Clinical History: A 45 year-old woman with a history of arthritis presents with progressive wrist pain. Fat-suppressed proton density-weighted axial (1a), fat-suppressed T2-weighted coronal (1b), and proton density-weighted sagittal (1c,1d) images are provided. What are the findings? What is your diagnosis?

1a

1b

1c

1d
Figure 1:
Fat-suppressed proton density-weighted axial (1a), fat-suppressed T2-weighted coronal (1b), and proton density-weighted sagittal (1c,1d) images.
Findings

2a
Figure 2:
Fat-suppressed proton density-weighted axial image reveals an increased interosseous space between the lunate (L) and capitate (C) bones in the region of the midcarpal joint space, suggesting injury.

3a
Figure 3:
Fat-suppressed T2-weighted coronal image of the wrist confirms a large fluid-filled gap in the region of the midcarpal joint (arrow), indicating abnormal widening of the joint.

4a
Figure 4:
Proton density-weighted sagittal image of the wrist demonstrates dorsal tilt of the lunate bone (L) with the lunate axis depicted by the red line. The capitate bone (C) demonstrates marked dorsal subluxation (arrowhead).

5a
Figure 5:
Proton density-weighted sagittal image of the wrist demonstrate marked dorsal angulation of the scaphoid bone (S) with the scaphoid axis depicted by the blue line.
Diagnosis
Midcarpal instability nondissociative, dorsal type.
Introduction
Carpal instability remains a complex topic, in part related to many different patterns of instability and also to the existence of countless intrinsic and extrinsic ligaments. Such instability relates to biomechanical alterations with multiple causes that, if not identified and treated in a timely fashion, will lead to gradual articular collapse. Knowledge of normal wrist anatomy is important for the proper diagnosis and treatment of carpal instability. (A list of abbreviations used in this Web Clinic may be found at the end of the text).
Anatomy
The wrist is not a single joint but is composed of many articulations with the carpal bones arranged in two rows, proximal and distal. The proximal carpal row consists of the scaphoid, lunate, and triquetrum, which articulate with the distal ends of the radius and ulna. The distal carpal row consists of the trapezium, trapezoid, capitate, and hamate. An additional carpal bone, the pisiform, acts as a sesamoid, providing an attachment for the flexor carpi ulnaris tendon.1
The radiocarpal joint is formed, in part, by the distal articular surface of the radius and the convexities of the scaphoid and lunate bones. The distal articular surface of the radius is biconcave with an average tilt of 10 degrees in the sagittal plane and ulnar inclination of 24 degrees in the frontal plane.2 The midcarpal joint is formed laterally by the scaphotrapeziotrapezoid (STT) space and the scaphocapitate space, centrally by the lunocapitate space, and medially by the triquetral-hamate space.3
Most of the wrist ligaments are intracapsular, except for the transverse carpal ligament and two ligaments attaching to the pisiform (i.e., pisohamate and pisometacarpal ligaments). There are two categories of intracapsular ligaments, extrinsic and intrinsic. Extrinsic ligaments connect the forearm bones (i.e. radius and ulna) with the carpal bones, while intrinsic ligaments connect two or more carpal bones (6a,7a,8a).

6a
Figure 6:
3D graphic representation of the volar ligaments with the most superficial ligaments labeled includes the radioscaphoid (RS), radioscaphocapitate (RSC), long radiolunate (LRL), ulnocapitate (UC), and pisohamate (PH) ligaments.

7a
Figure 7:
3D graphic representation with the superficial ligaments removed reveals the deep volar ligaments, including the scapholunate (SLIL) and lunotriquetral (LTIL) interosseous ligaments. Additional ligaments include the short radiolunate (SRL), ulnolunate (UL), ulnotriquetral (UT), triquetro-hamate-capitate (THC), triquetrohamate (TH), scaphocapitate (SC), scaphotrapeziotrapezoid (STT), capitotrapezoid (CT), and capitohamate (CH). The radioscapholunate (RSL) ligament (not a true ligament) is also indicated.

