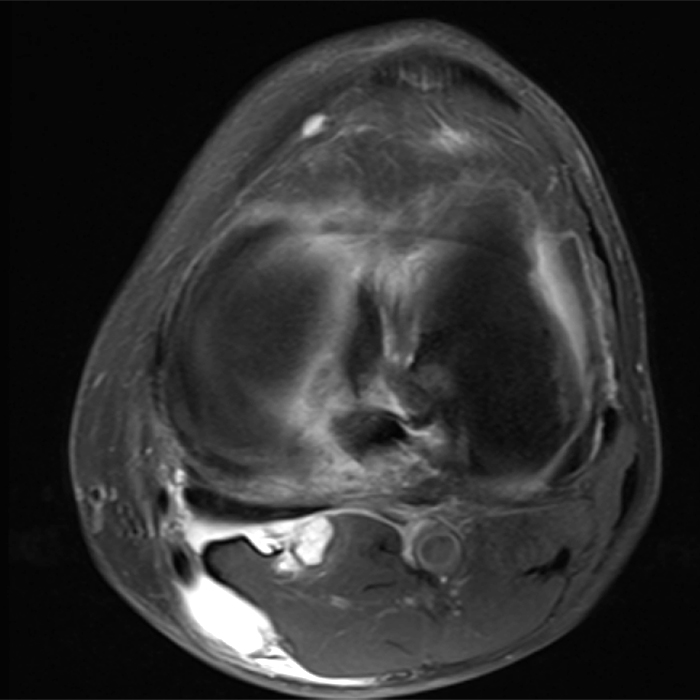
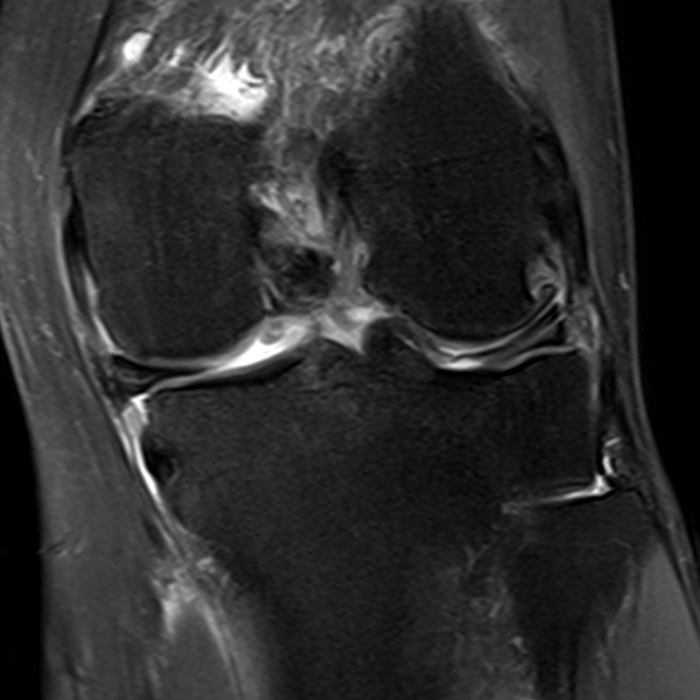
Clinical History: A 61-year-old female presents with left posteromedial and posterolateral knee pain for three weeks after hyperextending the knee while lying in bed. The pain was gradually resolving when she suffered a misstep off the sidewalk and a twisting injury two days before presentation. Axial (1A), contiguous coronal (1B), contiguous sagittal (1C), contiguous sagittal (1D), and coronal (1E) fat-suppressed proton-density-weighted images of the knee are provided. What are the findings? What is your diagnosis?
Findings
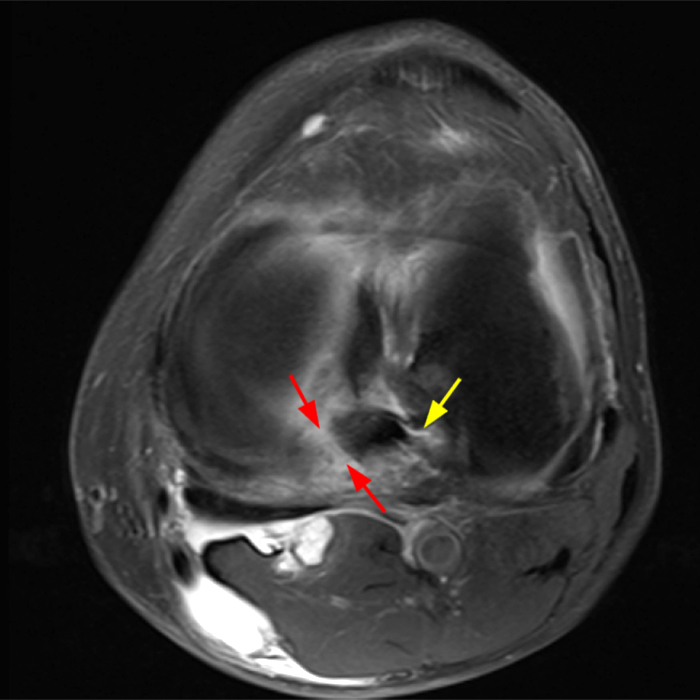
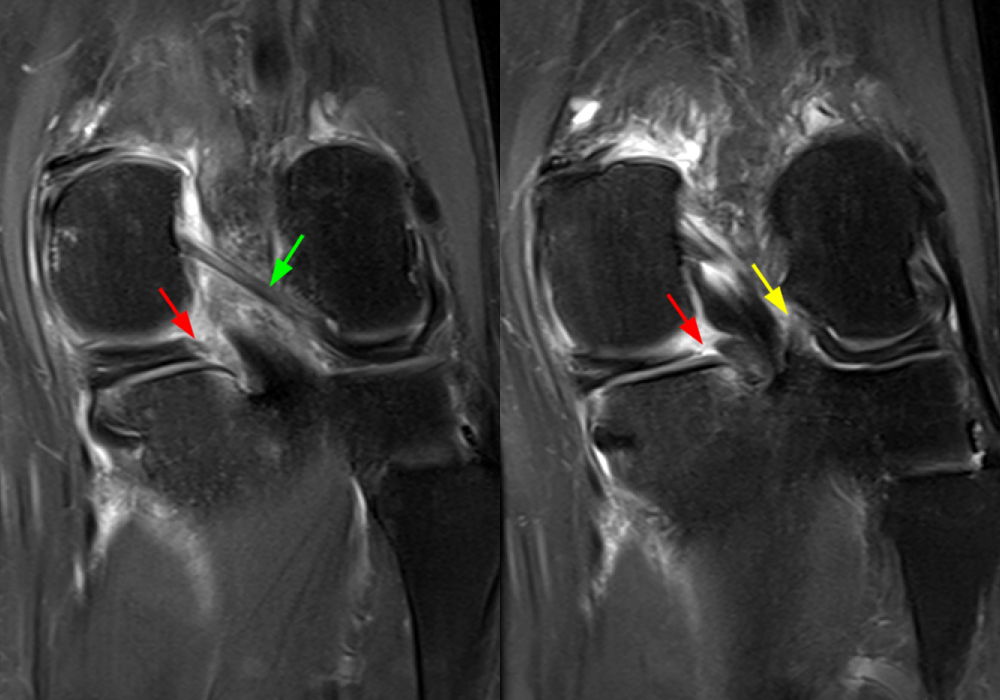
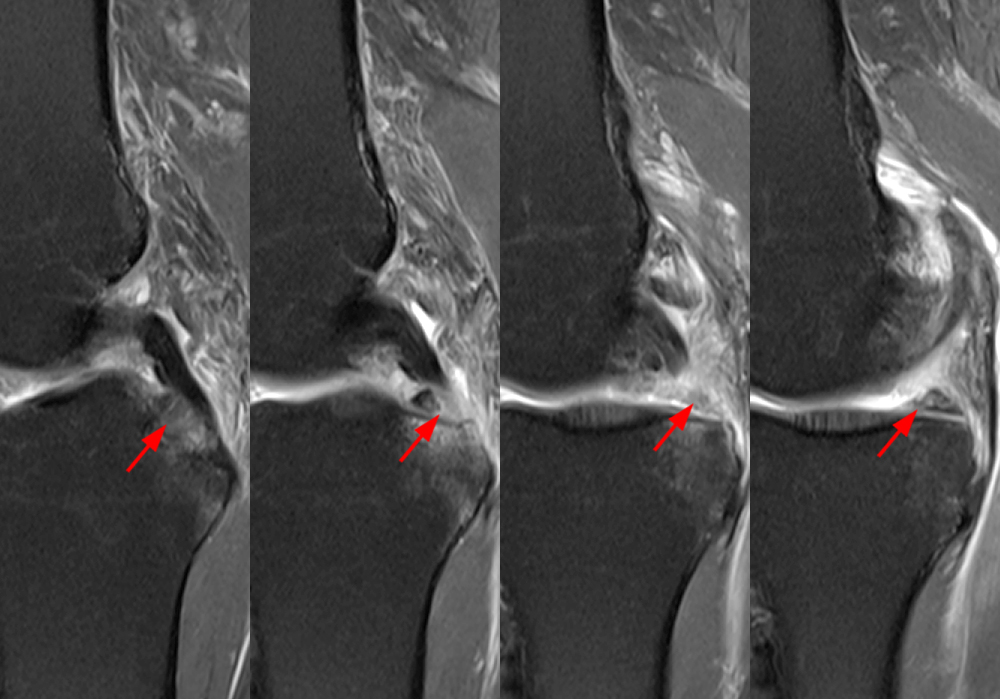
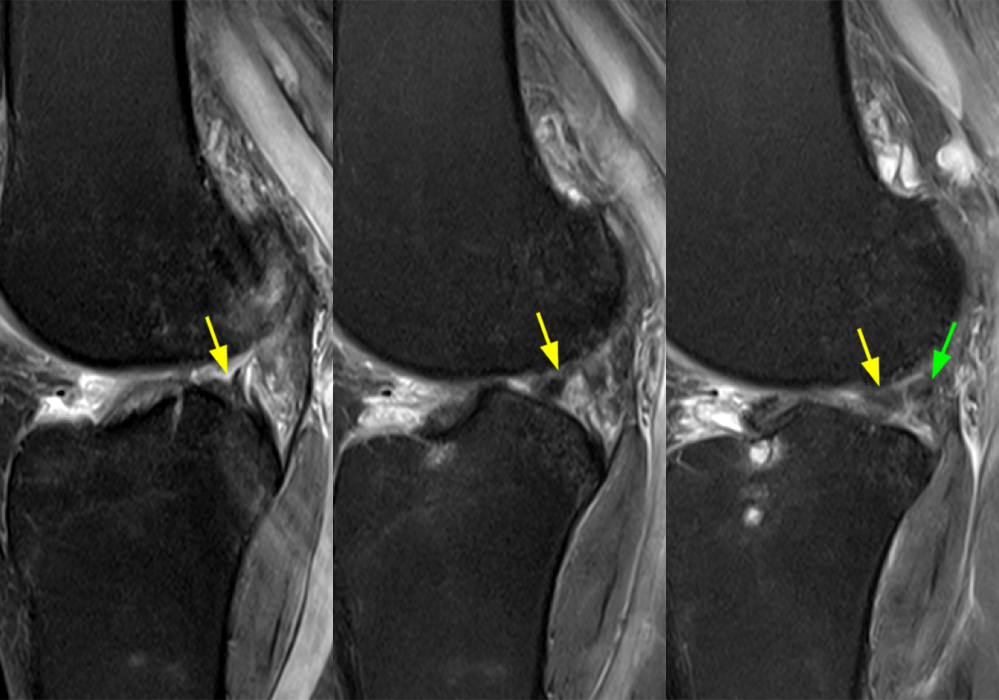
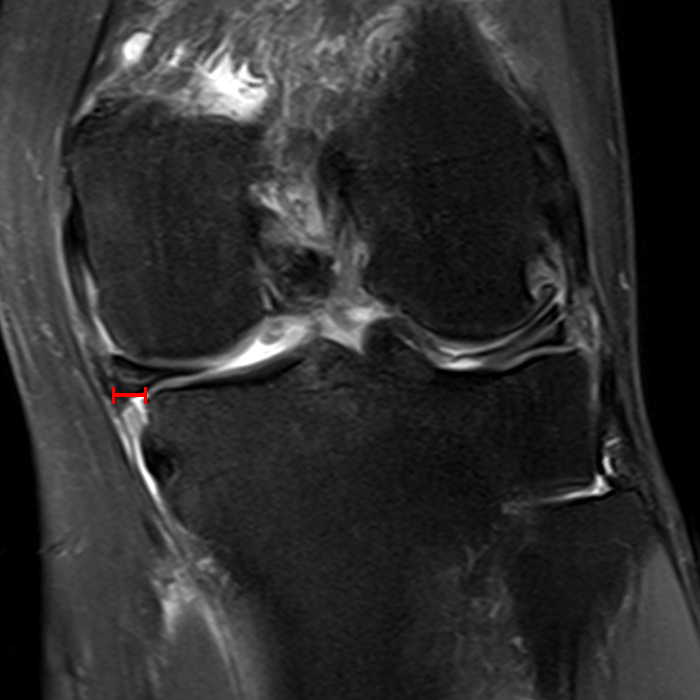
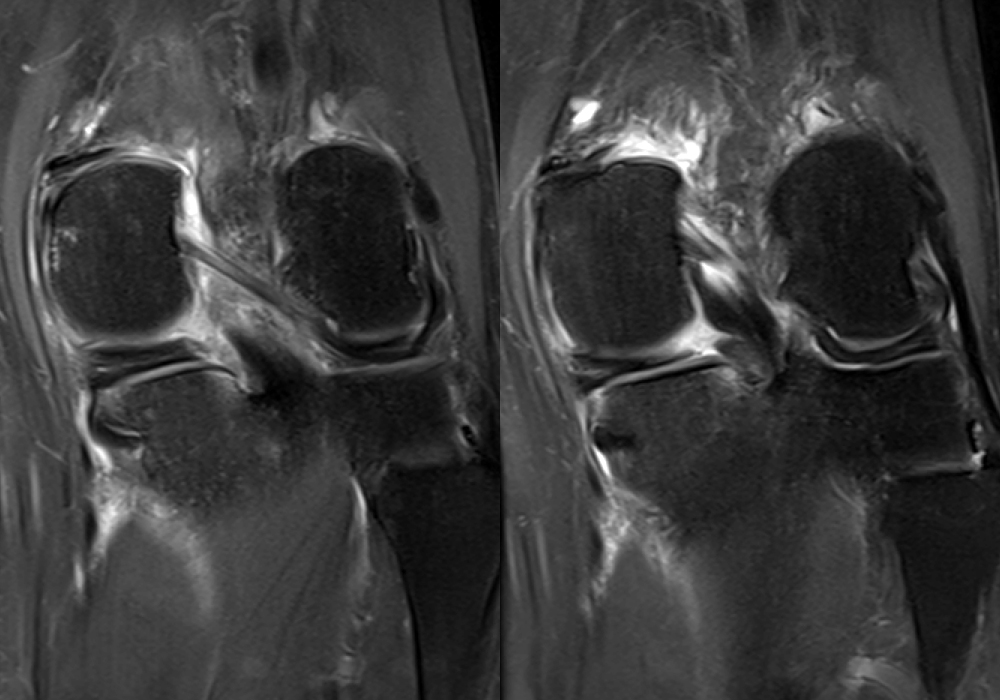
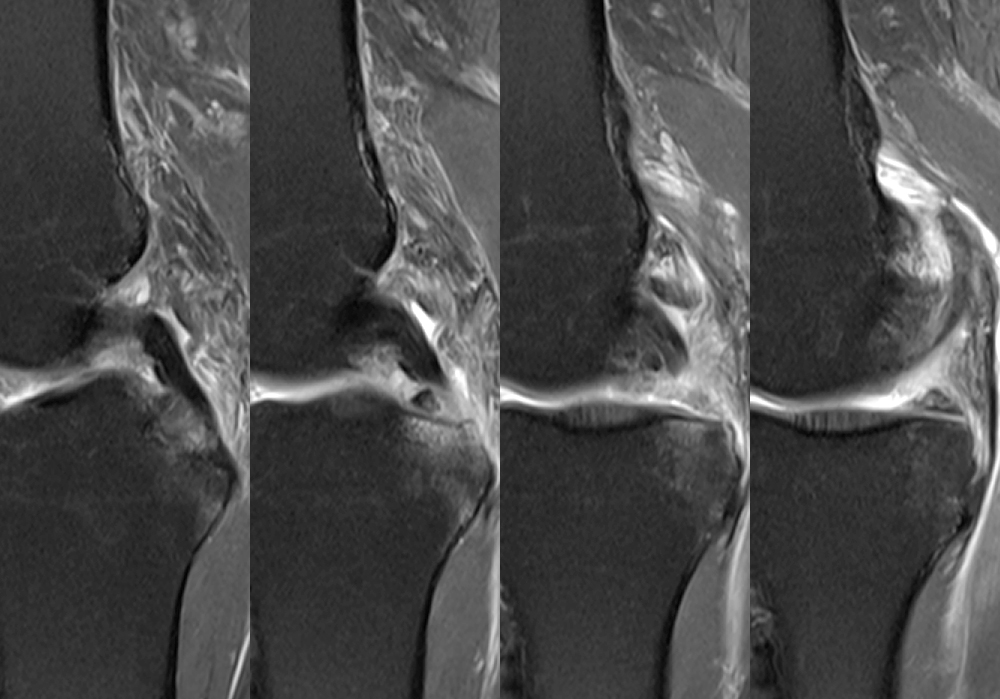
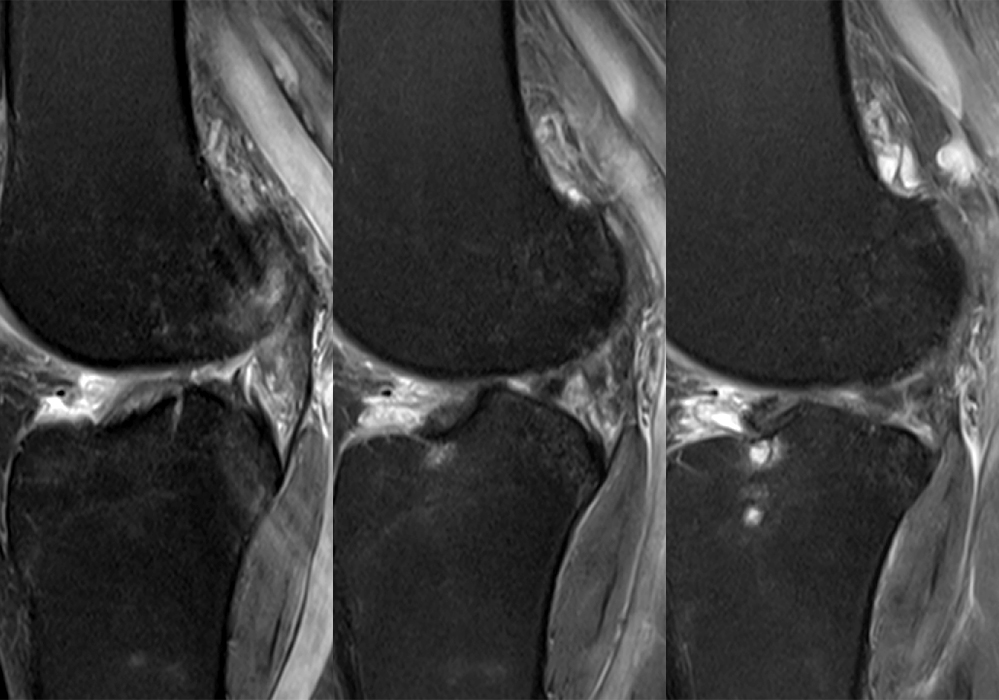
Figure 2: An axial fat-suppressed proton density-weighted image (2A) demonstrates a full-thickness hyperintense cleft along the posterior horn medial meniscus adjacent to the root insertion (red arrows) and abnormally increased T2 signal in the posterior horn lateral meniscus adjacent to the root insertion (yellow arrow). Two contiguous coronal fat-suppressed proton density-weighted images (2B) demonstrate edema within and adjacent to the posterior root medial meniscus with a fluid-filled cleft in the posterior horn adjacent to the root insertion (red arrow), an intact lateral meniscofemoral ligament (green arrow), and an edematous frayed posterior horn lateral meniscus adjacent to the root (yellow arrow). Four contiguous sagittal fat-suppressed proton density-weighted images from lateral to medial (2C) demonstrate an edematous poorly defined tear through the posterior horn medial meniscus immediately adjacent to the root insertion (red arrows) with underlying bone marrow edema (asterisk). Three contiguous sagittal fat-suppressed proton density-weighted images from medial to lateral (2D) demonstrate posterior horn lateral meniscus edema, fraying, and irregular contour adjacent to the root insertion (yellow arrows) with an intact meniscofemoral ligament (green arrow). Coronal image (2E) measuring 4 mm medial meniscus extrusion beyond the medial tibial plateau along the posterior margin of the tibial collateral ligament.
