Clinical History: A 25-year-old male presents with wrist pain. Axial T1- (1a) and axial fat-suppressed T2- (1b) weighted MRI images of the wrist are provided. What are your findings? What is your diagnosis?
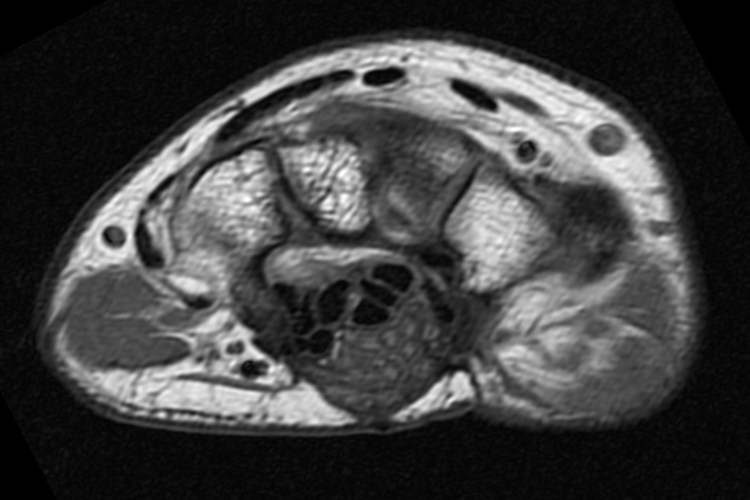
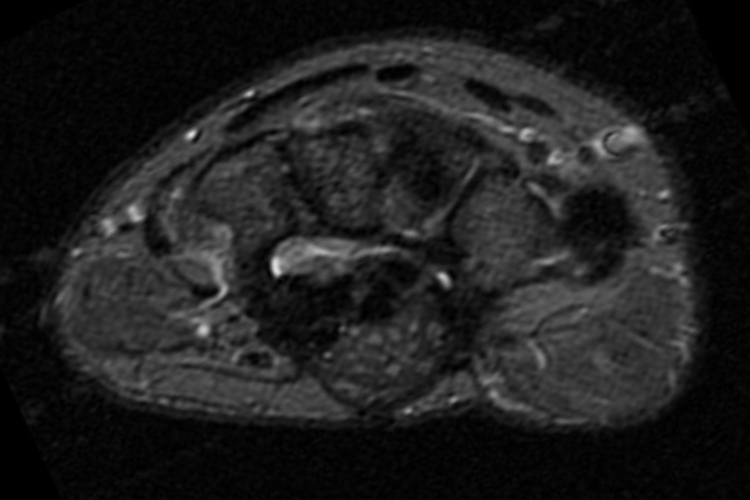
Figure 1
Findings
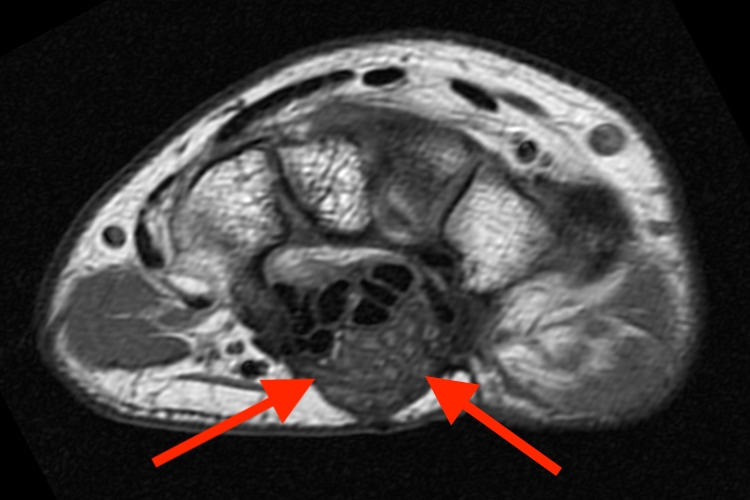
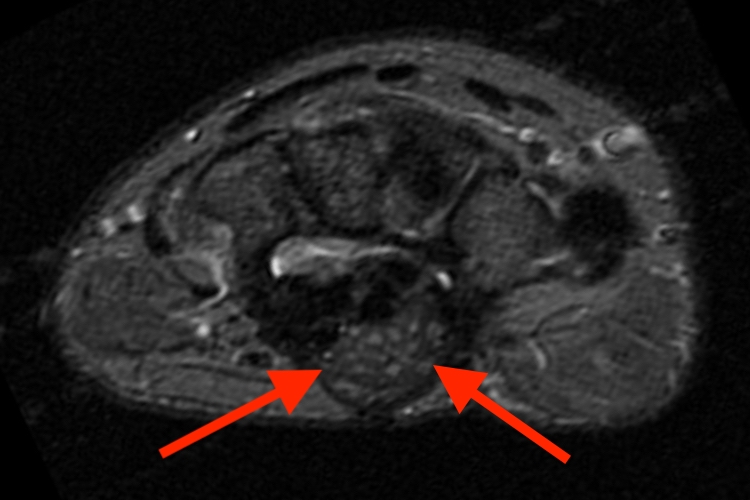

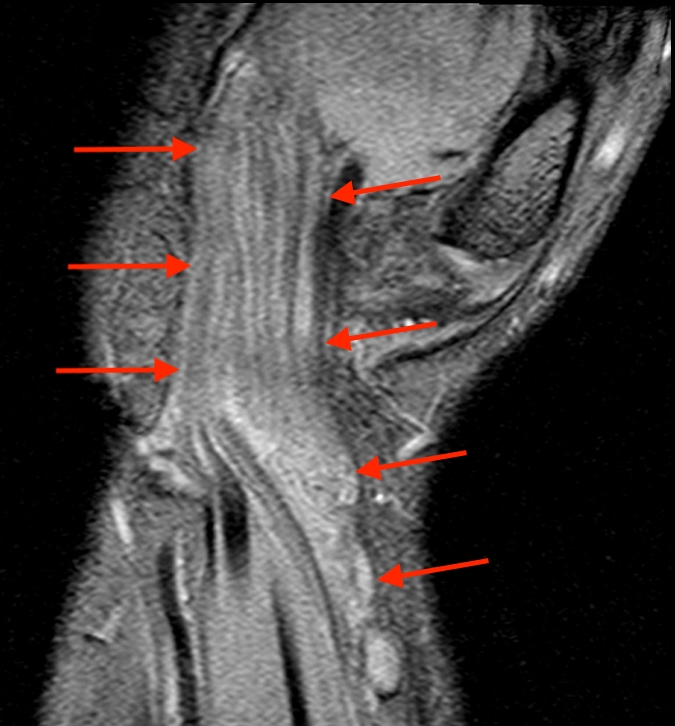
Figure 2: Axial T1- (2a) and axial fat-suppressed T2- (2b) weighted MRI images of the wrist at the level of the carpal tunnel demonstrate a mass-like expansion of the median nerve (arrows) with multiple enlarged neural fascicles and resultant volar bowing of the flexor retinaculum. Coronal T1-weighted (2c) and coronal gradient-echo (2d) images of the wrist demonstrate fusiform median nerve mass-like enlargement, extending from the forearm, through the carpal tunnel, into the hand (arrows).
Diagnosis
Lipomatosis of the median nerve.
