Clinical History
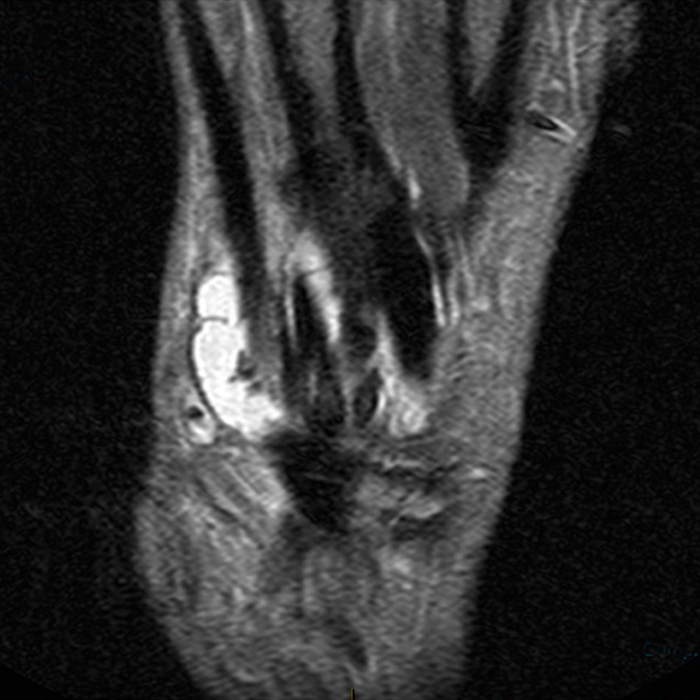
An 80-year-old male presents with a growing mass at the dorsal right wrist for 1 month. Coronal (1A and 1B), axial (1C), and sagittal (1D) STIR images of the wrist are provided, as well as a lateral radiograph (1E). What are the findings? What is your diagnosis?




Findings

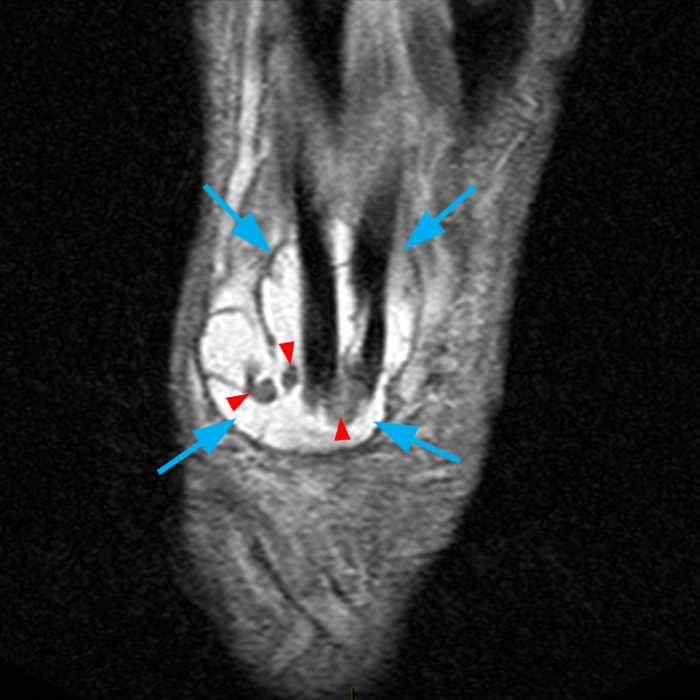
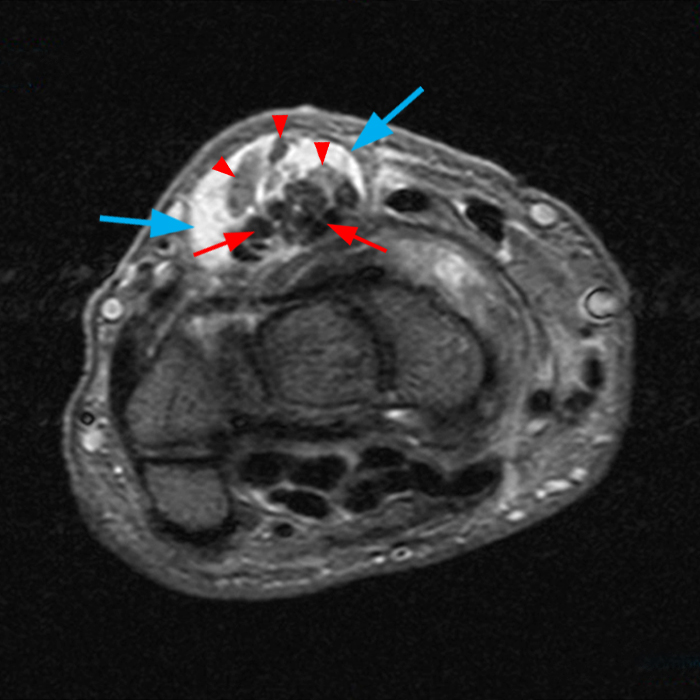
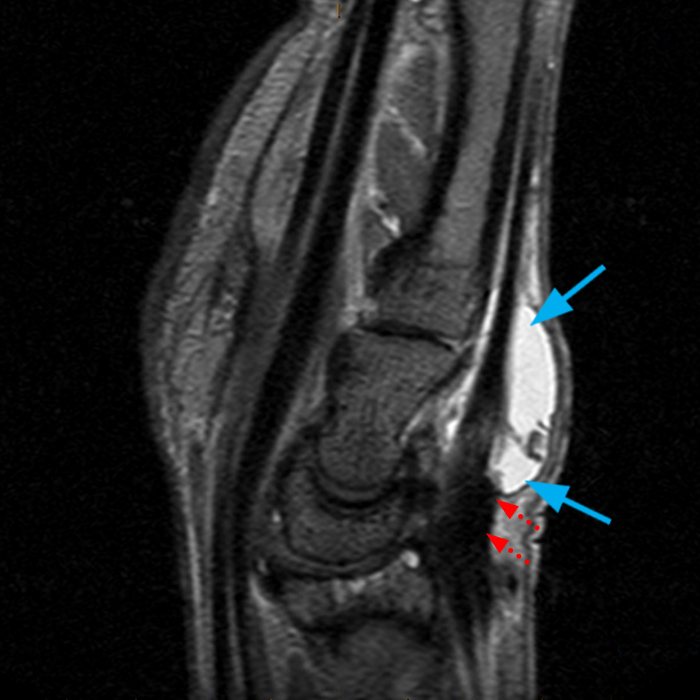

