

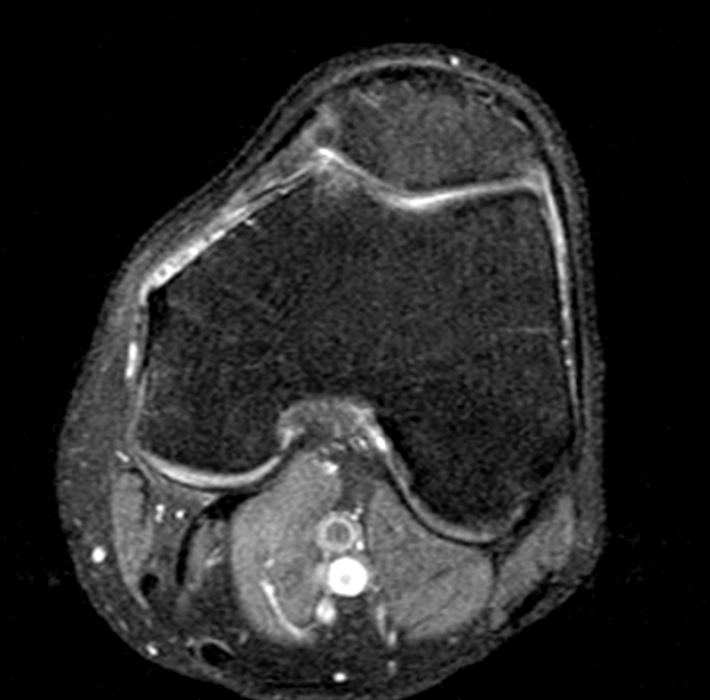


An active, previously healthy, 65-year-old man presents with a 3-week history of atraumatic left knee pain. A frontal radiograph (1a), proton density fat-suppressed sagittal MR image (1b), proton density fat-suppressed axial MR image (1c), and selected arthroscopic images (1d and 1e) are provided. What are the findings? What is the diagnosis?
Findings
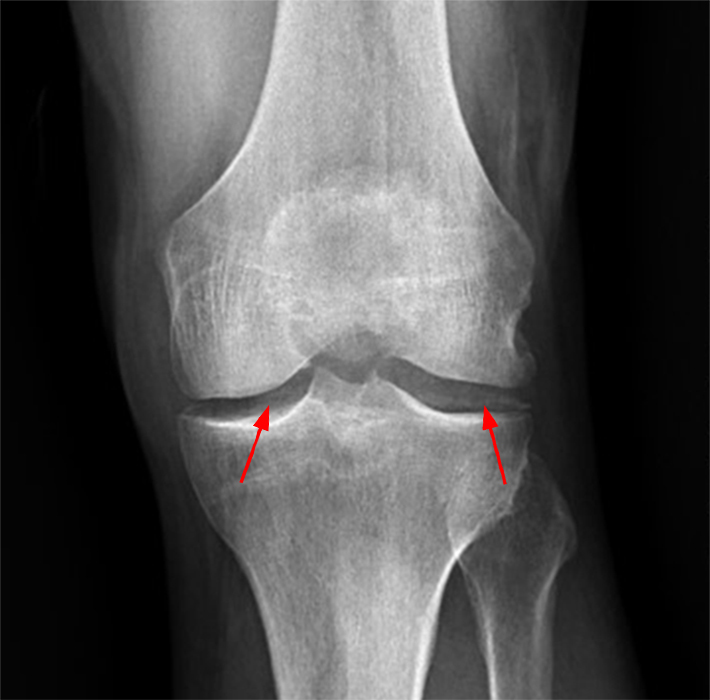