Introduction
Originally described by Mason in 19531, lipomatosis of nerve (LN) has undertaken several names including fibrolipomatous hamartoma, lipofibromatous hamartoma, neural fibrolipoma, lipofibroma, and fatty infiltration of the nerve2,3. The World Health Organization adopted the designation of lipomatosis of nerve in 2002, which remains the current preferred designation4. This uncommon condition results in tumorlike enlargement of a peripheral nerve (most commonly the median nerve5,6), potentially with involvement of distal branches, territorial bones, and adjacent soft tissues. This Web Clinic reviews the entity, clinical background, and provides multiple imaging examples.
Discussion
70% of patients with LN present before the age of 303. The majority in children present before age 10 and have no family history of the disease. Males and females are equally affected6. Patients often present with a non-painful soft tissue mass, following the distribution of the affected nerve. Patients can experience progressive pain, numbness, weakness, and parathesias, particularly in cases of neural compression or entrapment7,8. Macrodactyly is seen in 27-67% of cases, particularly when digital branches of the affected nerve are involved, and is termed macrodystrophia lipomatosa (figures 3, 6)2,6. When macrodactyly occurs, it typically involves the second and third digits of the hand or foot, but multiple digits may be affected6.
Figure 3: Lipomatosis of the median nerve with macrodystrophia lipomatosa - INTERACTIVE IMAGE. Artist rendering of the wrist and hand demonstrates lipomatosis of the median nerve with enlargement and extension into the first, second, and third digit digital nerves. Associated boney macrodactyly of the thumb, index, and middle finger is present, with fibrofatty enlargement of the thenar musculature. (To view the interactive image, use the left mouse button to click on an area at the right side of the image, then hold the button while dragging to the left.)
LN most commonly involves the upper extremity, with most (59.9%) cases involving the median nerve3. In median nerve cases, the LN is typically located within the carpal tunnel and may follow a branching pattern extending into the hand and fingers. Involvement proximal to the wrist is rare. Additional reported areas include the plantar (11.2%), ulnar (7%), radial, sciatic, femoral, obturator, tibial, superficial peroneal, and sural nerves3. Brachial plexus, lumbosacral plexus, and even cranial involvement have been reported3,9,10. LN does not seem to occur intradurally3.
The exact etiology of LN is not yet understood. Some believe the etiology is congenital or developmental abnormal growth of fibrofatty tissue, with possible genetic associations involving PIK3CA or other genes3,11. The entity has been found in some patients at birth, supporting a congenital origin12. Associations with Proteus syndrome and Klippel-Trenaunay-Weber syndrome have been discussed13. Others believe LN is an acquired or reactive process due to prior trauma, repetitive microtrauma or nerve irritation (such as in carpal tunnel syndrome patients). Some authors propose a combination of both congenital and microtrauma are responsible for the entity11.
On gross examination, LN demonstrates diffuse enlargement of the affected nerve, appearing as a tan-yellow fibrofatty mass within the nerve sheath2,6. Histologically, LN demonstrates a hamartomatous proliferation of mature fat and fibroblasts within the epineurium, interspersed among nerve bundles, resulting in marked expansion of the nerve. The proportion of the components may vary. The surrounding tissue shows no involvement or inflammation11. The infiltrative pattern of fat allows distinction from a soft-tissue lipoma adjacent to a nerve2. The nerve fibers are typically intrinsically normal but may show atrophy in cases of late disease2. In cases of macrodystrophia lipomatosa, patients have a diffuse disproportionate increase in fibroadipose tissue along the affected digit2,6. Bony enlargement results from endosteal and periosteal deposition of bone. The periosteum is studded with millimetric nodules containing chondroblasts, osteoblasts, and osteoclasts; these become larger and more numerous towards the distal ends of the phalanges14.
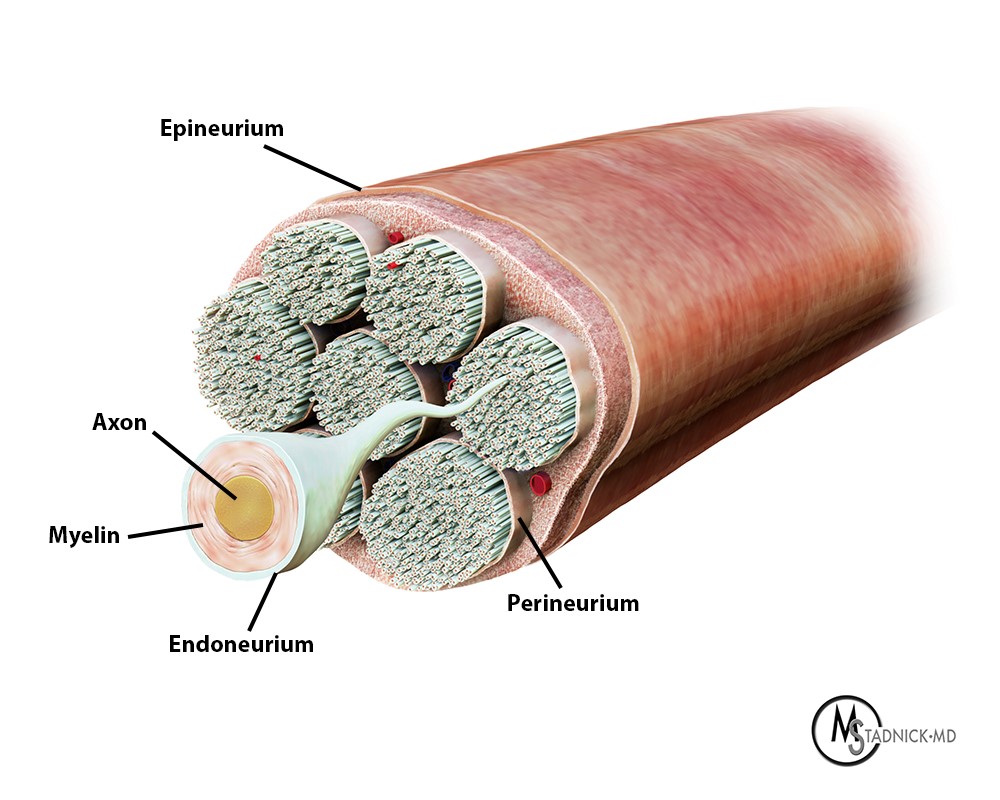

Figure 4: Renderings of Normal Nerve versus Lipomatosis of Nerve. 4a demonstrates normal peripheral nerve anatomy and connective tissue boundaries. Epineurium encases the entire nerve periphery. Perineurium surrounds each fascicle within the nerve. Endoneurium embeds each of the individual axons with the fascicles, bound together by the perineurium. 4b demonstrates a pathologic nerve, affected with lipomatosis. Proliferation of mature adipose tissue is present inside of the epineurium, with abundant fibrous tissue around the fascicles, resulting in prominent nerve enlargement.
