in scapholunate stability. The DIC ligament originates from the dorsal aspect of triquetrum with attachments to the lunate, scaphoid, capitate, trapezium, and trapezoid.9 The DIC ligament is the only dorsal ligament crossing the midcarpal joint and has a mechanical strength greater than that of the SLI ligament.2,9 Mitsuyasu et al. demonstrated a significant change in scaphoid and lunate alignment after sectioning the dorsal wrist capsule, the SLI ligament, and the DIC ligament.10 Blatt came to a similar conclusion, finding that both the SLI ligament and DIC ligament need to be disrupted before rotary subluxation of the scaphoid and widening of the scapholunate interosseous space occur.5 Based on these studies, it is clear that the DIC ligament is a critical secondary stabilizer of the scaphoid and lunate.

6a

6b
Figure 6:
3D graphic representation (6a) highlights the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments, which contribute to secondary scapholunate stability. A cadaveric image (6b) demonstrates the DIC and DRC ligaments (arrows).
There has been a recent addition to the list of secondary scapholunate stabilizers: the DCSS (figure 7). In a cadaveric study of 90 wrists, Viegas observed communicating fibers between the DIC ligament and the SLI ligament in 100% of the cadaveric specimens.9 Binder et al. documented a similar finding in 15 cadaveric wrists and suggested naming this structure the dorsal capsulo-scapholunate septum (DCSS).11 The DCSS is best described as a confluence of tissue between the DIC ligament, the dorsal radiocarpal capsule, and the dorsal aspect of the SLI ligament with mean dimensions of 5.8 mm in height and 4.0 mm in width.12 The DCSS is best imaged in the sagittal plane and can be seen coursing distally and dorsally from the SLI and DIC ligaments to attach to the radiocarpal capsule (figures 7a and 7b). Studies have emphasized the importance of the DCSS in providing stability to the scaphoid and lunate, both directly and indirectly. Elsaidi demonstrated that sectioning of the SLI ligament did not result in increased scaphoid flexion if the DCSS was intact.13 Multiple studies have demonstrated dorsal capsulodesis prevents rotary subluxation of the scaphoid.5,14,15 At least two studies have suggested that an injury to the DCSS increases arthroscopic grading of scapholunate instability.8,16Binder showed that isolated injuries at the attachment of DIC ligament to the DCSS can lead to instability, even with an intact SLI ligament.11 Bonte et al. described a similar but distinct injury called a “proximal avulsion of the radiocarpal capsule” (PARC) lesion, which can be a cause of posttraumatic wrist pain.17

