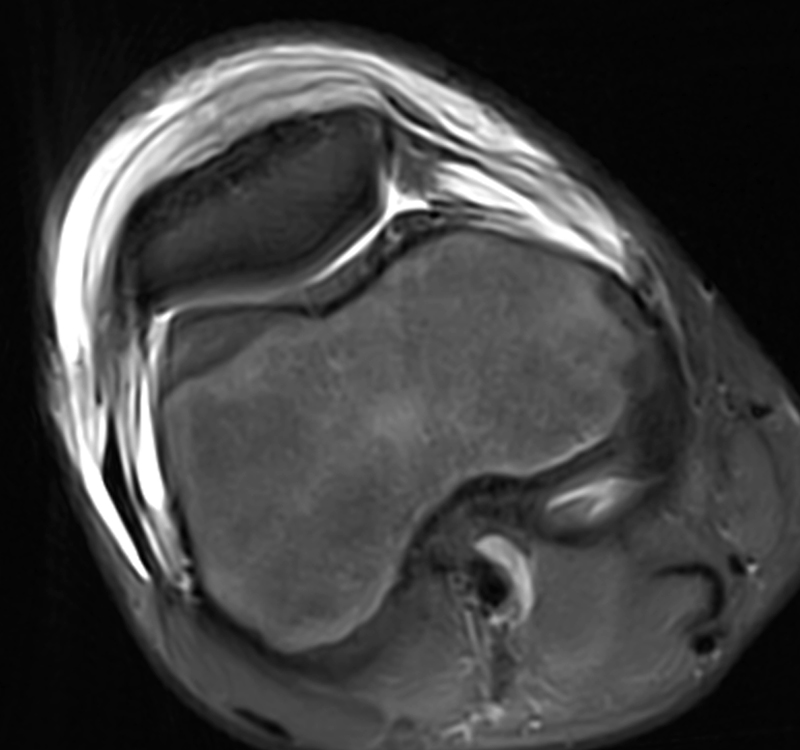
Clinical History: A 14-year-old male presents with a 5-day history of anterior pain and swelling. He suffered a minor incidental contact injury in football 3 weeks prior. T1-weighted (1a) and fat-suppressed proton density-weighted (1b) sagittal images and a fat-suppressed proton density-weighted (1c) axial image are provided. What are the findings? What is your diagnosis?


Findings
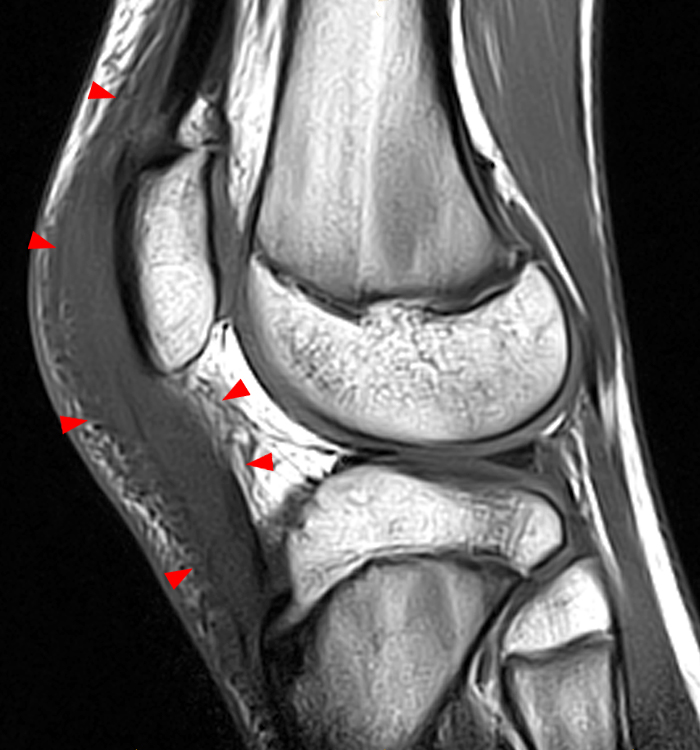
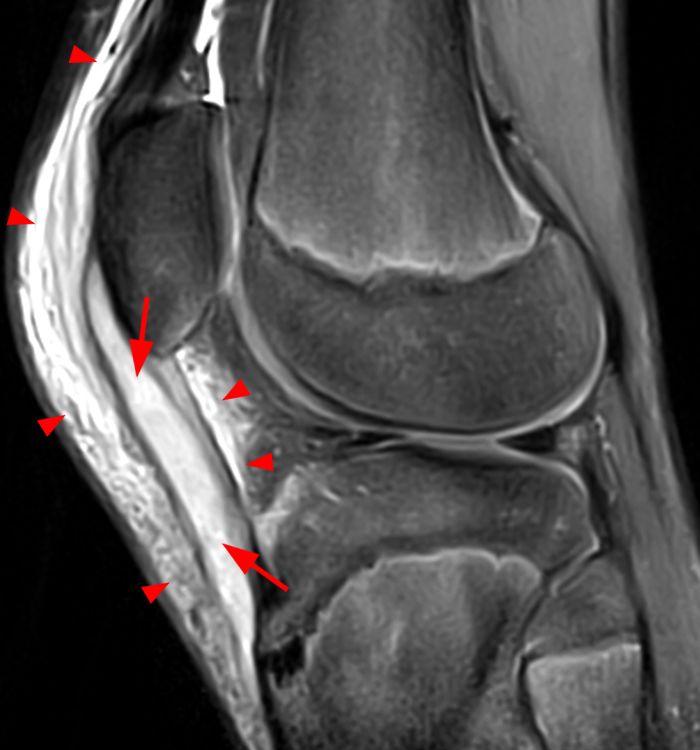
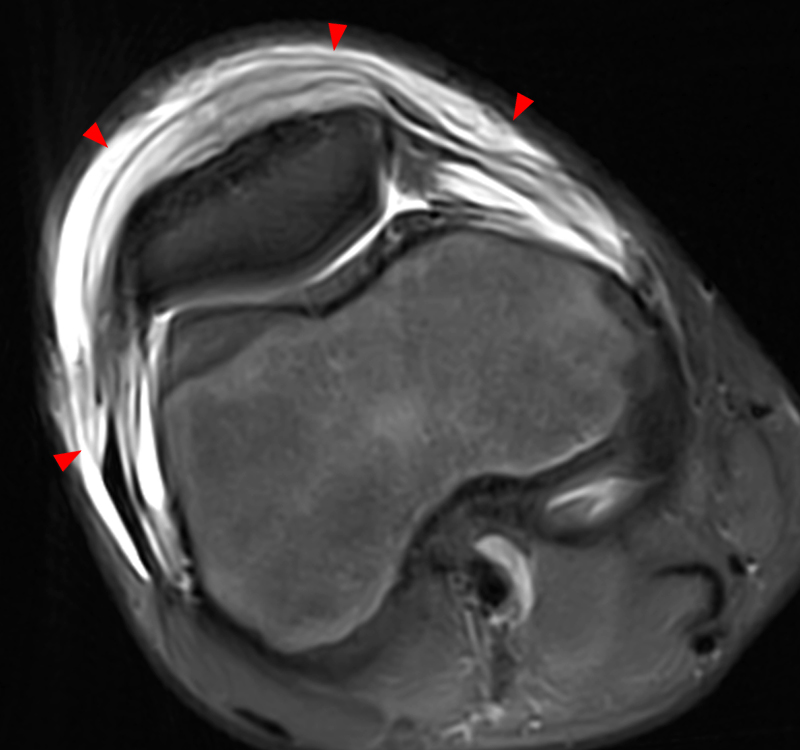
Figure 2: Anterior swelling and edema are apparent on the T1-weighted (2a) and fat-suppressed proton density-weighted (2b) sagittal images (arrowheads). Central fluid signal intensity is present within the patellar tendon (arrows) on the fat-suppressed proton density-weighted image. The pronounced anterior swelling and edema (arrowheads) are confirmed on the fat-suppressed proton density-weighted axial image (2c).
Diagnosis
Cellulitis of the anterior knee with a patellar tendon intratendinous abscess (pathologically proven).