Coronal (2A and 2B), axial (2C) and sagittal (2D) images demonstrate extensive tenosynovitis localized to the 4th dorsal extensor compartment (blue arrows) just distal to the extensor retinaculum (dotted arrows), with fluid and areas of prominent synovial thickening (arrowheads). Tendinosis of the extensor digitorum communis tendons is noted (2C, red arrows). The lateral radiograph demonstrates localized mass-like swelling at the dorsal wrist.
Diagnosis
Stenosing tenosynovitis of the 4th extensor compartment.
Introduction
Extensor tendon tenosynovitis is a significant cause of wrist pain and morbidity, often associated with inflammatory processes or overuse syndromes. While relatively uncommon, isolated tenosynovitis of the fourth dorsal extensor compartment can occur, typically in the setting of rheumatoid arthritis or following trauma, but occasionally due to impingement by the overlying extensor retinaculum causing stenosing tenosynovitis. This latter condition, akin to De Quervain tenosynovitis of the first extensor compartment, is under-recognized by both radiologists and clinicians.
Anatomy
The extensor tendons of the wrist are organized into six compartments, which house the tendons responsible for extending the fingers. The extensor retinaculum (ER) is an important structure overlying the extensor tendons at the radial, dorsal, and ulnar aspects of the wrist. It holds the extensor tendons in place and prevents bowstringing.1 The ER is a fibrous fascial thickening that arises from the antebrachial fascia of the forearm proximally, is continuous volarly with the volar carpal ligament, and distally it tapers becoming indistinguishable from the loose fascia over the metacarpals, which is part of the superficial fascia of the dorsal hand.2,3 At the level of the radiocarpal joint, the ER courses obliquely across the dorsal aspect of the carpal bones. The ER has fascial attachments to the underlying bones and periosteum, thereby forming the 6 distinct fibro-osseous compartments for the extensor tendons of the wrist. (Figure 3)
The fourth extensor compartment is the largest and contains the extensor digitorum communis (EDC) tendons and the extensor indicis proprius (EIP) tendon. The tendons pass deep to the ER within their tendon sheath, and after emerging from the fibro-osseous tunnel of the fourth compartment, diverge toward the index through small fingers. (Figure 4A)
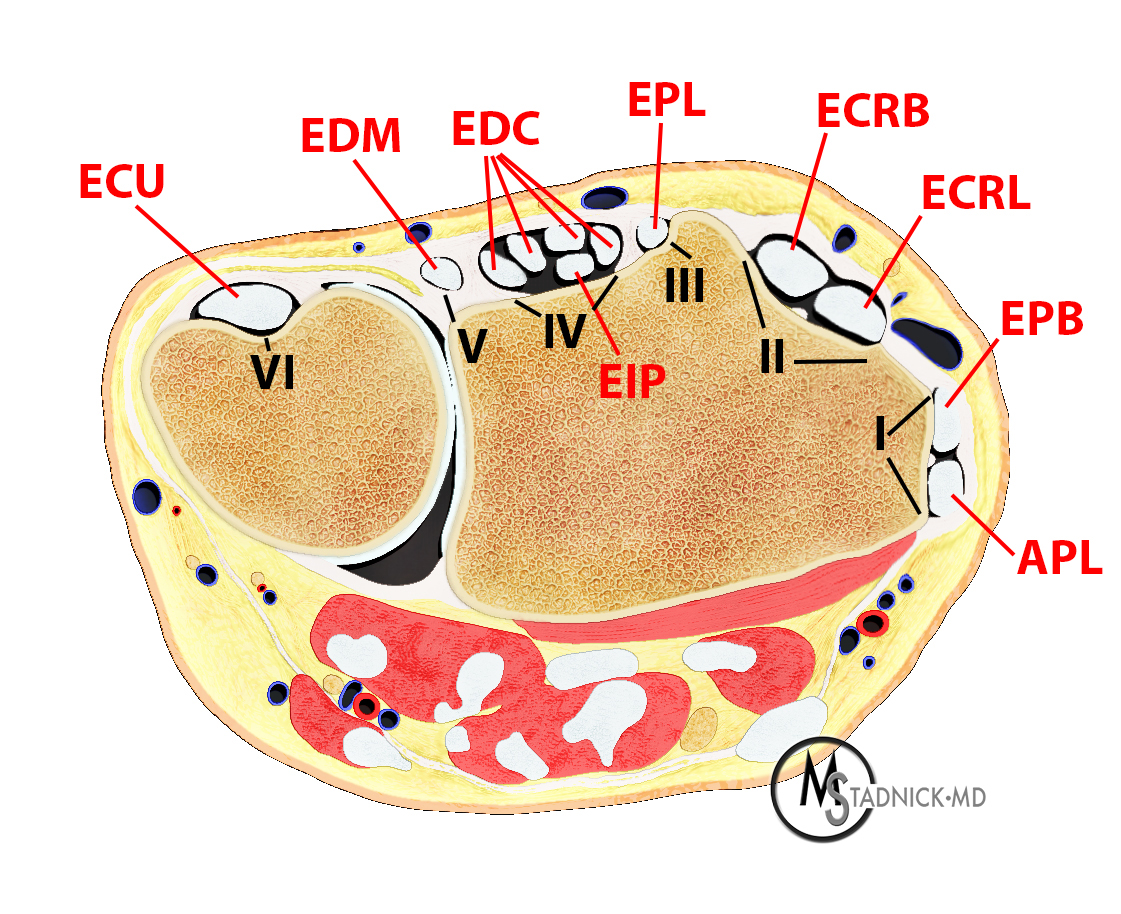
Figure 3: Axial render demonstrates the contents of the extensor compartments. Extensor compartment I contains the extensor pollicis brevis (EPB) and abductor pollicis longus (APL) tendon. Compartment II contains the extensor carpi radialis longus (ECRL) and brevis (ECRB) tendons. Compartment III contains the extensor pollicis longus (EPL) tendon. Compartment IV contains the extensor digitorum communis (EDC) tendons to the index - small finger and the extensor indicis proprius (EIP) tendon. Compartment V contains the extensor digiti minimi (EDM) tendon. Compartment VI contains the extensor carpi ulnaris (ECU) tendon.
Pathophysiology