7a

7b

7c

7d
Figure 7:
Sagittally oriented cadaveric section (7a) of the wrist demonstrates an intact DCSS (arrow). Oblique sagittal 3D graphic representation (7b) of the DCSS demonstrating its relationship to the SLI, DIC, and DRC ligaments. Additional coronal 3D graphic representations (7c and 7d) with the capsule removed and with retraction of the DIC demonstrating an intact DCSS.
It is clear that scapholunate stability is a complicated topic. New discoveries will undoubtedly be made, such as the recent finding that a type II lunate with two distal facets is associated with a lower incidence of malalignment after injury to the SLI ligament.3 More investigational studies are needed to clarify each contribution.
Scapholunate Alignment and Radiographic Assessment
Measurement of carpal angles and distances on static films is challenging due to variability amongst readers. Anatomic landmarks and well-defined standards are essential to provide reproducible results. Three measurements relating to the alignment of and relationship between the scaphoid and lunate have been described and widely accepted.
The first measurement relates to analysis of the distance between the scaphoid and lunate. Normal articulating carpal bones have parallel apposing bone surfaces separated by 2 mm or less.2 A gap between the scaphoid and lunate greater than 3mm on conventional radiographs is considered abnormal by most sources with reported “abnormal” values ranging from 2-4mm.18 In these reports, the method of measurement has varied. Some sources suggest measuring the smallest interval between the scaphoid and lunate bones.18 Others recommend measuring the scapholunate interosseous space at the midpoint between Gilula’s lines (the proximal and distal outlines of the proximal carpal row).1 Regardless of the method that is used, there will be some inherent inaccuracy as these radiographic criteria assume cartilage thickness between bones is the same across all patients. Measuring the gap between the scaphoid and lunate on MRI rather than conventional radiography is likely more accurate because the space between the cartilage can be measured and injury to the SLI ligament and secondary stabilizers of the wrist can be directly assessed.
The second measurement relating to scapholunate alignment is the scapholunate angle, described as the angle between: 1) A tangent connecting the proximal and distal volar convexities of the scaphoid bone; and 2) A perpendicular to a tangent connecting the palmar and dorsal tips of the lunate.11 The normal scapholunate angle ranges from 45–60°.2 When the scaphoid is destabilized, it has a natural tendency to flex, termed rotatory subluxation. In comparison, the lunate has a natural tendency to rotate into extension, thus increasing the scapholunate angle.
The third important measurement is the radiolunate angle, which is the angle between: 1) The long axis of the radius and 2) A perpendicular to a tangent connecting the volar and dorsal tips of the lunate.11 Again, a destabilized lunate may rotate into extension, thereby increasing the radiolunate angle, with a measurement of greater than 15° considered abnormal. An increased radiolunate angle combined with an increased scapholunate angle is termed dorsal intercalated segmental instability (DISI).

8a

8b
Figure 8:
Lateral 3D renderings of the wrist. Figure 8a shows the normal range of scapholunate (SL) and radiolunate (RL) angles. Figure 8b shows DISI, where the scaphoid rotates into flexion and the lunate rotates into extension, thus increasing the scapholunate and radiolunate angles.
Two other radiographic signs can be seen with scapholunate malalignment: the ring sign and the palmar “V” sign. As visualized in conventional PA radiographs of the wrist, when the scaphoid abnormally flexes and becomes foreshortened, the scaphoid tuberosity projects as a ring over the distal scaphoid, termed the ring sign. The palmar “V” sign is used to describe the resulting acute angle between the scaphoid and radius observed in a lateral radiograph when the scaphoid abnormally flexes.2
Patterns of Instability and Staging
Scapholunate instability, as mentioned previously, is the most common type of carpal instability. Watson et al. classified scapholunate instability into four different types: predynamic, dynamic, static and scapholunate advanced collapse (SLAC).10 Scapholunate instability was then further characterized into five stages by Kitay et al. The five stages of scapholunate instability are occult, dynamic, scapholunate dissociation, DISI, and SLAC.3
Stage 1: Predynamic, or occult, scapholunate instability is defined as attenuation or a tear of a portion of the SLI ligament: the volar SLI ligament or the central fibrocartilaginous membrane. This often results from a fall on an outstretched hand, and patients can present with localized wrist pain and dysfunction with mechanical loading. Both static and stress radiographs are often normal, making the initial diagnosis of predynamic instability difficult.3,10

9a

9b
Figure 9:
Stage 1 - Predynamic scapholunate instability. Fat-suppressed proton density-weighted axial (9a) and coronal (9b) images show attenuation of the volar SLI ligament (arrow) with an intact central fibrocartilaginous membrane, intact dorsal SLI ligament, and a normal scapholunate interosseous space.
Stage 2: Dynamic scapholunate instability is defined as a partial or complete tear of the SLI ligament, which includes involvement of the dorsal SLI ligament. In Stage 2 with a complete SLI ligament tear, the lunotriquetral interosseous (LTI) ligament and lunate attachment of the DIC ligament remain intact. Therefore, static radiographs often demonstrate a normal width of the scapholunate interosseous space and a normal scapholunate angle.3 Due to the ligamentous injuries; however, there are abnormal kinetics with loading, resulting in abnormal findings on stress radiographs and motion studies. The anteroposterior grip, carpal stress, and posteroanterior clenched pencil radiographic projections are most commonly used to evaluate for dynamic scapholunate instability. It is the clenched pencil view that is considered the most useful stress view, as it allows for comparison with the other wrist.3 Patients with dynamic instability of the wrist present with catching, popping, and pain. Additionally, patients will have a positive Watson test, which manifests as pain when pressure is applied to the scaphoid tubercle as the wrist is passively deviated from an ulnar to radial position. The pressure applied to the scaphoid tubercle prevents the scaphoid from flexing; however, if the SLI ligament is torn, the proximal scaphoid subluxes dorsally.11