Diagnosis
Recent complete radial tear posterior horn medial meniscus 5 mm from the root insertion with 4 mm extrusion and an ill-defined partial tear posterior root lateral meniscus about 4 mm from the root insertion with an intact meniscofemoral ligament
Introduction
The role of the meniscus in maintaining joint and especially chondral integrity is multifactorial, including shock absorption, load distribution, lubrication, nutrition, and secondary stability. The meniscal roots are ligament-like structures that anchor the menisci to bone and aid in translating axial loads into circumferential hoop stress. Meniscal root tears are biomechanically akin to high-grade radial tears and total meniscectomy because the loss of hoop stress drastically diminishes the ability of the joint to bear axial loads and increases contact forces incurred upon the cartilage, thereby predisposing to premature osteoarthritis.
Anatomy
The posterior root medial meniscus attaches anteromedial to the PCL. The anterior root attachment is more variable along the anterior tibial slope intercondylar crest, discussed in further detail in the February 2023 Web Clinic.
The anterior and posterior lateral meniscal root insertions are only about 10 mm apart. The anterior root lateral meniscus inserts beneath the ACL, and some of the fibers interdigitate.1 The posterior root attaches anterolateral to the medial meniscus posterior root and anterior to the PCL (Figure 3).
Biomechanically, the anterior lateral root is the strongest, and the anterior medial root is the weakest, however, the posterior roots are most frequently torn and thus the focus of our discussion.2
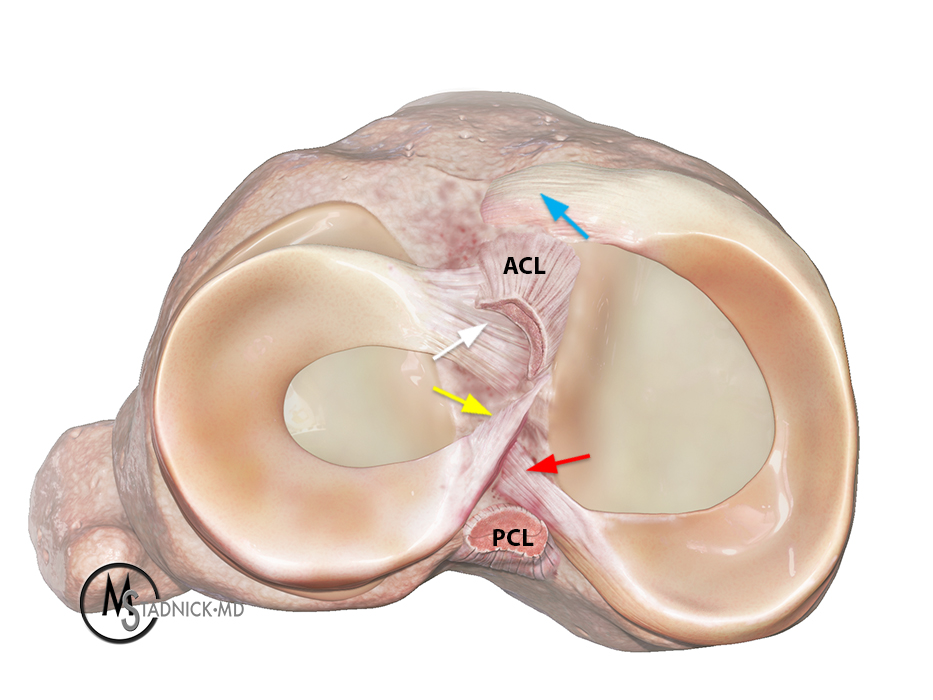