Imaging Findings
On radiography, LN patients without macrodactyly are often demonstrate normal x-rays, but may show a soft tissue mass with radiolucent fatty tissue14. If macrodactyly is present, osseous and soft tissue overgrowth is common, which occurs both longitudinally and axially (figure 6d), usually ceasing after puberty2,6,14. Bony overgrowth is more prominent volarly and distally, resulting in distal splaying and bowing2,6,14. On MRI, LN characteristically demonstrates serpentine longitudinally oriented low to intermediate signal nerve fascicles surrounded by adipose tissue, within a diffusely enlarged nerve2,6. The resultant morphology has been likened to a “spaghetti-like” appearance on longitudinal images3 and “coaxial cable-like” appearance on axial images. The latter finding has been described as pathognomonic for LN5,15, subsequently allowing a confident MRI diagnosis12. MRI is also useful preoperatively, as LN cannot be excised without sacrificing the pathologic nerve, distinguishing itself from other tumors such as an intraneural lipoma12. The neural branching pattern of LN is evident with MRI, which can be used to map out the extent of the disease. In patients with macrodactyly, increased fat is also noted within the affected digits2,6.
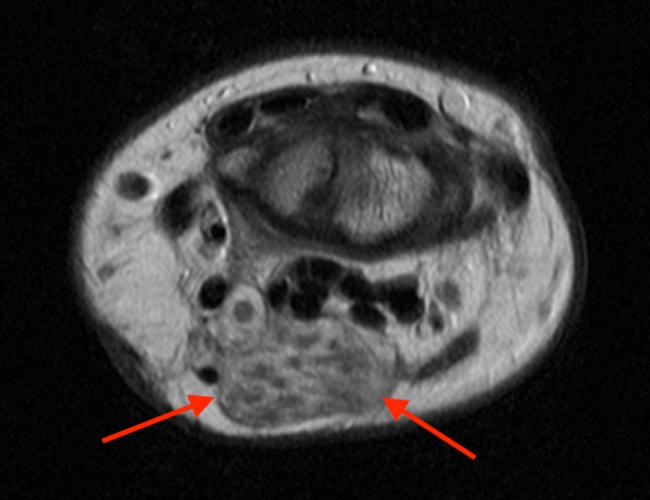
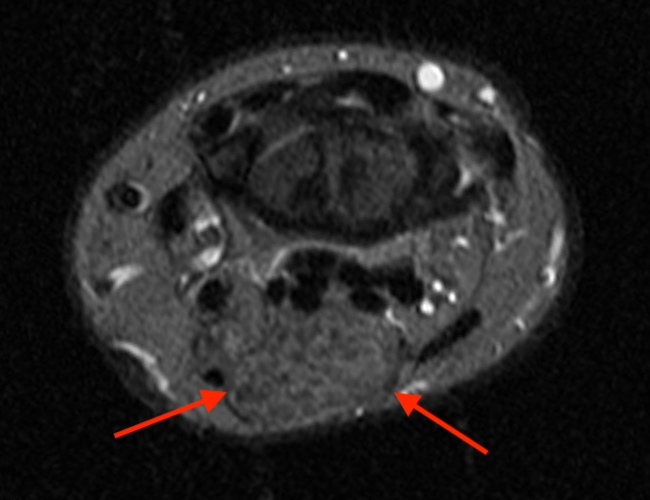
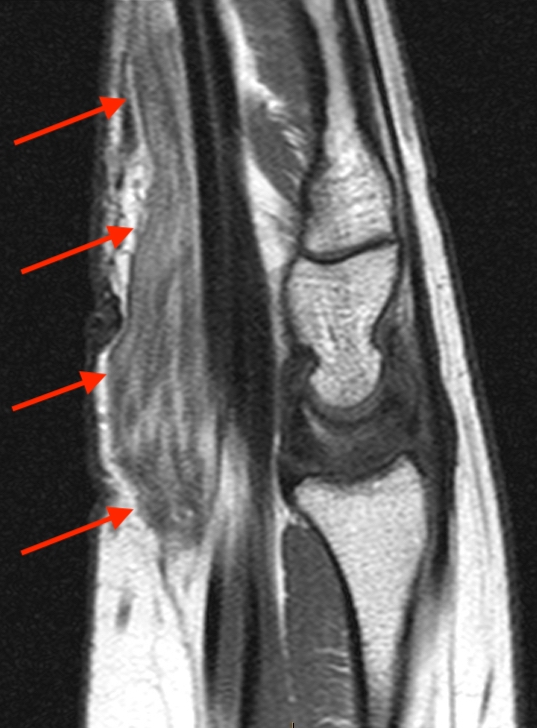

Figure 5: Lipomatosis of the median nerve (example 2). Axial proton density- (5a) and axial fat-suppressed T2- (5b) weighted MRI images of the wrist at the level of the proximal carpal row demonstrate a mass-like expansion of the median nerve (arrows). Sagittal T1-weighted image (5c) demonstrates the low signal enlarged neural fascicles embedded in surrounding hyperintense adipose tissue. Coronal gradient-echo (5d) images of the wrist demonstrates the extent of the median nerve mass-like enlargement, extending from the forearm, through the carpal tunnel, into the hand (arrows).
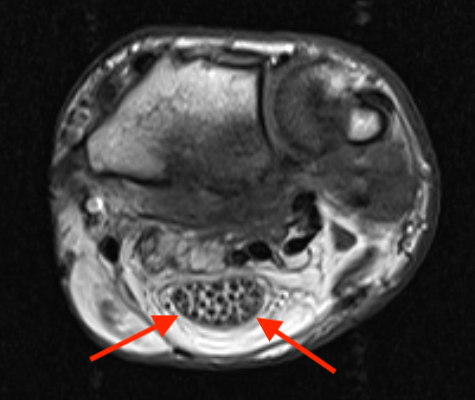
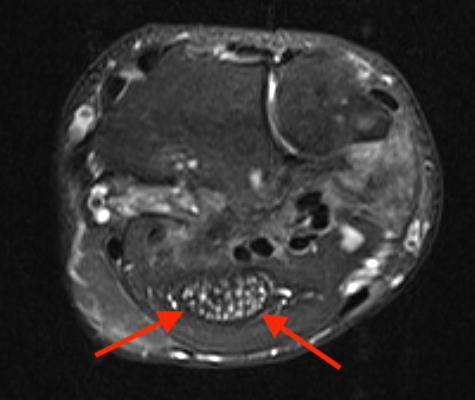


Figure 6: Lipomatosis of nerve with macrodystrophia lipomatosa. Axial proton density- (6a) and axial fat-suppressed T2- (6b) weighted MR images at the level of the distal forearm demonstrate a mass-like expansion of the median nerve (arrows). Coronal T1-weighted image (6c) demonstrates thenar muscle enlargement with fatty infiltration (arrow). A low signal oval body is also noted proximal to the triquetrum. Frontal hand radiograph (6d) demonstrates enlargement of the thumb and thenar musculature with second ray osteolysis extending to the metacarpal. Macrodystrophic enlargement of the thumb and long finger is also present.