In general, tenosynovitis arises from synovial proliferation and fluid production surrounding a tendon due to inflammatory, infectious, or post-traumatic factors. Stenosing tenosynovitis is a condition characterized by restricted gliding of a tendon through its fibro-osseous tunnel, and occurs when a size discrepancy exists between the tendon and the pulley or sheath through which the tendon passes.4 Inflammation of the tendon sheath results in fibrosis, which narrows the tendon canal and impedes the smooth gliding motion, leading to pain, catching, and restricted finger movement.5 This condition is often referred to as trigger finger and most commonly affects the flexor tendons at the A1 pulley. Stenosing tenosynovitis can also affect the 1st dorsal extensor compartment, referred to as De Quervain’s Tenosynovitis.
While relatively uncommon, stenosing tenosynovitis can affect the 4th extensor compartment. Overuse and chronic microtrauma may lead to localized thickening of the ER which impinges upon the extensor tendons, similar to findings seen in De Quervain’s tenosynovitis or trigger finger.6 Activities that require repetitive dorsiflexion of the wrist can contribute to overuse-type syndrome. VanHeest7 and Wilson8 have described cases of ER impingement on the EDC tendons in athletes who perform repetitive motions, including wrist hyperextension, such as in gymnasts, weight-lifters, platform divers, and shot put (track and field). The rigid distal border of the ER impinges on the gliding of the EDC or EIP tendons, causing thickening of the ER, adjacent tenosynovial thickening and tenosynovitis, and potential tendinosis and fraying of the underlying tendons (Figure 4B). Superimposed inflammatory conditions such as rheumatoid arthritis, seronegative spondyloarthropathies, or systemic disorders like diabetes mellitus may also contribute to tenosynovitis and cause tendon adhesions or thickening.
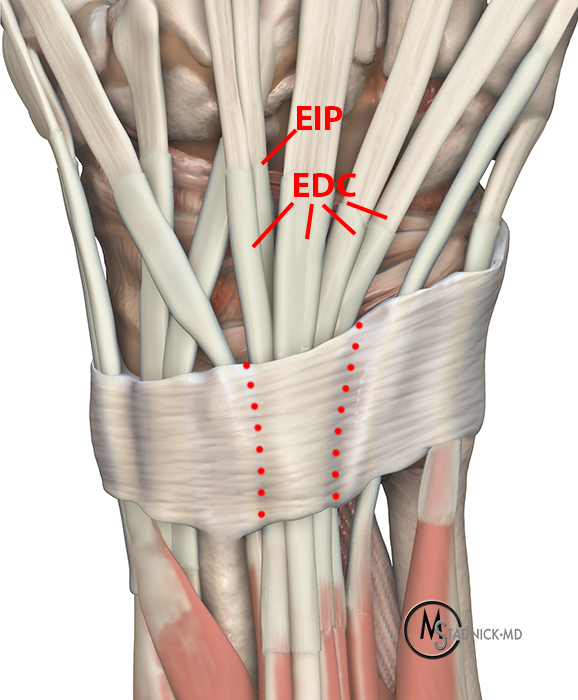
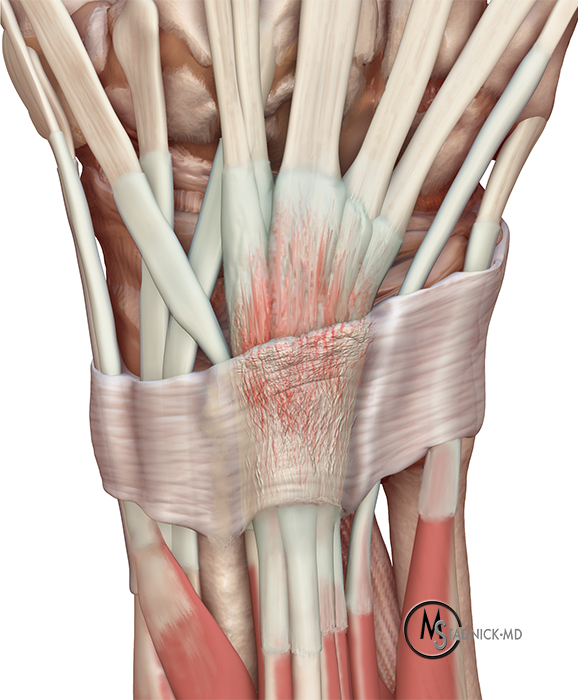
Figure 4: The 4th dorsal compartment contains the extensor digitorum communis (EDC) tendons and the extensor indicis proprius (EIP) (4A). A thickened distal extensor retinaculum at the fourth extensor compartment can impinge the EDC and EIP tendons and cause tenosynovitis and underlying fraying of the tendons (4B).
Clinical Presentation
Patients with stenosing tenosynovitis of the 4th extensor compartment present with dorsal wrist pain and swelling, typically of several weeks or months in duration7, which is worse with extension and exacerbated by load-bearing activities. Patients may complain of a mass or cyst dorsally (Figures 5, 6). Clinical examination demonstrates pain near the distal margin of the ER, with visible and palpable swelling overlying the extensor tendons just distal to the ER, and triggering with extension. Provocative testing reveals reproducible pain with resistance to finger and wrist extension.
Imaging and Diagnosis
MRI findings include isolated tenosynovitis of the 4th extensor compartment, most severe distal to the ER which may appear thickened (Figures 7-9). Underlying tendinosis, fraying, and/or partial tearing of the EDC and/or EIP tendons may be observed (Figures 10-14). Ultrasound demonstrates proliferative thickening of the EDC tendon sheath with fluid, hypoechoic thickening of the EDC tendons, hypoechoic thickening of the ER, and a dynamic impingement between the tendon and the ER.3,6 Anomalous muscles (Figure 15), intratendinous cysts (Figure 16), or surgical hardware at the distal radius (Figure 17) can contribute to the degree of impingement.1,6