Figure 3: A 3D Illustration depicts the medial and lateral menisci and their root attachments near the anterior (ACL) and posterior (PCL) cruciate ligaments. The posterior root (red arrow) and anterior root (blue arrow) of the medial meniscus and the posterior root (yellow arrow) and anterior root (white arrow) of the lateral meniscus are indicated.
Pathophysiology
A root tear is classically defined as a tear within 9mm of the root insertion.3 If the root itself is avulsed, it should be described as a root avulsion. If the tear is located within 9 mm of the root insertion, it should be described as a root-equivalent tear.
Statistically, the posterior roots are more commonly torn than the anterior roots because they are less mobile and bear larger loads, especially when the knee is flexed at 90 degrees.4 The posterior root medial meniscus is especially prone to injury as the posteromedial corner absorbs a greater degree of compressive forces, and medial meniscal posterior horn mobility is further constrained by the meniscotibial ligament.5,6
Posterior root medial meniscus tears often occur during daily tasks such as rising from a seated position or squatting with the knee hyperflexed. Patients often report posterior knee pain with a pop. In the United States, the population most affected includes middle-aged women with an elevated BMI. Varus malalignment is also a risk factor, and many of these patients present with some degree of underlying chondromalacia. On physical exam, patients may report joint line tenderness and pain with deep flexion.
In contrast, posterior root lateral meniscus tears often occur in younger patients with a history of trauma and a concomitant ACL tear or multi-ligament injury.
Anterior root tears are less common and may be degenerative, traumatic, or iatrogenic in etiology. Disruption of the lateral meniscus anterior and posterior roots may occur due to tibial tunnel reaming or misplacement during ACL reconstruction.7,8 Disruption of the anterior root medial meniscus may occur during anterograde intramedullary tibial nailing.9
MRI Findings
Meniscal root avulsion and root-equivalent tears are an important MRI diagnosis because initial clinical examination can be non-specific. In addition, meniscal extrusion is an imaging-driven diagnosis.
