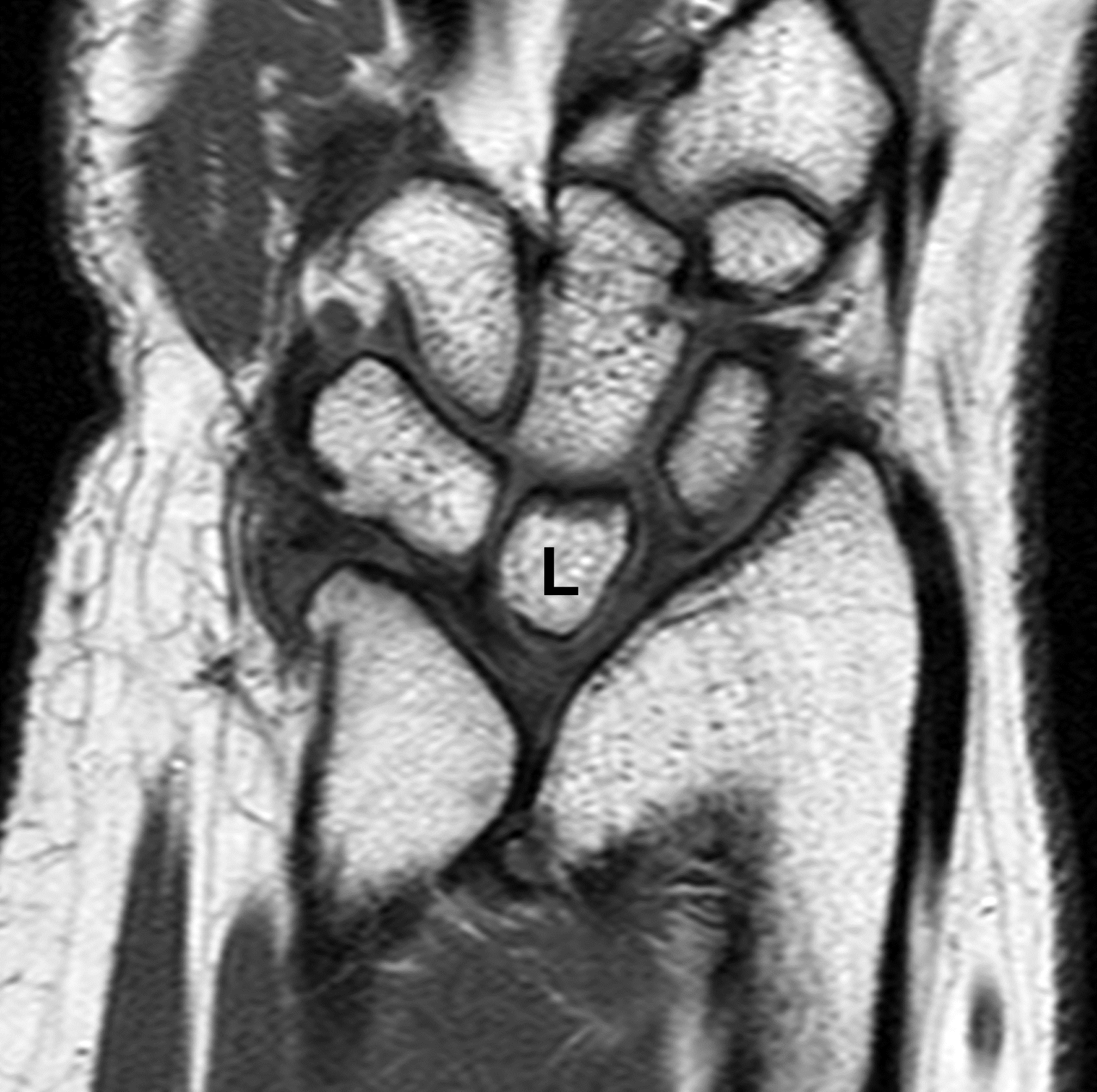
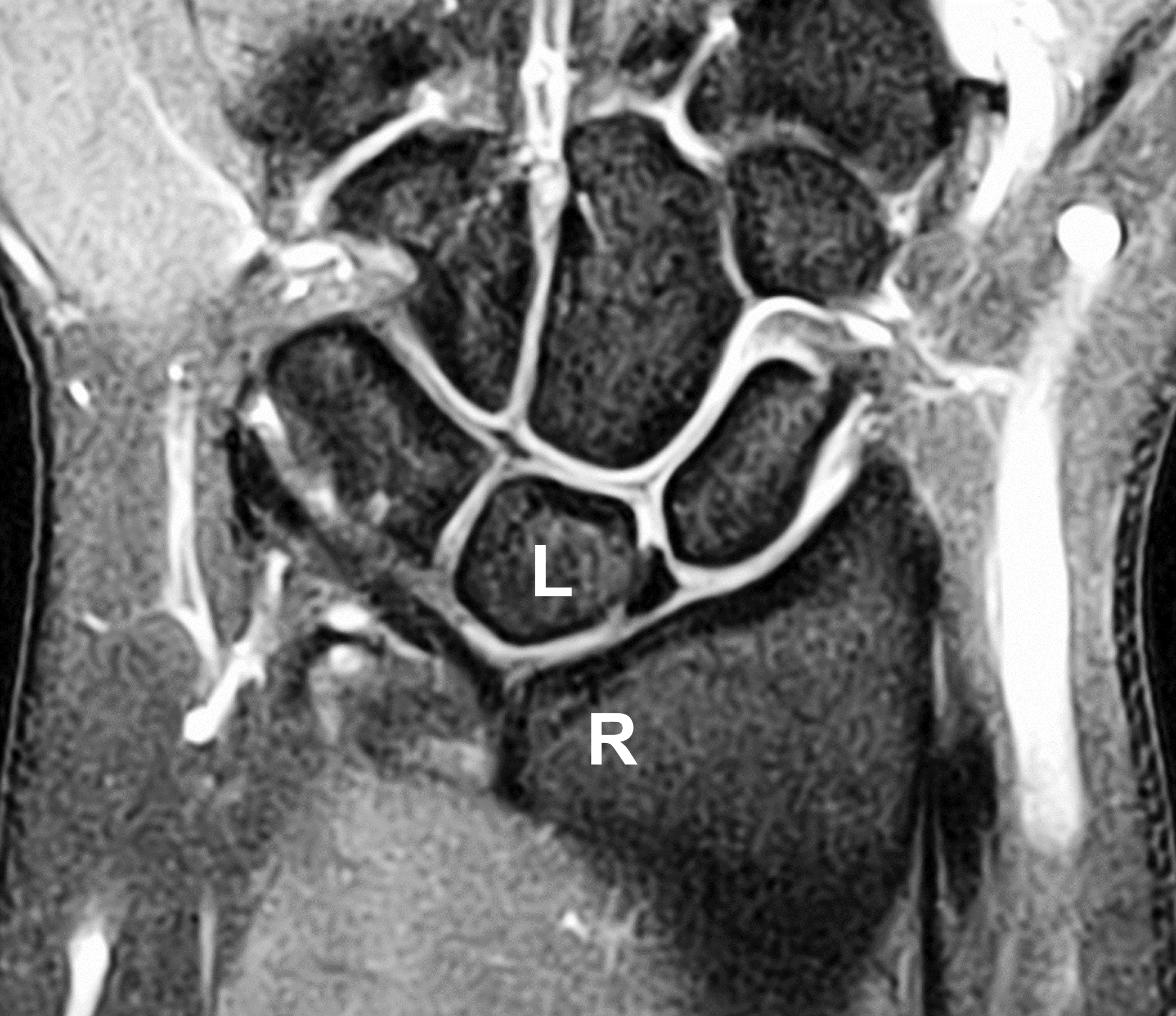
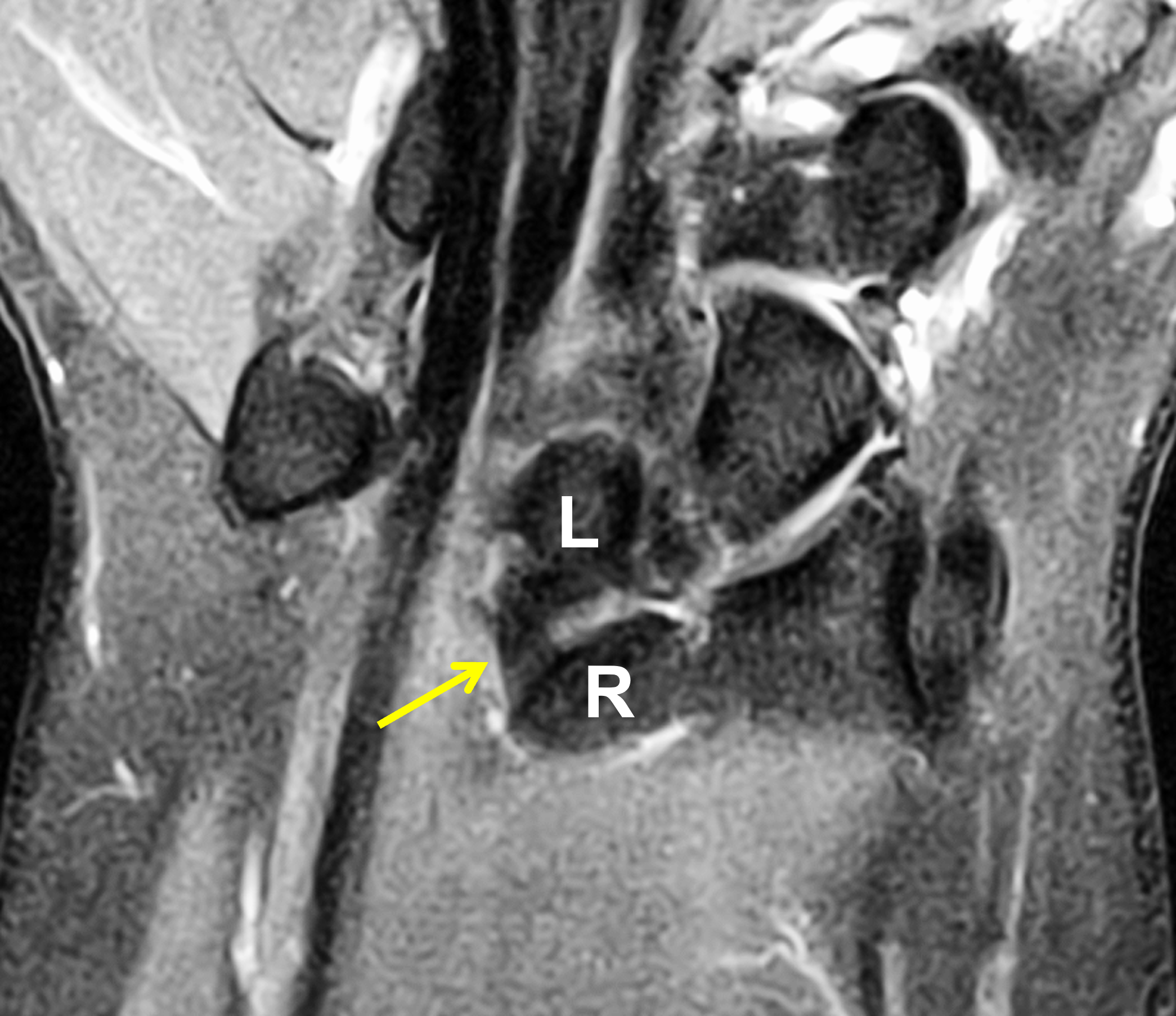
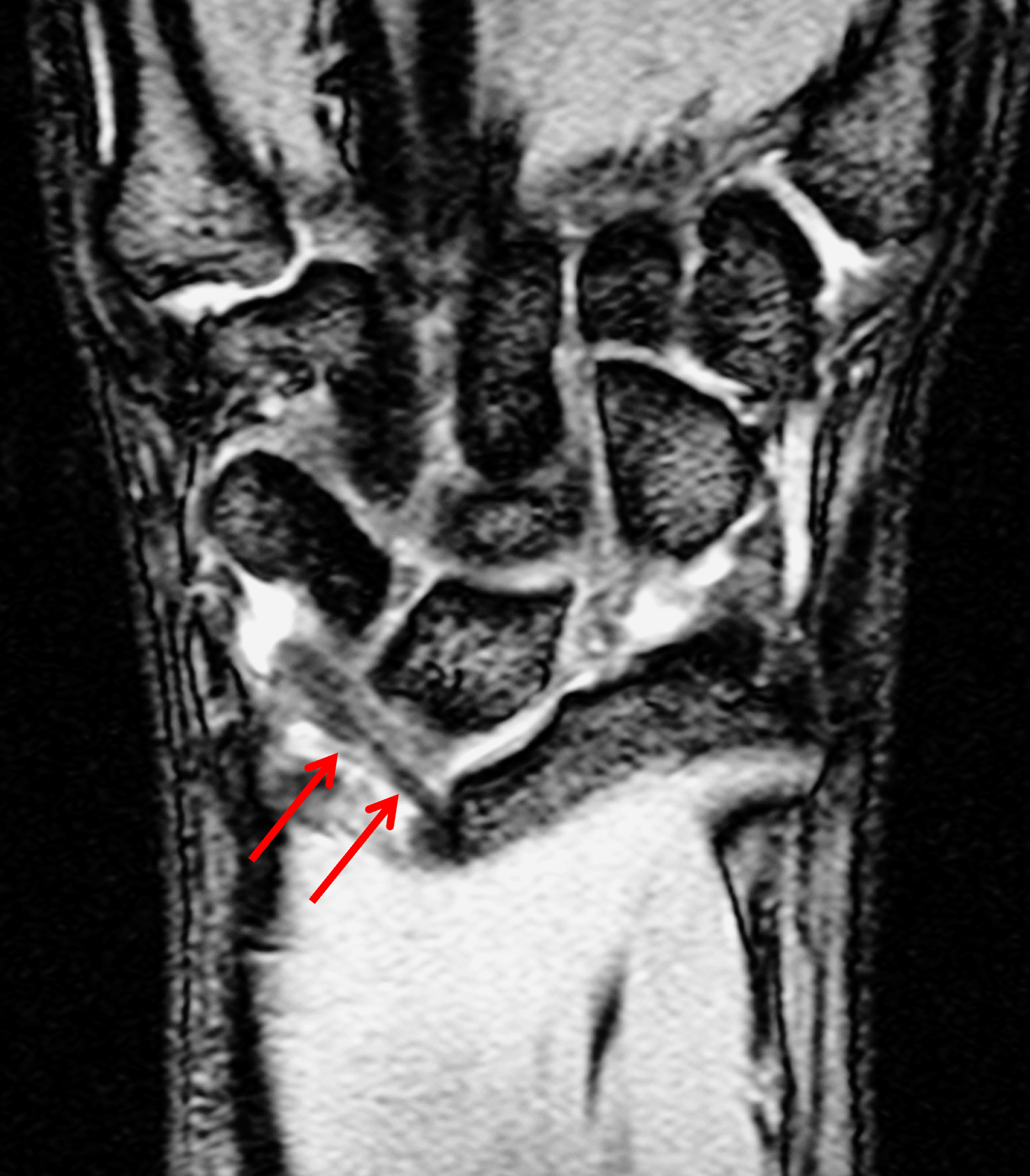
Clinical History: A 13-year-old girl presents with a progressive wrist deformity beginning a year ago. She has mild ulnar-sided wrist pain with activities. On exam, both wrists demonstrate dorsal prominence of the ulnar heads. Coronal T1-weighted (1a) and fat-suppressed proton density-weighted (1b) images and axial T1-weighted images (1c and 1d) are shown. What are the findings? What is your diagnosis?