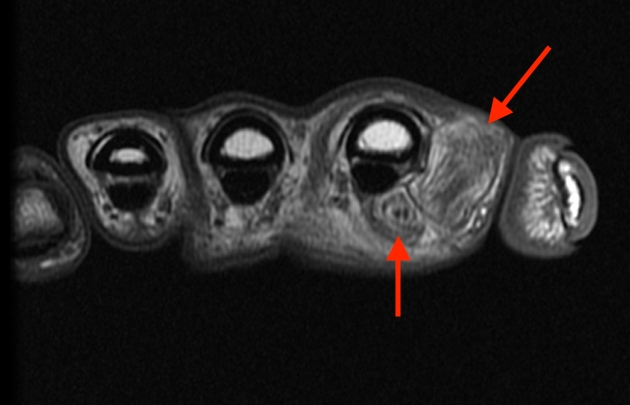
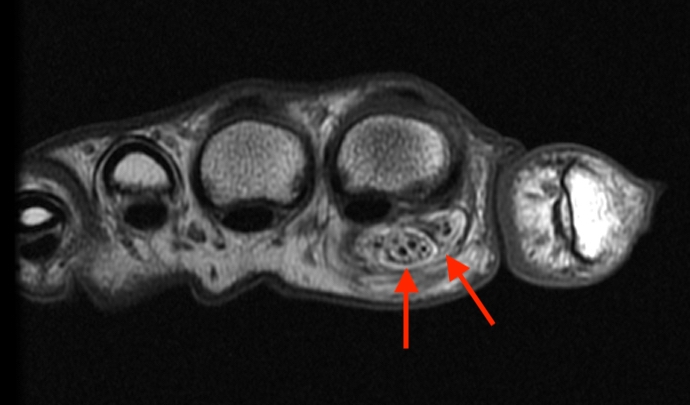
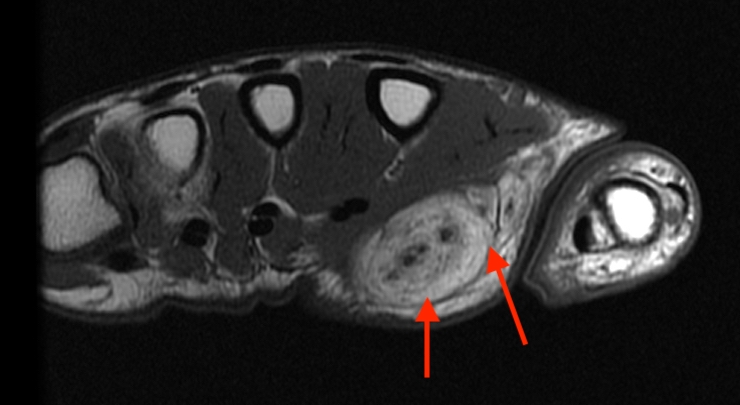
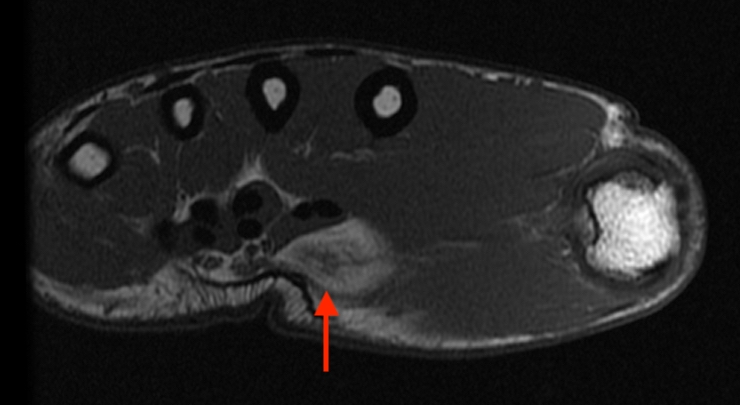
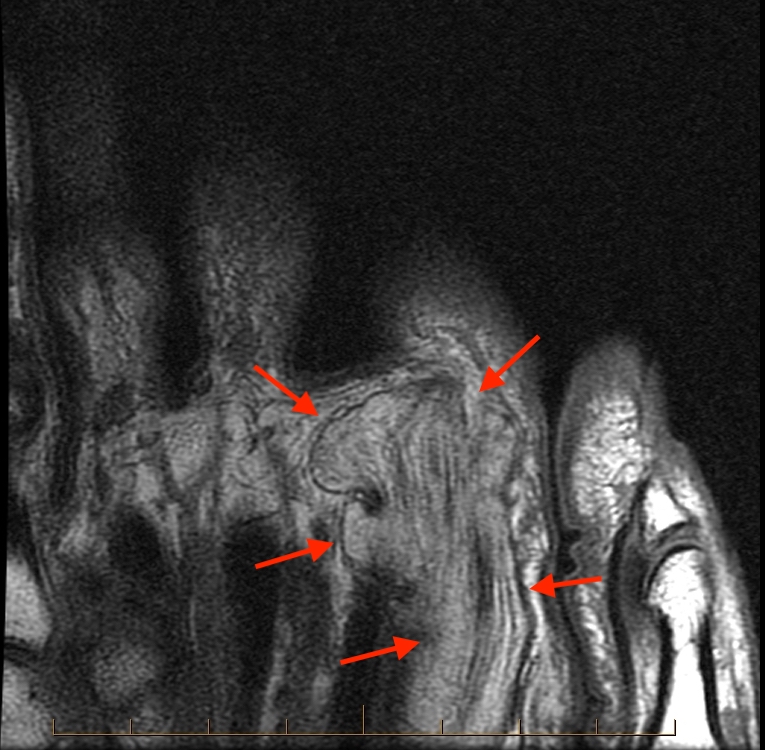
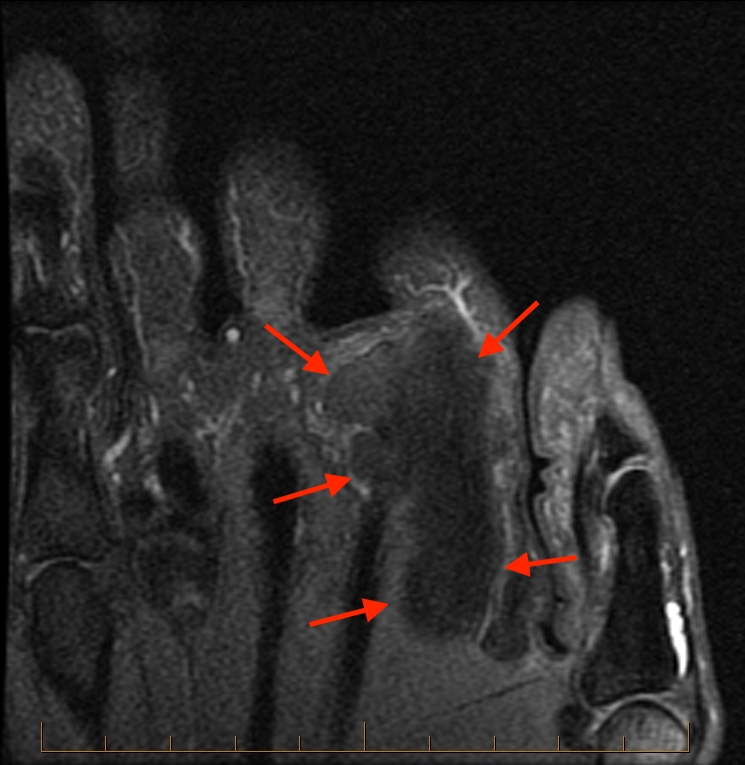
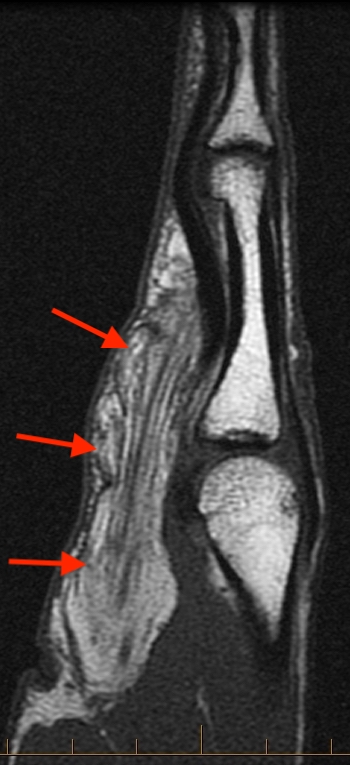

Figure 7: Lipomatosis of a digital nerve. Multiple distal to proximal T1-weighted axial images of the hand (7a-d) demonstrate masslike enlargement of index finger radial digital nerve, containing thickened neural fascicles. Coronal (7e-f) and sagittal (7g-h) T1-and fat-suppressed T2-weighted images nicely demonstrate the macroscopic fat contents within the neural enlargement.