Figure 5: 20-year-old female evaluated for a possible dorsal cyst. Coronal proton density-weighted fat-suppressed (A) and sagittal T2-weighted (B) images demonstrate moderate tenosynovitis of the 4th extensor compartment (arrows), which is most prominent just beyond the ER (dotted arrows)
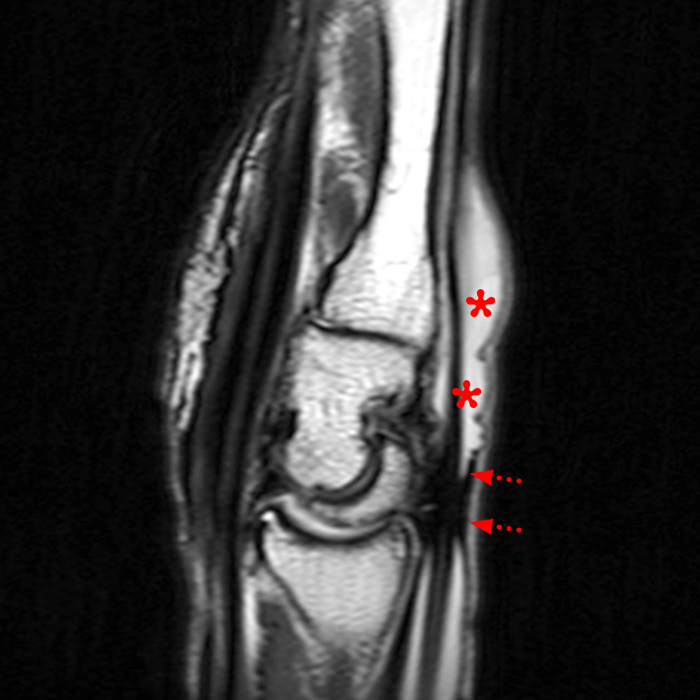