Case Discussion
The current case demonstrates an extremely rare diagnosis, an intratendinous abscess of the patellar tendon, and the first known depiction of the diagnosis with MRI. A literature search revealed only one other report of a patellar tendon abscess1. It occurred in an injection drug user who injected at the anterior knee, and that case report included only computed tomography and ultrasound as imaging. The patient’s initial minor football injury resulted in a small abrasion at the anterior knee. At presentation 3 weeks later, the 14-year-old male patient was very tender to touch at the anterior knee. Moderate warmth was found throughout the knee, greatest anteriorly, though only a trace knee effusion was present. MRI was performed on the same day following the initial office visit. As depicted above, the MR findings are striking. Although the patient had experienced minor trauma in football 3 weeks earlier, the MR findings were felt to be atypical for such minor trauma, and given the clinical presentation, infection was a strong consideration. After no improvement following 2 days of Ciprofloxacin, lab results demonstrated elevations of C-reactive protein and sedimentation rate, both markers of infection. The patient was taken to the operating room for incision and debridement. At surgery, a longitudinal incision was made at the anterior knee. A small area of breakdown was found within the central patellar tendon, and copious amounts of pus were found within the tendon, extending into infrapatellar fat. No communication with the intra-articular space was found. Cultures subsequently confirmed the causative organism as methicillin resistant staphylococcus aureus. The patient was placed on appropriate antibiotics, and at follow-up two weeks after surgery, his clinical situation was dramatically improved. Thank you to James Sikes, MD, Southern Bone and Joint Specialists, Hattiesburg, MS, for clinical, laboratory, and operative findings.
MRI of Tendon and Peritendinous Infections
Intratendinous abscesses are exceedingly rare, and as previously mentioned, there has been only one previous publication of an intratendinous abscess of the patellar tendon. The majority of reported tendon abscesses involve the Achilles tendon. An Achilles tendon abscess has been reported following a cat bite 2, following surgery3, and following a local steroid injection4. A single online report of a triceps tendon abscess in an immunocompromised patient has been published.5 Radsource’s case files also include a single example of a triceps tendon abscess in a patient with olecranon osteomyelitis (Figure 3).
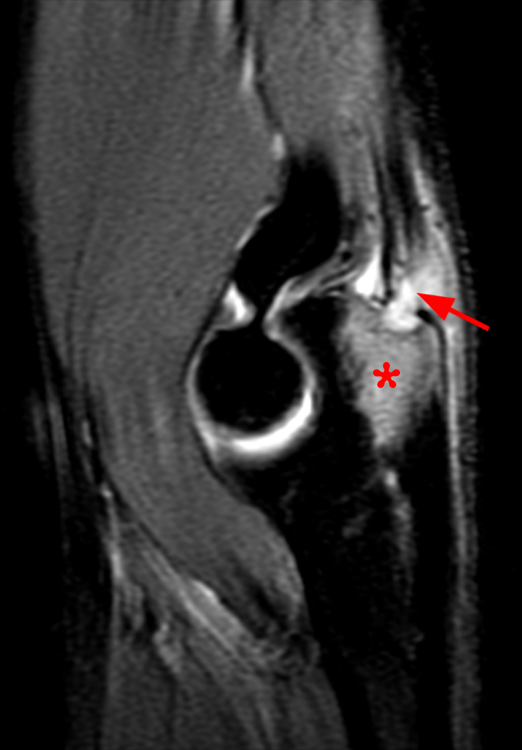
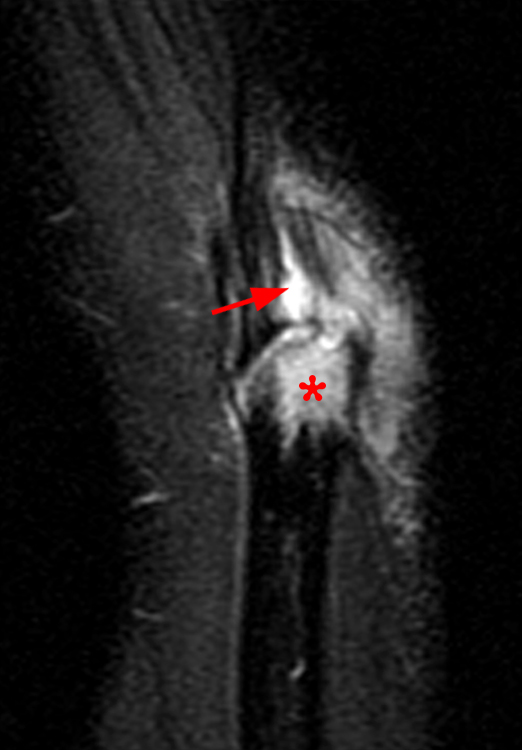
Figure 3: Fat-suppressed proton density-weighted sagittal (3a) and fat-suppressed T2-weighted coronal (3b) images of the elbow in a 29-year-old male who sustained a fall with an open wound. Focal marrow edema (asterisks) is apparent within the olecranon, later confirmed to be due to osteomyelitis. Adjacent fluid signal intensity is present within the distal triceps tendon (arrows), compatible with a small intratendinous abscess.