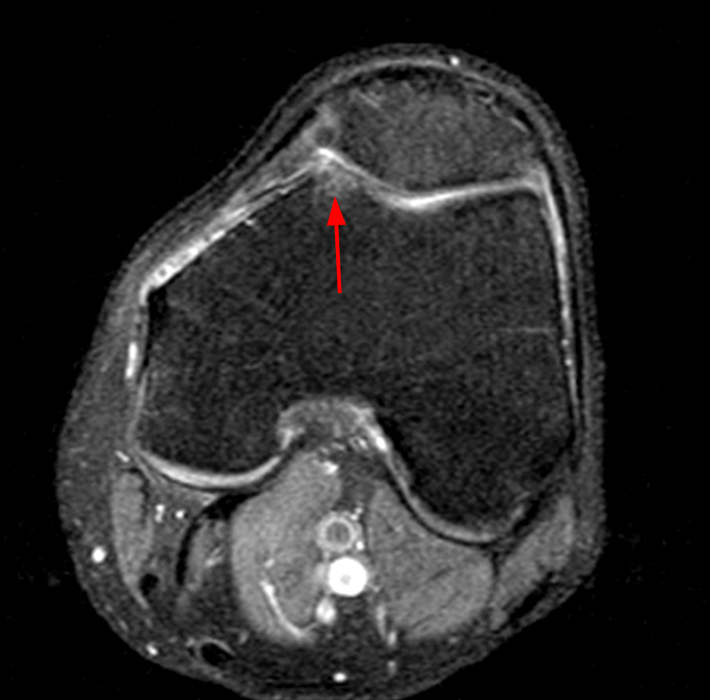
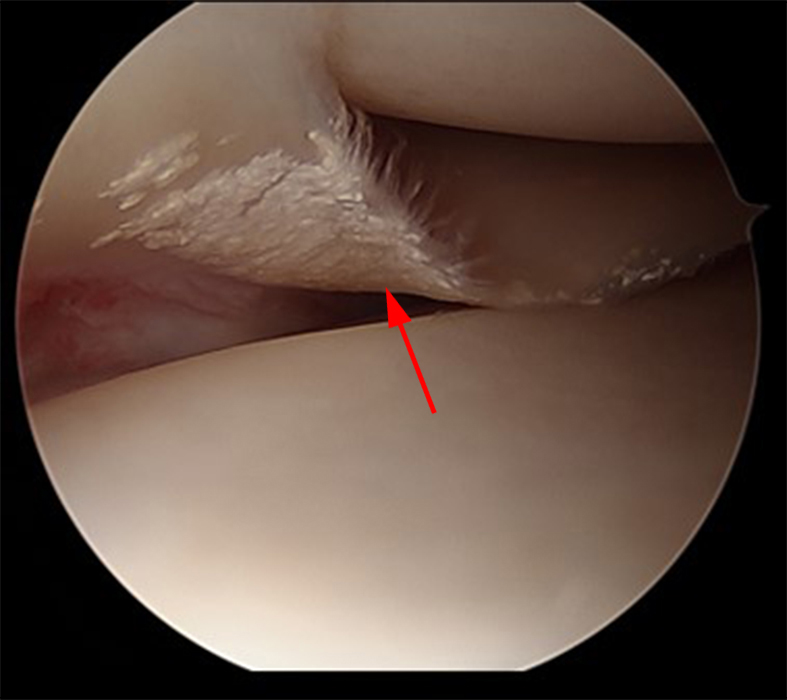
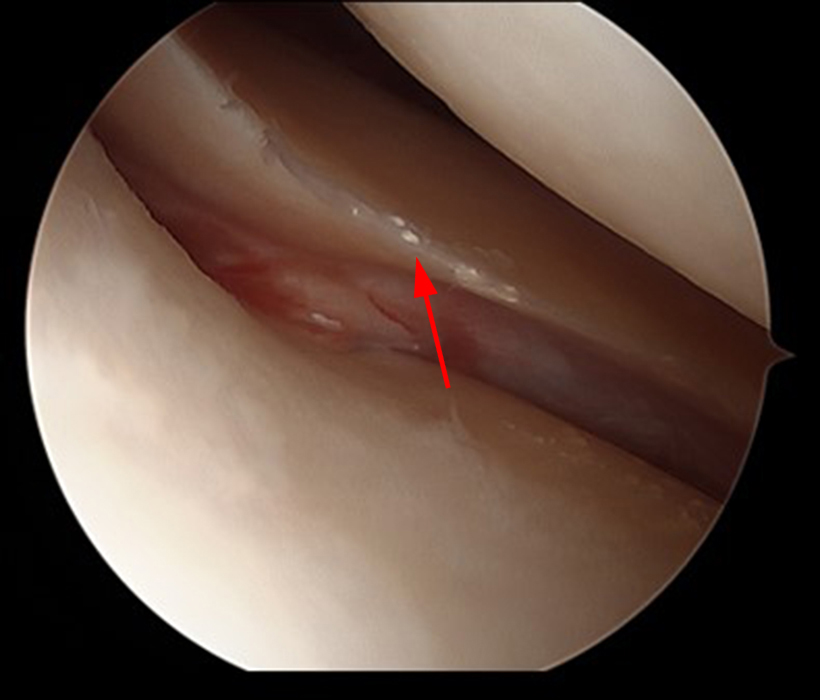
The knee radiograph demonstrates medial and lateral femorotibial compartment chondrocalcinosis, (2a, red arrows), and mild medial femorotibial compartment joint space narrowing. Proton density fat-suppressed sagittal (2b) and proton density fat-suppressed axial MR images (2c) demonstrate high grade trochlear cartilage loss with accompanying subchondral marrow edema and cystic change (red arrows). Selected arthroscopic images demonstrate mineralization of the medial (2d) and lateral (2e) menisci (red arrows). Synovial biopsy at the time of arthroscopy showed crystal deposits consistent with calcium pyrophosphate dihydrate crystal deposition disease.
Diagnosis
Calcium pyrophosphate dihydrate crystal deposition disease.
Introduction
Calcium pyrophosphate dihydrate (CPPD) crystal deposition disease is one of the most common articular disorders, particularly in the elderly population. The most recognized imaging feature of this disorder is cartilage calcification, termed chondrocalcinosis. Chondrocalcinosis alone, however, is not the only significant imaging feature of this disease. Additional characteristic imaging findings include other intraarticular and periarticular calcifications and structural joint damage, the latter termed pyrophosphate arthropathy. In fact, the pattern and distribution of pyrophosphate arthropathy are distinctive and can often be differentiated from the features of osteoarthrosis to allow an accurate diagnosis of CPPD crystal deposition disease even in the absence of chondrocalcinosis.1
Seminal work by McCarty and others in 1961 and 1962 discovered non-urate crystals in the joint fluid of patients experiencing gout-like attacks of arthritis, crystals that were subsequently identified as CPPD crystals by their x-ray diffraction powder pattern.2,3
Analysis of clinical and radiographic findings demonstrated that this same disease process had been described previously as chondrocalcinosis polyarticularis. Therefore, it became clear that patients with a distinctive gout-like pattern of arthritis (i.e., pseudogout syndrome) had crystal accumulation within joints (CPPD crystal deposition) that could cause cartilage calcification (chondrocalcinosis).
Terminology
Calcium pyrophosphate dihydrate (CPPD) crystal deposition disease: General term for a disorder characterized by the presence of CPPD crystals in and around joints.
Pseudogout: Term applied to one of the clinical patterns that may be associated with crystal deposition—intermittent acute attacks of arthritis that simulate those of gout.
Chondrocalcinosis: Term reserved for pathologically or radiographically evident cartilage calcification.
Articular and periarticular calcification: Term used for pathologically or radiographically evident calcification in and around joints.
Tophaceous pseudogout: Term used for soft tissue mass-like deposits of CPPD crystals.
Pyrophosphate arthropathy: Term used to describe a peculiar and specific pattern of structural joint damage occurring in CPPD crystal deposition disease, with some features that overlap with those of degenerative joint disease.
Clinical Patterns
CPPD crystal deposition disease affects both men and women and is generally observed in middle-aged and elderly patients.4 A pattern of disease simulating gout and therefore designated pseudogout occurs in about 10 to 25% of symptomatic patients with CPPD crystal deposition disease.5 This pattern is characterized by acute or subacute self-limited attacks of arthritis and may be precipitated by trauma, surgery, medical illness, or intraarticular injection.6 A second clinical pattern characterized by almost continuous attacks of arthritis simulating rheumatoid arthritis (i.e., pseudorheumatoid arthritis) is seen in about 5% of symptomatic patients.7,8 In 50-60% of symptomatic patients, chronic articular disease with or without acute exacerbations simulates osteoarthrosis (i.e. pseudo-osteoarthrosis).8 Additional less frequent patterns can mimic neuropathic osteoarthropathy1 and spondyloarthropathy.9 It should be emphasized, however, that most persons with CPPD crystal deposition disease are asymptomatic, with the deposits likely occurring as a consequence of aging and detected as an incidental and unexpected finding on imaging studies done for unrelated reasons.4
Familial forms of CPPD crystal deposition disease also exist. The two main forms of familial CPPD crystal deposition disease correspond to mutations at a locus on chromosome 8q (CCAL1) and mutations at a locus on chromosome 5p (CCAL2).10,11 These mutations are inherited in an autosomal dominant fashion, with a high degree of penetrance.10 Mutations in the ankylosis human analog (ANKH) gene on chromosome 5p are implicated in the CCAL2 subtype of familial CPPD crystal deposition disease, whereby ANKH protein activity is enhanced, elevating extracellular pyrophosphate levels and promoting the formation of CPPD crystals.10 Mutations in osteoprotegerin (OPG) have recently been implicated in the CCAL1 subtype of familial CPPD crystal deposition disease.12 Interestingly, this subtype of familial CPPD crystal deposition disease does not result in alterations in the ANKH signaling pathway, suggesting that CPPD crystal deposition can occur via multiple molecular pathways that may or may not intersect.11,12 The mechanism in which OPG mutations lead to CPPD crystal deposition is less understood, with a possible role for altered osteoclastogenesis in subchondral bone as a major contributor for degenerative joint disease.12 CCAL1 subtype familial CPPD crystal deposition disease generally presents with the onset of chondrocalcinosis well before the development of significant structural joint disease, whereas CCAL2 subtype cases demonstrate a simultaneous onset of generalized degenerative disease and chondrocalcinosis.12
Associated Diseases
A bevy of medical conditions have been reported in varying degrees of association with CPPD crystal deposition disease, with the strongest evidence related to its association with hyperparathyroidism, hemochromatosis, hypophosphatasia, and hypomagnesemia (including Bartter and Gitelman syndromes).
Classic musculoskeletal manifestations of hyperparathyroidism are well-known, including osteitis fibrosa cystica, salt-and-pepper degranulation of the calvarium, distal tapering of the clavicles, subperiosteal resorption, and brown tumors.13 With regard to hyperparathyroidism, it has been postulated that the proteoglycans that inhibit CPPD crystallization might be overwhelmed by systemic hypercalcemia and that altered cartilage metabolism in these patients promotes abnormally high enzymatic activity whereby calcium and pyrophosphate-containing material accumulate in the joints.13 A pseudogout attack after parathyroid surgery may be triggered by an abrupt decrease in serum calcium concentration in synovial fluid, making CPPD crystals more soluble so that they are shed into the synovial space.14,15
Hemochromatosis, a relatively common genetic disorder of iron metabolism with variable penetrance, has a long established association with CPPD crystal deposition disease,16 with 20-30% of patients with hereditary hemochromatosis shown to have CPPD crystal deposition disease.17 End-organ damage is secondary to increased intestinal absorption of iron and decreased hepcidin levels resulting in iron deposition in tissues throughout the body.16 With regard to the association of hemochromatosis with CPPD crystal deposition disease, both disease processes may share alterations in signaling pathways implicated in bone metabolism (e.g., alterations in osteoblast and osteoclast activity), suggesting some mechanistic overlap.18,19
Hypophosphatasia is a rare heterogeneous inborn error of bone metabolism caused by mutations in the ALPL gene encoding the tissue-nonspecific alkaline phosphatase isoenzyme (TNAP).20 Inorganic phosphate (PPi) is one of the physiologic substrates of TNAP, which accumulates in the setting of TNAP deficiency.21 Excess PPi supports the deposition of pyrophosphate and calcium in a crystallized form as CPPD crystals.20 CPPD crystal deposition is highly associated with hypophosphatasia, with one case series demonstrating an association of 71%.22
Bartter and Gitelman syndromes are two distinct hereditary disorders resulting in defects in renal tubular concentration of sodium, potassium, and chloride23 with resultant hypokalemia and metabolic alkalosis.24 These two disorders are also associated with CPPD crystal deposition disease. Hypomagnesemia is a hallmark of Gitelman syndrome and variably associated with subtypes of Bartter syndrome.23,25 Magnesium is a cofactor of various pyrophosphatases, including alkaline phosphatase.26 Decreased alkaline phosphatase activity due to hypomagnesemia could theoretically result in high extracellular levels of inorganic phosphate (PPi), predisposing to CPPD crystal deposition.26 It is thought that the classic association between Bartter syndrome and CPPD crystal deposition may have significant overlap with features of Gitelman syndrome, as no cases of Bartter syndrome without hypomagnesemia have been associated with CPPD crystal deposition disease.24
Imaging-Pathologic Correlation
Chondrocalcinosis:
Chondrocalcinosis is the hallmark feature of CPPD crystal deposition disease, whereby these crystals are deposited in hyaline cartilage or fibrocartilage, or both. Chondrocalcinosis is manifest by radiodense regions in the cartilage that are visible with conventional radiography and CT, and by foci of low signal intensity on MR images. Chondrocalcinosis involving fibrocartilage is most commonly seen in the menisci of the knee, symphysis pubis, triangular fibrocartilage of the wrist (Figures 3 and 4), annulus fibrosus of the intervertebral disc, acetabular labrum, and glenoid labrum. Hyaline cartilage calcification is most frequently seen in the knee, elbow, wrist, hip, and glenohumeral joints.1,27 Fibrocartilaginous calcifications appear as thick, shaggy, irregular radiodense areas, particularly within the central aspect of the joint. Hyaline cartilaginous deposits may be thin, linear, curvilinear, or punctate and are separate from and parallel to the subchondral bone plate.27
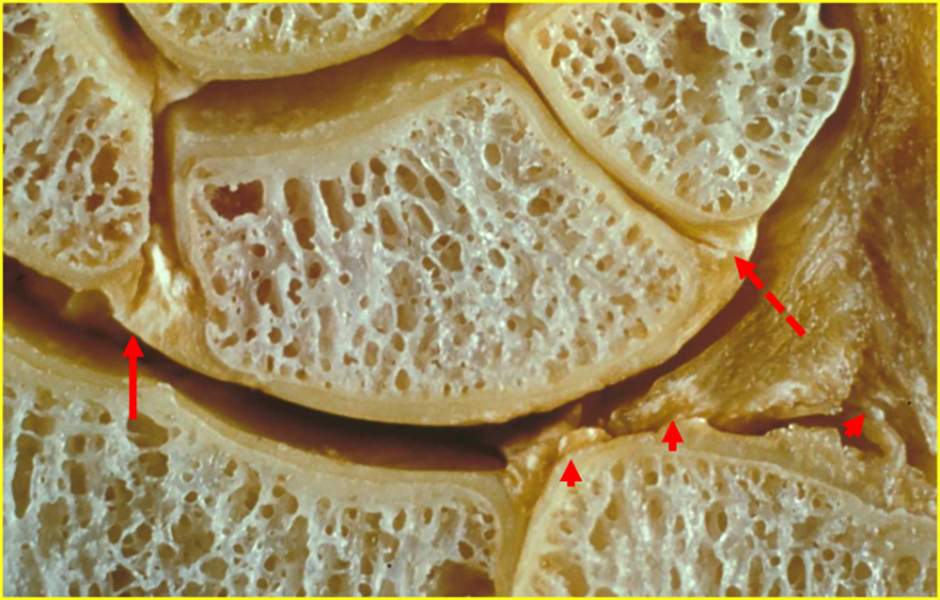
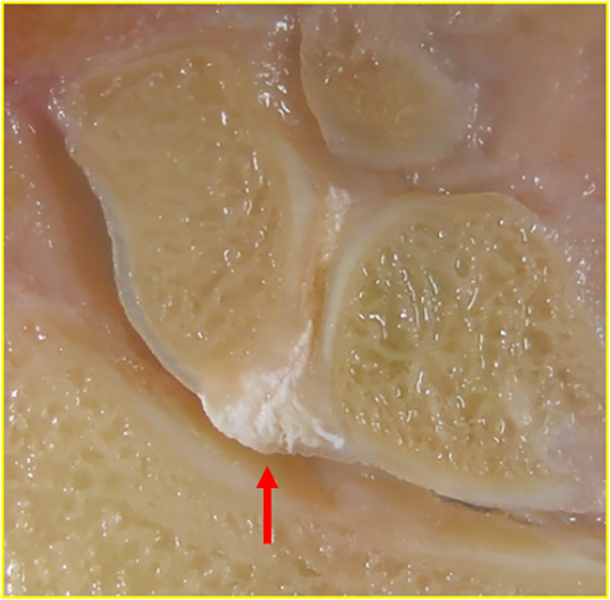
Figure 3. Chondrocalcinosis within the hand and wrist. Cadaveric coronal section through the wrist (3a) demonstrates CPPD crystal deposits in the scapholunate (red arrow) and lunotriquetral (dashed red arrow) interosseous ligaments, as well as in the torn triangular fibrocartilage (short red arrows). Coronal section through the wrist in a different cadaver demonstrates CPPD crystal deposits in the scapholunate interosseous ligament (red arrow).
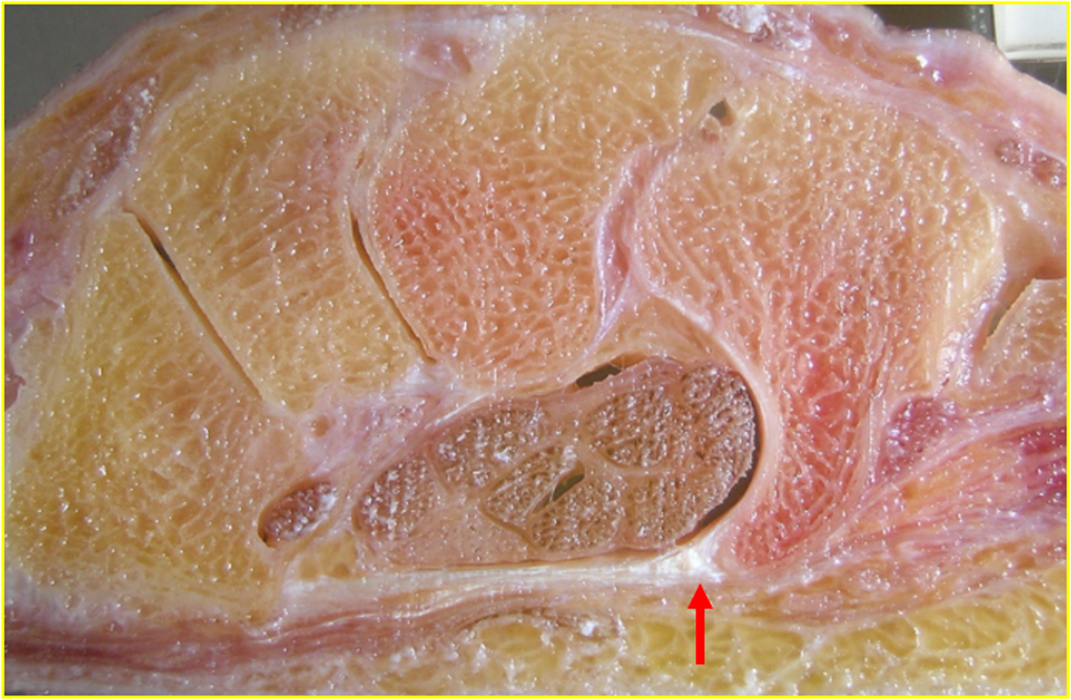
Figure 4. Cadaveric axial section through the wrist demonstrates CPPD crystal deposition at the hamate attachment of the transverse carpal ligament (red arrow).
Synovial/Capsular Calcification:
Calcification within the synovial membrane is a common feature of CPPD crystal deposition disease. Synovial deposits are most frequent in the wrist, particularly about the radiocarpal and distal radioulnar joints, knee, and metacarpophalangeal and metatarsophalangeal joints.1 Such deposits may mimic idiopathic synovial chondromatosis.1 CPPD crystal deposition within the joint capsule is most commonly observed in the elbow and metatarsophalangeal joints but is also observed in the metacarpophalangeal and glenohumeral joints.28
Tendon/Bursal/Ligament Calcification:
Calcification is most often observed in the Achilles, triceps, quadriceps, gastrocnemius, and supraspinatus tendons, as well as in the subacromial-subdeltoid bursa.28 These calcifications are typically more linear and elongated than those seen in calcium hydroxyapatite crystal deposition disease (Figure 5).
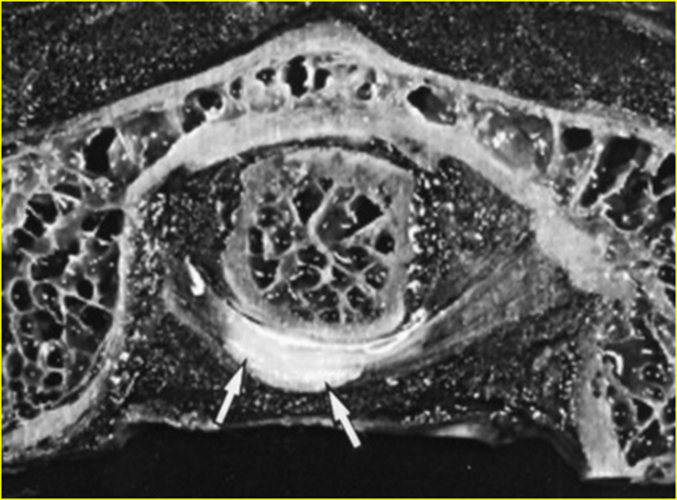
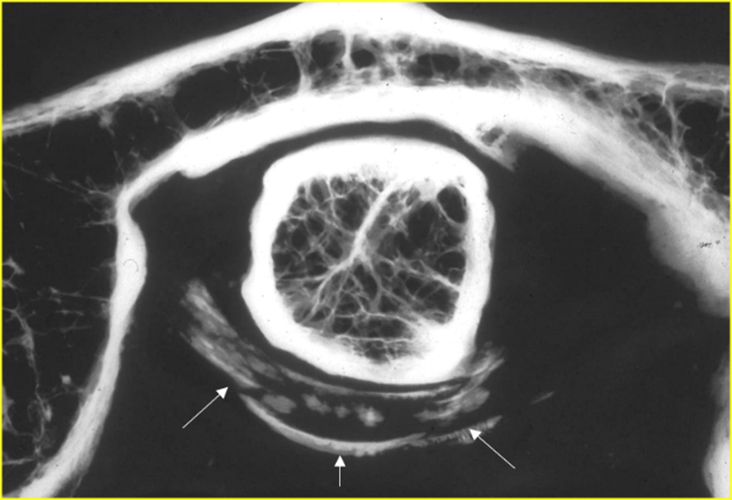
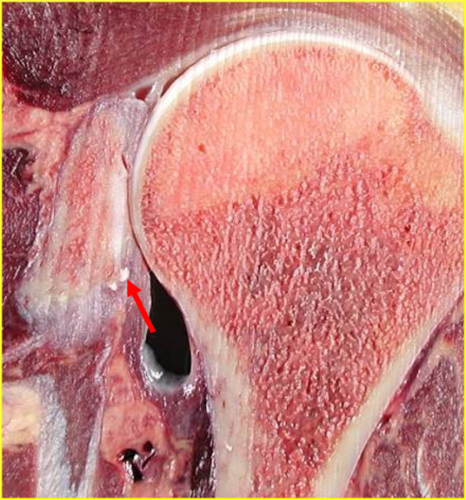

Figure 5. Ligament and tendon calcification in CPPD crystal deposition disease and calcium hydroxyapatite crystal deposition disease. Axial section (5a) and high resolution faxitron image (5b) in a cadaver centered at the atlantoaxial joint demonstrate curvilinear, elongated CPPD crystal deposits in the transverse ligament of the atlas (white arrows). The morphology of these deposits is in contradistinction to the round calcium hydroxyapatite crystal deposits in the tendon of the long head of the triceps muscle and in the supraspinatus tendon in cadaveric coronal sections through the shoulder (red arrows, 5c and 5d, respectively).
Soft Tissue Calcification (Tophaceous Pseudogout):
Tophaceous pseudogout is a term reserved for tumor-like or mass-like deposition of CPPD crystals within the soft tissues, sometimes distant from articular and periarticular structures.29 Imaging characteristics are nonspecific, with the differential diagnosis including such entities as tophaceous gout, idiopathic or secondary tumoral calcinosis, and benign or malignant neoplasms.29,30
Patients with tophaceous pseudogout may not show other stigmata of CPPD crystal deposition disease (e.g., chondrocalcinosis or pyrophosphate arthropathy). Soft tissue sampling yielding weakly positive birefringent crystals with polarized microscopy is pathognomonic for tophaceous pseudogout, as malignant or nonmalignant cartilaginous neoplasms are not associated with this phenomenon.29,30
The temporomandibular joint is the most common site of tophaceous pseudogout, followed by the hand, foot, wrist (Figure 6), cervical spine, and hip.29 Lower extremity involvement can be seen about the ankle30 and knee (Figure 7) as well.