Root tears have a varied appearance on MRI therefore, familiarity with the anatomy and interrogation in all three planes is essential. On MRI, normal meniscal roots sometimes demonstrate a striated appearance or nonspecific increased signal (Figure 4).
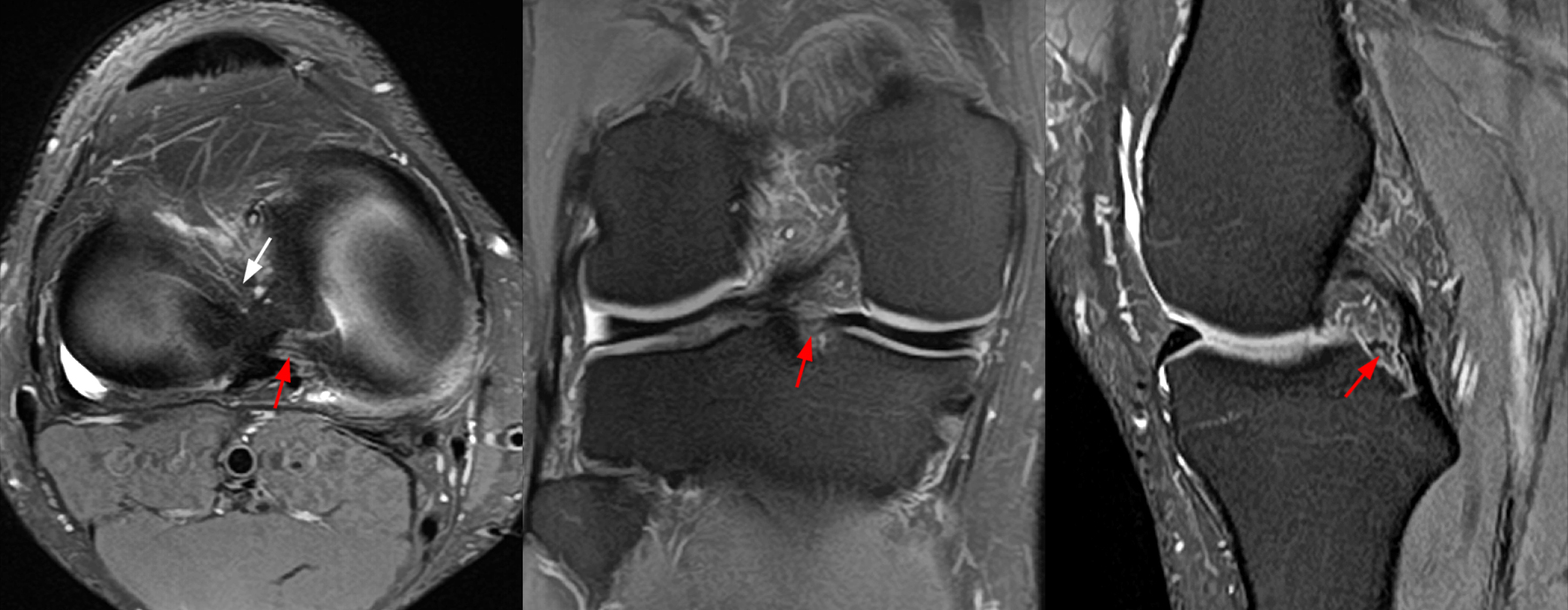
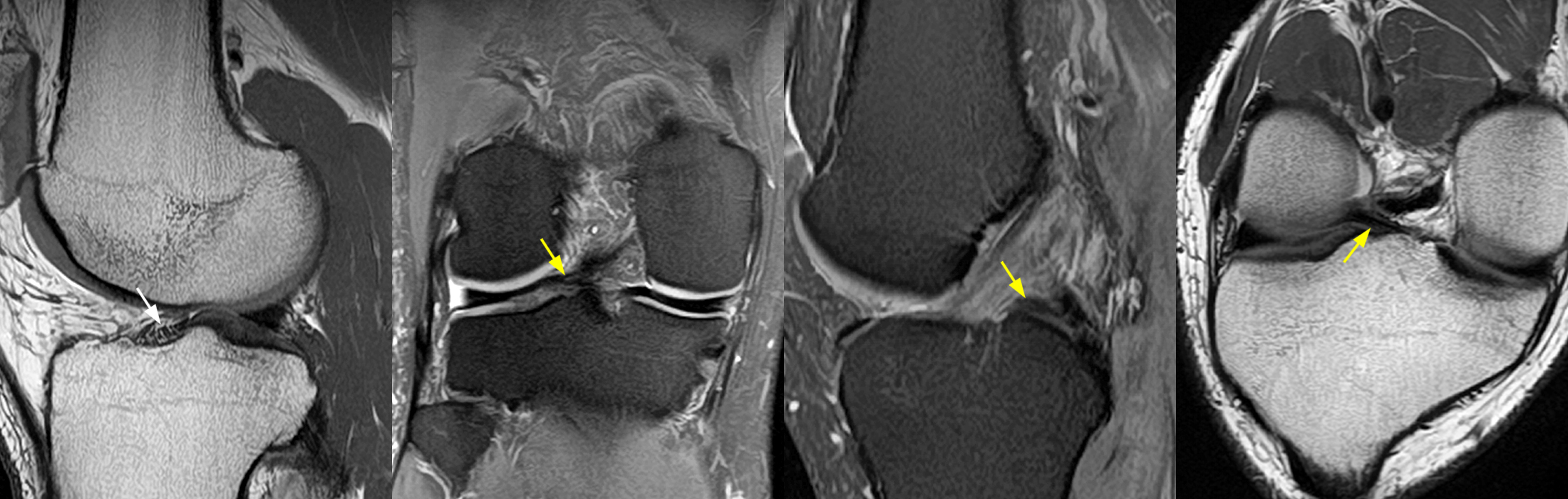
Figure 4: Axial, coronal, and sagittal fat-suppressed proton density-weighted images (4A) demonstrate the normal striated appearance of the posterior root medial meniscus (red arrows). The anterior root lateral meniscus is also evident (white arrow). Sagittal proton density-weighted, coronal and sagittal fat-suppressed proton density-weighted, and coronal oblique proton density-weighted images (4B) demonstrate the normal striated appearance of the anterior root lateral meniscus (white arrow) and the normal posterior root and adjoining posterior horn lateral meniscus (yellow arrows). The coronal oblique proton density-weighted image demonstrates the oblique course of the posterior root lateral meniscus (yellow arrow).
The root itself may be torn, or the tear may be located up to 9 mm from the root insertion (i.e., a root-equivalent tear). Root avulsion and root-equivalent tears may also be partial or complete, and most tears are radial or oblique. Root tears are also generally described as acute versus chronic. The most widely accepted classification system describing tear morphology is an arthroscopic classification, which radiologists should be aware of. However, it is best to describe the tear and leave the specifics of a type I-V designation to the arthroscopists.3 Additionally, a separate classification system to address posterior root lateral meniscus tears in the setting of an ACL tear with specific attention to the status of the meniscofemoral ligaments has also been proposed.10
Medial meniscus posterior root tears
Edema in the posterior root medial meniscus and the underlying bone generally signifies that the tear is more recent, whereas the absence of edema suggests chronicity, and an ossicle embedded in the torn meniscus clinches the diagnosis (Figure 5).