The much more common source of infection related to a tendon is infectious tenosynovitis, an entity found most often in the flexor tendons of the hand and fingers (MRI Web Clinic June 2013), where it is termed pyogenic flexor tenosynovitis (PFT). PFT is thought to represent up to 9.4% of hand infections6. Although the development of antibiotics and appropriate surgical therapy have decreased the incidence of serious sequelae from PFT, early recognition of the entity is important to minimize the potentially devastating consequences of delayed treatment. Kanavel in 1912 described his four signs that indicate a flexor tendon sheath infection7. The signs include symmetrical swelling of the digit, severe tenderness along the course of the flexor tendon, semiflexed posture, and pain with attempted passive extension of the digit. These signs remain valid today, though authors generally agree that the signs are highly sensitive but less specific for the diagnosis of PFT.8 Most cases of PFT occur following penetrating trauma to the digit. Staphylococcus aureus is the most common offending organism9, and methicillin-resistant staphylococcus aureus is found in up to 29% of cases10. Regardless of the etiology, prompt administration of antibiotics with broad-spectrum coverage is recommended in patients suspected of having PFT.
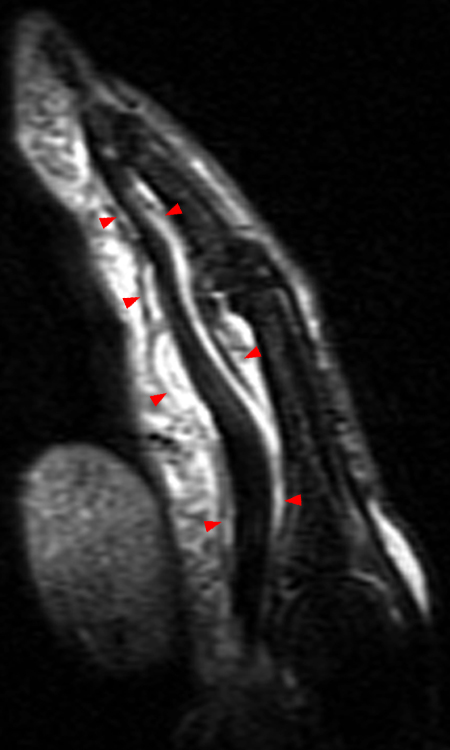
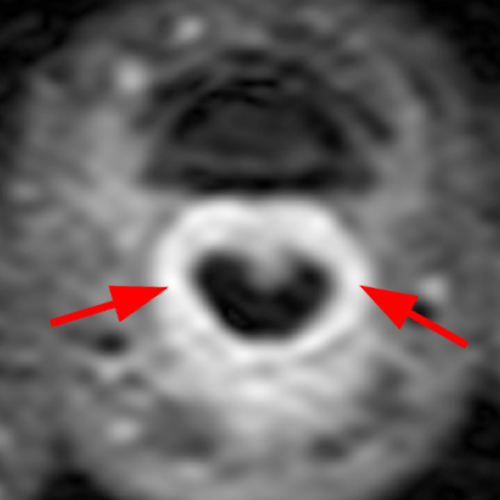
Figure 4: Sagittal STIR (4a) and axial fat-suppressed proton density-weighted (4b) images of the index finger in a 69-year-old male who presented with severe pain and swelling one week following a dog bite. Fluid distends the flexor tendon sheath on the sagittal image (arrowheads). The tenosynovitis is confirmed on the axial image (arrows), which demonstrates no intrinsic signal abnormality of the flexor tendons.

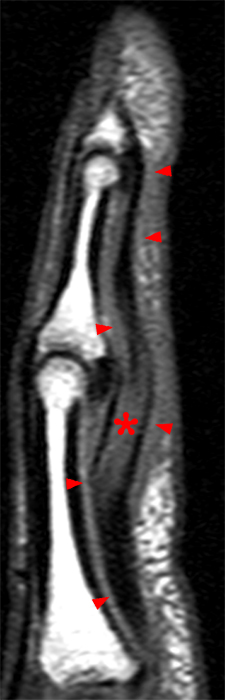

Figure 5: Sagittal STIR (5a) and T1-weighted images (5b) in a 47-year-old female who was finned by a catfish 8 weeks earlier demonstrate flexor tenosynovitis of the index finger (arrowheads). Intrinsically increased signal intensity is present within the flexor digitorum profundus tendon (asterisks) on the sagittal images and on the corresponding STIR axial image (5c) near the level of the PIP joint, suspicious for necrosis and longitudinal tearing.