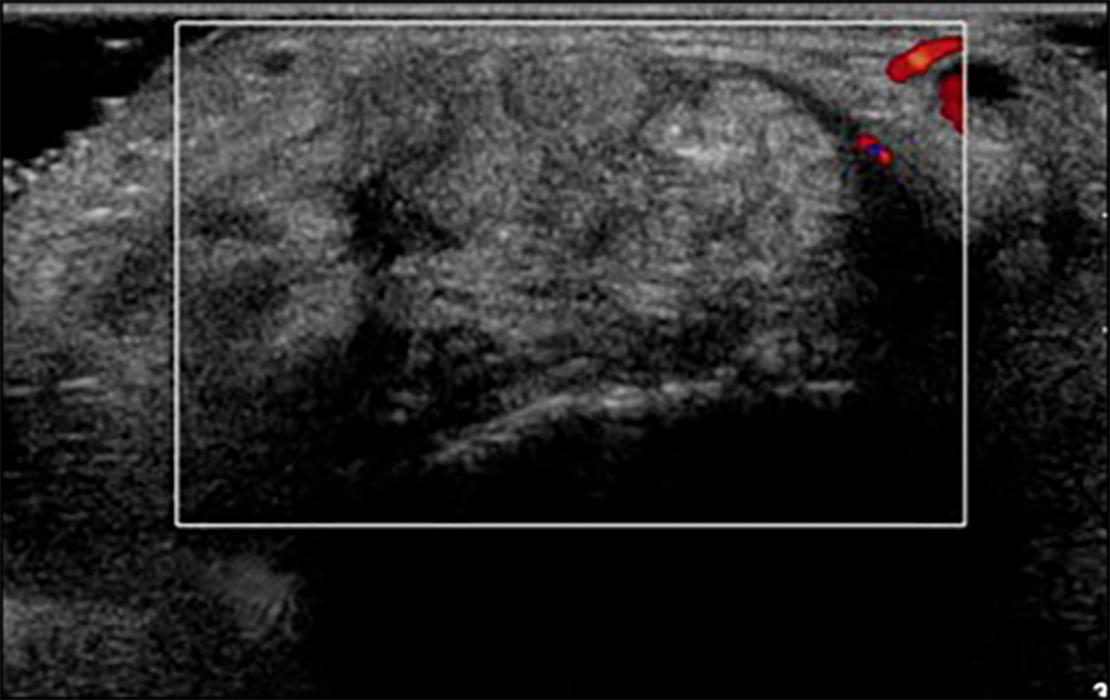
Figure 6. Tophaceous pseudogout. T1 weighted sagittal (6a) and T2 fat-saturated sagittal (6b) MR images demonstrate a dorsal tissue mass demonstrating low T1 and heterogenous T2 signal intensity (red arrows). Note enhancement of the mass and adjacent soft tissues with fat-suppressed T1-weighted postcontrast imaging (6c, red arrows). Ultrasonography (6d) shows peripheral doppler flow. Biopsy confirmed CPPD crystal deposition disease. (Case, courtesy of Youngwhan Lee, M.D.)
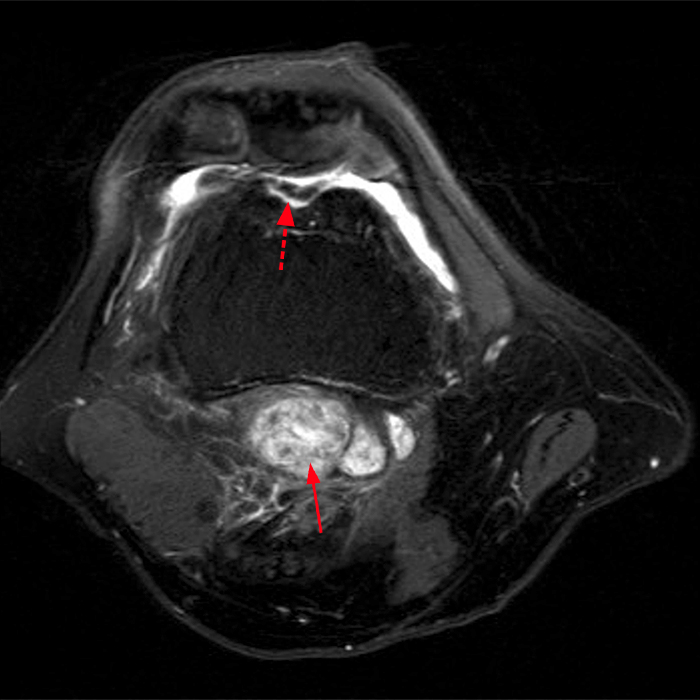
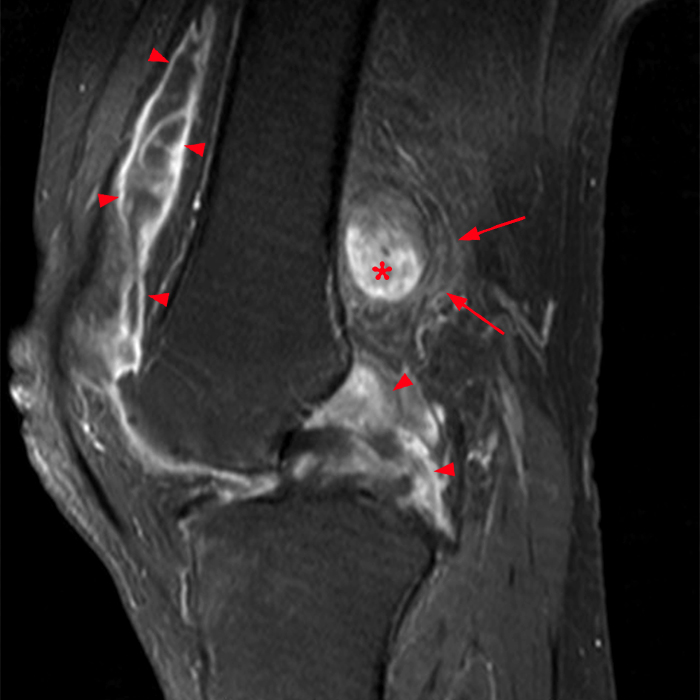
Figure 7. Tophaceous pseudogout. Fat-suppressed T2-weighted axial MR image (7a) demonstrates a multilobulated heterogeneously hyperintense soft tissue mass within the retrofemoral soft tissues (arrow) as well as full-thickness cartilage loss in the trochlea (dashed arrow). Fat-suppressed T1-weighted postcontrast sagittal image (7b) demonstrates enhancement of this mass (asterisk) and mild peripheral soft tissue enhancement (arrows) as well as synovial enhancement throughout the joint (arrowheads). Biopsy of this soft tissue mass confirmed CPPD crystal deposition (tophaceous pseudogout). (Case, courtesy of Brady Huang, M.D.)
Structural Joint Damage (Pyrophosphate Arthropathy):
The structural joint changes associated with CPPD crystal deposition disease are both common and characteristic and may appear without adjacent or distant articular calcification. Pyrophosphate arthropathy is most frequent in the knee, wrist, and metacarpophalangeal joints.28 Distribution is usually bilateral, although symmetric changes may not be present. Pyrophosphate arthropathy is similar to osteoarthrosis with regard to joint space narrowing and subchondral bone sclerosis and cyst formation; however, it differs in five respects:
- Unusual articular distribution: Although pyrophosphate arthropathy is seen in weight-bearing joints, such as the knee and hip, it is also apparent in sites that are less commonly involved in degenerative joint disease, such as the wrist, elbow, and glenohumeral joint.28
- Unusual intraarticular distribution: The distribution of pyrophosphate arthropathy in certain joints is characteristic.1,28 Isolated or significant involvement of the radiocarpal, triscaphe, patellofemoral, and talocalcaneonavicular joints may signify CPPD crystal deposition disease.
- Prominent subchondral cyst formation: In contradistinction to subchondral cystic change encountered with osteoarthrosis, the cysts associated with pyrophosphate arthropathy are numerous and may reach considerable size.28
- Destructive bone changes that are severe and progressive: Pyrophosphate arthropathy may be associated with extensive and rapid subchondral bone collapse and fragmentation, with the appearance of single or multiple intraarticular bodies simulating neuropathic osteoarthropathy.1,28
- Variable osteophyte formation: Large, irregular bony excrescences have been noted in some patients with pyrophosphate arthropathy, whereas joint space narrowing and bone sclerosis and fragmentation have been unaccompanied by osteophyte formation in others.28
Specific Sites of Involvement
Wrist:
Calcification in the wrist is observed most commonly in the triangular fibrocartilage;31,32 hyaline cartilage of the radiocarpal, midcarpal, and common carpometacarpal joints; synovium; and ligamentous structures, particularly the scapholunate and lunotriquetral interosseous ligamentous complexes.31,32 Carpal malalignment with scapholunate diastasis can occur, with disruption of the intervening interosseous ligament, as well as other intrinsic and extrinsic ligaments of the wrist31 (Figure 8).
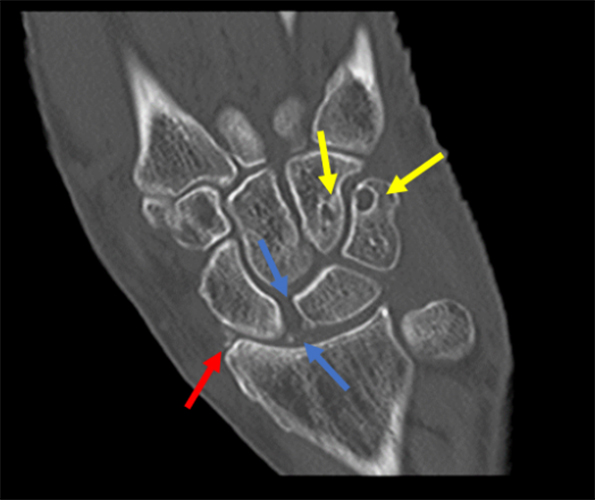
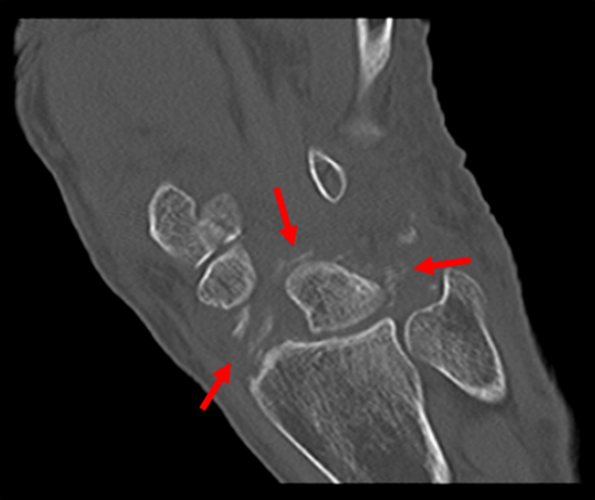