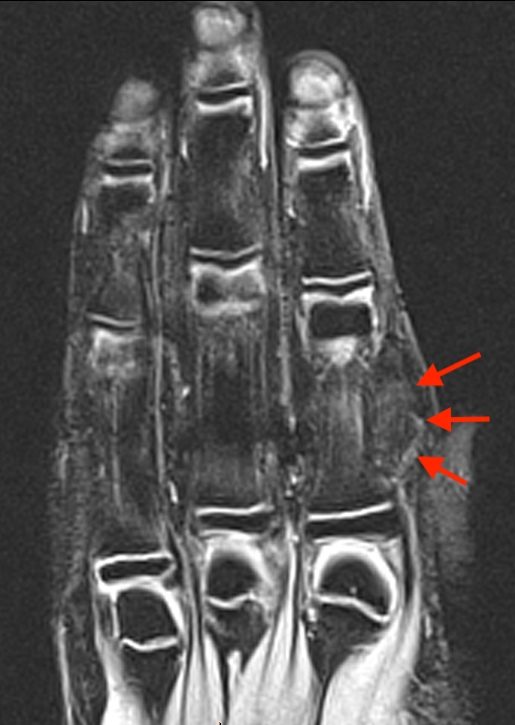
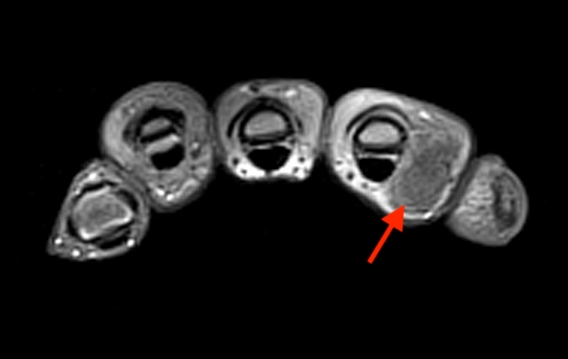
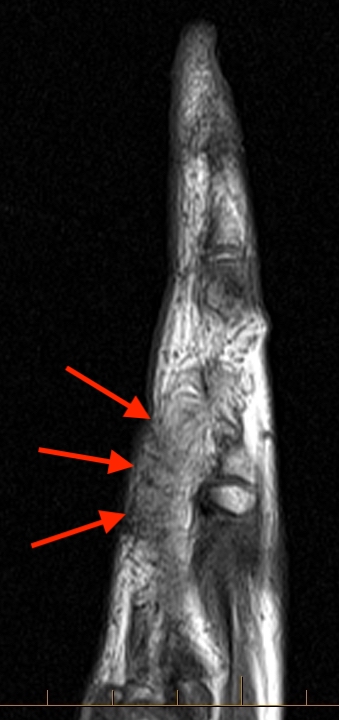
Figure 8: Lipomatosis of a digital nerve (example 2). Coronal T1- (8a), coronal fat-suppressed T2- (8b), axial fat-suppressed proton density-, and sagittal T2-weighted images demonstrate mass-like enlargement of the index finger radial digital nerve in this 12-year-old male, with thickened neural fascicles.


Figure 9: Lipomatosis of nerve with macrodystrophia lipomatosa (example 2). 9a: Clinical photograph demonstrating a 27-year-old male with macrodystrophia lipomatosa involving the radial aspect of the hand. The thumb (arrow) and thenar musculature (*) are enlarged. The enlarged second digit has been surgically resected. 9b: Corresponding radiograph of the same patient. The thumb (arrow) and thenar musculature (*) are enlarged. The residual second metacarpal base also demonstrates macrodystrophic enlargement. 9c: Sequential axials T1-weighted images of the same patient demonstrate macrodystrophic enlargement of the thumb and residual second metacarpal base, thenar musculature (with fatty infiltration), median, first and second digital nerves. Images courtesy of Brady Huang, University of California at San Diego
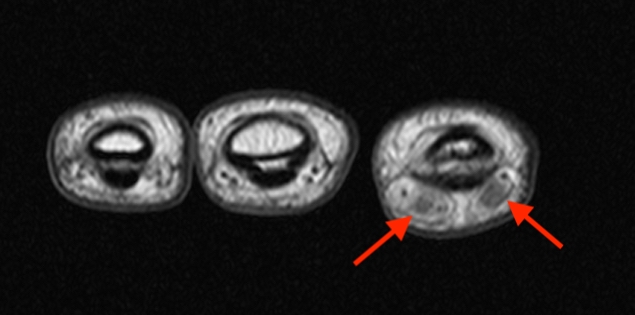
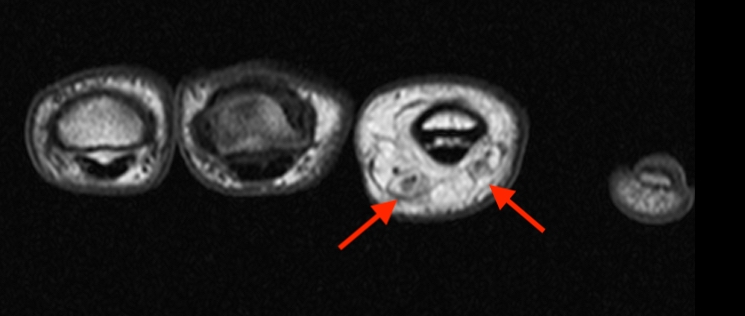
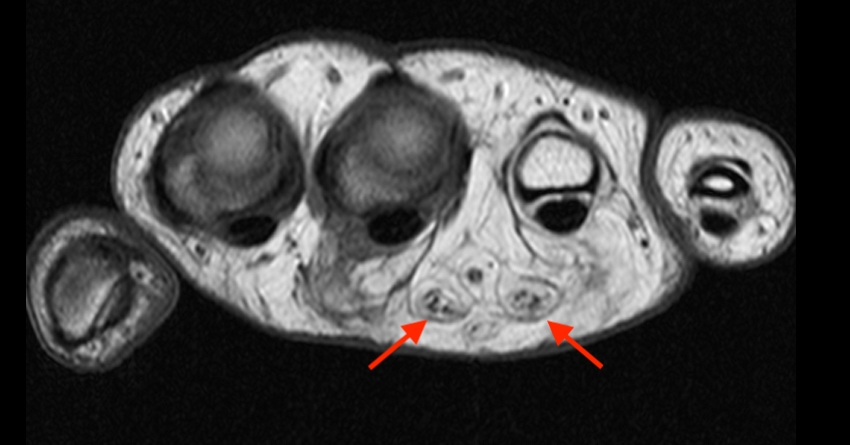
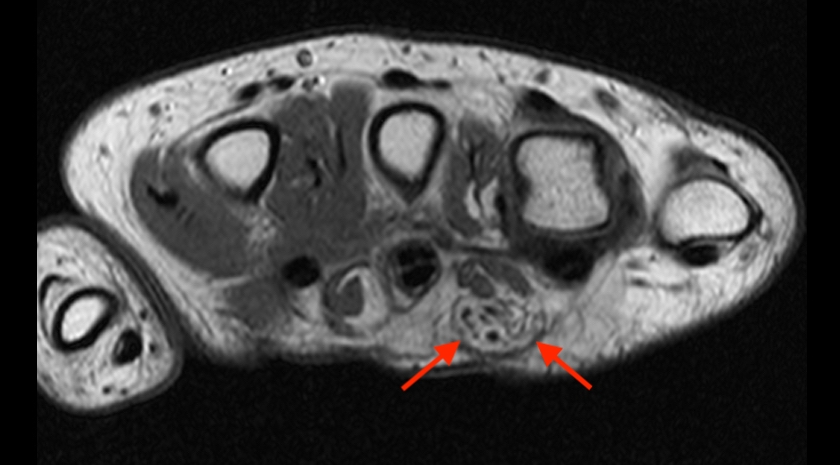


Figure 10: Lipomatosis of nerve with macrodystrophia lipomatosa (example 3). Multiple distal to proximal T1-weighted axial images of the hand (10a-d) demonstrate fibrofatty enlargement of the ring finger digital nerves. Coronal T1-weighted image of the hand (10e) demonstrates fibrofatty enlargement of the radial finger digital nerves, continuing into the common palmar digital nerves. Coronal inversion recovery image (10f) demonstrates macrodystrophia of the ring finger distal phalanx (arrows).