8a
Figure 8:
3D graphic representation demonstrates the main dorsal ligaments, the dorsal radiotriquetral (DRT) and dorsal intercarpal (DIC) ligaments.
The intrinsic ligaments include the scapholunate interosseous ligament (SLIL), lunotriquetral interosseous ligament (LTIL), midcarpal ligaments, and distal carpal row interosseous ligaments. The intrinsic ligaments demonstrate higher yield strength than the extrinsic ligaments and often fail through avulsion at their attachment sites.1 The dorsal portion of the SLIL and the volar portion of the LTIL are the strongest. With regard to the midcarpal ligaments, the triquetro-hamate-capitate (THC) and scaphocapitate (SC) ligaments are most important, together bridging the midcarpal joint as the arcuate ligament (9a). There is no distinct capsular ligament on the volar aspect of the wrist that connects the lunate and the capitate bones. This relatively weak region of the capsule is designated the space of Poirier. The distal carpal row interosseous ligaments are particularly important in the protection of the carpal tunnel contents.4

9a
Figure 9:
Fat-suppressed T1 weighted MR arthrogram coronal image of the deep volar aspect of the wrist demonstrates the two limbs of the arcuate ligament: the THC ligament (arrow) and the SC ligament (arrowhead). The distal pole of the scaphoid (S), triquetrum (T), and lunate (L) are also indicated.
The extrinsic ligaments may be further divided into the palmar and dorsal ligaments. There are several important extrinsic palmar radiocarpal and ulnocarpal ligaments: radioscaphocapitate (RSC), long radiolunate (LRL) or radiolunotriquetral, radioscaphoid (RS), short radiolunate (SRL), ulnocapitate (UC), ulnolunate (UL), and ulnotriquetral (UT) ligaments. The RSC and LRL ligaments can be identified on routine MR imaging (10a).

10a
Figure 10:
Fat-suppressed T1-weighted MR arthrogram coronal image of the wrist demonstrates the extrinsic RSC (blue bracket) and LRL (red bracket) ligaments. It is sometimes difficult to separate these two ligaments on MR images, however, as they may appear as one or more bands of tissue bridging the radio-volar portion of the radiocarpal joint. The distal pole of the scaphoid (S) and lunate (L) are also indicated.
The UC and RSC ligaments form the deltoid ligament, which is superficial to the arcuate ligament (11a).

11a
Figure 11:
Fat-suppressed T1-weighted MR arthrogram coronal image of the superficial volar aspect of the wrist demonstrates the two limbs of the deltoid ligament, which consists of the RSC ligament (arrow) and the UC ligament (arrowhead), the latter not well seen on this image.
The dorsal radiocarpal ligaments are less important than the palmar radiocarpal ligaments, although note should be made of the dorsal radiotriquetral (DRT) ligament which is a wide, fan-shaped ligament that connects the dorsal surfaces of the radius and the triquetrum.5
Biomechanics and Pathomechanics
Motion of the wrist occurs either passively by an external force or actively by muscle contraction. Wrist kinematics (dynamic movement of components of the carpus) and kinetics (ability to sustain high physiologic loads) are made possible by the interaction among tendons, ligaments, and joint surfaces.1 Since the bones of the proximal carpal row have no direct tendon attachments, movement is generated by muscle contraction initiated at the distal carpal row with the proximal row following passively, with most movement occurring at the capitolunate portion of the midcarpal joint. During radial and ulnar deviation, the proximal carpal bones move synergistically from a flexed position in radial deviation to an extended position in ulnar deviation. During flexion, the distal row synchronously rotates into flexion, but with some degree of ulnar deviation; during extension, the distal row extends with slight radial deviation. These movements allow the so-called “dart-throwing” motion, which combines radial and ulnar translocation of the proximal carpal row with flexion and extension at the radiocarpal joint.6 This movement plays a vital role in daily activities, and it is this mechanism that is affected in midcarpal instability, described below.
Stability of the wrist can be affected at any level, including the radiocarpal joint, midcarpal joint, distal carpal row, and proximal carpal row. Any injury or disease modifying bone geometry, articular inclination, ligament integrity, or muscle function may alter carpal motion, leading to carpal instability.1 The obliquity of the palmar and dorsal radiocarpal ligaments helps protect against the inherent tendency of the carpus to translate ulnarly and palmary, thereby stabilizing the radiocarpal joint.7 Especially important midcarpal stabilizers are the STT joint, the SC ligament laterally, and the THC ligament medially.8 Failure of these ligaments results in a distinctive pattern of carpal collapse characterized by abnormal flexion of the unconstrained proximal row and known as volar intercalated segment instability (VISI). In this pattern of sagittal malalignment, there is volar tilt of the lunate and scaphoid and dorsal tilt of the capitate, with the distal articular surface of the lunate facing toward the palm. An important stabilizer of the proximal row is the SLIL; when this ligament is torn, the scaphoid is no longer constrained by the rest of the proximal row, resulting in dorsal intercalated segment instability (DISI).1 On sagittal views, there is resultant volar tilt of the scaphoid and dorsal tilt of the lunate. DISI and VISI are two of the most common malalignment patterns in carpal instability and are best identified in the lateral projection (12a).