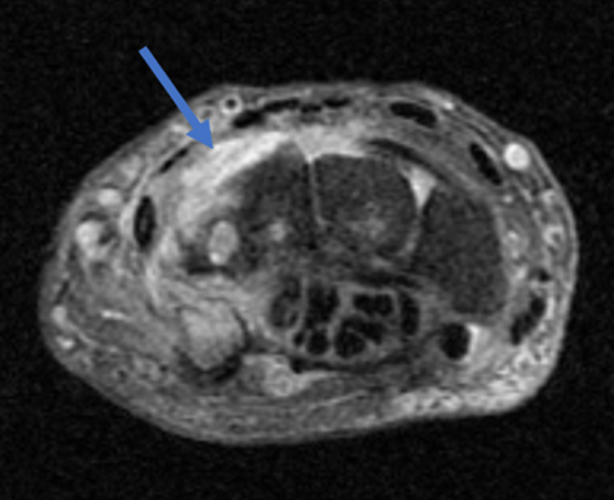
Figure 8. Pyrophosphate arthropathy in the wrist. Coronal CT images (8a, 8b), with 8b slightly volar to 8a, confirm widespread calcification of cartilage, synovial membrane, and volar extrinsic and intrinsic ligaments (red arrows in 8a and 8b). Note the widening of the scapholunate interosseous space with scapholunate ligament calcification (blue arrows). There are multiple subchondral cysts in several carpal bones, especially the triquetrum and the hamate (yellow arrows). T1-weighted coronal (8c) and fat-suppressed T2-weighted axial (8d) MR images confirm scapholunate dissociation (red arrow) and dorsal synovitis (blue arrow). (Case, courtesy of Brady Huang, M.D.)
The wrist arthropathy of CPPD crystal deposition disease demonstrates a predilection for the radiocarpal compartment.1,28 Joint space narrowing, subchondral bone sclerosis, and subchondral cystic change are observed, especially in the radioscaphoid portion of the joint with enlargement and deepening of the scaphoid fossa in the distal articular surface of the radius. Progressive changes include widening of the scapholunate interosseous space, narrowing of the lunate-capitate space, and abnormal tilting of the lunate, findings simulating those that occur in cases of post-traumatic scapholunate advanced collapse (SLAC)27 (Figure 9). These changes are in contradistinction to osteoarthrosis, in which degenerative changes are more typically seen in a first ray distribution.
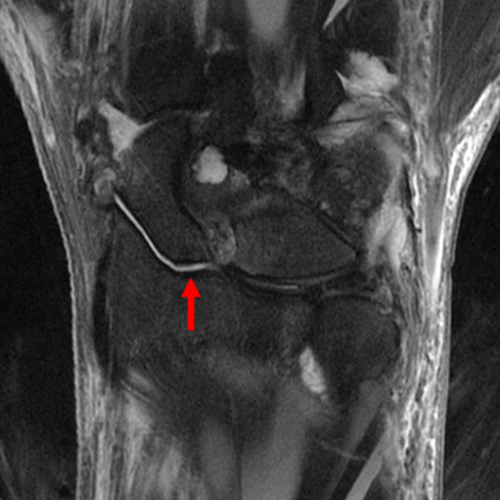
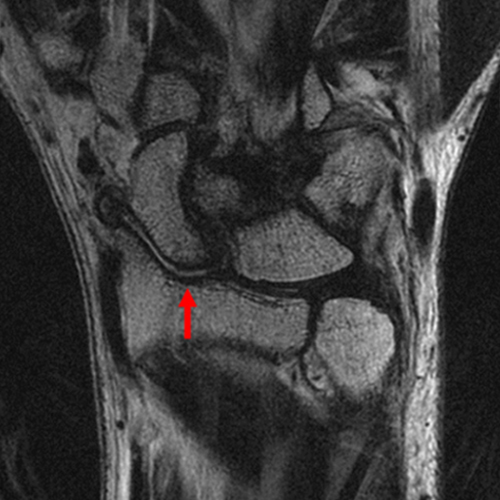
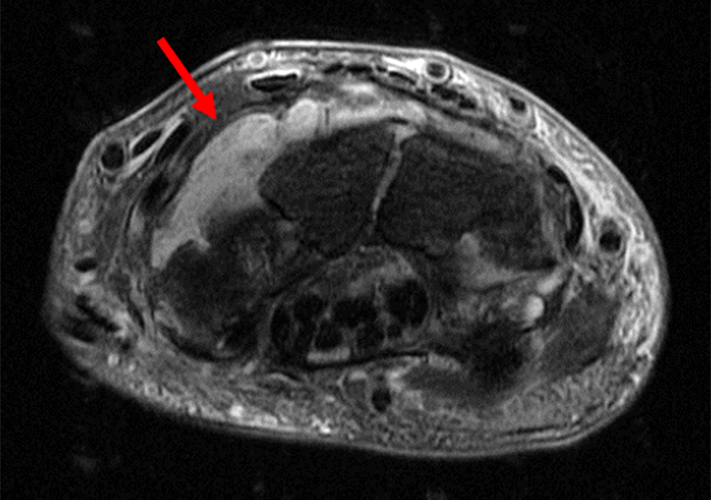
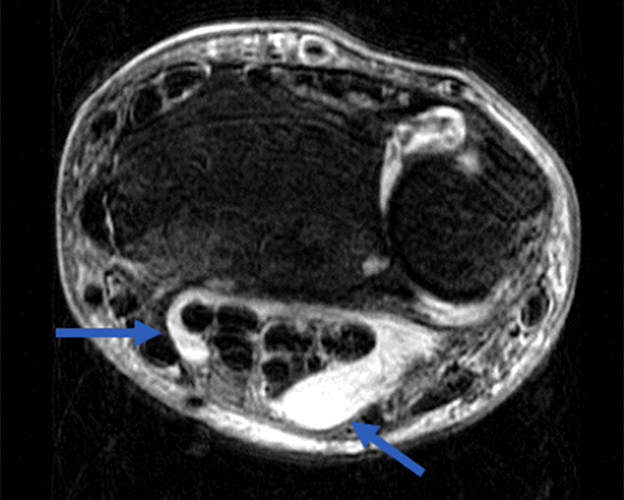
Figure 9. Pyrophosphate arthropathy in the wrist. Fat-suppressed T2-weighted coronal (9a) and proton density-weighted coronal (9b) MR images demonstrate severe radiocarpal joint abnormalities with deepening of the scaphoid fossa of the distal radius (red arrows) and scapholunate disassociation. There is proximal migration of the capitate, simulating the findings of post-traumatic scapholunate advanced collapse. Fat-suppressed T2-weighted axial MR images (9c and 9d), with 9d proximal to 9c, demonstrate dorsal carpal synovitis (red arrow) and radial and ulnar bursitis (blue arrows). (Case, courtesy of Brady Huang, M.D.)
Hand:
The metacarpophalangeal joints are frequently affected in CPPD crystal deposition disease, most commonly the second and third metacarpophalangeal joints,28,31 often in a bilateral distribution. Radiographic abnormalities in this location include cartilaginous, capsular, and synovial calcifications, as well as pyrophosphate arthropathy (Figure 10). This is in contradistinction to osteoarthrosis, in which degenerative changes predominate in the interphalangeal joints. Absence of bone erosions differentiates CPPD crystal deposition disease from rheumatoid arthritis. Hemochromatosis can demonstrate similar findings in the second and third metacarpophalangeal joints; however, involvement of the first, fourth and fifth metacarpophalangeal joints and hook-like osteophytes on the radial aspect of the metacarpal heads are more common in hemochromatosis33(Figure 11).


Figure 10. Pyrophosphate arthropathy in the hand and wrist. Frontal radiographs of the left (10a) and right (10b) hands demonstrate bilateral joint abnormalities. Some of these, such as the change in several of the interphalangeal joints, are identical to those of osteoarthrosis, whereas other findings suggest pyrophosphate arthropathy. Note chondrocalcinosis within the triangular fibrocartilage of both wrists (red arrows), bilateral scapholunate dissociation with proximal migration of the capitate (blue arrows), severe radiocarpal joint space narrowing with deepening of the scaphoid fossa (yellow arrows), and scattered metacarpophalangeal and proximal interphalangeal joint capsular calcification (orange arrows). Note cystic change of multiple bilateral carpal bones, particularly the hamate and triquetrum (purple arrows). The changes at the first carpometacarpal joints bilaterally resemble those seen in osteoarthrosis. Incidental note is made of a nonspecific, nonaggressive radiodense lesion in the proximal phalanx of the right thumb (green arrow). (Case, courtesy of Brady Huang, M.D.)

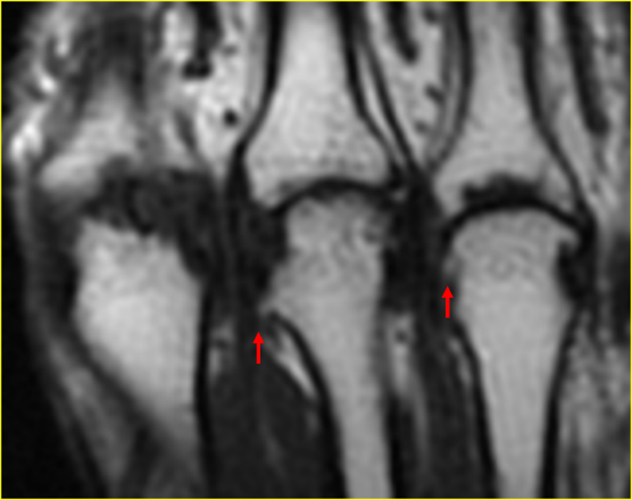
Figure 11. Hemochromatosis in the hand. Coned-down frontal radiograph of the hand (11a) demonstrates severe joint space narrowing of the second through fifth metacarpophalangeal joints with radially located hook-like osteophytes of the metacarpal heads (red arrows) and capsular calcification at the ulnar aspect of the fourth metacarpophalangeal joint (dashed red arrow). Involvement of all of the metacarpophalangeal joints and hook-like osteophytes such as these are more commonly seen in hemochromatosis than in CPPD crystal deposition disease. T1-weighted coronal MR image of the hand in a different patient with hemochromatosis (11b) demonstrates severe second through fourth metacarpophalangeal joint space narrowing with hook-like osteophytes on the radial aspect of some of the metacarpal heads (red narrows).
Knee:
The knee is the most commonly affected joint in CPPD crystal deposition disease.28 Chondrocalcinosis and synovial calcification may be seen alongside tendinous and ligamentous deposits in the quadriceps, gastrocnemius, and cruciate and collateral ligaments34(Figure 12). Chondrocalcinosis of the menisci and hyaline cartilage with gastrocnemius tendinous calcification is a characteristic appearance1,35(Figure 13).
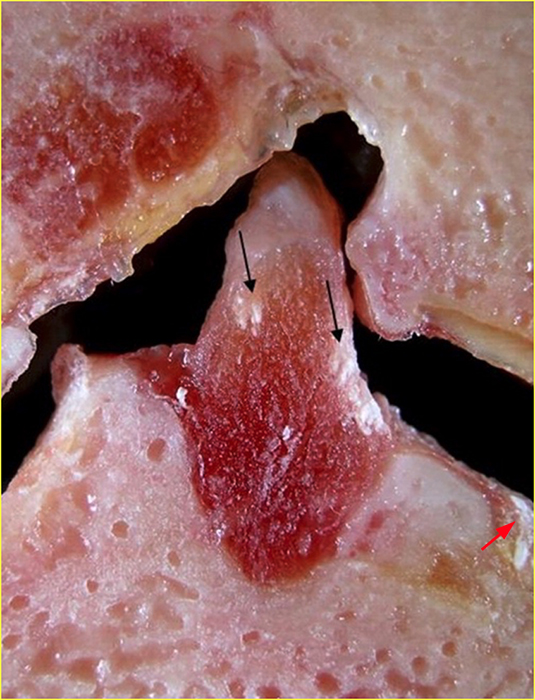
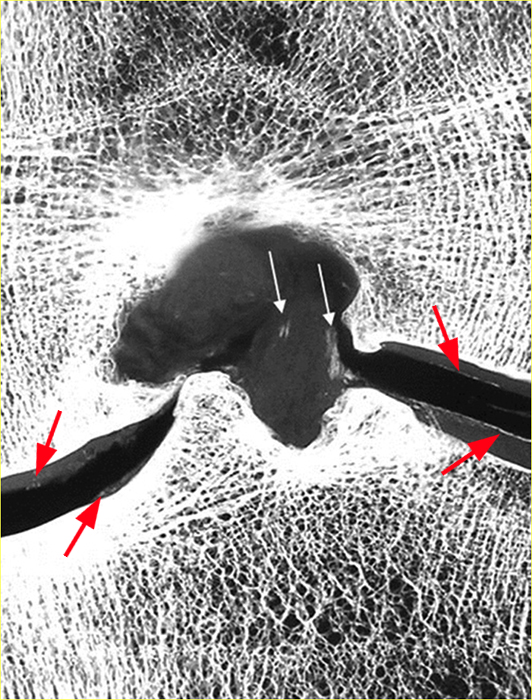
Figure 12. Ligamentous CPPD crystal deposition in the knee. Cadaveric coronal section (12a) and high resolution faxitron image of this section (12b) demonstrate CPPD crystal deposition within the anterior cruciate ligament (black and white arrows, respectively). Note medial and lateral femorotibial compartment hyaline cartilage chondrocalcinosis (red arrows).
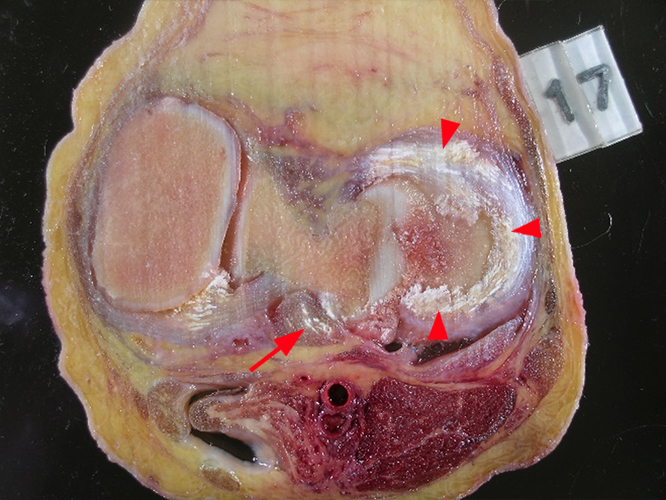
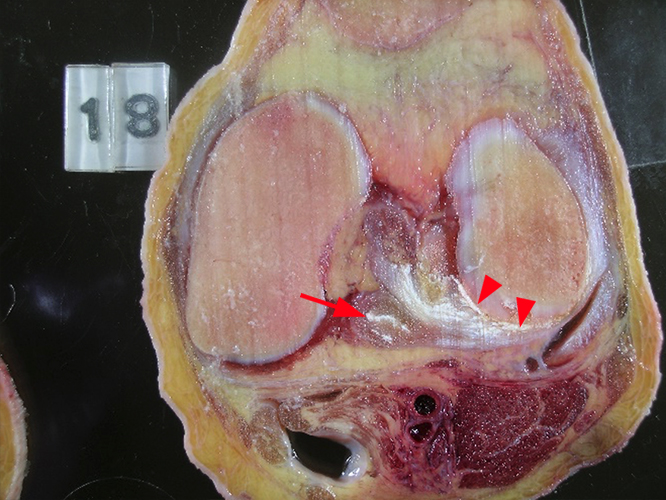
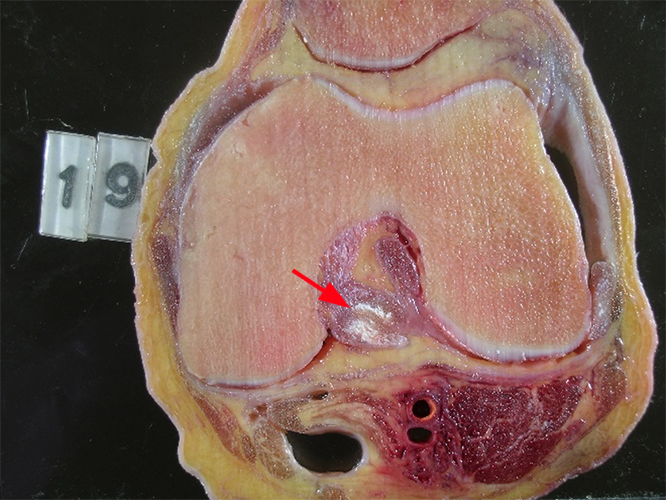
Figure 13. CPPD crystal deposition in the knee. Sequential axial cadaveric sections from distal to proximal (13 a-c) demonstrate chondrocalcinosis within the lateral meniscus (arrowheads) and the posterior cruciate ligament (arrows).
Pyrophosphate arthropathy predominates in the medial femorotibial compartment, with the patellofemoral compartment being the second most commonly involved compartment.36 Isolated or severe patellofemoral or lateral femorotibial compartment alterations, especially in men, are characteristic of CPPD crystal deposition disease28 (Figures 14 and 15).