Figure 6: 77-year-old female with wrist “mass” for two months. Sagittal T2-weighted (A) and axial proton density-weighted fat-suppressed (B) images demonstrate extensive tenosynovitis of the 4th compartment which accounted for the mass, most prominent distal to the thickened ER (dotted arrows, A).



Figure 7: 47-year-old male with right wrist pain, swelling and possible tendon injury. Sagittal T2-weighted (A), coronal proton density-weighted fat-suppressed (B), and axial proton density-weighted (C) images demonstrate extensive tenosynovitis of the 4th extensor compartment, with tendinosis and fraying of several of the EDC tendons (arrows, C), synovial hypertrophy/thickening (arrowheads, B), and thickening of the ER (dotted arrows, A).



Figure 8: 44-year-old female with wrist pain. Axial proton density-weighted fat-suppressed (A, B) and T1-weighted (C) images show tenosynovitis within the 4th extensor compartment (arrows A), a very focally thickened ER (dotted arrows B and C), and underlying tendinosis of the EDC tendons (arrowheads). This patient had subsequent surgical release of the ER.



Figure 9: 56-year-old female with Crohn's disease. Axial proton density-weighted fat-suppressed images (A-C) demonstrate 4th extensor compartment tenosynovitis (asterisk A), with tendinosis of the EDC tendons (arrows B) and a thickened and edematous ER (dotted arrows C). 4th compartment tenosynovitis is much more common in rheumatoid arthritis, but occasionally occurs in seronegative spondyloarthropathies.





Figure 10: 63-year-old female with left wrist pain, possible ganglion for 1 year increasing in size, feels like wrist is catching. Coronal proton density-weighted fat-suppressed (A), sagittal T2-weighted (B), and axial proton density-weighted fat-suppressed (C-E) images. Tenosynovitis is present at the 4th extensor compartment (asterisks), distal to a thickened ER (dotted arrows). Underlying tendinosis and fraying of the EDC tendons (arrows) and small intratendinous cyst (arrowhead) are present.




Figure 11: 63-year-old female with right wrist pain. Sagittal T2-weighted (A), coronal proton density-weighted fat-suppressed (B), axial proton density-weighted fat-suppressed (C) and T1-weighted (D) images demonstrate extensive tenosynovitis at the 4th extensor compartment (asterisks), with thickening of the ER (dotted arrows), tendinosis and fraying of the EDC tendons (arrowheads), and synovial thickening.