12a
Figure 12:
The capitolunate (CL) and scapholunate (SL) angles can help distinguish between DISI and VISI patterns in a standard lateral radiographic projection. The SL angle is the angle created by a line drawn tangential to the volar border of the scaphoid (S) and another line bisecting the lunate that is drawn perpendicular to its long axis (L). The CL angle is the angle created by a vertical line drawn through the capitate bone along its long axis (C) and another line bisecting the lunate that is drawn perpendicular to its long axis (L). In normal alignment, the SL angle is between 30° - 60°, and the long axis of the capitate and lunate is linear (CL = 0). In DISI, both the SL and CL angles are increased (SL > 60° , CL > 30°). In VISI, the SL angle is decreased (SL < 30°) and the CL angle is increased (> 30°).
Diagnosis
Patients presenting with carpal instability may or may not have had a prior traumatic event. The first line of imaging is conventional radiography. Radiographs allow the measurement of the SL and CL angles as previously described, as well as ulnar variance, radiolunate (RL) angle, and carpal height ratio. Further evaluation in some cases includes CT and MRI with or without arthrography. MRI demonstrates a sensitivity and specificity of 63% and 86%, respectively, in the diagnosis of SLIL injury.9 Stress testing and physical examination remain valuable in the diagnosis of carpal instability, although imaging and arthroscopy also provide important roles in the precise diagnosis.
Classification of Carpal Instability
Classification of carpal instability has evolved during the past 20 years. The Mayo classification (Table 1) divides carpal instability into four major categories:
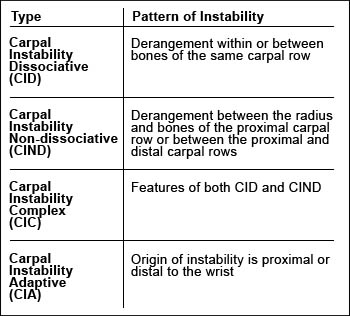
Table 1
Carpal instability-Mayo classification
CARPAL INSTABILITY DISSOCIATIVE (CID)
Carpal instability dissociative (CID) involves a derangement within or between bones of the same carpal row. This may involve the proximal carpal row, four examples of which are scapholunate dissociation (SLD), lunotriquetral dissociation, scaphoid fracture, and Kienbock’s disease; or the distal carpal row, so-called axial carpal dislocations. The most common instability pattern in this group is SLD, which is typically caused by an injury that leads to hyperextension and ulnar deviation of the wrist. This results in static carpal collapse with volar flexion of the scaphoid and dorsal tilt of the lunate.
Scapholunate dissociation
Scapholunate dissociation (SLD) refers to disruption of the mechanical linkage between the scaphoid and the lunate.10 SLD is the most frequent carpal instability pattern and may appear either as an isolated injury or in association with distal radial fractures or displaced scaphoid fractures. Rotary subluxation of the scaphoid represents an advanced stage of this injury,11 in which the ligaments attaching to both ends of the scaphoid have failed (13a), and the scaphoid bone has collapsed into flexion and pronation. If there is a concomitant failure of the scaphoid stabilizers, the palmar RSC and SC ligaments and the anterolateral STT ligament, permanent carpal malalignment occurs.12 A DISI deformity ensues, as the scaphoid tilts volarly and the lunate tilts dorsally (14a).