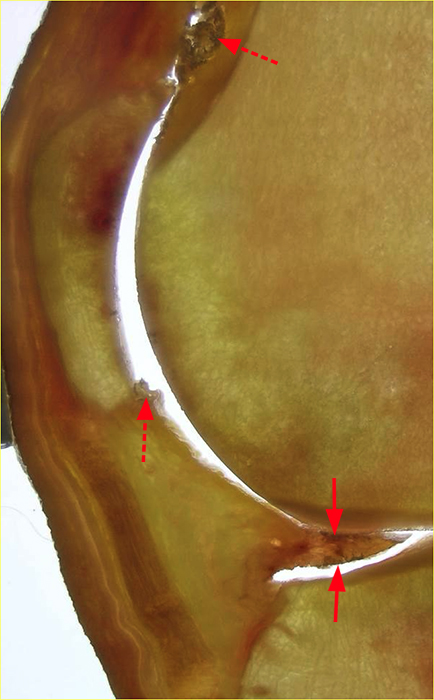
Figure 14. Pyrophosphate arthropathy in the knee. Cadaveric sagittal sections of the knee (14a and 14b) demonstrate severe patellofemoral compartment changes with high grade to complete loss of the articular cartilage in the patella and trochlea and an exaggerated concavity of the subchondral bone in the patella (arrowheads, 14a). There is chondrocalcinosis in the anterior horn of the meniscus ( arrows, 14b) and possibly in the synovium covering the infrapatellar fat pad and prefemoral fat (dashed red arrows, 14a and 14b). Severe patellofemoral compartment changes in the absence of significant abnormalities of the femorotibial compartments, especially in a man, are suggestive of the diagnosis of CPPD crystal deposition disease.
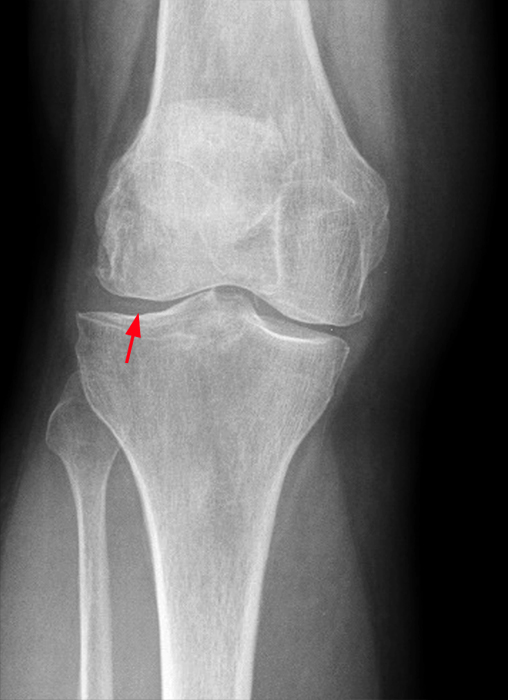

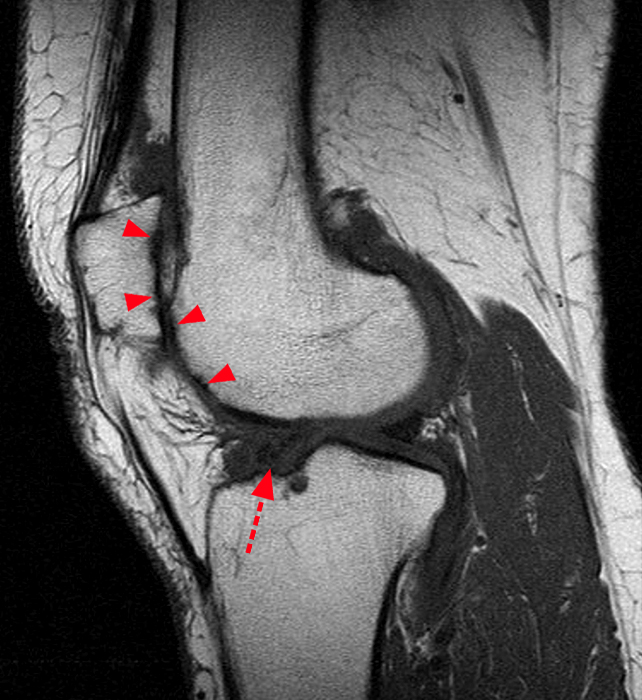

Figure 15. Pyrophosphate arthropathy in the knee. Frontal (15a) and lateral (15b) radiographs demonstrate lateral femorotibial compartment chondrocalcinosis (red arrow) and isolated severe joint space narrowing in the patellofemoral compartment with subtle erosion of the anterior femoral surface just above the trochlea (blue arrow). T1-weighted sagittal (15c) and short tau inversion recovery (STIR) sagittal (15d) MR images demonstrate full-thickness patellofemoral compartment cartilage loss with accompanying subchondral reactive marrow edema (arrowheads), as well as abnormalities of the lateral meniscus (dashed red arrows). (Case, courtesy of Brady Huang, M.D.)
Hip:
Fibrocartilaginous calcification of the acetabular labrum and hyaline cartilage calcification can be observed in CPPD crystal deposition disease28 (Figure 16). Joint space narrowing may be confined to the superolateral aspect of the articulation or be seen throughout the entire joint, simulating osteoarthrosis and rheumatoid arthritis, respectively. Prominent subchondral cyst formation may be present. Rapid and extensive destruction of the femoral head and acetabulum may occur as well, simulating neuropathic osteoarthropathy (Figure 17).1
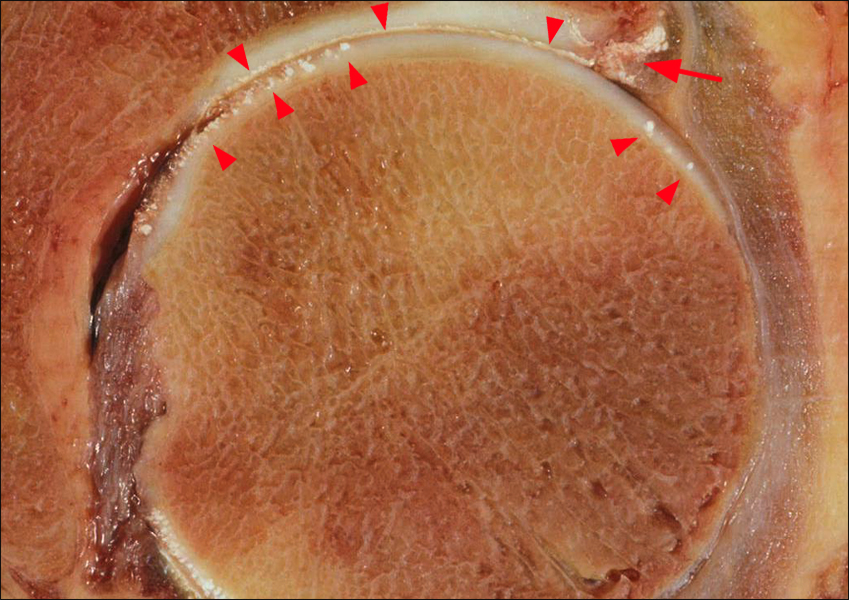
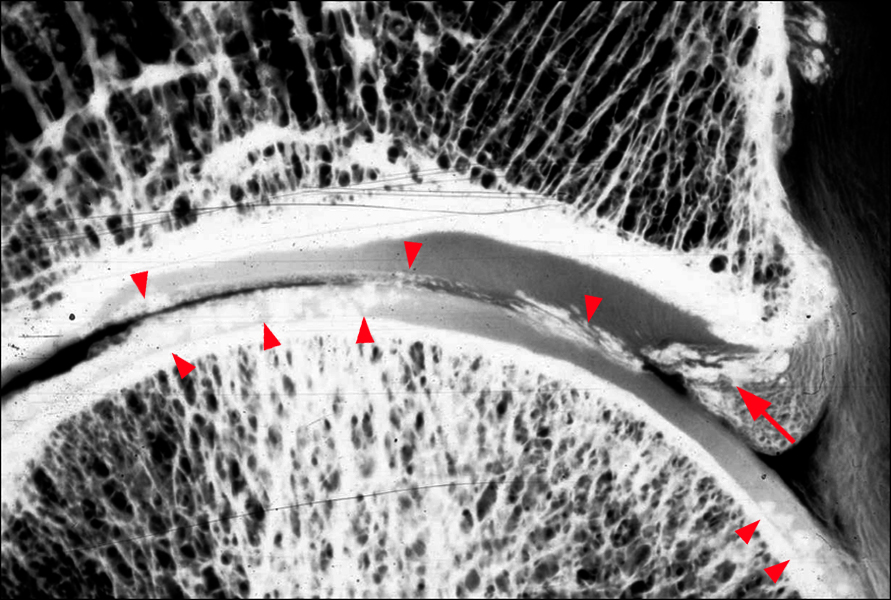
Figure 16. Chondrocalcinosis in the hip. Cadaveric coronal section (16a) and high resolution faxitron image of this section (16b) demonstrate chondrocalcinosis within the hyaline cartilage (arrowheads) and the acetabular labrum (red arrows).
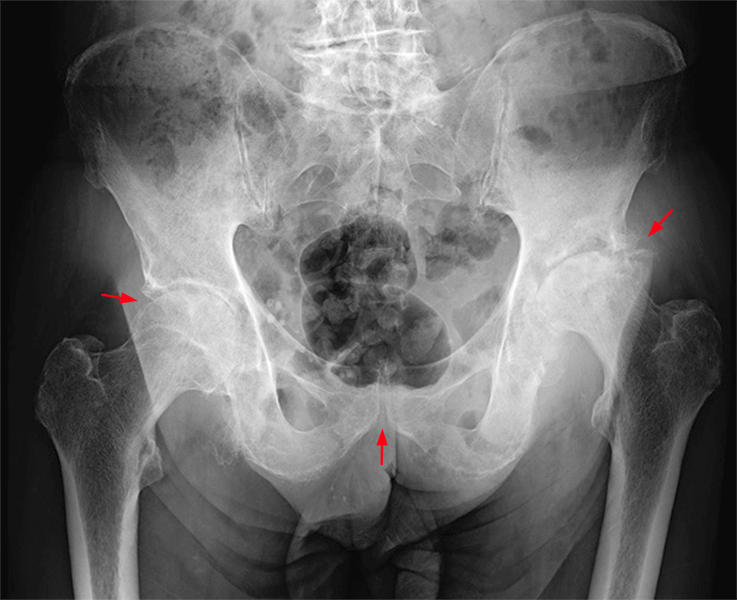
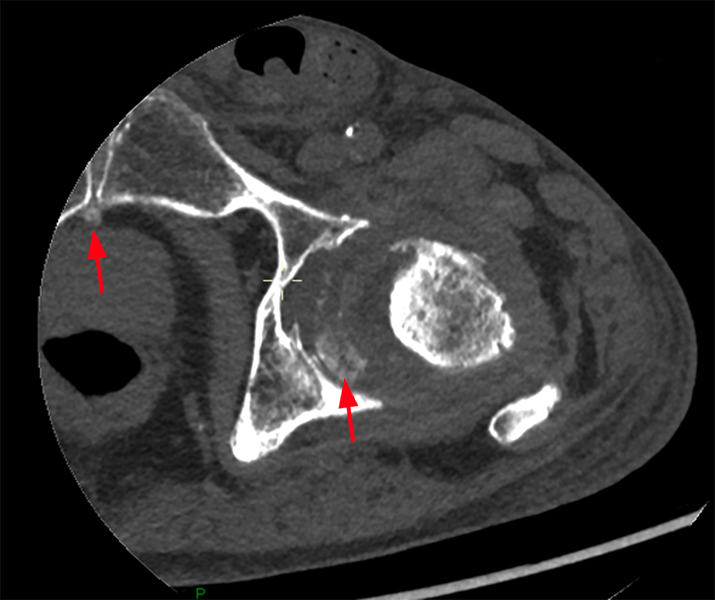