10a

10b

10c
Figure 10:
Stage 2 - Dynamic scapholunate instability. Fat-suppressed T2-weighted axial image (10a) demonstrates a partial tear of the volar SLI ligament (arrow) and attenuation of and altered signal in the dorsal SLI ligament (arrowhead) and altered signal in the scaphoid. Fat-suppressed proton density-weighted coronal image (10b) and T2-weighted sagittal image (10c) demonstrate a normal scapholunate interosseous space and normal alignment of the lunate with the capitate and radius.
Stage 3: Scapholunate dissociation is defined as the loss of the normal alignment and movement between the scaphoid and lunate. Scapholunate dissociation infers an injury to the SLI ligament and a deficiency of at least one of the secondary stabilizing ligaments. On radiographs, findings that are suspicious for scapholunate dissociation are widening of the scapholunate interosseous space greater than 2-4 mm, the scaphoid ring sign, an increased scapholunate angle that is greater than 60 degrees, and the palmar V sign, as described previously.2 Scapholunate misalignment on both static and stressed radiographs is defined as static scapholunate instability.
Mitsuyasu found that in the setting of a completely torn SLI ligament and a deficient scaphoid attachment of the DIC ligament, there is rotary subluxation of the scaphoid but only in the loaded position. Once both attachments of the DIC ligament to the scaphoid and to the lunate were deficient, in the setting of a complete tear of the SLI ligament, findings included a flexed position of the scaphoid and a widened scapholunate interosseous space on both static and stressed radiographs. This finding was also supported by the results of an investigation by Özkan et al., in which a partial tear of the DIC ligament and/or DRC ligament was required before static scapholunate dissociation over 2 mm was observed.18 Basically, deficiency in a secondary stabilizing ligament in addition to the SLI ligament is what allows progression from Stage 2 dynamic scapholunate instability to Stage 3 scapholunate dissociation.

11a

11b

11c
Figure 11:
Stage 3 - Scapholunate dissociation. Post-contrast T1-weighted fat-suppressed axial arthrogram image (11a) shows a tear of the volar SLI ligament (arrow), a tear of the dorsal SLI ligament (arrowhead), and attenuation of the DIC ligament (asterisk). Coronal (11b) and sagittal (11c) post-contrast T1-weighted fat-suppressed VIBE arthrogram images show widening of the scapholunate interosseous space (star) and an intact DCSS (arrow).
Stage 4: DISI is characterized by rotary subluxation of the scaphoid and an extended position with dorsal tilting of the lunate with the radiolunate angle exceeding 15 degrees.1 As described previously, there are multiple important secondary stabilizers of the scaphoid and lunate including the DIC ligament, dorsal radiotriquetral (DRT) ligament, STT ligament, RSC ligament and LR ligament. Several studies have investigated the roles of these stabilizing ligaments with respect to the development of DISI.
Perez, Short, and their collaborators found that a deficiency of the LR ligament, in addition to a complete tear of the SLI ligament, was not sufficient to produce a DISI deformity.1,7 Additionally Mitsuyasu et al. found that a complete tear of the SLI ligament plus a deficiency of the scaphoid attachment of the DIC ligament resulted in an increase in lunate extension but did not result in a DISI deformity.10 A study by Elsaidi et al. found that there was no significant difference in lunate extension before and after sectioning of the volar extrinsic ligaments in the setting of a complete tear of the SLI ligament.1 A deficiency in the volar extrinsic ligaments in combination with a deficiency of the DIC ligament in the setting of a complete SLI ligament tear; however, did result in a DISI deformity.
A DISI deformity was also seen after a complete SLI ligament tear plus a deficient DIC ligament at both the scaphoid and lunate attachments.1,10 Mitsuyasu hypothesized that that the DIC ligament attachment to the lunate helps stabilize the dorsal aspect of the lunate with respect to the triquetrum; and, further, once the DIC ligament attachment to the lunate is deficient, there will be enough rotational torque on the lunate from the volar LTI ligament such that a DISI deformity will develop.10 Perez et al. also found that a DISI deformity was encountered in the following scenarios: a complete SLI ligament tear and a deficient STT ligament; 2) a complete SLI ligament tear and a deficient lunate attachment of the DIC ligament, with or without a deficient LR ligament.
These studies show the importance of the scaphoid and lunate attachments of the DIC ligament as well as the importance of critical stabilizing ligaments in the development of DISI. It is this combination of injuries to the dorsal and volar extrinsic ligaments and/or the deficiency of certain critical intrinsic ligaments, in addition to a complete tear of the SLI ligament, that allows progression of Stage 3 scapholunate dissociation to a Stage 4 DISI.