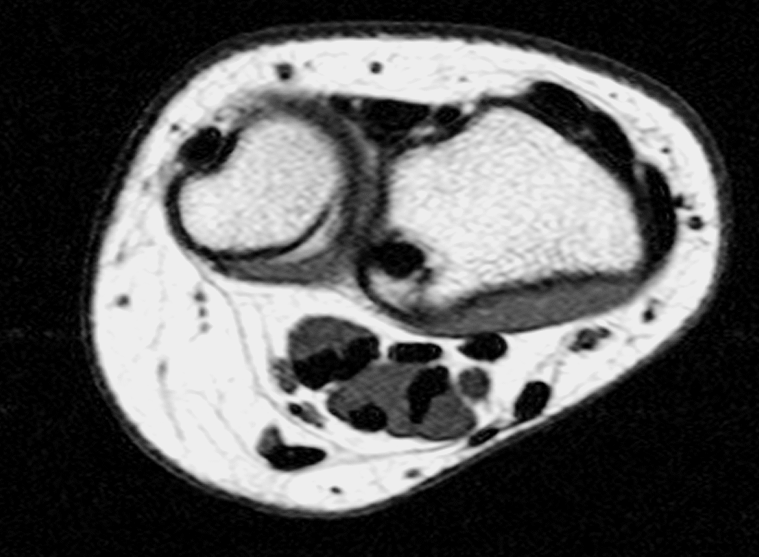
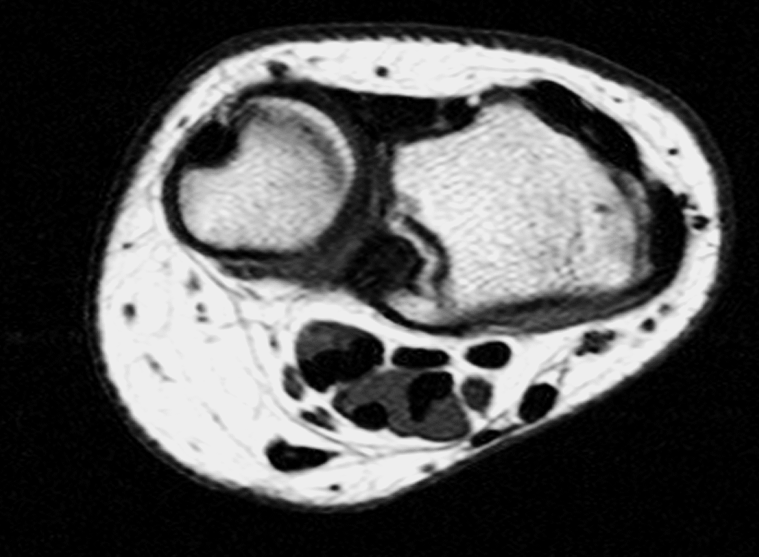
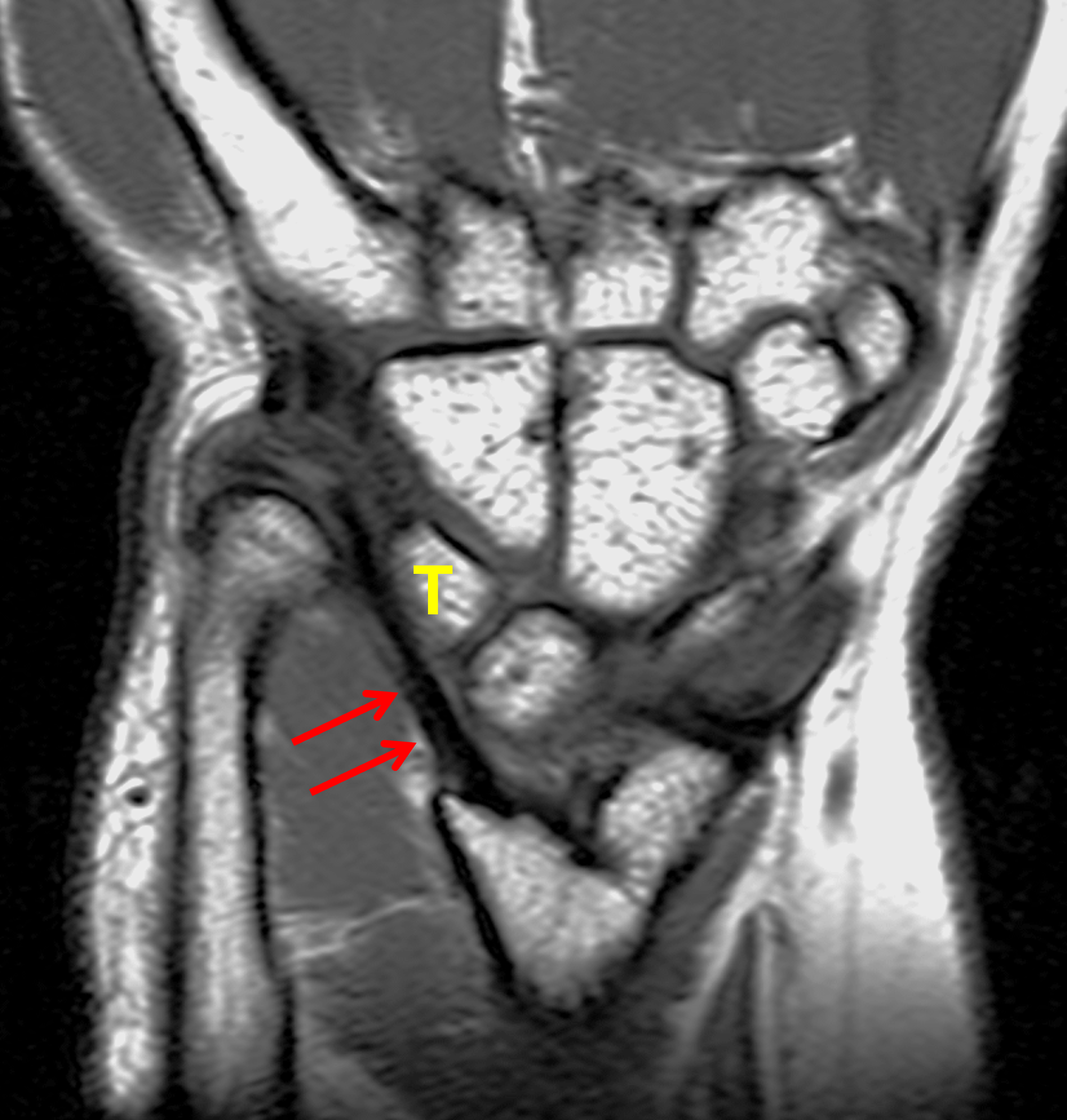
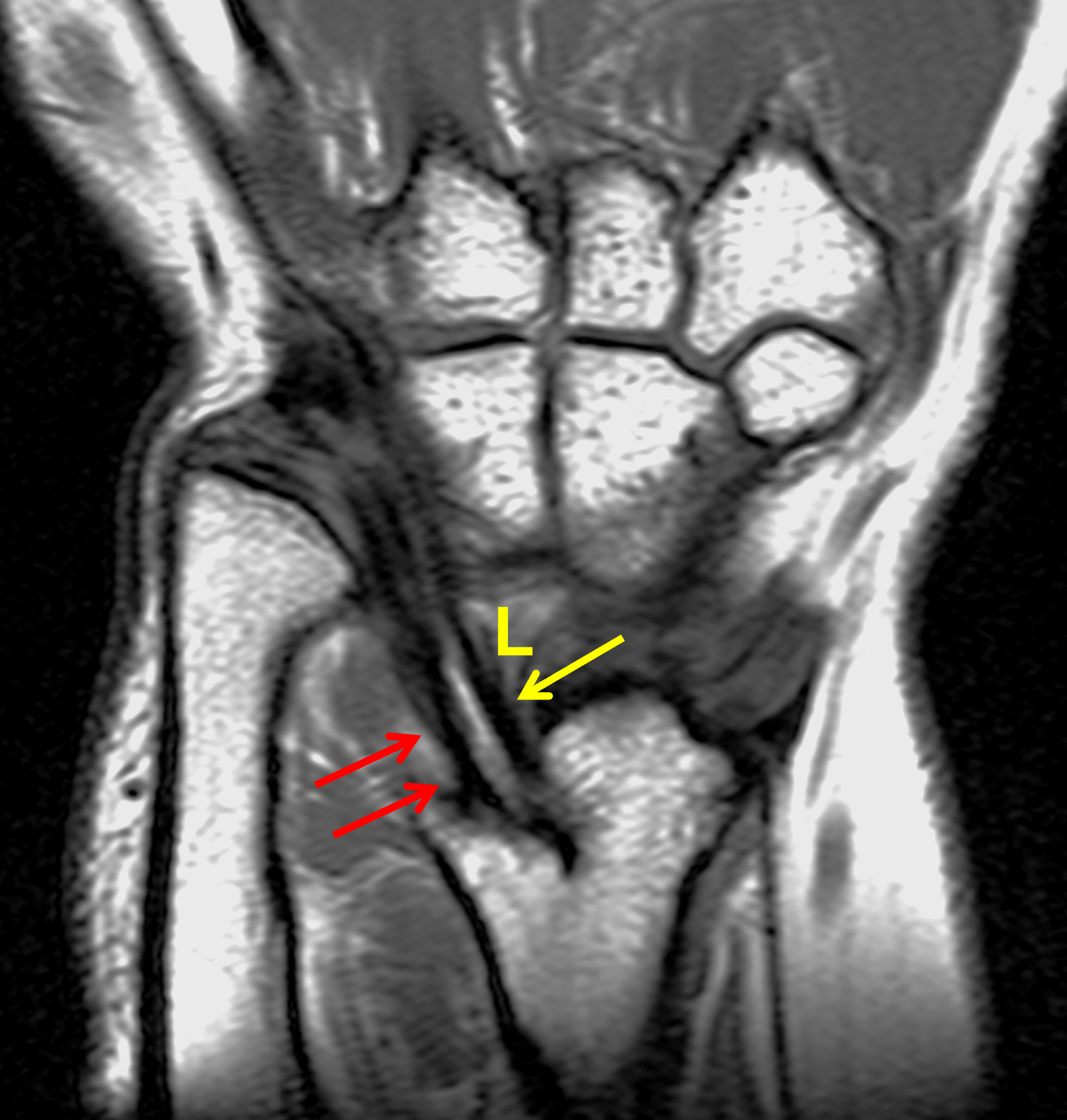
Coronal (1a) T1-weighted and (1b) fat-suppressed T2-weighted images of the wrist. Axial T1-weighted images (1c and 1d) through the distal forearm.