Figure 17. Pyrophosphate arthropathy in the hip. Frontal radiograph (17a) shows chondrocalcinosis in both hip joints and in the symphysis pubis (red arrows). Axial (17b) and coronal (17c) CT images of the left hip confirm the presence of chondrocalcinosis within the hip joint and symphysis pubis (red arrows). There appears to be calcific debris in the hip as well. Note that the abnormalities of the hip are far too severe for osteoarthrosis alone, including severe superolateral joint space narrowing and subchondral bony sclerosis (blue arrow). Such changes often resemble neuropathic osteoarthropathy, and they may occur rapidly. (Case, courtesy of Rodrigo Aguiar, M.D.)
Spine:
CPPD crystal deposition disease is accompanied by intervertebral disc calcification, with deposits initially appearing peripherally in the outer fibers of the annulus fibrosus.28 Deposits can be seen in other spinal tissues, including the ligamentum flavum, posterior longitudinal ligament, interspinous and supraspinous ligaments, and interspinous bursae.37,38
Intervertebral disc space narrowing is a common finding in CPPD crystal deposition disease, which may be widespread and associated with pronounced vertebral body sclerosis.37 Destructive changes in adjacent vertebral bodies may be present as well, simulating infection or neuropathic osteoarthropathy.37
At the atlantoaxial joint, CPPD crystal deposition is most typically seen in the posterior median atlantoaxial joint, causing inflammation about the odontoid process (so-called crowned dens syndrome)37,38,39 (Figure 18). The resulting mass may compress the spinal cord and predispose to dens fractures and atlantoaxial subluxation39 (Figure 19).
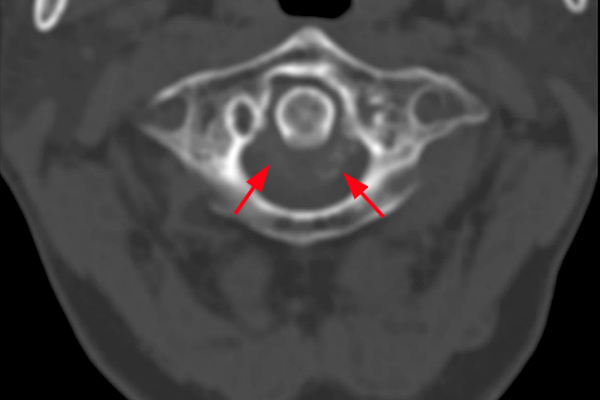
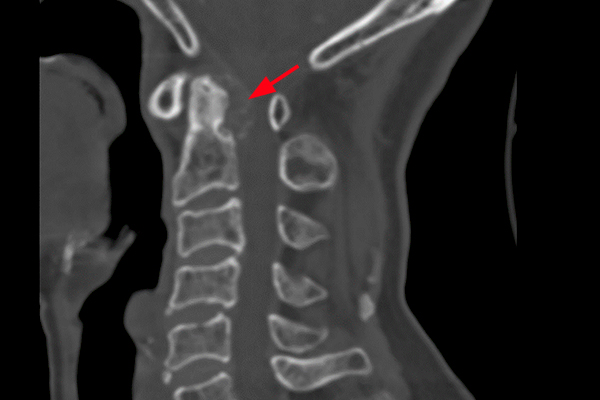


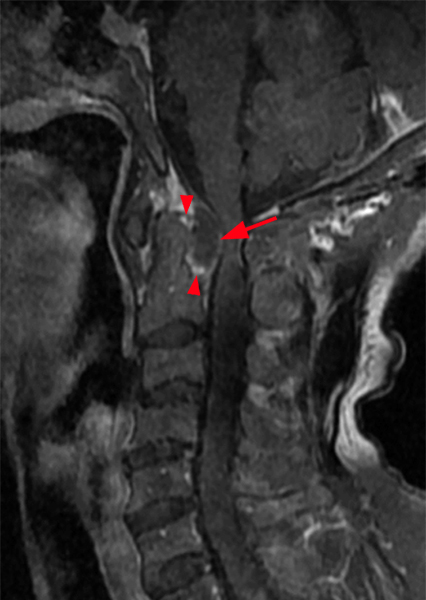
Figure 18. Crowned dens syndrome. Axial (18a) and sagittal (18b) CT images of the cervical spine demonstrate a calcified soft tissue mass located mainly posterior to the odontoid process, in the location of the posterior median atlantoaxial joint (red arrows). There is erosion of the posterior surface of the dens. Sagittal fat-suppressed T2-weighted (18c), T1=weighted (18d), and fat-suppressed T1-weighted postcontrast (18e) MR images demonstrate the synovial hypertrophy and calcification within this joint (arrows) as well as synovial enhancement following contrast administration (arrowheads). (Case, courtesy of Youngwhan Lee, M.D.)

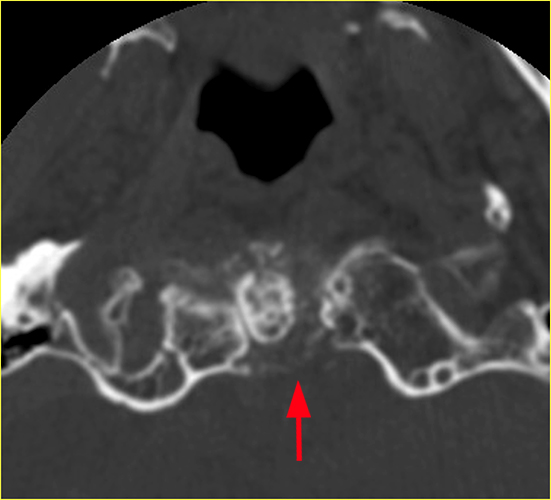
Figure 19. Crowned dens syndrome with type II odontoid process fracture. Sagittal (19a) and axial (19b) CT images of the cervical spine demonstrate a calcified soft tissue mass located mainly posterior to the odontoid process, in the location of the posterior median atlantoaxial joint (red arrows) with an accompanying fracture at the base of the odontoid process (blue arrow). Such fractures may occur with minor trauma, especially if the odontoid process has been eroded by the adjacent synovitis. Note, also the widespread changes throughout the cervical spine including disc space narrowing, irregular vertebral body surfaces, osteophytes, and minor subluxations.
Other sites:
The foot and ankle are less frequent sites of CPPD crystal deposition disease. As with the aforementioned sites of involvement, chondrocalcinosis can be observed without (Figure 20) or with (Figure 21) changes related to pyrophosphate arthropathy. Case reports in the literature have demonstrated pseudoneuropathic pseudogout in the midfoot40 and tophaceous pseudogout in the hindfoot.30
As noted previously, the temporomandibular joint is the most common site of tophaceous pseudogout.29,41 The sternoclavicular joint is an additional site of CPPD crystal deposition, with prevalence increasing with advancing age.42,43

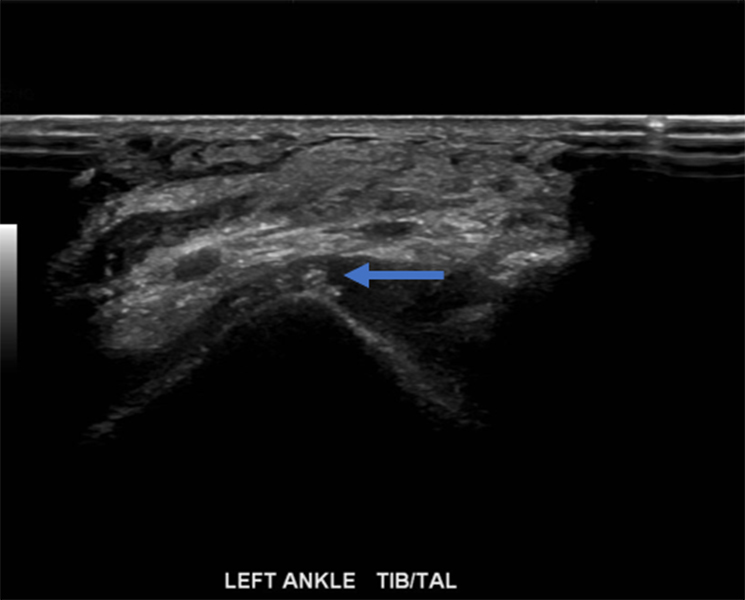
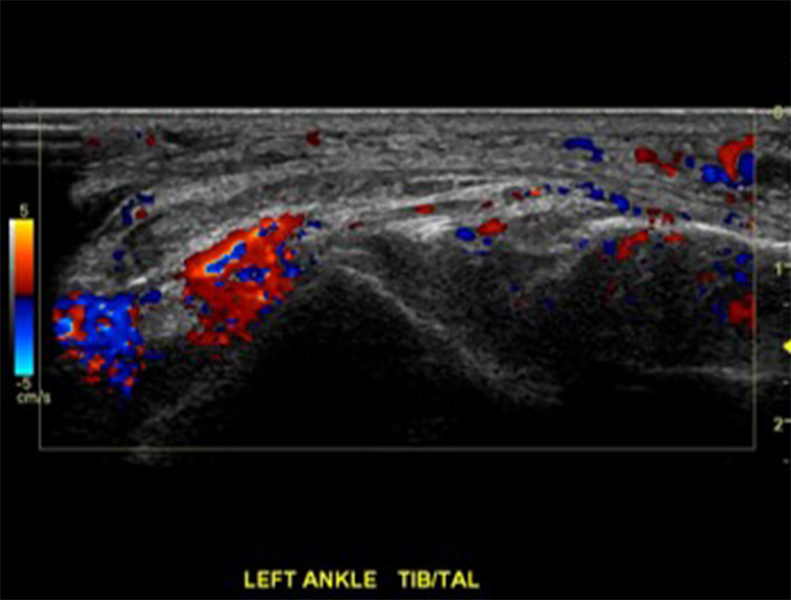
Figure 20. Chondrocalcinosis within the tibiotalar joint. Lateral radiograph (20a) of the ankle demonstrates chondrocalcinosis within the tibiotalar joint (red arrow). Greyscale ultrasonography (20b) demonstrates calcification within the tibiotalar joint (blue arrow). Doppler ultrasonography (20c) demonstrates associated synovitis. (Case, courtesy of Brady Huang, M.D.)


Figure 21. Pyrophosphate arthropathy in the ankle. Frontal radiograph (21a) demonstrates cartilage and synovial calcification (red arrows) and structural damage of the tibiotalar joint, with medial joint space narrowing and subchondral bone sclerosis (blue arrow). CT coronal image (21b) confirms the severe joint abnormalities (blue arrow) and better shows the synovial calcification in a lateral recess of the ankle (red arrow). (Case, courtesy of Kyung Jin Suh, M.D.)
Advanced Imaging Methods
CT:
With CT, many of the findings of CPPD crystal deposition disease that are seen on conventional radiographs, namely chondrocalcinosis, periarticular calcification, and soft tissue calcification, are visible with characteristic increased Hounsfield unit density. The advantages of CT versus conventional radiography are most apparent in the assessment of the spinal manifestations of this disease. Of note, dual energy CT has been shown to be less sensitive in the detection of CPPD crystals versus that of monosodium urate crystals44,45(Figure 22).
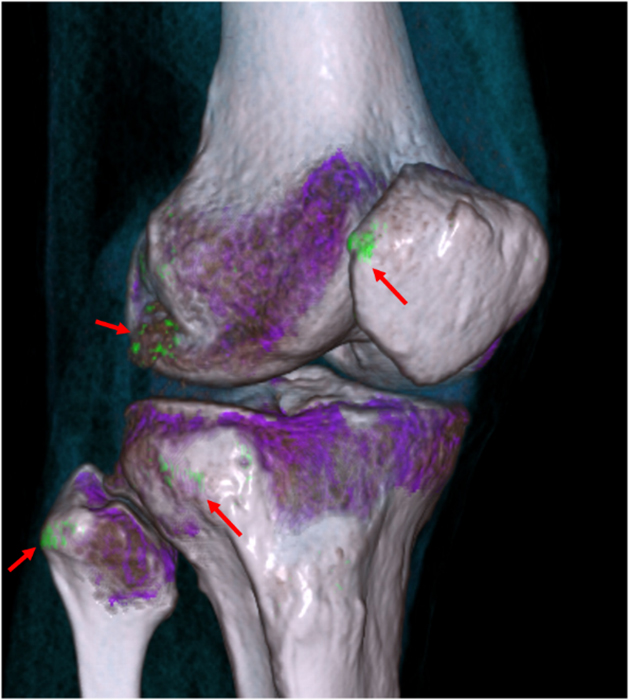
Figure 22. Monosodium urate crystal deposition (gout). Reconstructed dual energy 3D image of the knee demonstrates monosodium urate crystal deposition (green foci) at the lateral patellar facet, lateral femoral condyle, lateral tibial plateau, and fibular head (red arrows), the differentiation of which is made possible by the principle that material containing elements of higher atomic number (e.g., calcium) demonstrates higher attenuation at higher photon energies than material containing elements of lower atomic number (e.g., monosodium urate). (Case, courtesy of Diego Lessa, M.D.)
MR Imaging:
CPPD crystal deposition is less apparent with MR imaging when compared with conventional radiography or CT. Chondrocalcinosis may be manifest by areas of low signal within the articular cartilage, though MR imaging may severely underestimate the extent of such calcification when compared with radiographs.46 Additionally, certain sequence parameters may increase the signal intensity of fibrocartilaginous structures such as the knee menisci, worsening the sensitivity and specificity for MR detection of meniscal tears.47 More recent literature suggests a role for ultrashort time to echo (UTE) sequence imaging in the evaluation of CPPD crystal deposition in the knee.48
While MR imaging is not particularly sensitive or specific with regard to screening for CPPD crystal deposition, this modality’s excellent soft tissue contrast and display of intraarticular and periarticular structures provide a vital tool in the evaluation of pyrophosphate arthropathy and tophaceous pseudogout.
Ultrasonography:
Diagnostic musculoskeletal ultrasound allows identification of CPPD crystal deposits in peripheral joints and within the soft tissues.49 Such deposits are characterized by either thin hyperechogenic foci paralleling the joint surface or focal nodular hyperechogenic foci on greyscale ultrasonography.49 Doppler ultrasonography allows identification of synovitis in affected joints (Figures 6 and 20). Reports indicate that ultrasonography has high specificity and sensitivity for detection of chondrocalcinosis (greater than 90 and 80 percent, respectively45,49); however, it must be noted that the success of this technique is highly operator dependent.
Differential Diagnosis
Abnormal Calcification:
Abnormal intraarticular and periarticular calcification is characteristic of basic calcium phosphate crystal deposition disease, also designated calcium hydroxyapatite crystal deposition disease. This condition may occur on an idiopathic basis, as an inherited disorder, or as a complication of a number of underlying disorders, especially collagen vascular diseases, renal osteodystrophy, hyperparathyroidism, and hypervitaminosis D.50 In contradistinction to CPPD crystal deposition, basic calcium phosphate deposits often begin as poorly defined cloudlike areas of calcification, eventually becoming more sharply delineated.50 The most common site of calcification in this disorder is within the tendons of the rotator cuff, often at or near the footprint of the involved tendon (Figures 23 and 24). Although calcification of the rotator cuff tendons can also be seen in cases of CPPD crystal deposition disease, this is an infrequent site of involvement and the resulting calcifications are linear or curvilinear in appearance, sometimes extending over a long segment of the tendon.
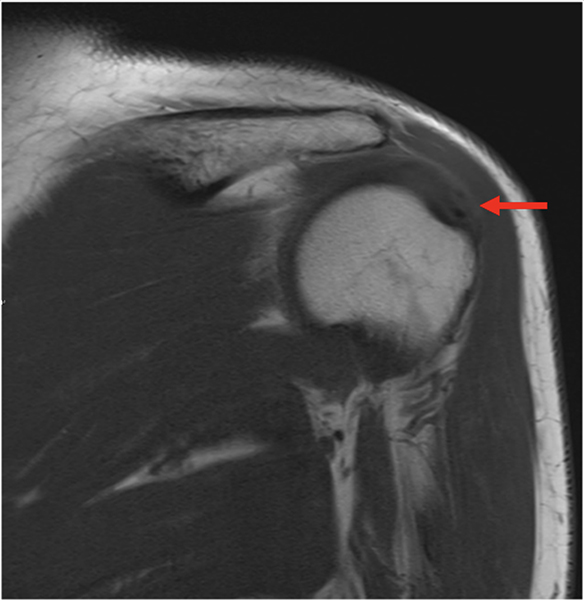
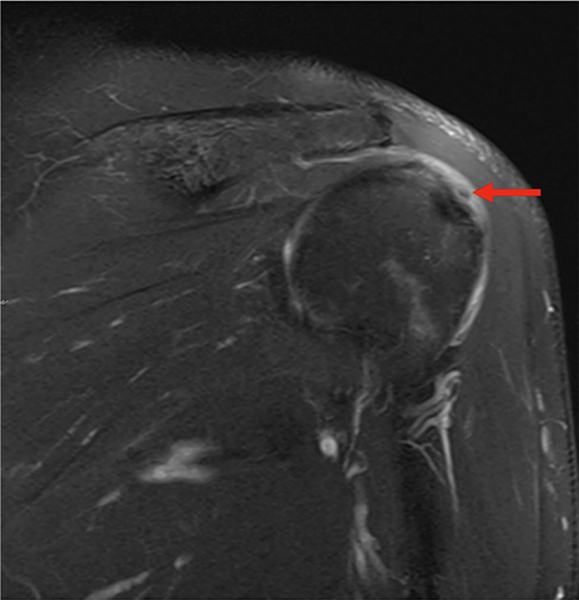
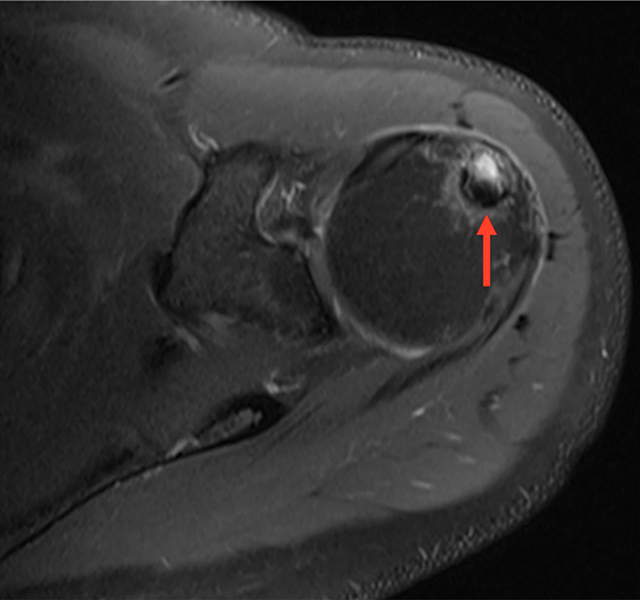