13a
Figure 13:
Fat suppressed T2-weighted coronal image demonstrate failure of the ligaments at both ends of the scaphoid (red arrows), with an increased scapholunate space, measuring more than 4.5 mm (arrowhead).

14a
Figure 14:
On the left, a T1-weighted sagittal image through the scaphoid demonstrates a volarly tilted scaphoid axis (blue line). The proximal pole of the scaphoid "rides" on the dorsal rim of the distal radial articular surface (arrowhead). On the right, a T1-weighted sagittal image through the lunate in the same patient demonstrates a dorsally tilted lunate axis (red line).The scapholunate angle is 90°, and the findings are compatible with DISI resulting from scapholunate dissociation.
Scapholunate advanced collapse (SLAC) is a clinical condition in which there have been progressive degenerative changes resulting from chronic SLD. This distinctive arthropathy is characterized by severe RS space narrowing followed by progressive proximal migration of the capitate bone (15a) that migrates between the scaphoid and the lunate.11

15a
Figure 15:
T1-weighted coronal image demonstrates severe narrowing of the RS joint (arrow) with severe degenerative changes, including subarticular sclerotic bony change and remodeling. The capitate demonstrates significant proximal migration into the abnormally widened SL interosseous space (arrowhead), compatible with SLAC.
The clinical diagnosis of SLD is established by a positive scaphoid shift test.13 On this test, firm pressure is applied to the palmar tuberosity of the scaphoid while the wrist is moved from ulnar to radial deviation. If the SLIL is torn, the proximal pole of the scaphoid subluxes dorsally with respect to the radius, producing pain on the dorsoradial aspect of the wrist. When pressure is released, the scaphoid assumes a normal position and a typical snapping occurs. Imaging reveals an increased SL space,14 characterized by a widened and irregular SL interosseous gap of more than 4.5 mm, lack of parallelism of the scaphoid and lunate bones in coronal images and accumulation of fluid adjacent to the torn ligament or an absent ligament. In sagittal images, the appearance of DISI should raise suspicion of SLD.10
Lunotriquetral dissociation
Causes for lunotriquetral dissociation (LTD) include trauma or ulnocarpal abutment, with a frequent association with triangular fibrocartilage complex lesions.15 Most isolated injuries to the LTIL occur secondary to a fall backward on an outstretched hand, with the arm externally rotated, the forearm supinated, and the wrist extended and radially deviated. With LTD, slight dorsal translation of the lunate is caused by flexion of the scaphoid, which is attached to the lunate via an intact SLIL, resulting in a VISI deformity.
The accuracy of MRI in the diagnosis of a torn LTIL is only about 50%. An indirect sign is accumulation of fluid about the torn ligament.
CARPAL INSTABILITY NONDISSOCIATIVE (CIND)
CIND is defined as symptomatic carpal dysfunction between the radius and the proximal row or between the proximal and distal carpal rows, without disruption within or between the bones of the proximal or distal carpal row.16 CIND is subdivided into radiocarpal and midcarpal patterns.17,18
Radiocarpal CIND relates to insufficiency or disruption of the obliquely orientated extrinsic radiocarpal ligaments, allowing the proximal row to slide ulnarly along the sloping articular surface of the distal portion of the radius.7,19 Radiocarpal CIND is seen in a variety of conditions, such as rheumatoid arthritis or developmental abnormalities including Madelung’s deformity, following surgical excision of the distal ulna, or after an injury.21 The three most common forms of radiocarpal CIND are ulnar translocation, radial translocation, and pure radiocarpal dislocation.
Ulnar translocation
With ulnar translocation, a portion of or the entire proximal carpal row slides in an ulnar direction along the sloping distal articular surface of the radius. Hyperextension, pronation and ulnar deviation of the wrist on a fixed hand at the time of injury may produce this instability pattern.
Taleisnik reported two types of ulnar translocation.19 In type I (16a), the entire carpus, including the scaphoid, is displaced in an ulnar direction, typically related to the failure of RS and RSC ligaments, and the distance between the radial styloid process and the scaphoid is widened (17a). In type II ulnar translocation, the scaphoid and the radius remain in their anatomic position, and the other carpal bones move in an ulnar direction as a unit, causing a markedly increased scapholunate interval (18a,19a).17