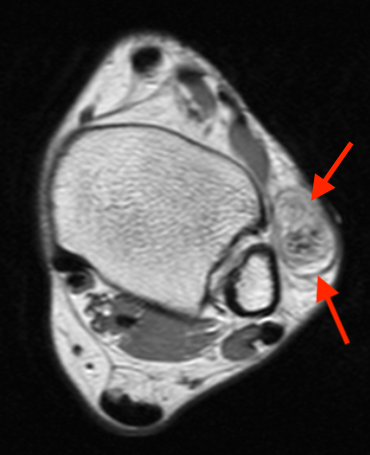
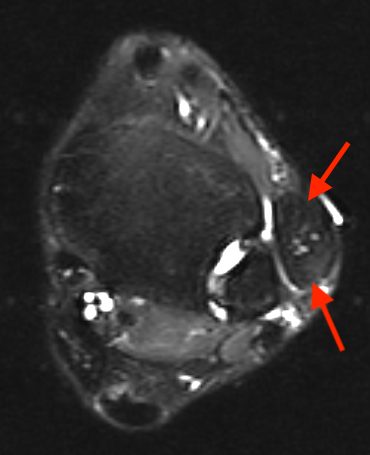
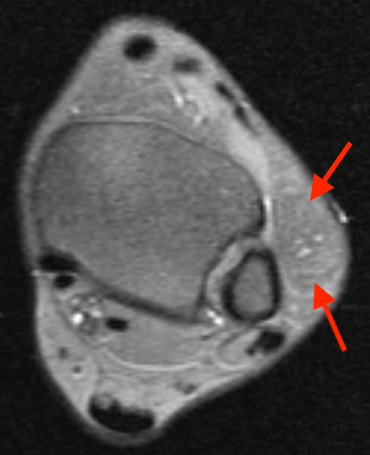
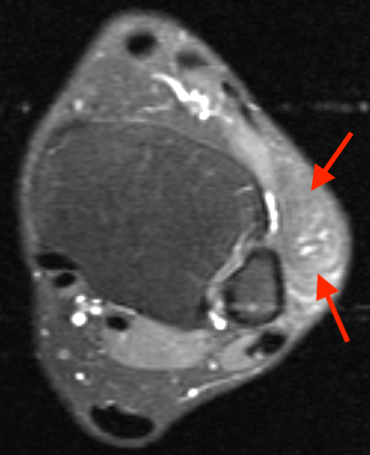
Figure 11: Lower extremity - lipomatosis of the lateral cutaneous nerve. Axial T1-(11a), axial fat-suppressed T2- (11b), and axial fat-suppressed T1- (11c) weighted images demonstrate mass-like enlargement of the lateral cutaneous nerve at the level of the ankle, containing macroscopic fat and enlarged neural fascicles, consistent with a FLH. A fat-suppressed post-IV contrast sequence (11d) demonstrates no significant enhancement.

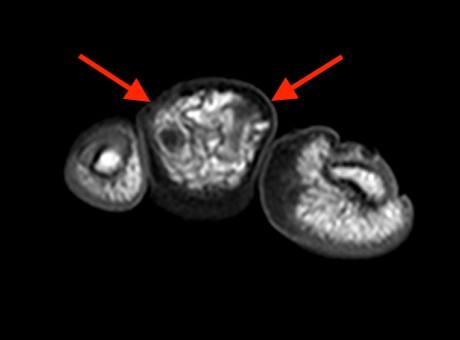
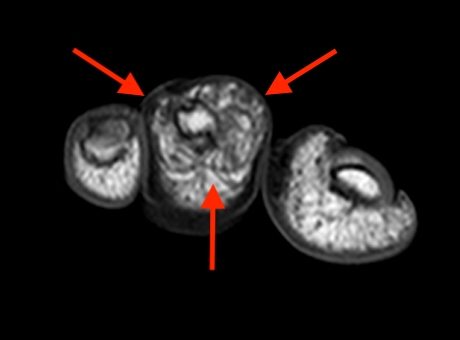
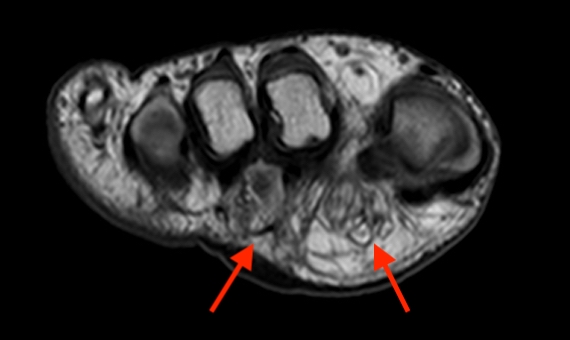
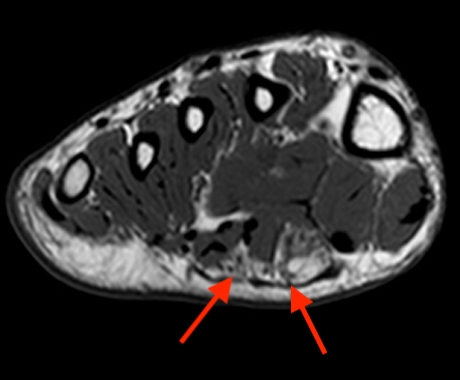
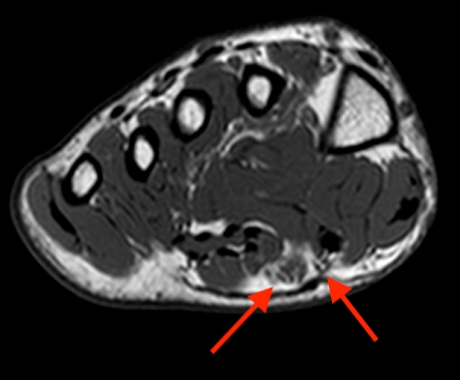
Figure 12: Lower extremity - lipomatosis of plantar and digital nerves. Coronal fat-suppressed proton density- (12a) and axial T1- (12b) weighted images demonstrate macrodystrophic enlargement of the second toe distal phalanx (arrows). Progressive axial T1-weighted images into the foot (12c-f) demonstrate fatty enlargement of the first and second plantar digital nerves, extending into the midfoot (arrows).