Findings
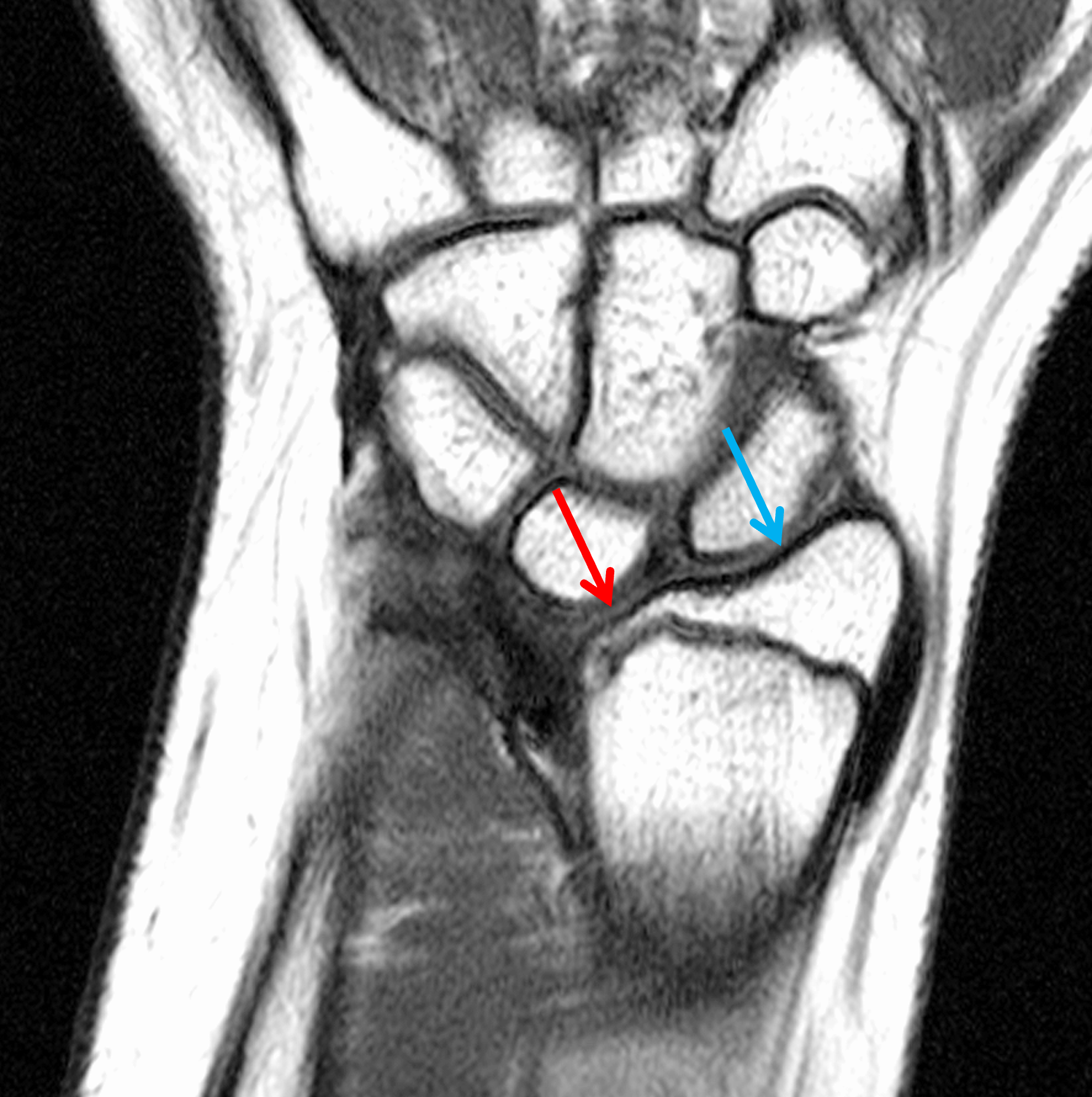

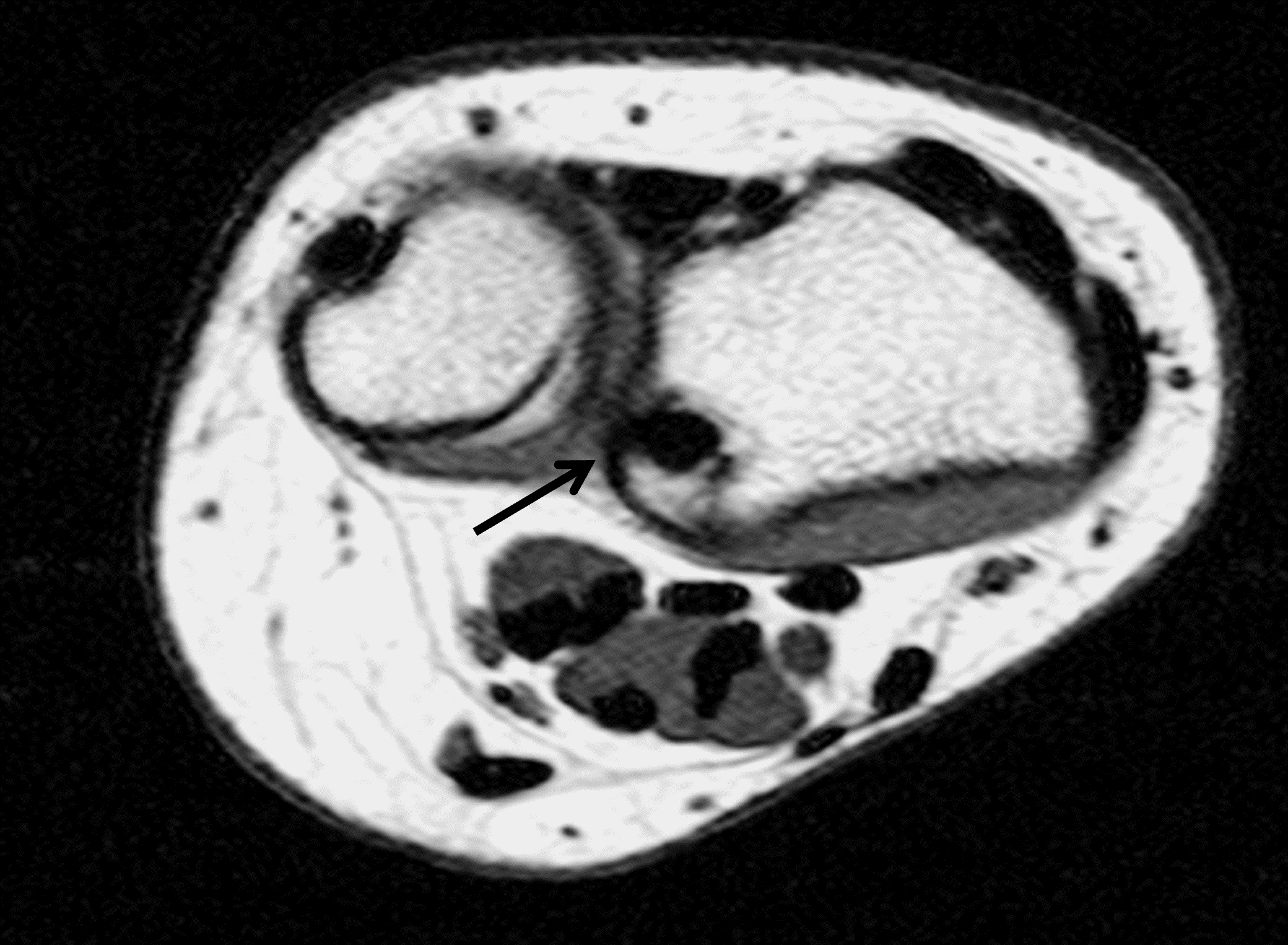
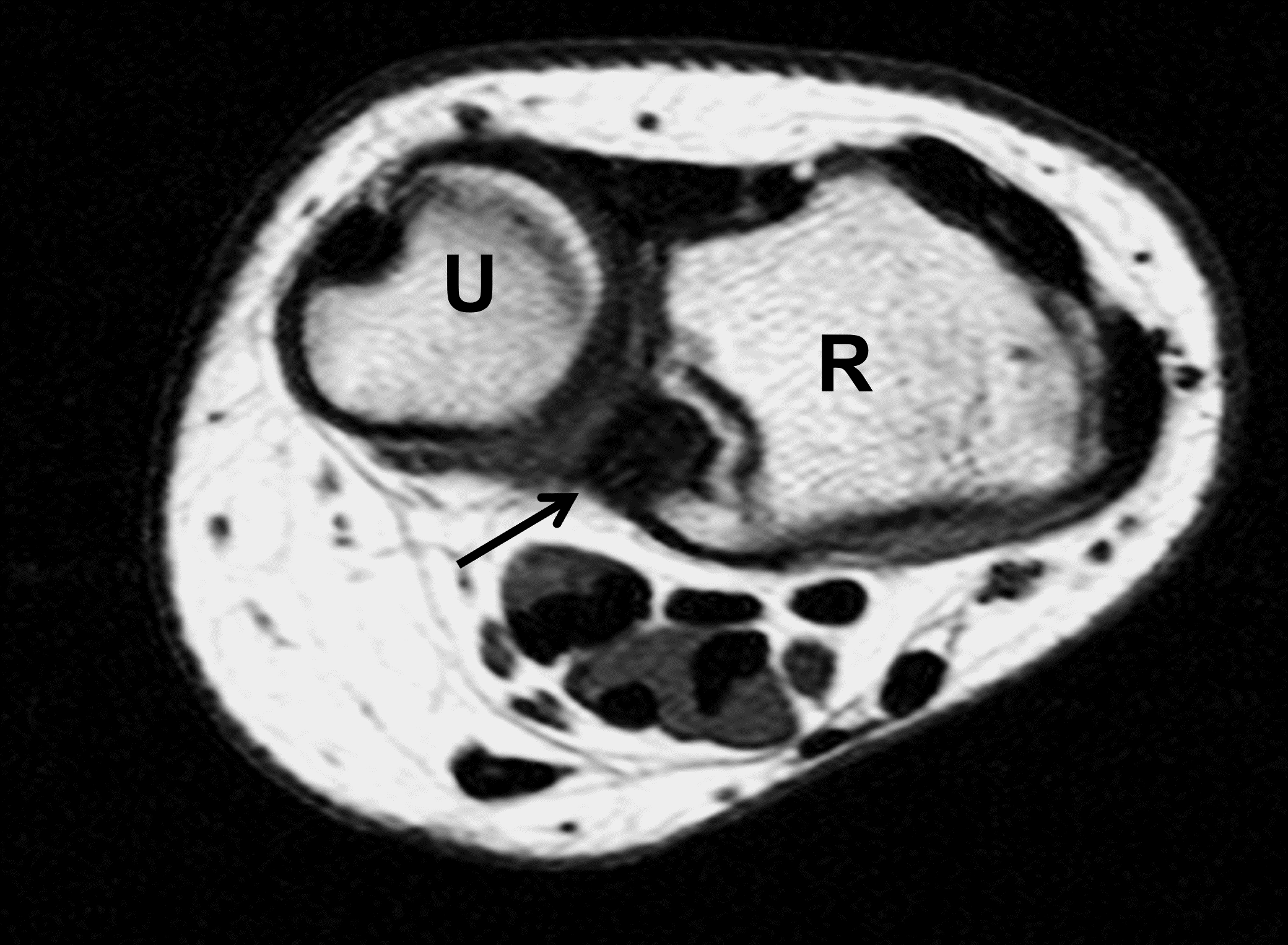
Madelung deformity. The coronal T1-weighted image (2a) shows a growth disturbance of the distal radius with the ulnar side of the epiphysis (red arrow) underdeveloped compared to the radial side (blue arrow). On the T2-weighted image (2b), an anomalous volar ligament (yellow arrows) originates proximal to the distal radial growth plate and extends to the triquetrum (T). The axial images (2c and 2d) show the radial origin of the anomalous ligament (arrows). Note the mild dorsal subluxation of the ulnar head (U) relative to the distal radius (R).
Diagnosis
Madelung deformity with an anomalous volar radiotriquetral ligament.
Introduction
Madelung deformity is a relatively rare abnormality of the wrist, first described in 1834 by Guillaume Dupuytren (better known for the finger contracture named after him), and more fully by Otto Madelung in 1878.1 It is characterized primarily by a developmental growth deficiency of the ulnar and volar aspect of the distal radius resulting in secondary changes in the morphology of the carpus. Classically, the condition has been associated with an abnormal volar short radiolunate ligament (Vickers ligament). However, recent investigations have identified a second anomalous radiotriquetral ligament in many cases.
Pathophysiology
Madelung deformity is caused by premature closure of the ulnovolar portion of the distal radial physis, leading to increased radial inclination and volar tilt of the distal radius. In approximately 83% of cases, an abnormally thick volar short radiolunate