16a
Figure 16:
Pattern of ulnar translocation - type I: Widening of the radial styloid-scaphoid space (red arrow), with tearing of the RSC (yellow asterisk), RS (blue asterisk), and LRL (green asterisk) ligaments. The SL interosseous space remains intact. The entire carpus is translocated in an ulnar direction (blue arrow).

17a
Figure 17:
T1-weighted coronal image demonstrates ulnar translocation of the entire carpus in a patient with suspected rheumatoid arthritis. The distance between the radial styloid and scaphoid is widened (arrow), and more than 50% of the proximal lunate articulates solely with the distal ulna (asterisk). The SL interosseous space is not widened (arrowhead). The intercarpal, radioscaphoid, ulnolunate, and midcarpal spaces are narrowed, resulting in loss of carpal height.

18a
Figure 18:
Pattern of ulnar translocation - type II: both the RSC (yellow asterisk) and RS (blue asterisk) ligaments are intact, with complete disruption of the SLIL (red arrowheads) and LRL (green asterisk). Only the lunate, triquetrum, and pisiform are translocated in an ulnar direction (blue arrow). This pattern of ulnar translocation, in reality, represents a severe form of scapholunate dissociation and carries a worse prognosis.

19a
Figure 19:
T1-weighted coronal image demonstrates ulnar translocation of only the lunate (L) and triquetrum (T) bones (pisiform bone is not depicted on this image). The SLIL is torn, and the scapholunate space is widened (arrowhead). The scaphoid bone (S) remains in its native position.
Midcarpal instability nondissociative (or midcarpal instability; MCI)
Midcarpal instability is related to dysfunction of both the radiocarpal and midcarpal joints (with predominance of midcarpal joint involvement). Especially important stabilizers of this joint are the THC ligament, dorsolateral STT ligament, and RSC ligament, as these ligaments cross the midcarpal joint.1 There are four major types of midcarpal instability: palmar, dorsal, combined, and extrinsic (20a).

20a
Figure 20:
The four types of midcarpal instability. Palmar (I) - entire proximal row appears abnomally flexed (red curved arrows). Dorsal (II) - dorsal tilt of lunate and scaphoid with dorsal subluxation of capitate (blue arrow). Combined (III) - exaggeration of the dorsal pattern with additional dorsal subluxation of the lunate and scaphoid (blue arrow). Extrinsic (IV) - dorsal tilt of the radius from prior fracture resulting in similar dorsal tilt of the lunate and dorsal subluxation of the capitate.
In palmar MCI, the entire proximal carpal row flexes volarly leading to a VISI pattern, related to failure of those intrinsic ligaments that cross the midcarpal joint. The primary ligament injured in this pattern is the THC ligament, with additional insufficiency of the dorsal radiocarpal ligament. Dorsal MCI usually presents in young patients with bilateral hypermobile wrists.1 It is characterized by dorsal subluxation of the capitate and dorsal tilting of the scaphoid and lunate, related to additional failure of the volar RSC ligament.
Combined MCI is characterized by an exaggerated dorsal MCI with additional dorsal subluxation of the lunate, scaphoid, and capitate. Extrinsic MCI results from a malunited fracture of the distal radius with resultant dorsal tilting of the articular surface with subsequent similar dorsal tilt of the lunate.
CARPAL INSTABILITY COMPLEX (CIC)
When the carpal derangement has altered the relationship both (a) between bones within the same carpal row (CID features) and (b) between the proximal and distal carpal rows (CIND features), the dysfunction is categorized as a CIC. Five groups of CIC have been identified.
- Dorsal perilunate dislocation (lesser arc injury)
- Dorsal perilunate fracture-dislocation (greater arc injury)
- Palmar perilunate dislocation (lesser or greater arc injury)
- Axial dislocation
- Isolated carpal bone dislocation
Pure ligamentous injuries of the wrist are classified as lesser arc injuries, while the transosseous variants are regarded as greater arc injuries, in which one or several bones around the lunate have a concomitant fracture.
The first two groups have in common a carpal derangement occurring around the lunate, the first group characterized as a lesser arc injury and the second group regarded as a greater arc injury. The third group, although perilunate, results from a different mechanism producing palmar displacement of the distal carpal row relative to the lunate. The fourth and fifth groups represent various non-perilunate dislocations, usually the result of high-energy trauma.1
Dorsal perilunate dislocation (lesser arc injury)
Different forms of carpal injury exist under the pattern of dorsal perilunate dislocation, confined to a relatively vulnerable area around the lunate. Along with the scapholunate injuries, dorsal perilunate dislocations are one of the most common injuries seen; the lunate remains within the lunate fossa of the radius while the remainder of the carpus displaces dorsally. As part of a lesser arc injury, this pattern is a pure dislocation without an associated fracture.
Mayfield et al reported four stages of progressive perilunate instability (21a-24a).20