Figure 12: Middle-aged male with left-sided wrist pain. Axial proton density-weighted fat-suppressed (A) and post-gadolinium-enhanced axial T1-weighted fat-suppressed (B) images demonstrate tenosynovitis at the 4th compartment with diffuse synovial enhancement (B), severe tendinosis and fraying of the EIP tendon (arrows, A and B). Ultrasound images (C) of both wrists shows unilateral tenosynovitis on the left, with fluid surrounding the tendons (arrow C) and relative thickening of the tendons (red asterisks) as compared to the right (blue asterisks).



Figure 13: Chronic wrist pain in a patient with rheumatoid arthritis. Axial proton density-weighted fat-suppressed images (A-C) show tenosynovitis at the 4th compartment, with an intratendinous cyst within the EIP tendon (arrow A) and severe tendinosis and high-grade partial tearing of the EIP tendon (arrowheads B,C). This patient developed spontaneous rupture of the EIP tendon shortly after the MRI.

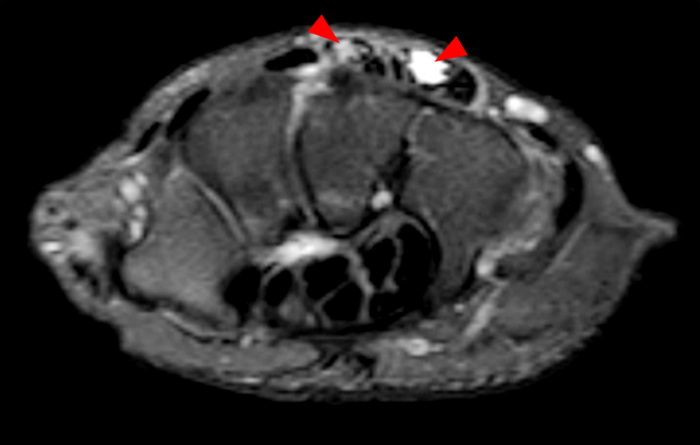



Figure 14: Middle-aged male with typical symptoms of stenosing tenosynovitis. Axial proton density-weighted fat-suppressed (A-C), coronal proton density-weighted fat-suppressed (D) and sagittal T2-weighted (E) images show fluid signal tracking within the EDC tendons (arrowheads). At surgery, there were typical features of tenosynovitis. The surgeon debrided several of the extensor tendons, and histopathology showed “intra-tendinous tenosynovitis”.


Figure 15: 24-year-old male with right hand pain, acute extensor tenosynovitis, with EIP dysfunction. Axial STIR (A) and sagittal proton density-weighted (B) images demonstrate tenosynovitis of the 4th extensor compartment. An accessory muscle (extensor digitorum brevis manus muscle) (asterisk) is noted at the dorsal aspect of the wrist and proximal hand which may be a contributory factor.
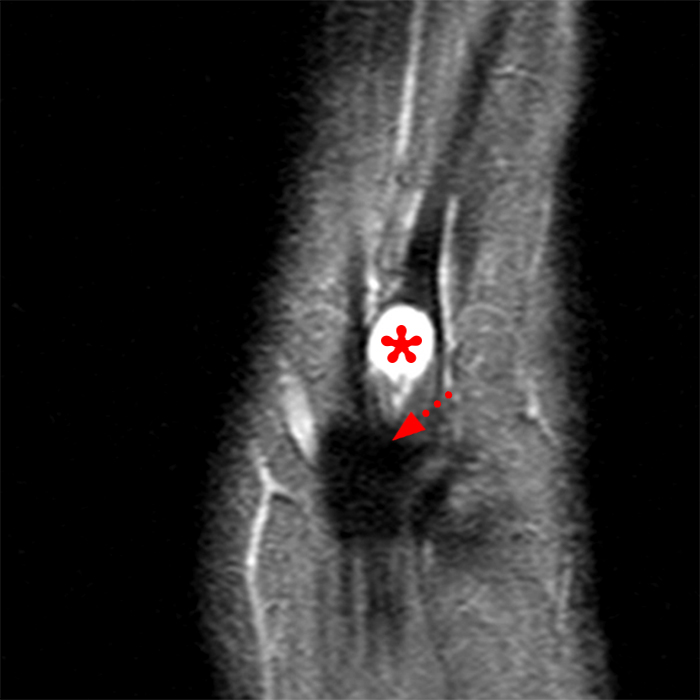



Figure 16: A 51-year-old female with left wrist pain for weeks. Coronal (A), sagittal (B), and axial (C,D) STIR images demonstrate a 7 x 7 x 10 mm intratendinous cyst (asterisks) within the EIP tendon, just distal to the ER (dotted arrows A,B).