ligament, known as Vickers ligament, can be identified.2,3 Unlike the normal short radiolunate ligament that originates from the distal radial epiphysis, Vickers ligament originates in the metaphysis proximal to the physis so that is crosses the ulnar aspect of the distal radial growth plate, potentially tethering it and restricting growth.2, 4,5,6 However, Vickers ligament is not typically visible at surgery until approximately 7 years of age, leading some authors to posit that it may be a result of the deformity and not its primary cause.3 Recently, a second anomalous ligament has been identified in some patients with Madelung deformity – a volar radiotriquetral ligament – that can occur in isolation or together with Vickers ligament.7,8,9,10 This ligament also has an origin in the distal radial metaphysis, proximal to the physis. Based on MR appearances, both ligaments tend to insert along the ulnar margins of either the lunate or triquetrum (Figure 3).
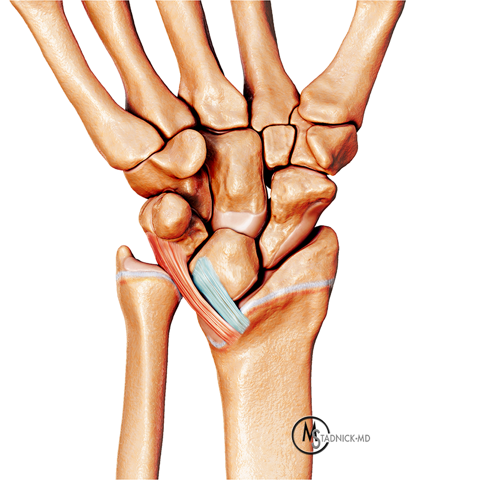
Drawing showing the anatomic features of Madelung deformity before skeletal maturity, viewed from the palmar side. The ulnar aspect of the distal radial epiphysis is hypoplastic resulting in increased inclination of the distal articular surface towards the ulna, as well as radial shortening and positive ulnar variance. The lunate is displaced proximally with a triangular configuration of its proximal surface. A thick volar short radiolunate (Vickers) ligament (blue) and anomalous volar radiotriquetral ligament (red) are shown originating proximal to the distal radial growth plate. In clinical cases, one or both ligaments may be present.