12a

12b

12c
Figure 12:
Stage 4 - DISI. Fat-suppressed T2-weighted axial image (12a) shows complete tears of the volar SLI ligament, central fibrocartilaginous membrane, dorsal SLI ligament, and scaphoid attachment of the DIC ligament (arrow). Fat-suppressed T2-weighted coronal image (12b) shows a widened scapholunate interosseous space (asterisk). T2-weighted sagittal image (12c) shows a torn DRC ligament (arrow) and dorsal tilting of the lunate.

13a

13b

13c
Figure 13:
Stage 4 - DISI (continued). Post-contrast fat-suppressed T1-weighted arthrogram axial (13a) and coronal (13b) images show a complete tear of the SLI ligament and widening of the scapholunate interosseous space. Post-contrast fat-suppressed T1-weighted sagittal VIBE arthrogram image (13c) shows an intact but thickened DCSS, suggesting prior injury (arrow).
Stage 5: Over time the deficiency of the secondary stabilizing ligaments in addition to a complete SLI ligament tear leads to proximal translation of the capitate and distal carpal row with resultant degenerative changes. This stage is designated SLAC and has been further classified into three main types. Degenerative changes at the most radial aspect of the distal radioscaphoid joint are categorized as SLAC I. SLAC II indicates degenerative changes that involve the entire radioscaphoid joint. SLAC III occurs when degenerative changes are seen in the radial aspect of the midcarpal joint. A type IV SLAC has also been described, defined as degenerative changes at the radiolunate aspect of the radiocarpal joint and the entire carpus.3