21a
Figure 21:
Stage I perilunate dislocation.
Progressive perilunate instability. Schematic representation of the four stages of perilunate instability (21a-24a), viewed from the ulnar side. The numbers in the diagrams correspond to the numbers used in the text descriptions of each stage after each image. The red arrows depict the distraction forces occurring in the ligaments.
Stage I: As the distal carpal row is forced into hyperextension (blue arrow), the scaphotrapeziocapitate ligament [1] pulls the scaphoid into extension, thus opening the space of Poirier (red asterisk). The lunate cannot extend as much as the scaphoid, because it is directly constrained by the SRL [2]. When the SL torque reaches a certain level, the SLIL ligament may fail, usually on a palmar to dorsal direction. SLD is defined by the disruption of the dorsal SLIL [3]. (21a)

22a
Figure 22:
Stage II peirlunate dislocation.
Stage II: The scaphoid-capitate row complex may dislocate dorsal to the lunate as it is dissociated from the lunate. The extent of this dorsal translation (blue arrow) is determined by the RSC ligament [4]. The entire distal row and the dissociated radial portion of the proximal row follow the capitate dorsally, further opening the space of Poirier. (22a)

23a
Figure 23:
Stage III perilunate dislocation.
Stage III: If hyperextension persists (blue arrow), the ulnar limb (i.e., THC ligament) of the arcuate ligament [5] may pull the triquetrum into abnormal extension. As the triquetrum extends, this torque is transmitted to the LTIL. A tear of the LTIL or an avulsion fracture of the triquetrum may result. With complete disruption of the LTIL [6], the ulnar expansions of the LRL ligament also tears, leaving the SRL [2] ligament and the volar UL ligament as the only stabilizing forces on the lunate. (23a,25a,26a).

24a
Figure 24:
Stage IV perilunate dislocation.
Stage IV: Finally, the dorsally displaced capitate may be pulled proximally and volarly (blue arrows) into the radiocarpal space by a still-intact RSC [4] ligament. The capitate pushes the lunate volarly, causing it to hinge on the still intact SRL [2] and displace volarly through the space of Poirier in a rotary fashion. Thus, lunate dislocation is the end stage of a dorsal perilunate dislocation (24a,25a,26a).

25a
Figure 25:
T1-weighted sagittal image demonstrates stage IV of progressive perilunate instability, with severe volar lunate (L) subluxation. The lunate still articulates with the distal radius as the short radiolunate ligament remains intact (arrow), however, there is dislocation of the lunocapitate articulation (arrowhead).

26a
Figure 26:
T1-weighted sagittal image demonstrates volar displacement of the lunate (L); known as the "spilled teacup sign," the lunate on-end resembling a tipped cup. In addition, the capitate (C) is seen dorsal to the lunate. Note in this case, the volar ulnolunate ligament is also intact (arrow), providing another stabilizing force on the lunate.