Treatment
LN treatment options vary and are usually determined on a case-by-case basis and can range from observation to complete nerve resection. Asymptomatic patients are typically treated with observation8. In symptomatic LN cases involving the median nerve at the carpal tunnel, carpal tunnel release is often performed (figure 13) and can decrease pain and improve oppositional strength10. Carpal tunnel release may be performed in conjunction with external neurolysis8. More invasive procedures such as debulking and microsurgical interfascicular dissection are typically reserved for patients with more progressive symptoms and/or nerve compression. Due to the involvement of intraneural elements, these procedures carry a high complication risk as postoperative fibrosis may impair nerve conduction and result in long-term functional deficits8,11. Complete excision of the lesion is rarely recommended for LN due to the benign nature of the lesion, risk of functional impairment, and possible formation of painful postoperative neuromas8 . Macrodactyly cases with deformity may be treated with debulking procedures and/or amputation, with the intent of reducing symptoms, cosmetics, or improving function2,3. Recurrent overgrowth can also occur after debulking procedures, requiring additional operations3.
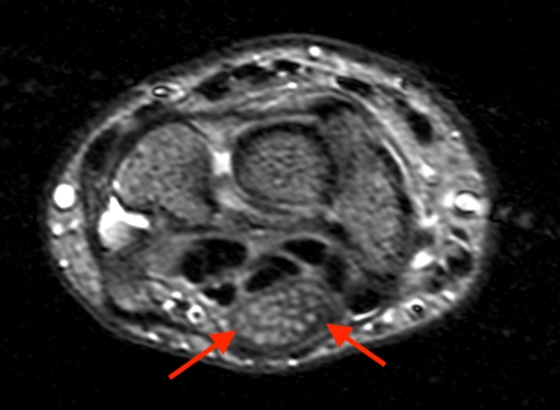
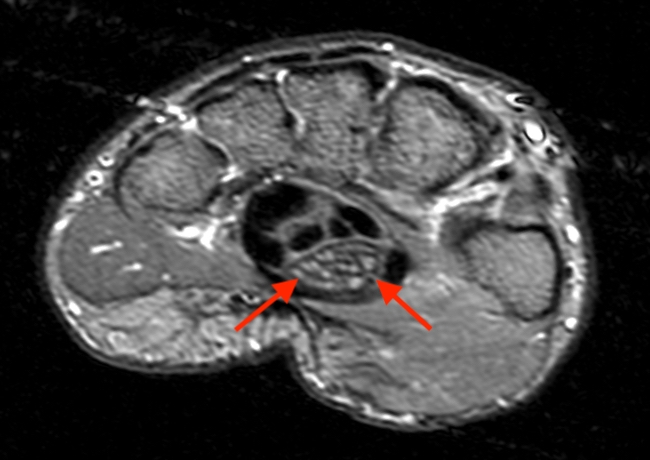
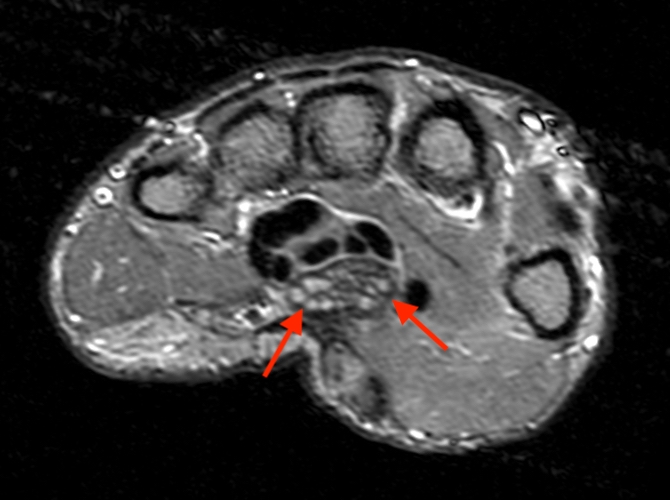
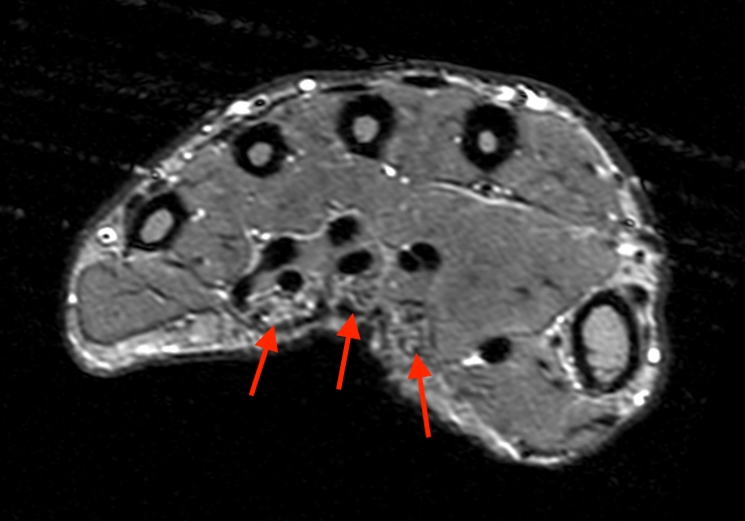


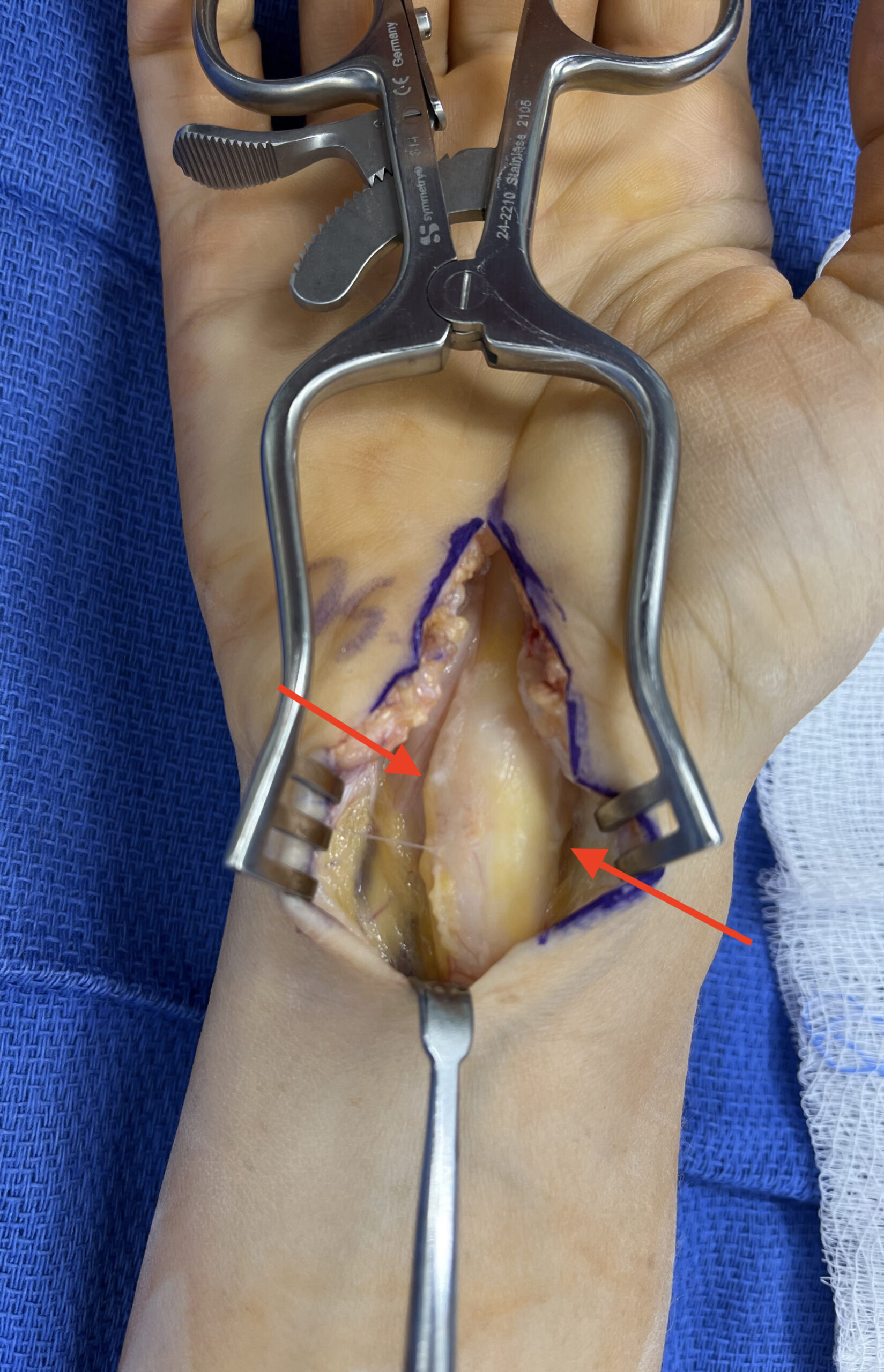
Figure 13: Lipomatosis of the median nerve – treatment example. Multiple axial inversion recovery images (13a-d) demonstrate fasciculated enlargement of the median nerve throughout the carpal tunnel, continuing into the proximal volar digital branches (arrows). Coronal T1-weighted (13e) and gradient-echo (13d) images demonstrate the mass-like median nerve enlargement (arrow). Intraoperative image (13e) confirms the mass-like enlargement of the median nerve (arrow), and a carpal tunnel release was performed. Image courtesy of Samuel Crosby, MD – Elite Sports Medicine & Orthopedics, Nashville, TN
Summary
Lipomatosis of nerve has been known by several eponyms, is a benign overgrowth of mature fat and fibrous tissue contained within the epineurium of a nerve, and results in expansile masslike neural enlargement. The most common location is within the median nerve at the carpal tunnel. The etiology is uncertain and may be related to prior nerve injury and/or an underlying genetic abnormality. The MRI imaging appearance is pathognomonic, demonstrating a “coaxial cable-like” appearance on axial images. Treatment options vary, with conservative measures often preferred to maintain nerve function.