Clinical Features
The overall incidence of Madelung deformity is unknown because mild cases may be asymptomatic and go unrecognized. Girls are affected more frequently than boys, in a ratio of approximately 4:1.11,12The condition can occur spontaneously or have a familial occurrence, related to mutations in the short stature homeobox (SHOX) gene located on the X and Y sex chromosomes, which are inherited with a pseudoautosomal dominant pattern.13 Madelung deformity is also seen in association with Leri-Weill dyschondrosteosis, a skeletal dysplasia characterized by histologic abnormalities in the growth zone of the physis. These patients present with mesomelia (short forearms), dwarfism, and bilateral symmetric Madelung deformity.13 Like patients with the congenital form of Madelung deformity, individuals with Leri-Weill syndrome have a mutation in the SHOX gene.14 Additionally, Madelung deformity can develop in some patients with Turner’s syndrome (Figure 4); these patients have only one X chromosome meaning that one copy of the SHOX gene will be absent.13, 15


Madelung deformity in a 45-year-old woman with Turner’s syndrome. PA (4a) and lateral (4b) radiographs show the typical findings of Madelung deformity including deficiency of the ulnar side of the distal radius resulting in increased radial and volar inclination of the radius, positive ulnar variance, and dorsal subluxation of the ulnar head. The severe shortening of the fourth metacarpal is a characteristic of Turner’s syndrome.



45-year-old woman with “entire radius” subtype of Madelung deformity. PA (5a) and lateral (5b) forearm radiographs show severe shortening and bowing of the entire radius in addition to findings of Madelung deformity at the wrist. Similar findings were present on the contralateral side. Genetic testing was not performed in this case, but the patient likely has Leri-Weill dyschondrosteosis given the overall shortening of the forearm. Acute symptoms were due to a fracture of the distal ulna (arrow). A coronal fat-suppressed proton density-weighted image (5c) shows a portion of an anomalous radiotriquetral ligament (arrows). Marrow edema in the ulnar shaft (U) is related to the fracture.
Imaging Findings
The diagnosis of Madelung deformity is typically made radiographically.12, 15 The findings are characteristic: Prior to skeletal maturity the ulnar side of the distal radial epiphysis will be deficient and a physeal bar may be visible crossing the adjacent growth plate, with the PA radiograph showing excessive inclination of the distal radius towards the ulna, which results in the lunate displaced proximally into a deep concavity in the distal radius (Figure 6). In older patients, the lunate and proximal carpal row can acquire a pyramidal or V-shape. A flame-shaped notch may be visible in the distal radial metaphysis (Figure 7), corresponding the origin site of an anomalous volar ligament,5, 14 although in one large series 4 out of 54 patients with a radiographic notch did not have a Vickers ligament at surgical exploration, while 12 of 62 patients with a surgically proved Vickers ligament did not show a notch.3 Positive ulnar variance can be severe, with incongruity or subluxation at the distal radioulnar joint.5 In the whole-radius variant severe bowing of the radial shaft and widening of the radiocapitellar joint is characteristic (Figure 5). On the lateral view of the wrist, the distal radius shows excessive volar tilt, with volar subluxation of the carpus and dorsal displacement of the ulnar head.20


Madelung deformity in an 11-year-old girl. PA (6a) and lateral (6b) radiographs show severe deficiency of the ulnar half of the distal radial epiphysis and a probable physeal bar in the ulnar aspect of the growth plate. The lunate fossa shows excessive inclination towards the ulna. Note the positive ulnar variance and dorsal subluxation of the ulnar head.


Severe Madelung deformity in an adult (same patient as Figure 5). A PA radiograph (7a) shows a characteristic “notch” configuration in the ulnar aspect of the metaphyseal region of the distal radius (arrows). The axial T1-weighted image (7b) through the corresponding aspect of the radius shows that the bone deformity corresponds to the origin of Vickers ligament (arrow).
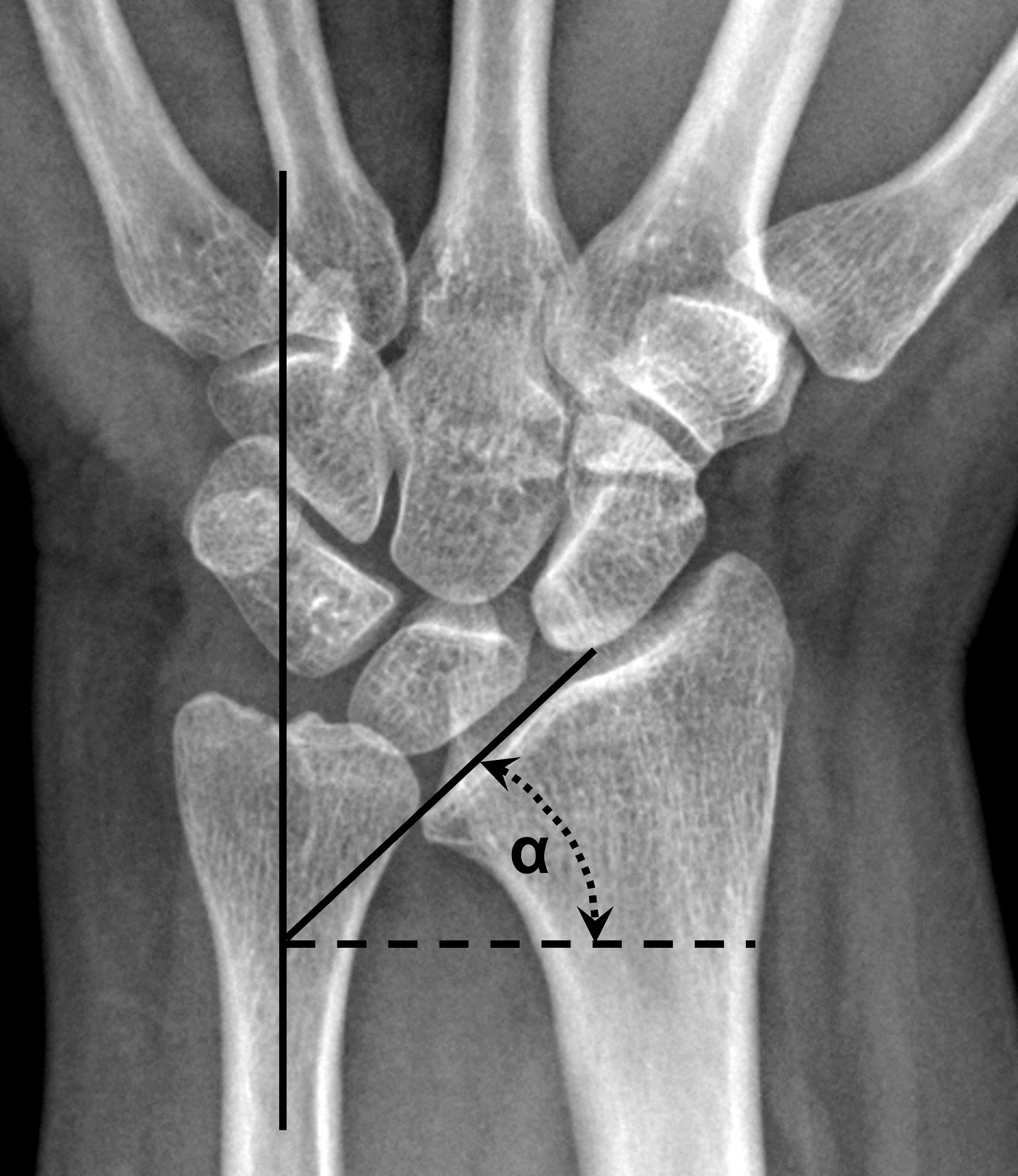
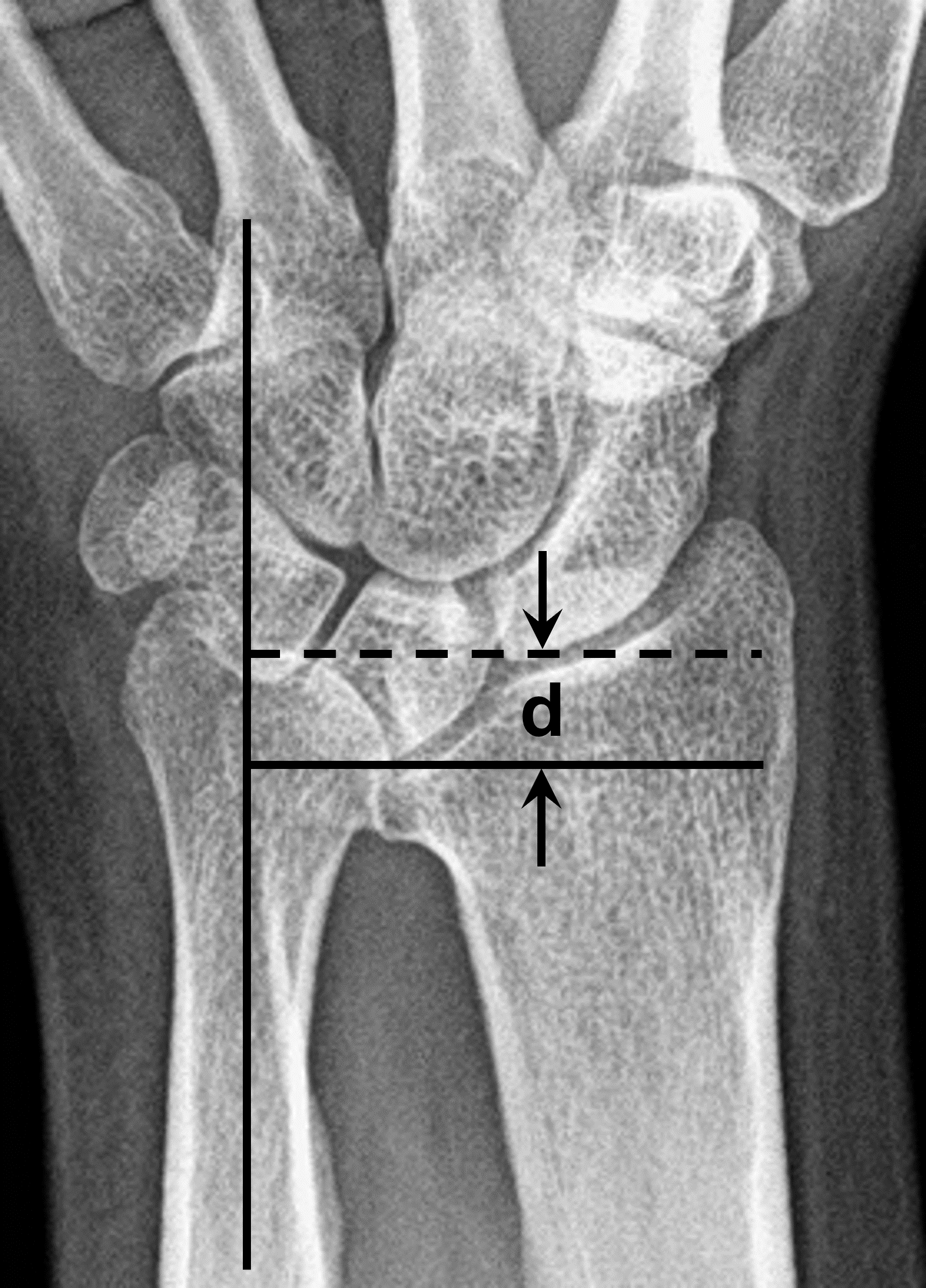
Radiographic measurements in Madelung deformity in two different patients. The lunate fossa angle (8a) is defined as the complement of the angle formed by the long axis of the ulnar shaft and the lunate fossa of the radius. An angle (α) greater or equal to 35° is associated with Madelung deformity. Lunate subsidence (8b) is the distance between the distal articular surface of the ulnar head and proximal-most cortex of the lunate, measured perpendicular to the long axis of the ulnar shaft. A measurement (d) greater or equal to 4 mm is characteristic of advanced Madelung deformity, but is relatively insensitive.

Madelung deformity in a 38-year-old woman. A Coronal T1-weighted (9a) image shows excessive inclination of the distal radius surface, primarily involving the lunate fossa. Note the triangular configuration of the lunate (L) and proximal carpal row. On the T2*-weighted gradient-echo image, the triangular fibrocartilage disc (arrow) has a steep oblique orientation.