27a
Figure 27:
Gradient echo coronal image depicts the intact volar ulnolunate (arrow). Note that the lunate (L) has an appearance of a "piece of pie", and appears more volar than the remaining bones of the proximal carpal row.
Dorsal perilunate fracture-dislocation (greater arc injury)
Dorsal perilunate fracture-dislocations refer to perilunate dislocation with concomitant fracture of either the scaphoid, capitate, hamate, or triquetrum bones. The only true greater arc injury is a trans-scaphoid, transcapitate, transtriquetral, and transhamate perilunate fracture-dislocation. All other perilunate fracture-dislocations involve ligament ruptures, bone avulsions, and additional fractures. The most common form of greater arc injury is a trans-scaphoid perilunate dislocation.
CARPAL INSTABILITY ADAPTIVE (CIA)
Carpal dysfunction is not always the consequence of intracarpal pathology, but it can also result from extracarpal pathology.1 A typical example of CIA is malunion of a distal radial fracture that has induced a postural adaption of the proximal carpal row to conform to the abnormal radial tilt (28a). Another example may result from a Madelung’s deformity, where there is volar tilt of the distal radius and an elongated, dorsally subluxed ulna, with adaptive changes of the bones of the proximal carpal row.23 For the diagnosis of CIA to be made, it is important to exclude significant intracarpal ligament injury, which aids in its differentiation from extrinsic MCI in which there is typically significant injury to ligaments crossing the midcarpal joint. However these patterns are still very similar, and it may be difficult to differentiate between the two, as extracarpal pathology is common to both. Treatment is directed at correction of the malunion.24,25