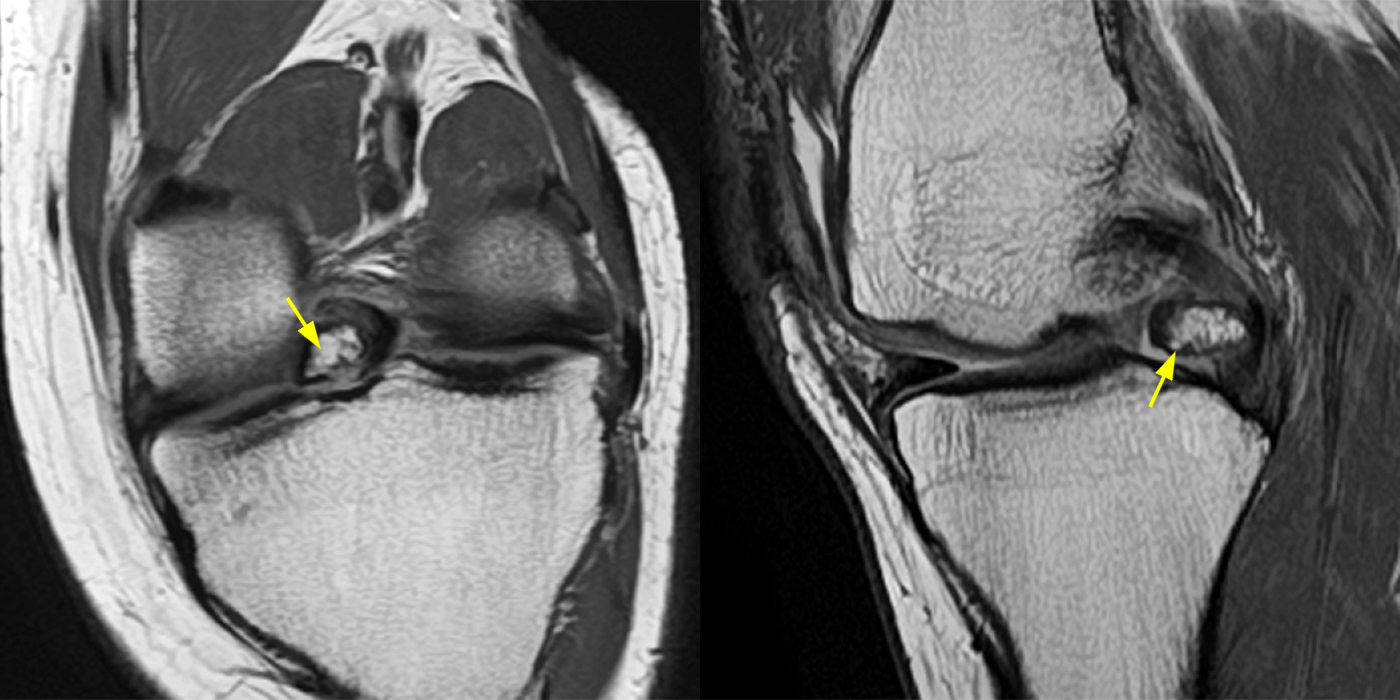
Figure 5: Coronal oblique and sagittal proton density-weighted images demonstrating chronic posterior root medial meniscus avulsion with a large, embedded ossicle (yellow arrows).
Secondary findings frequently associated with medial meniscus posterior root tears include meniscal extrusion due to an increase in contact pressure across the joint, an edematous swollen posterior horn, and subchondral marrow edema or a subchondral fracture along the weight-bearing surface signifying joint overload.
The most accepted definition of extrusion is protrusion of the meniscus by 3 mm or more beyond the outer margin of the tibial plateau.11,12 The preferred method to measure medial meniscus extrusion is a mid-coronal image along the posterior margin of the MCL, and if a bone spur is present, it should be included in the measurement (Figure 6).13
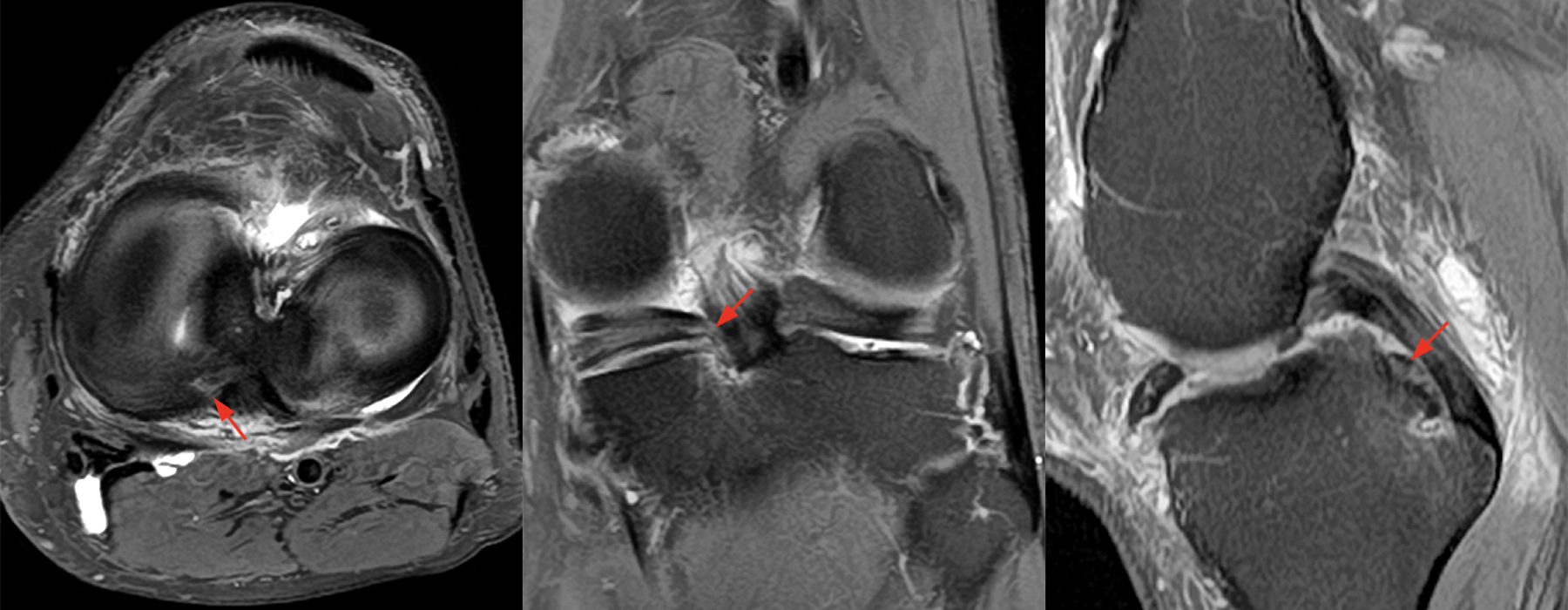

Figure 6: 62-year-old male with left knee pain after getting out of bed and feeling his knee “shift forward” 1 week ago. Axial, coronal, and sagittal fat-suppressed proton density-weighted images(6A) demonstrate an edematous posterior root medial meniscus (red arrows) with underlying bone marrow edema and posterior horn expansion with increased signal. Coronal image (6B) measuring 3 mm medial meniscus extrusion beyond the medial tibial plateau along the posterior margin of the MCL.
If the root appears abnormal due to edema or degeneration, bone marrow edema immediately subjacent to the root insertion can suggest an occult or impending tear and should be described as such (Figure 7).14,15 Similarly, ill-defined partial tears can progress to complete tears in a short time (Figure 8). Traumatic medial meniscus posterior root tears are less common but also occur in the setting of valgus injury (Figure 9).
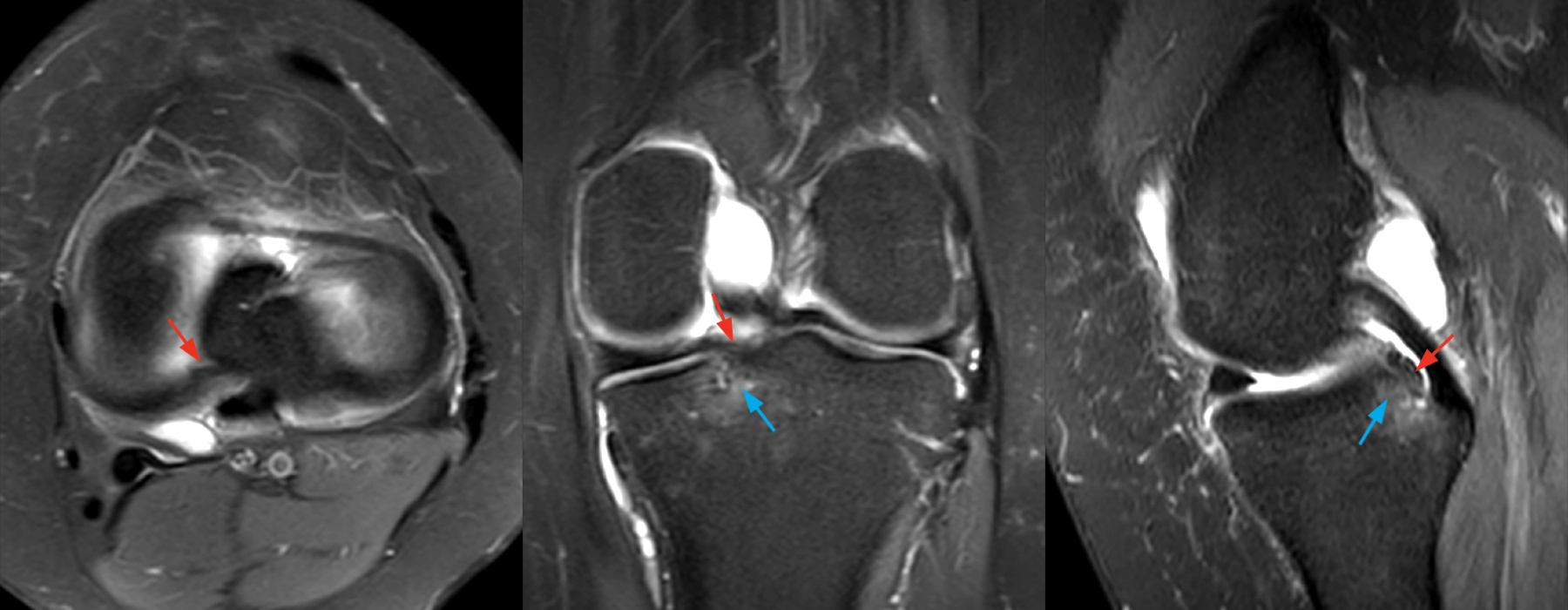
Figure 7: 53-year-old female with left knee pain after a twisting injury three months prior. Axial, coronal, and sagittal fat-suppressed proton density-weighted images demonstrate marrow edema deep to the medial meniscus posterior root insertion (blue arrows) with an intact root (red arrows). These findings are suspicious for impending root avulsion.