67-year-old woman with Madelung deformity resulting in ulnocarpal impaction. A PA radiograph (10a) shows typical findings of Madelung deformity, including positive ulnar variance. A coronal T1-weighted image (10b) shows impaction of the ulnar head against the lunate, with a small subchondral lunate cyst, and absent triangular fibrocartilage (TFC) tissue between the two bones (black arrow). A residual fragment of the TFC (red arrow) is visible adjacent to the ulnar styloid. The patient was managed with an ulnar shortening osteotomy.
31-year-old woman with Madelung deformity and a Vickers ligament. Coronal fat-suppressed proton density-weighted image (11a) shows a mild Madelung deformity. An image located more volarly (11b) shows a thick radiolunate ligament (Vickers ligament, arrow) inserting on the ulnar aspect of the lunate (L). (R) = radius.

25-year-old woman with Madelung deformity and an anomalous radiotriquetral ligament. PA radiograph (12a) shows a mild Madelung deformity. An anomalous radiotriquetral ligament (arrows) is visible on the coronal T2*-weighted gradient-echo image (12b).
25-year-old woman with both a Vickers ligament and an anomalous radiotriquetral ligament. Sequential coronal T1-weighted images (13a and 13b) show an anomalous radiotriquetral ligament (red arrows) inserting along the ulnar margin of the triquetrum (T) and a Vickers ligament (yellow arrows) attached to the ulnar margin of the lunate (L). Note that the radiotriquetral ligament origin is located ulnar to Vickers ligament.


Post-traumatic Madelung-type deformity in 17-year-old boy, who experienced a Salter-Harris IV distal radius fracture 5 years previously. A PA radiograph (14a) shows radial shortening with positive ulnar variance. Note that the deformity of the distal radius does not primarily involve the lunate fossa, unlike in true Madelung deformity. The coronal CT reconstruction (14b) shows location of prior physeal bar that resulted in premature physis closure (arrows).
Treatment Options
Conservative therapy with non-steroidal anti-inflammatory drugs, activity modification, and splinting will often suffice in patients with mild symptoms,24 with sequential radiographs acquired until skeletal maturity to monitor progression of the deformity.11 For more symptomatic patients, surgery is usually recommended. The choice of operation depends on the age of the patient and the anatomic abnormalities present. In patients who are still growing, resection of Vickers ligament and/or an anomalous radiotriquetral ligament is typically performed to relieve pain and prevent progression of the deformity;25 when combined with a radial physiolysis (resection of a physeal bar and fat interposition) this is known as a Langenskiöld procedure.2, 6, 26 Alternatively or in addition, epiphysiodesis of the distal ulnar and radial aspect of the distal radial growth plates can be performed to arrest growth and maintain a more normal relationship between the distal radius and ulna.26 After skeletal maturity, deformity progression is no longer an issue so surgical treatment is indicated for severe chronic pain or decreased motion, with the goal of addressing the deformity that has already occurred.16, 25 This may be accomplished through a distal radius dome osteotomy allowing for multiplanar correction, ulnar head resection, Suavé-Kapandji procedure (distal radioulnar joint arthrodesis with an ulnar osteotomy proximal to the fusion site), ulnar shortening osteotomy, or distal radioulnar arthroplasty.12, 16, 27
Differential Diagnosis
Other conditions may result in a wrist appearance that appears similar to classic Madelung deformity, sometimes referred to as a Madelung-type or pseudo-Madelung deformity. These include prior childhood trauma that damages the distal radial growth plate (Figure 14), either a Salter-Harris fracture or chronic, repetitive injury as might occur with gymnast’s wrist.11, 15, 28Prior infection or juvenile chronic arthritis can also arrest growth in a portion of the distal physis, causing a Madelung-type deformity.14, 29 When detected before skeletal maturity, cases of premature segmental growth plate closure can be managed surgically by resection of a physeal bar and/or epiphysiodesis and osteotomies. Madelung-type deformities have also been reported in association with multiple epiphyseal dysplasia (Figure 15), Ollier disease (multiple enchondromas), and multiple hereditary exostosis.5, 14 While their deformities may morphologically resemble classic Madelung deformity, wrists in patients with Madelung-type deformities should not harbor a Vickers or anomalous radiotriquetral ligament.15


18-year-old woman with Madelung-type deformity due to multiple epiphyseal dysplasia. A PA radiograph (15a) shows morphology of the distal radius that mimics Madelung deformity. Note, however, the severe shortening of all the metacarpal bones. MRI including a T2*-weighted coronal gradient-echo sequence (15b) showed no evidence of a Vickers ligament nor anomalous radiotriquetral ligament.