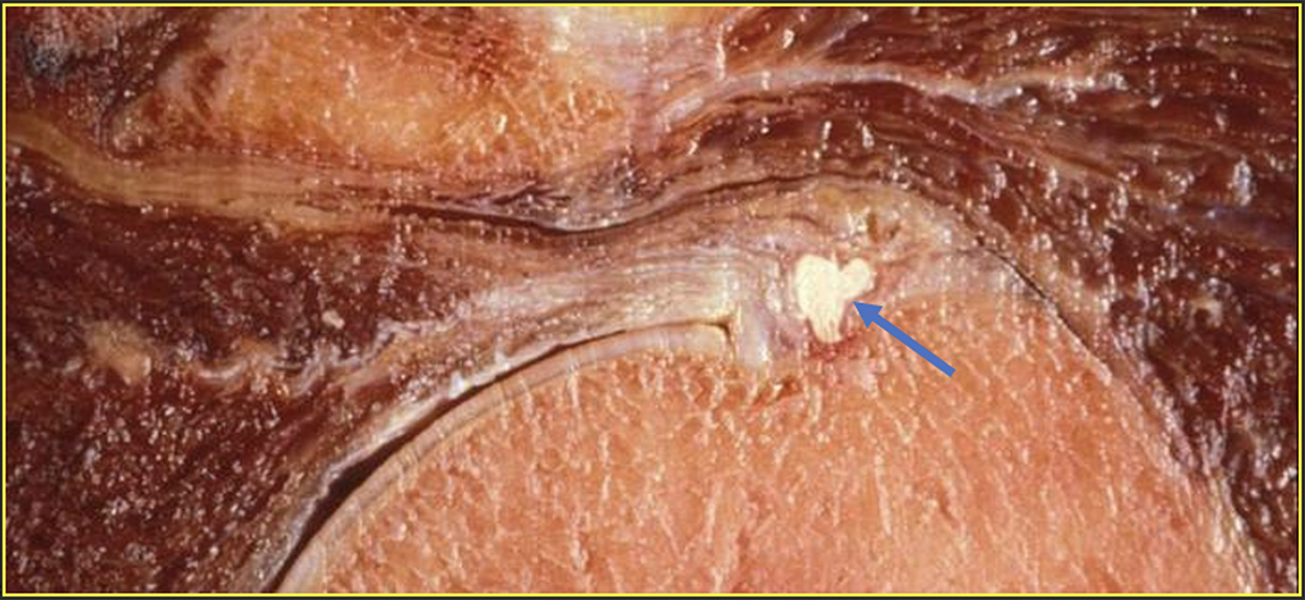
Figure 23. Basic calcium phosphate/hydroxyapatite crystal deposition at the shoulder. T1=weighted coronal (23a) and fluid-sensitive coronal (23b) MR images demonstrate a globular focus of low T1 and low T2 signal (red arrows) within the infraspinatus tendon at and near its footprint with accompanying bursal fluid. Fluid-sensitive axial MR image of the left shoulder (23c) in a different patient demonstrates intraosseous migration of similar appearing low-signal material into the humeral head (red arrow). CT coronal image (23d) of the left shoulder of the same patient as in figure 23c confirms the presence of amorphous calcification at and near the infraspinatus tendon footprint (red arrow). Intraosseous migration of calcific collections in the rotator cuff tendons, although uncommon, can be associated with any of these tendons but are most often seen when calcification occurs in the supraspinatus tendon. A similar phenomenon may occur at other anatomic sites independent of the shoulder. Cadaveric coronal section from an unrelated donor through the greater tuberosity (23e) demonstrates characteristic amorphous calcification of the supraspinatus tendon at and near its insertion with irregularity of the bone surface (blue arrow). (Case (a-d), courtesy of Diego Lessa, M.D.)


Figure 24. CPPD crystal deposition at the shoulder. High-resolution faxitron images of coronal sections in two cadavers (24a-b) following arthrography show CPPD crystal deposition within the supraspinatus and infraspinatus tendons (red arrows). Note the curvilinear, elongated character of these calcific deposits, in contradistinction to the round and globular basic calcium phosphate/calcium hydroxyapatite crystal deposits within the same tendons in figure 23.
Gout, a frequently encountered crystalline arthropathy, does not typically demonstrate chondrocalcinosis, although there are reports of the association of gout with CPPD crystal deposition.51 Additionally, calcification of monosodium urate deposits has been noted, especially in patients with chronic renal disease.27 Uric acid crystals are well-displayed with dual-energy CT scanning.45 Erosions are characteristic of gout and are not typical in cases of CPPD crystal deposition disease.
Tophaceous pseudogout can sometimes provide a diagnostic dilemma, necessitating differentiation from chondroid or other mineralized neoplasms. Tissue sampling may be required (Figure 25).
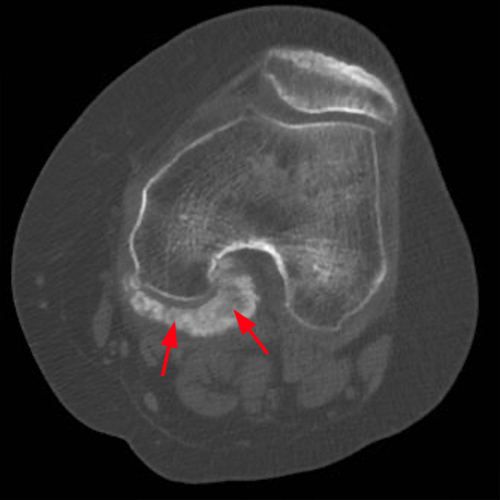

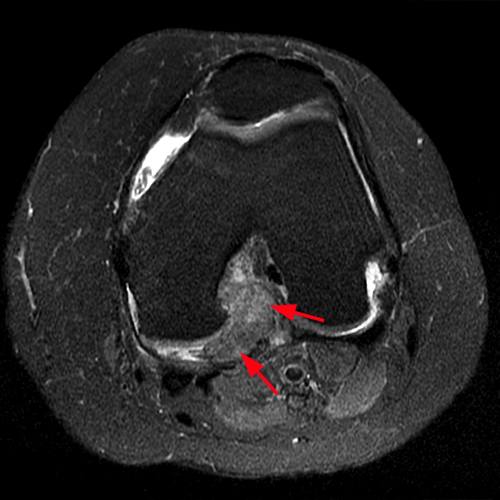
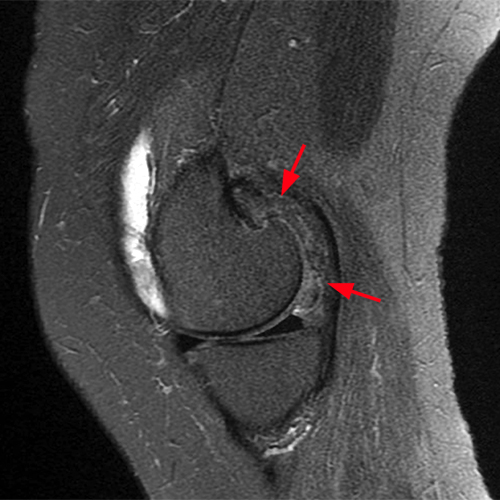
Figure 25. Tophaceous pseudogout. Axial (25a) and sagittal (25b) CT images demonstrate a calcified soft tissue mass closely associated with the posterior aspect of the medial femoral condyle (red arrows). Axial (25c) and sagittal (25d) fluid-sensitive MR images show this soft tissue mass with heterogeneous, but predominantly low, signal intensity, which corresponds to the areas of calcification seen on the CT images (red arrows). Excisional biopsy of this mass demonstrated findings consistent with CPPD crystal deposition (Case, courtesy of Brady Huang, M.D.)
Conditions That Mimic Pyrophosphate Arthropathy:
Pyrophosphate arthropathy closely resembles degenerative joint disease, although, as indicated previously, there are a few characteristics of pyrophosphate arthropathy that are relatively distinctive. These include the involvement of specific joints or regions of joints that are uncommonly involved in osteoarthrosis and some distinctive morphologic features that include extensive bone sclerosis, subchondral cysts that are often multiple and sometimes large, variable osteophyte formation, and, in some cases, rapid and progressive joint destruction (Figure 26). These findings, however, may simulate other disorders such as neuropathic osteoarthropathy, steroid-induced arthropathy, osteonecrosis, and infection.1,28