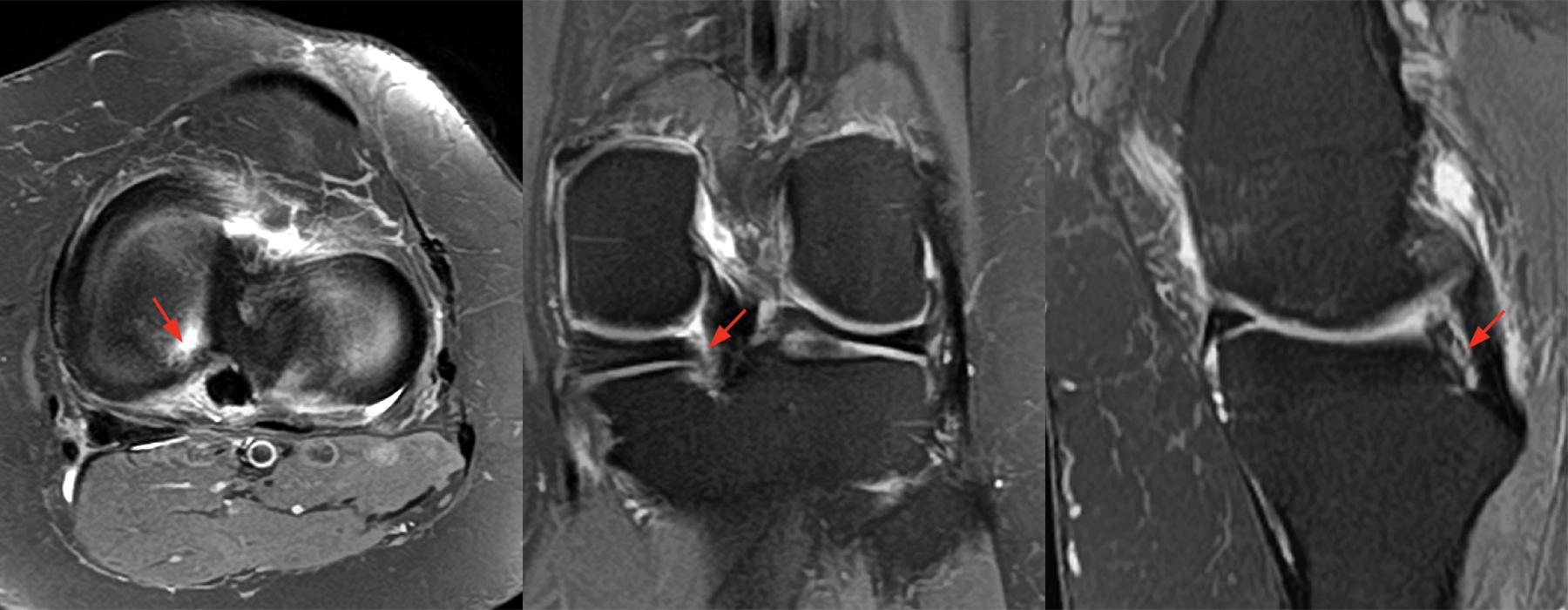
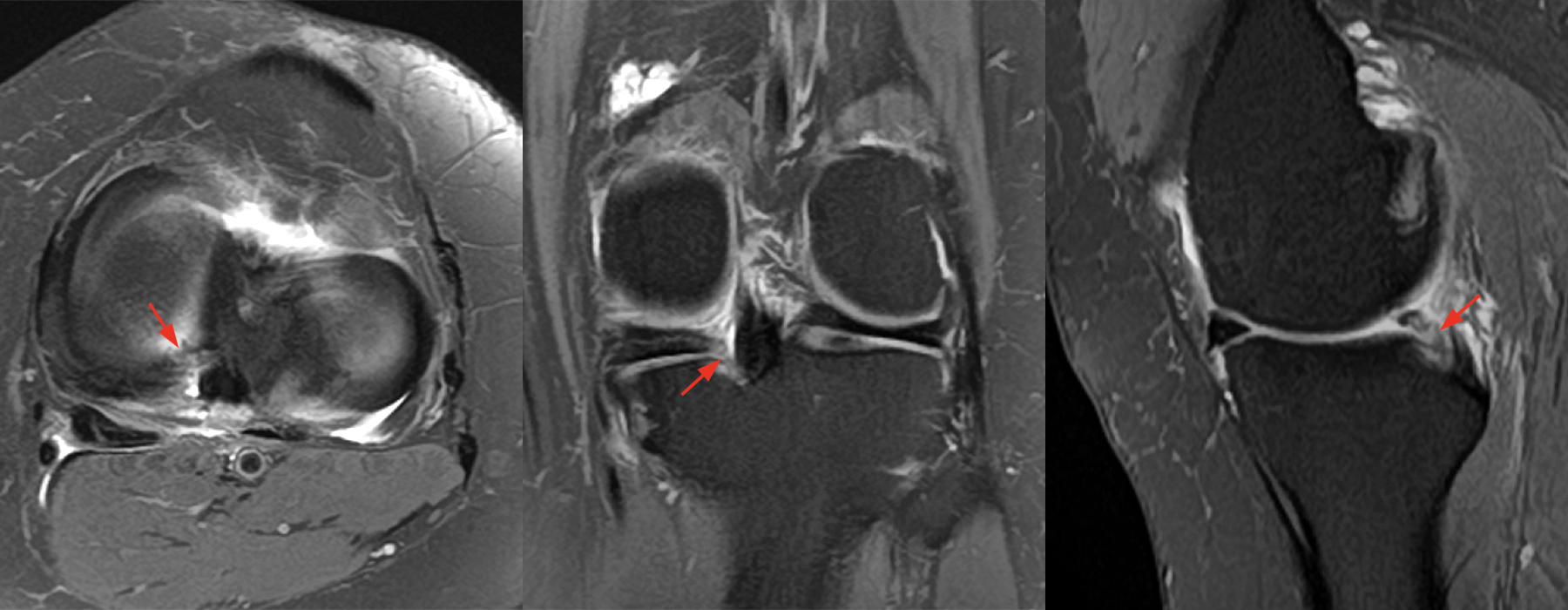
Figure 8: 48-year-old female with worsening left posterolateral knee pain 6 months status-post right knee medial meniscus root repair. Axial, coronal, and sagittal fat-suppressed proton density-weighted images (8A) demonstrating edematous partially torn posterior root medial meniscus with underlying bone marrow edema. The patient was managed conservatively. However, the pain worsened, and the patient returned for an MRI 3 weeks later (8B), which demonstrates a high-grade root tear (red arrows), confirmed at arthroscopy.