14a

14b
Figure 14:
Stage 5 - SLAC wrist. T1-weighted coronal (14a) and sagittal (14b) images show a widened scapholunate interosseous space, proximal migration of the capitate, narrowing of the radioscaphoid joint (arrow), and dorsal tilting of the lunate with degenerative changes.
An arthroscopic classification of scapholunate instability has also been described by Geissler who grades scapholunate instability by the appearance of the SLI ligament and of midcarpal alignment visualized from the radiocarpal portal.3,18,19 Grade 1 is characterized by attenuation of the SLI ligament without midcarpal malalignment. Grade 2 is characterized by a slight gap between the scaphoid and lunate with carpal malalignment and attenuation of the SLI ligament. In grade 3, there is incongruence of carpal alignment with a large scapholunate interosseous gap. Grade 4 is defined as incongruence of carpal alignment and gross instability with at least a 2.7 mm gap between the scaphoid and lunate, an arthroscopic observation that is termed the drive-through sign.(3) Lee et al. reported that Grade 4 injuries were not seen unless the DIC ligament was also torn.18,20
This arthroscopic classification of scapholunate instability was further modified and is designated the Messina-EWAS classification.(11,17) In this modified arthroscopic classification, scapholunate instability was assessed from the midcarpal radial portal rather than from the radiocarpal portal. Stage I was defined as no scapholunate incongruency. Stage II was described as a partial tear involving the membranous SLI ligament without associated scapholunate widening. Stage III was further divided into stage IIIA (a lesion involving the volar SLI ligament), stage IIIB (a lesion involving the dorsal SLI ligament with a partial lesion of the DIC ligament), and stage IIIC (a complete tear of the SLI ligament with widening of the scapholunate space, which manifests during stress maneuvers, and a lesion of either the DIC or the RSC/LR ligaments). In stage IV there is a complete tear of the SLI ligament with associated widening of the scapholunate space allowing passage of a probe from the midcarpal to the radiocarpal space. Stage IV was also associated with a tear of the DIC ligament and the RSC/LR ligaments. Lastly, in Stage V the scapholunate interosseous space is widened with a complete tear of the SLIL, DIC, and RSC/LR ligaments and involvement of additional ligaments such as the triquetral-hamate, STT, and DRC ligaments.(11,17)
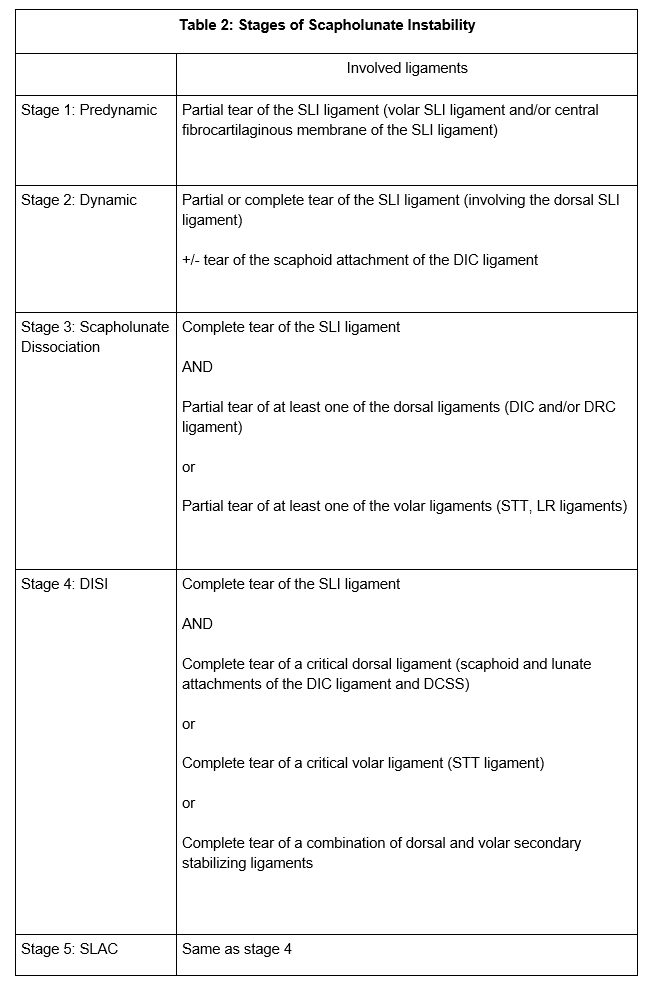
It is clear from this review that the observations reported in many of the publications dealing with the stages of scapholunate instability are not uniform, and that there is considerable variability in the reported ligaments whose injury characterizes each stage in the process. Table 2 provides a summary of the major conclusions provided by the results of these studies. With further research, the sites of ligament injury that accompany these stages will likely be modified, but all of these data underscore the importance of assessment of more than the SLI ligament when viewing MRI studies of scapholunate instability. This assessment must include analysis of many of the intrinsic and dorsal and volar extrinsic ligaments of the wrist. The results of this analysis will influence the choice of a specific therapeutic strategy.