Conclusion
Madelung deformity of the wrist results from a growth disturbance primarily involving the ulnar aspect of the distal radius, and is frequently associated with an anomalous volar short radial ligament (Vickers ligament) and/or radiotriquetral ligament. Diagnosis is made radiographically by identification of several characteristic features. MRI is useful to identify associated anomalous ligament(s), which affects treatment, especially before skeletal maturity. In longstanding cases, MRI is used to identify complications secondary to the deformity. Several other conditions can produce similar findings called Madelung-like deformities, but in these wrists, anomalous ligaments are not present.
References
- Arora AS, Chung KC. Otto W. Madelung and the recognition of Madelung’s deformity. J Hand Surg Am. 2006;31(2):177-182. doi:10.1016/j.jhsa.2005.09.001 ↩
- Vickers D, Nielsen G. Madelung deformity: surgical prophylaxis (physiolysis) during the late growth period by resection of the dyschondrosteosis lesion. J Hand Surg Br. 1992;17(4):401-407. doi:10.1016/s0266-7681(05)80262-1 ↩
- Farr S, Martinez-Alvarez S, Little KJ, Henstenburg J, Ristl R, Stauffer A, et al. The prevalence of Vickers’ ligament in Madelung’s deformity: a retrospective multicentre study of 75 surgical cases. J Hand Surg Eur Vol. 2021;46(4):384-390. doi:10.1177/1753193420981522 ↩
- Tuder D, Frome B, Green DP. Radiographic spectrum of severity in Madelung’s deformity. J Hand Surg Am. 2008;33(6):900-904. doi:10.1016/j.jhsa.2008.01.031 ↩
- Kozin SH, Zlotolow DA. Madelung Deformity. J Hand Surg Am. 2015;40(10):2090-2098. doi:10.1016/j.jhsa.2015.03.033 ↩
- Babu S, Turner J, Seewoonarain S, Chougule S. Madelung’s Deformity of the Wrist-Current Concepts and Future Directions. J Wrist Surg. 2019;8(3):176-179. doi:10.1055/s-0039-1685488 ↩
- Cook PA, Yu JS, Wiand W, Lubbers L, Coleman CR, Cook AJ, 2nd, et al. Madelung deformity in skeletally immature patients: morphologic assessment using radiography, CT, and MRI. J Comput Assist Tomogr. 1996;20(4):505-511. doi:10.1097/00004728-199607000-00001 ↩
- Stehling C, Langer M, Nassenstein I, Bachmann R, Heindel W, Vieth V. High resolution 3.0 Tesla MR imaging findings in patients with bilateral Madelung’s deformity. Surg Radiol Anat. 2009;31(7):551-557. doi:10.1007/s00276-009-0476-0 ↩
- Hanson TJ, Murthy NS, Shin AY, Kakar S, Collins MS. MRI appearance of the anomalous volar radiotriquetral ligament in true Madelung deformity. Skeletal Radiol. 2019;48(6):915-918. doi:10.1007/s00256-018-3094-2 ↩
- De Leucio A, Castelein S, Bellemans M, Simoni P. Radiotriquetral Ligament in Madelung’s Deformity Associated with Leri-Weill’s Dyschondrosteosis. Cureus. 2020;12(2):e7100. doi:10.7759/cureus.7100 ↩
- Ghatan AC, Hanel DP. Madelung deformity. J Am Acad Orthop Surg. 2013;21(6):372-382. doi:10.5435/JAAOS-21-06-372 ↩
- Dang Y, Du X, Ou X, Zheng Q, Xie F. Advances in diagnosis and treatment of Madelung’s deformity. Am J Transl Res. 2023;15(7):4416-4424. ↩
- Huguet S, Leheup B, Aslan M, Muller F, Dautel G, Journeau P, et al. Radiological and clinical analysis of Madelung’s deformity in children. Orthop Traumatol Surg Res. 2014;100(6 Suppl):S349-352. doi:10.1016/j.otsr.2014.06.007 ↩
- Ali S, Kaplan S, Kaufman T, Fenerty S, Kozin S, Zlotolow DA. Madelung deformity and Madelung-type deformities: a review of the clinical and radiological characteristics. Pediatr Radiol. 2015;45(12):1856-1863. doi:10.1007/s00247-015-3390-0 ↩
- Knutsen EJ, Goldfarb CA. Madelung’s Deformity. Hand (N Y). 2014;9(3):289-291. doi:10.1007/s11552-014-9633-y ↩
- Farr S, Zlotolow DA, Bachy M, Peymani A, Hulsemann W, Winge MI. State of the art review: The pathogenesis and management of Madelung deformity. J Hand Surg Eur Vol. 2023;48(11):1116-1125. doi:10.1177/17531934231191208 ↩
- Zebala LP, Manske PR, Goldfarb CA. Madelung’s deformity: a spectrum of presentation. J Hand Surg Am. 2007;32(9):1393-1401. doi:10.1016/j.jhsa.2007.08.012 ↩
- Ducloyer P, Leclercq C, Lisfranc R, Saffar P. Spontaneous ruptures of the extensor tendons of the fingers in Madelung’s deformity. J Hand Surg Br. 1991;16(3):329-333. doi:10.1016/0266-7681(91)90064-u ↩
- Jebson PJ, Blair WF. Bilateral spontaneous extensor tendon ruptures in Madelung’s deformity. J Hand Surg Am. 1992;17(2):277-280. doi:10.1016/0363-5023(92)90405-e ↩
- McCarroll HR, Jr., James MA, Newmeyer WL, 3rd, Manske PR. Madelung’s deformity: diagnostic thresholds of radiographic measurements. J Hand Surg Am. 2010;35(5):807-812. doi:10.1016/j.jhsa.2010.02.003 ↩
- McCarroll HR, Jr., James MA, Newmeyer WL, 3rd, Molitor F, Manske PR. Madelung’s deformity: quantitative assessment of x-ray deformity. J Hand Surg Am. 2005;30(6):1211-1220. doi:10.1016/j.jhsa.2005.06.024 ↩
- McCarroll HR, James MA, Newmeyer WL, 3rd, Manske PR. Madelung’s deformity: quantitative radiographic comparison with normal wrists. J Hand Surg Eur Vol. 2008;33(5):632-635. doi:10.1177/1753193408092496 ↩
- Farr S, Guitton TG, Ring D, Science of Variation G. How Reliable is the Radiographic Diagnosis of Mild Madelung Deformity? J Wrist Surg. 2018;7(3):227-231. doi:10.1055/s-0037-1612636 ↩
- Shahi P, Sudan A, Sehgal A, Meher D, Meena U. Madelung Deformity of the Wrist Managed Conservatively. Cureus. 2020;12(5):e8225. doi:10.7759/cureus.8225 ↩
- Bebing M, de Courtivron B, Pannier S, Journeau P, Fitoussi F, Morin C, et al. Madelung’s deformity in children: Clinical and radiological results from a French national multicentre retrospective study. Orthop Traumatol Surg Res. 2020;106(7):1339-1343. doi:10.1016/j.otsr.2020.03.036 ↩
- Otte JE, Popp JE, Samora JB. Treatment of Madelung Deformity With Vicker Ligament Release and Radial Physiolyses: A Case Series. J Hand Surg Am. 2019;44(2):158 e151-158 e159. doi:10.1016/j.jhsa.2018.04.033 ↩
- Steinman S, Oishi S, Mills J, Bush P, Wheeler L, Ezaki M. Volar ligament release and distal radial dome osteotomy for the correction of Madelung deformity: long-term follow-up. J Bone Joint Surg Am. 2013;95(13):1198-1204. doi:10.2106/JBJS.L.00714 ↩
- Field JS, Rizzo M. Madelung deformity with prior distal radius fracture: a case report. Am J Orthop (Belle Mead NJ). 2007;36(6):E91-93. ↩
- Sifuentes Giraldo WA, Gamir Gamir ML. Acquired Madelung’s deformity in rheumatoid factor-positive polyarticular juvenile idiopathic arthritis. Reumatol Clin. 2014;10(4):266-267. doi:10.1016/j.reuma.2013.11.008 ↩