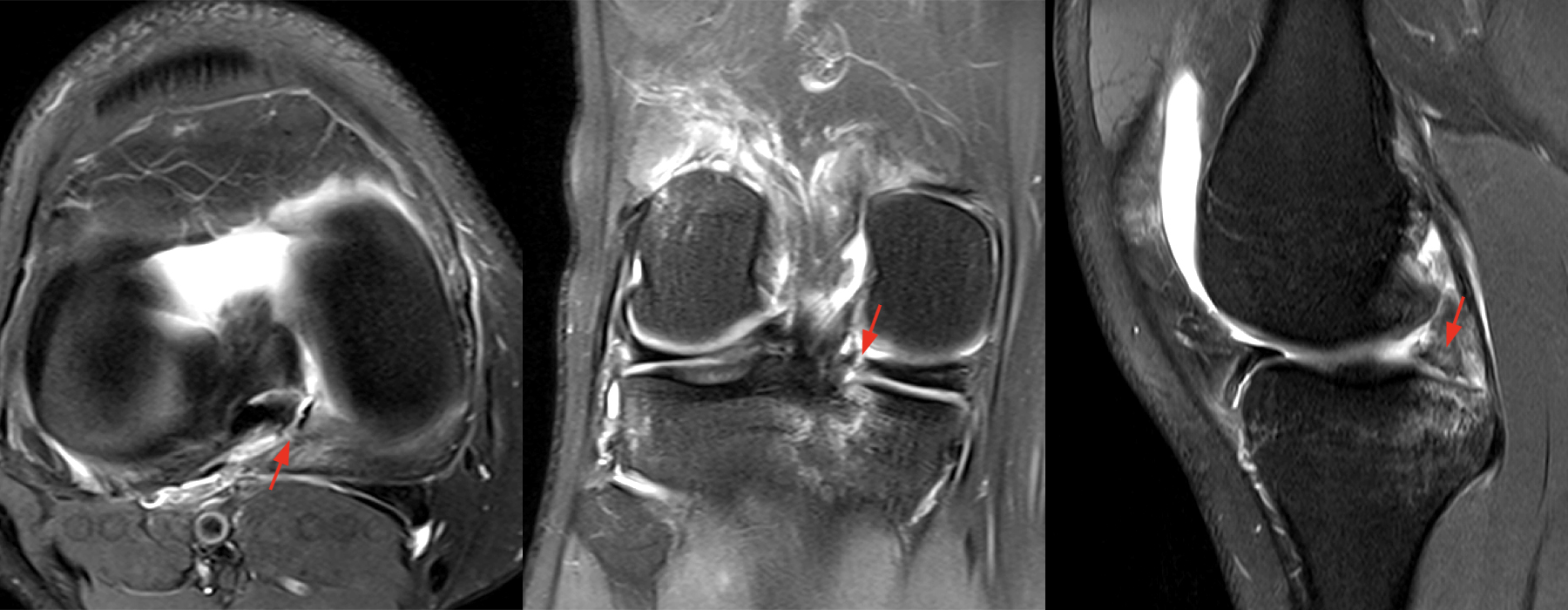
Figure 9: Axial, coronal, and sagittal proton density-weighted images demonstrating an acute full-thickness radial tear through the posterior horn medial meniscus 3 mm from the root insertion (red arrows) in a 20-year-old male following a valgus ski injury with a low-grade femoral MCL sprain and posterolateral tibiofemoral contusions (not shown). At arthroscopy, this was a type 2A tear (complete radial tear 0 to <3 mm from attachment).
Lateral meniscus posterior root tears
The lateral meniscus posterior root insertion and adjacent posterior horn are more challenging to assess on MRI given an oblique course, which is not always appreciated in all three imaging planes. As mentioned above, these tears are more often identified in a younger population with antecedent trauma (Figures 10 and 11).
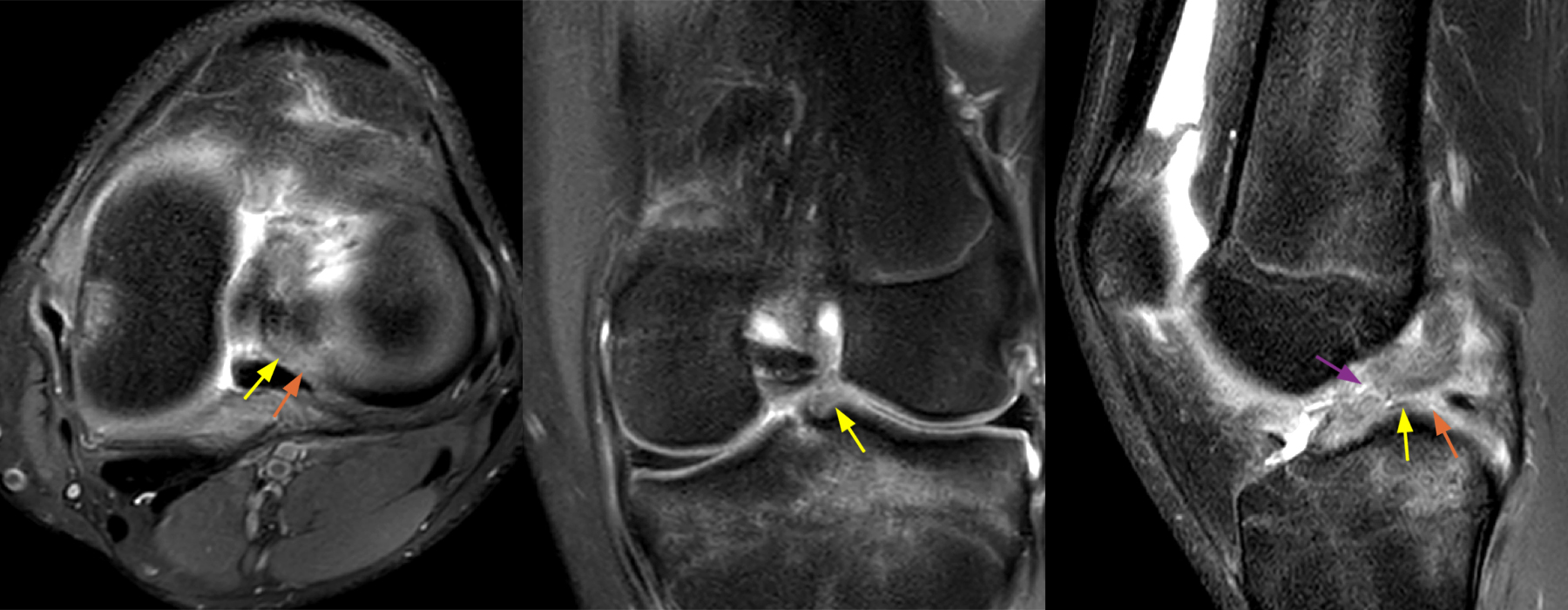
Figure 10: 16-year-old male, rule out ACL tear. Axial, coronal, and sagittal proton density-weighted images demonstrate an edematous ill-defined posterior root lateral meniscus (yellow arrows) with an adjacent full-thickness radial defect (orange arrows) in the setting of an acute ACL mid-substance rupture (purple arrow). The meniscofemoral ligament was intact.

Figure 11: 61-year-old female with medial knee pain after twisting injury 1 week ago. Sequential coronal proton density-weighted images from anterior to posterior demonstrate a diminutive posterior root lateral meniscus (yellow arrow) and adjacent posterior horn with a radial defect (orange arrows). Arthroscopy confirmed a complex root/root-equivalent tear.
The integrity of the meniscofemoral ligaments and any evidence of meniscal extrusion should also be reported, as the meniscofemoral ligaments can confer a degree of stability even in the setting of root avulsion or a root-equivalent tear. Interestingly, lateral meniscus root tears are more prevalent in patients with an ACL tear and lateral femoral notch impaction >2 mm.16
Treatment
The mainstay of treatment is preserving joint contact pressures and preventing or prolonging osteoarthritis progression. Nonoperative treatment is more often recommended in older patients with an elevated BMI and Outerbridge grade 3-4 chondromalacia or Kellgren-Lawrence grade 3-4 osteoarthritis.17 This may consist of activity modification, NSAIDs, injections, and unloader bracing, among other interventions. For patients with a well-maintained joint space and minimal to no chondromalacia in the affected compartment, meniscus root repair is recommended. Surgical intervention is recommended in a timely fashion, as it has been shown that chronicity (>12 months) leads to increased meniscal extrusion and advanced cartilage wear.18 It should be noted that arthroscopic debridement of the meniscus root tear alone does not provide symptomatic relief.19
Therefore, an arthroscopic root repair utilizing a transtibial pullout technique is the standard of care for patients in whom operative intervention is indicated (Figure 12).20 Moreover, the treating surgeon should always obtain pre-operative long leg alignment radiographs and consider a concomitant off-loading osteotomy when indicated.
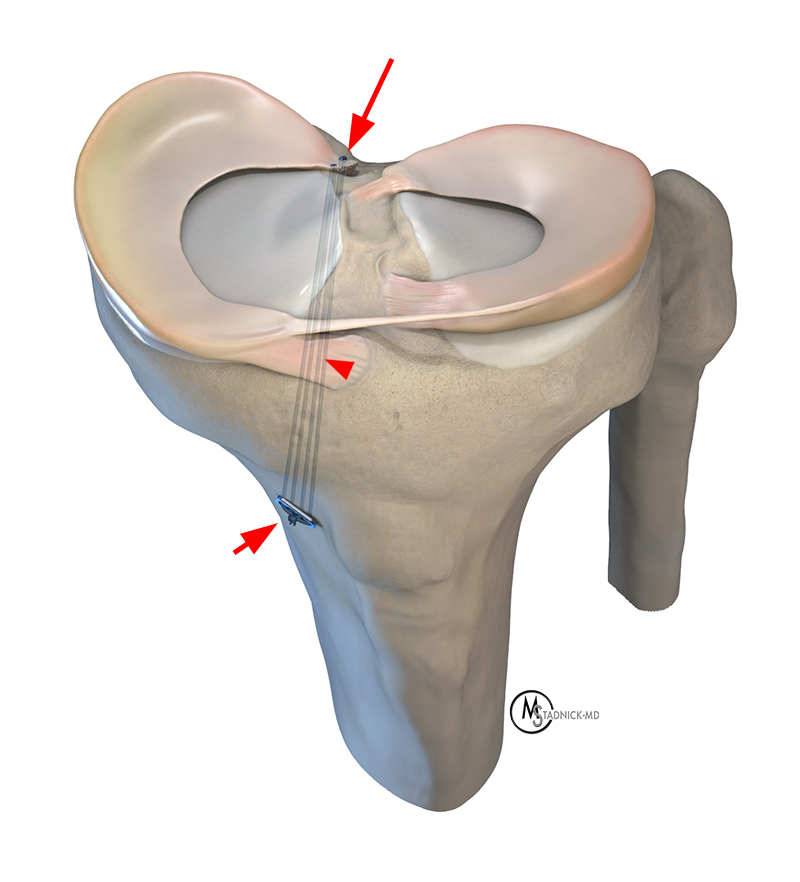
Figure 12: Illustration of the transtibial pullout repair for a tear of the posterior horn medial meniscal root (arrow). The anterior and posterior sutures are passed through a tibial tunnel (arrowhead), and the sutures are tied over a cortical fixation device or Endobutton (short arrow) to secure the root repair.