Figure 26. Destructive arthropathy of the wrist in a patient with dorsal soft tissue swelling. Frontal (26a) and lateral (26b) radiographs of the left wrist show destructive arthropathy of the radiocarpal and intercarpal joints, not typical for CPPD crystal deposition disease. Note erosive and destructive abnormalities of the radius, ulna, and multiple carpal bones (red arrows), as well as prominent dorsal soft tissue swelling (blue arrows). Coronal T1-weighted (26c) and fat-suppressed T1-weighted postcontrast (26d) MR images confirm the radiographic findings of destructive arthropathy, with markedly enhancing synovial proliferation (yellow arrows) accounting for radiographically evident soft tissue swelling. Synovial biopsy yielded CPPD crystals. The extent of the erosive abnormalities raises the additional possibility of gout; however, no monosodium urate crystals were seen at the time of synovial biopsy. (Case, courtesy of Brady Huang, M.D.)
Treatment
No disease-modifying therapies currently exist to reduce CPPD crystal deposits; treatment is aimed at controlling the inflammatory response and decreasing the frequency and severity of symptoms.52 Current treatment methods include non-steroidal anti-inflammatory drugs, colchicine, and intra-articular corticosteroid injections.
Refractory cases may be treated with immune modulators. Anakinra, an interleukin-1R antagonist, has a proven efficacy in autoimmune inflammatory conditions and has been shown to effectively treat refractory symptomatic CPPD crystal deposition disease.52 Tocilizumab, an interleukin-6 antagonist, demonstrates similar promise.52
Conclusion
CPPD crystal deposition disease is a well-known and common disease process with specific articular, periarticular, and soft tissue manifestations as detailed throughout this Web Clinic. Conventional radiography, CT, and ultrasonography can each be used to allow identification of regions of abnormal calcification and to display sites of pyrophosphate arthropathy. MR imaging is less helpful in the analysis of sites of abnormal calcification but can provide useful diagnostic information in cases of tophaceous pseudogout or spinal involvement. When interpreting MR imaging examinations, meticulous review of all the patient’s imaging studies, including x-ray based examinations, is essential to establish the correct diagnosis of CPPD crystal deposition disease. Although other processes can lead to calcific deposits simulating those of CPPD crystal deposition disease, knowledge of the typical sites of involvement and the distinctive morphologic features should allow accurate diagnosis of this very common crystal deposition disease in most cases.
References
- Martel W, McCarter DK, Solsky MA, et al. Further observations on the arthropathy of calcium pyrophosphate crystal deposition disease. Radiology. 1981;141(1):1-15. doi:10.1148/radiology.141.1.6270724 ↩
- MCCARTY DJ, HOLLANDER JL. Identification of urate crystals in gouty synovial fluid. Ann Intern Med. 1961;54:452-460. doi:10.7326/0003-4819-54-3-452 ↩
- KOHN NN, HUGHES RE, McCARTY DJ Jr, FAIRES JS. The significance of calcium phosphate crystals in the synovial fluid of arthritic patients: the “pseudogout syndrome”. II. Identification of crystals. Ann Intern Med. 1962;56:738-745. doi:10.7326/0003-4819-56-5-738 ↩
- Abhishek A, Doherty M. Update on calcium pyrophosphate deposition. Clin Exp Rheumatol. 2016;34(4 Suppl 98):32-38. ↩
- Macmullan P, McCarthy G. Treatment and management of pseudogout: insights for the clinician. Ther Adv Musculoskelet Dis. 2012;4(2):121-131. doi:10.1177/1759720X11432559 ↩
- Ali Y, Weinstein M, Jokl P. Acute pseudogout following intra-articular injection of high molecular weight hyaluronic acid. Am J Med. 1999;107(6):641-642. doi:10.1016/s0002-9343(99)00255 ↩
- Rosenthal AK, Ryan LM. Calcium Pyrophosphate Deposition Disease. N Engl J Med. 2016;374(26):2575-2584. doi:10.1056/NEJMra1511117 ↩
- Resnick D, Williams G, Weisman MH, Slaughter L. Rheumatoid arthritis and pseudo-rheumatoid arthritis in calcium pyrophosphate dihydrate crystal deposition disease. Radiology. 1981;140(3):615-621. doi:10.1148/radiology.140.3.6269144 ↩
- Morales H. Infectious Spondylitis Mimics: Mechanisms of Disease and Imaging Findings. Semin Ultrasound CT MR. 2018;39(6):587-604. doi:10.1053/j.sult.2018.11.006 ↩
- Netter P, Bardin T, Bianchi A, Richette P, Loeuille D. The ANKH gene and familial calcium pyrophosphate dihydrate deposition disease. Joint Bone Spine. 2004;71(5):365-368. doi:10.1016/j.jbspin.2004.01.011 ↩
- Williams CJ, Rosenthal AK. Pathogenesis of calcium pyrophosphate deposition disease. Best Pract Res Clin Rheumatol. 2021;35(4):101718. doi:10.1016/j.berh.2021.101718 ↩
- Williams CJ, Qazi U, Bernstein M, et al. Mutations in osteoprotegerin account for the CCAL1 locus in calcium pyrophosphate deposition disease. Osteoarthritis Cartilage. 2018;26(6):797-806. doi:10.1016/j.joca.2018.03.005 ↩
- Rubin MR, Silverberg SJ. Rheumatic manifestations of primary hyperparathyroidism and parathyroid hormone therapy. Curr Rheumatol Rep. 2002;4(2):179-185. doi:10.1007/s11926-002-0014-0 ↩
- Bilezikian JP, Connor TB, Aptekar R, et al. Pseudogout after parathyroidectomy. Lancet. 1973;1(7801):445-446. doi:10.1016/s0140-6736(73)91876-x ↩
- McCarty DJ. Calcium pyrophosphate dihydrate crystal deposition disease–1975. Arthritis Rheum. 1976;19 Suppl 3:275-285. doi:10.1002/1529-0131(197605/06)19:3+<275::aid-art1780190702>3.0.co;2-0 ↩
- Mitton-Fitzgerald E, Gohr CM, Williams CM, Rosenthal AK. Identification of Common Pathogenic Pathways Involved in Hemochromatosis Arthritis and Calcium Pyrophosphate Deposition Disease: a Review. Curr Rheumatol Rep. 2022;24(2):40-45. doi:10.1007/s11926-022-01054-w ↩
- Nguyen CD, Morel V, Pierache A, et al. Bone and joint complications in patients with hereditary hemochromatosis: a cross-sectional study of 93 patients. Ther Adv Musculoskelet Dis. 2020;12:1759720X20939405. Published 2020 Jul 16. doi:10.1177/1759720X20939405 ↩
- Mitton-Fitzgerald E, Gohr CM, Williams CJ, Ortiz A, Mbalaviele G, Rosenthal AK. Effects of the TNFRSF11B Mutation Associated With Calcium Pyrophosphate Deposition Disease in Osteoclastogenesis in a Murine Model. Arthritis Rheumatol. 2021 Aug;73(8):1543-1549. doi: 10.1002/art.41678. Epub 2021 Jun 8. PMID: 33559312; PMCID: PMC8324507. ↩
- Li J, Hou Y, Zhang S, et al. Excess iron undermined bone load-bearing capacity through tumor necrosis factor-α-dependent osteoclastic activation in mice. Biomed Rep. 2013;1(1):85-88. doi:10.3892/br.2012.6 ↩
- Hofmann C, Girschick HJ, Mentrup B, et al. Clinical Aspects of Hypophosphatasia: An Update. Clinical Reviews in Bone and Mineral Metabolism. 2013;11(2):60-70. doi:https://doi.org/10.1007/s12018-013-9139-0 ↩
- Whyte MP, Landt M, Ryan LM, et al. Alkaline phosphatase: placental and tissue-nonspecific isoenzymes hydrolyze phosphoethanolamine, inorganic pyrophosphate, and pyridoxal 5′-phosphate. Substrate accumulation in carriers of hypophosphatasia corrects during pregnancy. J Clin Invest. 1995;95(4):1440-1445. doi:10.1172/JCI117814 ↩
- Rauf MA, Kotecha J, Moss K. Reducing diagnostic delay in hypophosphatasia: a case series of 14 patients presenting to general rheumatology. Osteoporos Int. 2023 Sep;34(9):1647-1652. doi: 10.1007/s00198-023-06749-z. Epub 2023 Apr 28. PMID: 37118032; PMCID: PMC10427523. ↩
- Al Shibli A, Narchi H. Bartter and Gitelman syndromes: Spectrum of clinical manifestations caused by different mutations. World J Methodol. 2015 Jun 26;5(2):55-61. doi: 10.5662/wjm.v5.i2.55. PMID: 26140272; PMCID: PMC4482822. ↩
- Favero M, Calò LA, Schiavon F, Punzi L. Miscellaneous non-inflammatory musculoskeletal conditions. Bartter’s and Gitelman’s diseases. Best Pract Res Clin Rheumatol. 2011;25(5):637-648. doi:10.1016/j.berh.2011.10.013 ↩
- Knoers, N.V., Levtchenko, E.N. Gitelman syndrome. Orphanet J Rare Dis 3, 22 (2008). https://doi.org/10.1186/1750-1172-3-22 ↩
- Rachow JW, Ryan LM: Inorganic pyrophosphatase metabolism in arthritis. Rheum Dis Clin North Am 1988;14:289–302 ↩
- Freire V, Moser TP, Lepage-Saucier M. Radiological identification and analysis of soft tissue musculoskeletal calcifications. Insights Imaging. 2018;9(4):477-492. doi:10.1007/s13244-018-0619-0 ↩
- Resnick D, Niwayama G, Goergen TG, et al. Clinical, radiographic and pathologic abnormalities in calcium pyrophosphate dihydrate deposition disease (CPPD): pseudogout. Radiology. 1977;122(1):1-15. doi:10.1148/122.1.1 ↩
- Ishida T, Dorfman HD, Bullough PG. Tophaceous pseudogout (tumoral calcium pyrophosphate dihydrate crystal deposition disease). Hum Pathol. 1995;26(6):587-593. doi:10.1016/0046-8177(95)90161-2 ↩
- Seybold JD, Dahl WJ, Kadakia AR. Tophaceous pseudogout of the ankle: case report. Foot Ankle Int. 2011;32(7):717-721. doi:10.3113/FAI.2011.0717 ↩
- Resnik CS, Miller BW, Gelberman RH, Resnick D. Hand and wrist involvement in calcium pyrophosphate dihydrate crystal deposition disease. J Hand Surg Am. 1983;8(6):856-863. doi:10.1016/s0363-5023(83)80081-1 ↩
- Yang BY, Sartoris DJ, Djukic S, Resnick D, Clopton P. Distribution of calcification in the triangular fibrocartilage region in 181 patients with calcium pyrophosphate dihydrate crystal deposition disease. Radiology. 1995;196(2):547-550. doi:10.1148/radiology.196.2.7617875 ↩
- Jägefr HJ, Mehring U, Götz GF, et al. Radiological features of the visceral and skeletal involvement of hemochromatosis. Eur Radiol. 1997;7(8):1199-1206. doi:10.1007/s003300050274 ↩
- Yang BY, Sartoris DJ, Resnick D, Clopton P. Calcium pyrophosphate dihydrate crystal deposition disease: frequency of tendon calcification about the knee. J Rheumatol. 1996 May;23(5):883-8. PMID: 8724303. ↩
- Foldes K, Lenchik L, Jaovisidha S, Clopton P, Sartoris DJ, Resnick D. Association of gastrocnemius tendon calcification with chondrocalcinosis of the knee. Skeletal Radiol. 1996 Oct;25(7):621-4. doi: 10.1007/s002560050147. PMID: 8915044. ↩
- Bencardino JT, Hassankhani A. Calcium pyrophosphate dihydrate crystal deposition disease. Semin Musculoskelet Radiol. 2003;7(3):175-185. doi:10.1055/s-2003-43228 ↩
- Resnick D, Pineda C. Vertebral involvement in calcium pyrophosphate dihydrate crystal deposition disease. Radiographic-pathological correlation. Radiology. 1984;153(1):55-60. doi:10.1148/radiology.153.1.6089266 ↩
- Sekijima Y, Yoshida T, Ikeda S. CPPD crystal deposition disease of the cervical spine: a common cause of acute neck pain encountered in the neurology department. J Neurol Sci. 2010;296(1-2):79-82. doi:10.1016/j.jns.2010.05.028 ↩
- Chang EY, Lim WY, Wolfson T, et al. Frequency of atlantoaxial calcium pyrophosphate dihydrate deposition at CT. Radiology. 2013;269(2):519-524. doi:10.1148/radiol.13130125 ↩
- Lindenmeyer C, Sobel A, Nazarian L, Mandel S, Raikin S, Karanjia H. A Case Study of Pseudo-Neuropathic Pseudogout. The Medicine Forum. 2013;14(1). doi:https://doi.org/10.29046/tmf.014.1.016 ↩
- Zweifel D, Ettlin D, Schuknecht B, Obwegeser J. Tophaceous calcium pyrophosphate dihydrate deposition disease of the temporomandibular joint: the preferential site?. J Oral Maxillofac Surg. 2012;70(1):60-67. doi:10.1016/j.joms.2011.06.207 ↩
- Borowski A, Heikaus S, Kurt M. Calcium Pyrophosphate Dihydrate Crystal Deposition Disease of the Sternoclavicular Joint. Thorac Cardiovasc Surg Rep. 2015 Dec;4(1):46-8. doi: 10.1055/s-0034-1390153. Epub 2014 Oct 31. PMID: 26693128; PMCID: PMC4670306. ↩
- Shirazian H, Chang EY, Wolfson T, Gamst AC, Chung CB, Resnick DL. Prevalence of sternoclavicular joint calcium pyrophosphate dihydrate crystal deposition on computed tomography. Clin Imaging. 2014 Jul-Aug;38(4):380-383. doi: 10.1016/j.clinimag.2014.02.016. Epub 2014 Mar 6. PMID: 24642252. ↩
- Budzik JF, Marzin C, Legrand J, Norberciak L, Becce F, Pascart T. Can Dual-Energy Computed Tomography Be Used to Identify Early Calcium Crystal Deposition in the Knees of Patients With Calcium Pyrophosphate Deposition?. Arthritis Rheumatol. 2021;73(4):687-692. doi:10.1002/art.41569 ↩
- Kravchenko D, Karakostas P, Kuetting D, et al. The role of dual energy computed tomography in the differentiation of acute gout flares and acute calcium pyrophosphate crystal arthritis. Clin Rheumatol. 2022;41(1):223-233. doi:10.1007/s10067-021-05949-4 ↩
- Abreu M, Johnson K, Chung CB, et al. Calcification in calcium pyrophosphate dihydrate (CPPD) crystalline deposits in the knee: anatomic, radiographic, MR imaging, and histologic study in cadavers. Skeletal Radiol. 2004;33(7):392-398. doi:10.1007/s00256-004-0767-9 ↩
- Kaushik S, Erickson JK, Palmer WE, Winalski CS, Kilpatrick SJ, Weissman BN. Effect of chondrocalcinosis on the MR imaging of knee menisci. AJR Am J Roentgenol. 2001;177(4):905-909. doi:10.2214/ajr.177.4.1770905 ↩
- Finkenstaedt T, Biswas R, Abeydeera NA, et al. Ultrashort Time to Echo Magnetic Resonance Evaluation of Calcium Pyrophosphate Crystal Deposition in Human Menisci. Invest Radiol. 2019;54(6):349-355. doi:10.1097/RLI.0000000000000547 ↩
- Sullivan J, Pillinger MH, Toprover M. Chondrocalcinosis: Advances in Diagnostic Imaging. Curr Rheumatol Rep. 2021;23(10):77. Published 2021 Oct 8. doi:10.1007/s11926-021-01044-4 ↩
- Resnik CS, Resnick D. Crystal deposition disease. Semin Arthritis Rheum. 1983 May;12(4):390-403. doi: 10.1016/0049-0172(83)90019-7. PMID: 6308832. ↩
- Ankli B, Kyburz D, Hirschmann A, et al. Calcium pyrophosphate deposition disease: a frequent finding in patients with long-standing erosive gout. Scand J Rheumatol. 2018;47(2):127-130. doi:10.1080/03009742.2017.1332239 ↩
- Stack, John, and Geraldine McCarthy. “Calcium pyrophosphate deposition (CPPD) disease–Treatment options.” Best Practice & Research Clinical Rheumatology 35.4 (2021): 101720. ↩