Treatment
The various stages of scapholunate dissociation serve as key factors influencing management and treatment. In the setting of occult instability, the treatment is conservative with casting, medication (NSAIDs), physical therapy, and sometimes arthroscopic debridement. Thermal shrinkage has also been used in the setting of an attenuated SLI ligament. Treatment for Stage 2 dynamic instability and Stage 3 scapholunate dissociation is directed at the sagittal and coronal plane alignment abnormalities. Sagittal plane abnormalities are related to the abnormal rotation of the scaphoid and are best addressed with dorsal capsulodesis. The coronal plane injury is related to tearing of the SLI ligament and is best addressed with repair or reconstruction of the ligament. In the setting of a non-repairable SLI ligament, a bone-ligament-bone graft, ligamentoplasty, scapholunate pseudoarthrosis and/or intercarpal fusion have been performed.(2,3) In subacute or chronic cases of SLI ligament injury, scapholunate fixation using K-wires or screws has been used.
In the setting of Stage 4 DISI, the goal of surgery is for symptomatic relief and prevention of progression to a SLAC wrist. Procedures are tailored to restore carpal alignment and stabilize the scaphoid, which is achieved primarily through intercarpal arthrodesis including scaphotrapezial-trapezoid arthrodesis and arthrodesis of the scaphoid, capitate and lunate. The downside of this latter procedure is the reduced range of motion in the dart thrower’s plane, which is important for activities of daily living. Once there is development of a SLAC wrist, the procedures are mostly salvage-type, which include a 4-corner arthrodesis and proximal row carpectomy. Once extensive degenerative changes have developed, the surgical options include a total wrist arthrodesis, total wrist arthroplasty, or a wrist hemiarthroplasty. The latter procedure is reserved for younger persons with higher activity demands.(2,3)
Conclusion
It is clear that scapholunate instability is a complicated subject. Based on prior investigations, it is evident that in addition to SLI ligament injury, there must also be injury to at least one other secondary stabilizer before static malalignment occurs. The secondary stabilizers include numerous intrinsic and extrinsic ligaments of the wrist, the DCSS, and the surrounding muscles and tendons. More investigation is required to fully understand each structure’s contribution to scapholunate stability as well as instability. Early and accurate imaging staging leads to optimal treatment, thus improving symptoms and long-term outcomes.