Summary
The meniscal roots anchor the menisci to bone, and root tears eliminate the joint’s ability to control hoop stress which drastically increases contact pressure, leads to joint overload, and osteoarthritis progression. A root tear is classically defined as a tear within 10 mm of the root insertion. If the root itself is avulsed, it should be described as root avulsion. If the tear is located within 9 mm of the root insertion, it should be described as a root-equivalent tear. Lateral meniscus posterior root tears are more commonly associated with acute trauma and concomitant ligament injury. Medial meniscus posterior root tears are more commonly reported while performing ordinary daily tasks, and more often associated with bone marrow edema and extrusion. Meniscal extrusion 3 mm beyond the outer tibial margin is generally agreed upon as pathologic. Posterior root lateral meniscus tears may be stable if the meniscofemoral ligament is intact. When describing meniscal root tears, it is also important to mention any chondromalacia or osteoarthritis that may affect treatment decisions.
References
- Steineman BD, Moulton SG, Haut Donahue TL, Fontboté CA, LaPrade CM, Cram TR, Dean CS, LaPrade RF. Overlap Between Anterior Cruciate Ligament and Anterolateral Meniscal Root Insertions: A Scanning Electron Microscopy Study. Am J Sports Med. 2017 Feb;45(2):362-368. doi: 10.1177/0363546516666817. Epub 2016 Oct 13. PMID: 27729320. ↩
- Kopf S, Colvin AC, Muriuki M, Zhang X, Harner CD. Meniscal Root Suturing Techniques: Implications for Root Fixation. The American Journal of Sports Medicine. 2011;39(10):2141-2146. doi:10.1177/0363546511413250 ↩
- LaPrade CM, James EW, Cram TR, Feagin JA, Engebretsen L, LaPrade RF. Meniscal root tears: a classification system based on tear morphology. Am J Sports Med. 2015 Feb;43(2):363-9. doi: 10.1177/0363546514559684. Epub 2014 Dec 1. PMID: 25451789. ↩
- Guimarães JB, Chemin RN, Araujo FF, Link TM, Silva FD, Bitar A, Nico MAC, Filho AGO. Meniscal Root Tears: An Update Focused on Preoperative and Postoperative MRI Findings. AJR Am J Roentgenol. 2022 Aug;219(2):269-278. doi: 10.2214/AJR.22.27338. Epub 2022 Mar 16. PMID: 35293231. ↩
- Rocco Papalia and others, Meniscal root tears: from basic science to ultimate surgery, British Medical Bulletin, Volume 106, Issue 1, June 2013, Pages 91-115, https://doi.org/10.1093/bmb/ldt002 ↩
- Thompson, W. O.; Thaete, F. L.; Fu, F. H.; Dye, S. F. (1991). Tibial meniscal dynamics using three-dimensional reconstruction of magnetic resonance images. The American Journal of Sports Medicine, 19(3), 210–216. doi:10.1177/036354659101900302 ↩
- Vadhera AS, Lee JS, Singh H, Gursoy S, Kunze KN, Verma NN, Chahla J. Injury to the Posterior Horn of the Lateral Meniscus from a Misplaced Tibial Tunnel for Anterior Cruciate Ligament Reconstruction: A Case Report. Am J Case Rep. 2022 Nov 3;23:e937581. doi: 10.12659/AJCR.937581. PMID: 36327165; PMCID: PMC9641552. ↩
- LaPrade CM, Smith SD, Rasmussen MT, Hamming MG, Wijdicks CA, Engebretsen L, Feagin JA, LaPrade RF. Consequences of tibial tunnel reaming on the meniscal roots during cruciate ligament reconstruction in a cadaveric model, Part 1: The anterior cruciate ligament. Am J Sports Med. 2015 Jan;43(1):200-6. doi: 10.1177/0363546514554769. Epub 2014 Oct 31. PMID: 25361859. ↩
- Ellman MB, James EW, LaPrade CM, LaPrade RF. Anterior meniscus root avulsion following intramedullary nailing for a tibial shaft fracture. Knee Surg Sports Traumatol Arthrosc. 2015 Apr;23(4):1188-91. doi: 10.1007/s00167-014-2941-5. Epub 2014 Mar 19. PMID: 24643359. ↩
- Forkel P, Reuter S, Sprenker F, Achtnich A, Herbst E, Imhoff A, Petersen W. Different patterns of lateral meniscus root tears in ACL injuries: application of a differentiated classification system. Knee Surg Sports Traumatol Arthrosc. 2015 Jan;23(1):112-8. doi: 10.1007/s00167-014-3467-6. Epub 2014 Dec 12. PMID: 25502611. ↩
- Boxheimer L, Lutz AM, Treiber K, Goepfert K, Crook DW, Marincek B, Weishaupt D. MR imaging of the knee: position related changes of the menisci in asymptomatic volunteers. Invest Radiol. 2004 May;39(5):254-63. doi: 10.1097/01.rli.0000116895.04239.84. PMID: 15087719. ↩
- Costa CR, Morrison WB, Carrino JA. Medial meniscus extrusion on knee MRI: is extent associated with severity of degeneration or type of tear? AJR Am J Roentgenol. 2004 Jul;183(1):17-23. doi: 10.2214/ajr.183.1.1830017. PMID: 15208101. ↩
- Farivar D, Hevesi M, Fortier LM, Azua E, LaPrade RF, Chahla J. Meniscal Extrusion Measurements After Posterior Medial Meniscus Root Tears: A Systematic Review and Meta-analysis. Am J Sports Med. 2022 Dec 21:3635465221131005. doi: 10.1177/03635465221131005. Epub ahead of print. PMID: 36541434. ↩
- Furumatsu T, Hiranaka T, Kintaka K, Okazaki Y, Higashihara N, Tamura M, Ozaki T. A characteristic MRI finding to diagnose a partial tear of the medial meniscus posterior root: an ocarina sign. Knee Surg Relat Res. 2021 Oct 9;33(1):38. doi: 10.1186/s43019-021-00120-4. PMID: 34627395; PMCID: PMC8502318. ↩
- Nakamura R, Okano A, Yoshida I, Shimakawa T. A spreading roots sign: Characteristic sign of the preliminary stage of medial meniscus posterior root tear on magnetic resonance imaging. J Orthop Sci. 2022 Sep;27(5):1107-1113. doi: 10.1016/j.jos.2021.07.005. Epub 2021 Aug 5. PMID: 34364758. ↩
- Berthold DP, Muench LN, Herbst E, Mayr F, Chadayammuri V, Imhoff AB, Feucht MJ. High prevalence of a deep lateral femoral notch sign in patients with anterior cruciate ligament (ACL) and concomitant posterior root tears of the lateral meniscus. Knee Surg Sports Traumatol Arthrosc. 2021 Apr;29(4):1018-1024. doi: 10.1007/s00167-020-06071-9. Epub 2020 May 21. PMID: 32440714. ↩
- Randazzo E, Duerr R, Baria MR. Meniscus Root Tears: A Clinical Review. Curr Sports Med Rep. 2022 May 1;21(5):155-158. doi: 10.1249/JSR.0000000000000959. PMID: 35522439. ↩
- Krych AJ, Johnson NR, Mohan R, Hevesi M, Stuart MJ, Littrell LA, Collins MS. Arthritis Progression on Serial MRIs Following Diagnosis of Medial Meniscal Posterior Horn Root Tear. J Knee Surg. 2018 Aug;31(7):698-704. doi: 10.1055/s-0037-1607038. Epub 2017 Sep 26. Erratum in: J Knee Surg. 2018 Aug;31(7):e1. PMID: 28950387. ↩
- Eseonu KC, Neale J, Lyons A, Kluzek S. Are Outcomes of Acute Meniscus Root Tear Repair Better Than Debridement or Nonoperative Management? A Systematic Review. Am J Sports Med. 2022 Sep;50(11):3130-3139. doi: 10.1177/03635465211031250. Epub 2021 Oct 11. PMID: 34633226. ↩
- 2022 Jul 1;30(13):613-619. doi: 10.5435/JAAOS-D-21-01153. Epub 2022 Apr 16. PMID: 35439222. ↩