References
- Mason M. AMERICAN Society for Surgery of the hand. J Bone Joint Surg Am. 1953;35-A(1):257-275. ↩
- Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. Benign musculoskeletal lipomatous lesions. Radiographics. 2004;24(5):1433-1466. doi:10.1148/rg.245045120 ↩
- Marek T, Mahan MA, Carter JM, et al. What’s known and what’s new in adipose lesions of peripheral nerves? Acta Neurochir (Wien). 2021;163(3):835-842. doi:10.1007/s00701-020-04620-2 ↩
- Folpe A, Giannini C. Soft Tissue and Bone Tumours WHO Classification of Tumours. Vol 3. 5th ed. IARC Publications; 2020. ↩
- Toms AP, Anastakis D, Bleakney RR, Marshall TJ. Lipofibromatous hamartoma of the upper extremity: A review of the radiologic findings for 15 patients. American Journal of Roentgenology. 2006;186(3):805-811. doi:10.2214/AJR.04.1717 ↩
- Murphey MD, Smith WS, Stacy, Smith E, Kransdorf MJ, Thomas Temple H. From the Archives of the AFIP Imaging of Musculoskeletal Neurogenic Tumors: Radiologic-Pathologic Correlation. Vol 19.; 1999. ↩
- Oleaga L, Florencio MR, Erefio C, et al. Skeletal Radiology Fibrolipomatous Hamartoma of the Radial Nerve: MR Imaging Findings Clinical Information. Vol 24.; 1995. ↩
- Roh YT, Song SW, Jeong C, Kang Y, Park IJ. Carpal tunnel syndrome caused by lipofibromatous hamartoma of the median nerve. J Korean Neurosurg Soc. 2020;63(5):664-670. doi:10.3340/jkns.2020.0082 ↩
- Azeemuddin M, Waheed AA, Khan N, Sayani R, Ahmed A. Fibrolipomatous Hamartoma of the Median Nerve with Macrodystrophia Lipomatosa. Cureus. Published online March 9, 2018. doi:10.7759/cureus.2293 ↩
- Barraza-Silva J, Berebichez-Fridman R, Corona-Cobian LE, Bernal-López LM, Álvarez-San Martín R. Lipofibromatous hamartoma of a digital branch of the median nerve: A case report and review of literature. Clin Case Rep. 2021;9(9). doi:10.1002/ccr3.4728 ↩
- Soffar MM, Fadali G, Ghalab MA, Abouzaid AM. Lipofibromatous hamartoma of digital nerve: A case report. Plast Reconstr Surg Glob Open. 2021;9(12). doi:10.1097/GOX.0000000000003981 ↩
- De Maeseneer Jaovisidha L Lenchik D Witte ME Schweitzer DJ Sartoris D Resnick MS, De Maeseneer M, Jaovisidha S, et al. Fibrolipomatous Hamartoma: MR Imaging Findings. Vol 26.; 1997. ↩
- Kuo YL, Wu YH, Hsiao PF, Hsieh YJ. Lipofibromatous hamartoma of the superficial peroneal nerve: Two case reports. Dermatologica Sinica. 2012;30(1):21-24. doi:10.1016/j.dsi.2011.09.007 ↩
- Goldman’ And AB, Kaye’ JJ. Macrodystrophia Lipomatosa : Radiographic Diagnosis. Vol 128.; 1977. www.ajronline.org ↩
- Bordalo-Rodrigues M, Amin P, Rosenberg ZS. MR imaging of common entrapment neuropathies at the wrist. Magn Reson Imaging Clin N Am. 2004;12(2):265-279. doi:10.1016/j.mric.2004.02.008 ↩