References
- Pérez AJ, Jethanandani RG, Vutescu ES, Meyers KN, Lee SK, Wolfe SW. Role of Ligament Stabilizers of the Proximal Carpal Row in Preventing Dorsal Intercalated Segment Instability: A Cadaveric Study. J Bone Joint Surg Am. 2019 Aug 7;101(15):1388-1396. doi: 10.2106/JBJS.18.01419. ↩
- Hayton, M., Ng, C. Y., Funk, L., Watts, A., & Walton, M. (2019). Sports injuries of the hand and wrist. Cham, Switzerland: Springer. ↩
- Kitay A, Wolfe SW. Scapholunate instability: current concepts in diagnosis and management. J Hand Surg Am. 2012 Oct;37(10):2175-96. doi: 10.1016/j.jhsa.2012.07.035. ↩
- Berger RA. The ligaments of the wrist. A current overview of anatomy with considerations of their potential functions. Hand Clin. 1997 Feb;13(1):63-82. Review. ↩
- Blatt G. Capsulodesis in reconstructive hand surgery. Dorsal capsulodesis for the unstable scaphoid and volar capsulodesis following excision of the distal ulna. Hand Clin. 1987 Feb;3(1):81-102. ↩
- Linscheid RL, Dobyns JH, Beabout JW, Bryan RS. Traumatic instability of the wrist: diagnosis, classification, and pathomechanics. J Bone Joint Surg Am. 2002 Jan;84(1):142. ↩
- Short WH, Werner FW, Green JK, Masaoka S. Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate. J Hand Surg Am. 2002 Nov;27(6):991-1002. ↩
- Overstraeten LV, Camus EJ, Wahegaonkar A, Messina J, Tandara AA, Binder AC, Mathoulin CL. Anatomical Description of the Dorsal Capsulo-Scapholunate Septum (DCSS)-Arthroscopic Staging of Scapholunate Instability after DCSS Sectioning. J Wrist Surg. 2013 May;2(2):149-54. doi: 10.1055/s-0033-1338256. ↩
- Viegas SF, Yamaguchi S, Boyd NL, Patterson RM. The dorsal ligaments of the wrist: anatomy, mechanical properties, and function. J Hand Surg Am. 1999 May;24(3):456-68. ↩
- Mitsuyasu H, Patterson RM, Shah MA, Buford WL, Iwamoto Y, Viegas SF. The role of the dorsal intercarpal ligament in dynamic and static scapholunate instability. J Hand Surg Am. 2004 Mar;29(2):279-88. ↩
- Binder AC, Kerfant N, Wahegaonkar AL, Tandara AA, Mathoulin CL. Dorsal wrist capsular tears in association with scapholunate instability: results of an arthroscopic dorsal capsuloplasty. J Wrist Surg. 2013 May;2(2):160-7. ↩
- Tommasini Carrara de Sambuy M, Burgess TM, Cambon-Binder A, Mathoulin CL. The Anatomy of the Dorsal Capsulo-Scapholunate Septum: A Cadaveric Study. J Wrist Surg. 2017 Aug;6(3):244-247. ↩
- Elsaidi GA, Ruch DS, Kuzma GR, Smith BP. Dorsal wrist ligament insertions stabilize the scapholunate interval: cadaver study. Clin Orthop Relat Res. 2004 Aug;(425):152-7. ↩
- Lavernia CJ, Cohen MS, Taleisnik J. Treatment of scapholunate dissociation by ligamentous repair and capsulodesis. J Hand Surg Am. 1992 Mar;17(2):354-9. ↩
- Wintman BI, Gelberman RH, Katz JN. Dynamic scapholunate instability: results of operative treatment with dorsal capsulodesis. J Hand Surg Am. 1995 Nov;20(6):971-9. ↩
- Ruch DS, Poehling GG.Wrist Arthroscopy: Ligamentous Instability. In: Green DP, Hotchkiss RN, Pederson WC, eds. Green’s Operative Hand Surgery. 4th ed. Philadelphia: Churchill Livingstone; 1999:200–206. ↩
- Bonte F, Mathoulin CL. The PARC Lesion: A Proximal Avulsion of the Radiocarpal Capsule. J Wrist Surg. 2017 Feb;6(1):80-86. doi: 10.1055/s-0036-1584162. Epub 2016 May 25. Erratum in: J Wrist Surg. 2017 Aug;6(3):258-260. ↩
- Özkan S, Kheterpal A, Palmer WE, Chen NC. Dorsal Extrinsic Ligament Injury and Static Scapholunate Diastasis on Magnetic Resonance Imaging Scans. J Hand Surg Am. 2019 Aug;44(8):641-648. doi: 10.1016/j.jhsa.2019.03.003. Epub 2019 Apr 29. ↩
- Geissler WB, Freeland AE, Savoie FH, McIntyre LW, Whipple TL. Intracarpal Soft-Tissue Lesions Associated with an Intra-articular Fracture of the Distal End of the Radius. J Bone Joint Surg Am. 1996;78(3):357-365. ↩
- Lee SK, Model Z, Desai H, Hsu P, Paksima N, Dhaliwal G. Association of Lesions of the Scapholunate Interval With Arthroscopic Grading of Scapholunate Instability via the Geissler Classification. J Hand Surg Am. 2015;40(6):1083-1087. ↩