Figure 17: 46-year-old female with a distal radius fracture internally fixed with a volar plate and screws. Lateral x-ray (A) demonstrates the screws extending beyond the dorsal cortex of the distal radius (arrow, A) impinging on the 4th extensor compartment. Sagittal T2-weighted (B) and axial proton density-weighted fat-suppressed (C,D) images demonstrate extensive tenosynovitis of the 4th extensor compartment (asterisk) just distal to the radius, with tearing of the extensor tendons (arrowheads). This patient had a rupture of her index and long finger extensor tendons, and was treated surgically by removal of the hardware and primary tendon repairs.
Treatment
Non-operative treatment includes rest, immobilization, ice, and NSAIDs. Corticosteroid injection into the tendon sheath can reduce swelling and improve mobility. Surgical intervention is considered when conservative measures fail.
Upon surgery, pathologic findings include abnormal thickening at the distal border of the ER, thickened synovium, and the underlying tendons can be thickened and frayed near the site of impingement. Surgical procedure includes decompression with partial resection of the ER, tenosynovectomy, and debridement of the tendons as needed, with high success rate7(Figure 18). Histopathologic examination (in patients without RA) reveals a distinct tenosynovitis that resembles traumatic tenosynovitis, with fibrotic changes and little or no synovial hyperplasia or inflammatory reaction.6,9
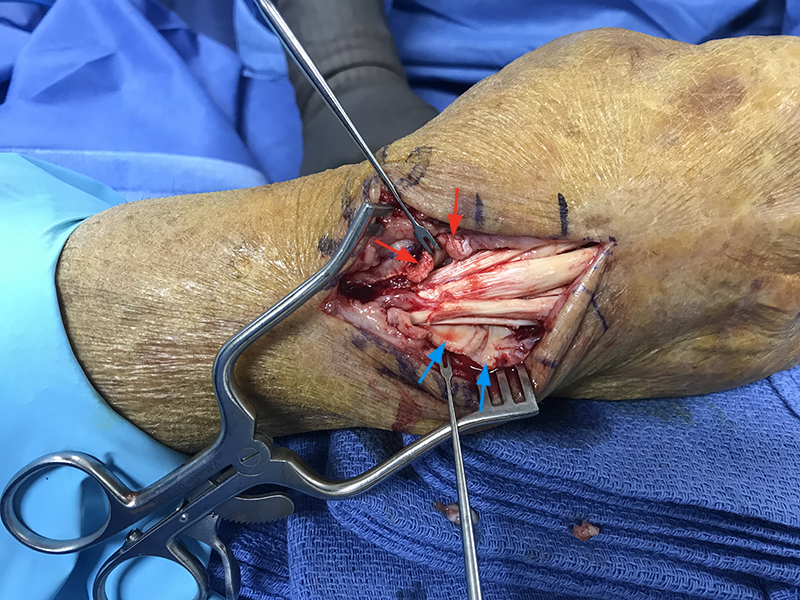
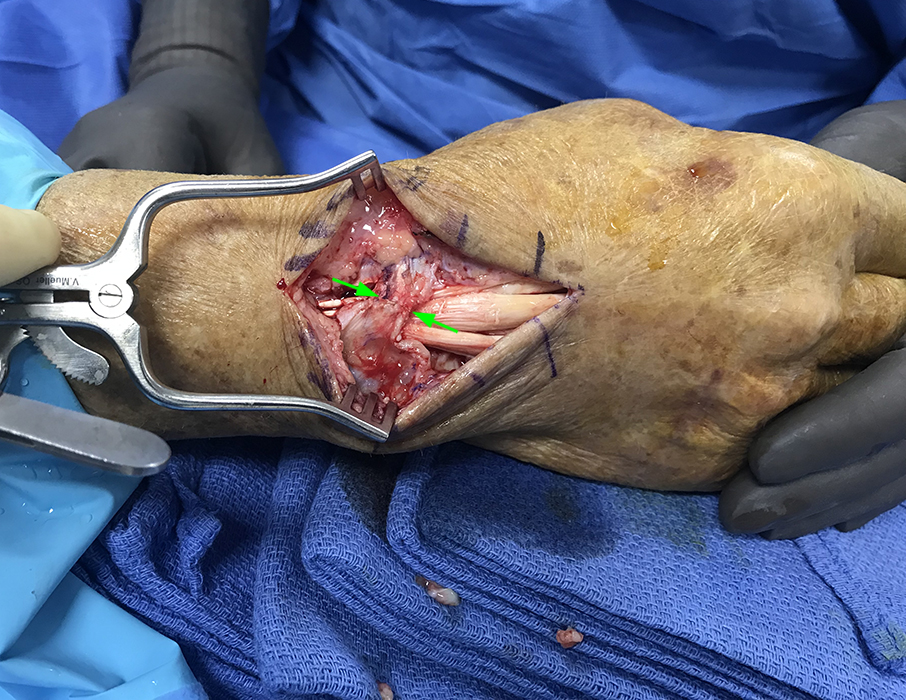
Figure 18: Intraoperative photos for the patient from the test case in Figure 1. (18A) Step cut release of the extensor retinaculum over the 4th extensor compartment with the radial segment of the incised retinaculum (red arrows) held by retractor and the ulnar segment folded ulnarly (blue arrows) revealing the thickened and frayed extensor tendons within the 4th compartment. (18B) After step cut and lengthening repair of the extensor retinaculum shows closure of the extensor retinaculum defect ( green arrows). The clinical, imaging, and operative findings are consistent with 4th extensor compartment stenosing tenosynovitis. (Photographs courtesy of Tom Dovan, MD, Elite Sports Medicine and Orthopaedics, Nashville, TN.)
Conclusion