28a
Figure 28:
T1-weighted sagittal image of the wrist reveals post-traumatic deformity of the distal radius with dorsal inclination of the articular surface (arrow). There is additional dorsal tilting of the lunate bone (asterisk). These findings are compatible with carpal instability adaptive.
Principles of Treatment
A description of treatment of carpal instability is beyond the scope of this review and is dependent on the specific type of carpal instability. The basic determinants of the treatment include the presence or absence of arthritic changes, chronicity of injury, quality of tissues that need to be repaired, and reducibility of deformity.26
In a relatively acute injury with good quality of soft tissues and reducible deformity, the principles of treatment include the restoration of normal anatomy whenever possible. This implies ligament repair, restoration of normal carpal angles, and anatomic reconstruction. In similar cases where tissue quality is poor, ligament reconstruction or salvage procedures are considered. Salvage procedure include intercarpal arthrodesis or total wrist arthrodesis.
Conclusion
Carpal instability is often a confusing and challenging topic, whose understanding requires a basic knowledge of anatomy and pathophysiology. Such knowledge can then be applied to the analysis of imaging studies, including MRI, allowing a more complete and meaningful diagnosis in cases of wrist instability. Specifically, understanding the classification system of wrist instability that is currently being used by many hand surgeons will promote a more meaningful conversation between the radiologist and the referring physician.
Abbreviations
CH – CAPITOHAMATE
CL – CAPITOLUNATE
CT – CAPITOTRAPEZOID
DIC – DORSAL INTERCARPAL
DISI – DORSAL INTERCALATED SEGMENT INSTABILITY
DRT – DORSAL RADIOTRIQUETRAL
LRL – LONG RADIOLUNATE (aka RADIOLUNOTRIQUETRAL)
LTD – LUNOTRIQUETRAL DISSOCIATION
LTIL – LUNOTRIQUETRAL INTEROSSEOUS LIGAMENT
RL – RADIOLUNATE
RS – RADIOSCAPHOID
RSC – RADIOSCAPHOCAPITATE
RSL – RADIOSCAPHOLUNATE LIGAMENT
SC – SCAPHOCAPITATE
SL – SCAPHOLUNATE
SLD – SCAPHOLUNATE DISSOCIATION
SLIL – SCAPHOLUNATE INTEROSSESOUS LIGAMENT
SRL – SHORT RADIOLUNATE
STT – SCAPHOTRAPEZIOTRAPEZOID
TH – TRIQUETROHAMATE
THC – TRIQUETRO-HAMATE-CAPITATE
UC – ULNOCAPITATE
UL – ULNOLUNATE
VISI – VOLAR INTERCALATED SEGMENT INSTABILITY
References
1 Garcia-Elias M, Geissler WB. Carpal instability. In: Green DP, Hotchkiss RN, Pederson WC, et al, editors. Operative hand surgery. 5th edition. Philadelphia: Elsevier; 2005. p. 465-520.
2 Schuind FA, Linscheid RL, et al. A normal database of posteroanterior roentgenographic measurements of the wrist. J Bone Joint Surg Am 1992;74:1418-1429.
3 Moritomo H, Apergis E, et al. IFSSH Committee report of wrist biomechanics committee: biomechanics of the so-called dart-throwing motion of the wrist. J Hand Surg [Am] 2007;32:1447-1453.
4 Garcia-Elias M, Dobyns JH, et al. Traumatic axial dislocations of the carpus. J Hand Surg [Am] 1989;14:446-457.
5 Berger RA. The ligaments of the wrist: a current overview of anatomy with considerations of their potential functions. Hand Clin 1997;13:63-82.
6 Toms A, Chojnowski, et al. Midcarpal instability: a radiologic perspective. Skeletal Radiol 2011;40:533-541.
7 Rayhack JM, Linscheid RL, et al. Posttraumatic ulnar translation of the carpus. J Hand Surg [Am] 1987;12:180-189.
8 Lichtman DM, Wroten ES. Understanding midcarpal instability. J Hand Surg [Am] 2006;31:491-498.
9 Morley J, Bidwell J, et al. A comparison of the findings of wrist arthroscopy and magnetic resonance imaging in the investigation of wrist pain. J Hand Surg [Br] 2001;26:544-546.
10 Linscheid RL, Dobyns JH, Beabout JW, et al. Traumatic instability of the wrist: diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 1972;54:1612-1632.
11 Watson HK, Weinzweig J, Zeppieri J. The natural progression of scaphoid instability. Hand Clin 1997;13:39-49.
12 Short WH, Werner FW, Green JK, et al. Biomechanical evaluation of ligamentous stabilizers of the scaphoid and lunate: Part III. J Hand Surg (Am) 2007;32:297-309.
13 Watson HK, Ashmead D IV, Makhlouf MV. Examination of the scaphoid. Hand Surg (Am) 1988;13:657-660.
14 Schimmerl-Metz SM, Metz VM, Totterman SMS, et al. Radiologic measurement of the scapholunate joint: implications of biologic variation in scapholunate joint morphology. J Hand Surg (Am) 1999;24:1237-1244.
15 Shin AY, Weinstein LP, Berger RA, et al: Treatment of isolated injuries of the lunotriquetral ligament: comparison of arthrodesis, ligament reconstruction and ligament repair. J Bone Joint Surg Br 2001;83:1023-1028.
16 Wright TW, Dobyns JH, Linscheid RL et al. Carpal instability non-dissociative. J Hand Surg (Br) 1994;19:763-773.
17 Resnick D, Heung KS, et al. Internal Derangement of Joints, 2nd edition. Philadelphia: W. B. Saunders; 2006.
18 Dobyns JH, Linsheid RL, Chao EY, Weber, ER, et al. Traumatic instability of the wrist. In Instructional Course Lectures, The American Academy of Orthopaedic Surgeons, Vol. 24. St. Louis: C. V. Mosby;1975. p. 182-199.
19 Taleisnik J. The wrist. New York: Churchill Livingstone;1985.
20 Mayfield JK, Johnson RP, Kilcoyne RK. Carpal dislocations: pathomechanics and progressive perilunar instability. J Hand Surg 1980;5:226-241.
21 Cooney WP, Dobyns JH, Linscheid RL. Complications of Colles’ fractures. J Bone Joint Surg Am 1980;62(4):613-619.
22 Cooney, W.P. External fixation of distal radius fractures. Clin Orthop 1983;180:44-49.
23 Taleisnik J, Watson HK. Midcarpal instability caused by malunited fractures of the distal radius. J Hand Surg 1984;9A:350-357.
24 Carlsen BT, Shin AY. Wrist instability. Scand J Surg 2008;97(4):324-32.