Stenosing tenosynovitis of the 4th dorsal extensor compartment is an under-recognized entity that can significantly impact hand function and wrist extension. MRI provides a sensitive method to detect stenosing tenosynovitis and its possible contributing factors. Radiologists should be familiar with this diagnosis in order to guide patient management and improve outcomes.
References
- Massaki AN, Tan J, Huang BK, Chang EY, Trudell DJ, Resnick DL. Extensor retinaculum of the wrist: gross anatomical correlation with MR imaging after ultrasound-guided tenography with emphasis on anatomical features in wrist dorsiflexion responsible for tendon impingement. Skeletal Radiol. 2013 Dec;42(12):1727-37. doi: 10.1007/s00256-013-1739-8. ↩
- Palmer AK, Skahen JR, Werner FW, Glisson RR. The extensor retinaculum of the wrist: an anatomical and biomechanical study. J Hand Surg Br. 1985 Feb;10(1):11-6. doi: 10.1016/s0266-7681(85)80006-1. ↩
- Robertson BL, Jamadar DA, Jacobson JA, Kalume-Brigido M, Caoili EM, Margaliot Z, De Maeseneer MO. Extensor retinaculum of the wrist: sonographic characterization and pseudotenosynovitis appearance. AJR Am J Roentgenol. 2007 Jan;188(1):198-202. doi: 10.2214/AJR.05.0764. ↩
- Adams JE, Habbu R. Tendinopathies of the Hand and Wrist. J Am Acad Orthop Surg. 2015 Dec;23(12):741-50. doi: 10.5435/JAAOS-D-14-00216. Epub 2015 Oct 28. Erratum in: J Am Acad Orthop Surg. 2016 Feb;24(2):123. ↩
- Khazzam M, Patillo D, Gainor BJ. Extensor tendon triggering by impingement on the extensor retinaculum: a report of 5 cases. J Hand Surg Am. 2008 Oct;33(8):1397-400. doi: 10.1016/j.jhsa.2008.04.007. ↩
- Moraux A, Le Corroller T, Aumar A, Bianchi S. Stenosing tenosynovitis of the extensor digitorum tendons of the hand: clinical and sonographic features. Skeletal Radiol. 2021 Oct;50(10):2059-2066. doi: 10.1007/s00256-021-03784-x. ↩
- VanHeest AE, Luger NM, House JH, Vener M. Extensor retinaculum impingement in the athlete: a new diagnosis. Am J Sports Med. 2007 Dec;35(12):2126-30. doi: 10.1177/0363546507305803. ↩
- Wilson SM, Dubert T, Rozenblat M. Extensor tendon impingement in a gymnast. J Hand Surg Br. 2006 Feb;31(1):66-7. doi: 10.1016/j.jhsb.2005.08.010. ↩
- Mahajan NP, Palange ND, Pawar E, Supe A. Surgical Treatment of Tenosynovitis of Extensor Tendons of Fourth Compartment of Wrist in Nonrheumatoid Patients-A Case Series of 10 Patients in India. J Hand Microsurg. 2019 Apr;11(1):45-49. doi: 10.1055/s-0038-1669368. ↩