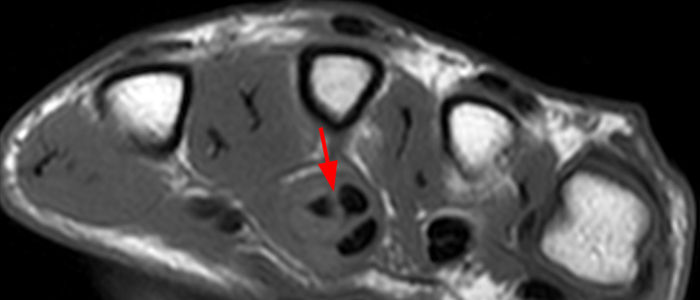
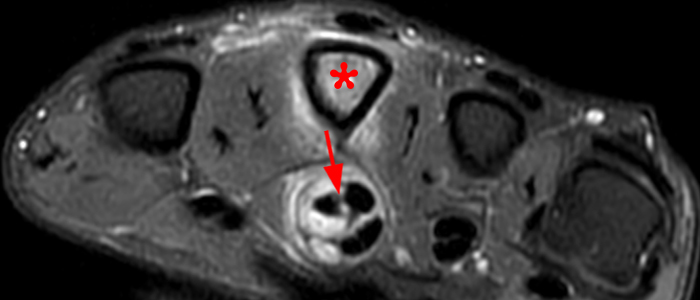
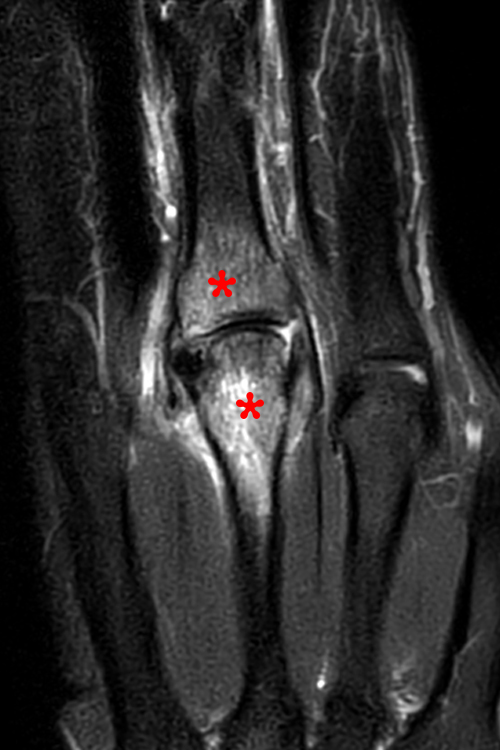
Figure 6: T1-weighted (6a) and fat-suppressed proton density-weighted (6b) images from a 38-year-old male who presented with severe long finger pain and swelling several weeks after penetrating injury from a sea urchin. The axial images reveal severe flexor tenosynovitis with complete longitudinal splitting of the flexor digitorum profundus tendon (arrows). Marrow edema is apparent within the metacarpal shaft (asterisk) on the fat-suppressed proton density-weighted axial image. Intense marrow edema is confirmed within the distal metacarpal and the base of the proximal phalanx (asterisks) on the fat-suppressed T2-weighted coronal view (6c), compatible with osteomyelitis.
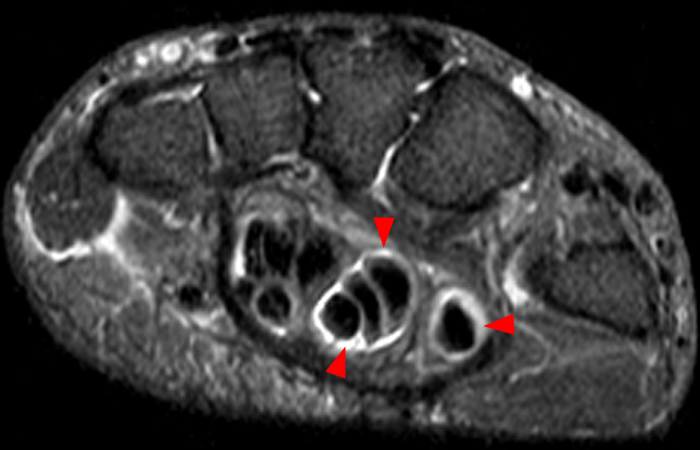
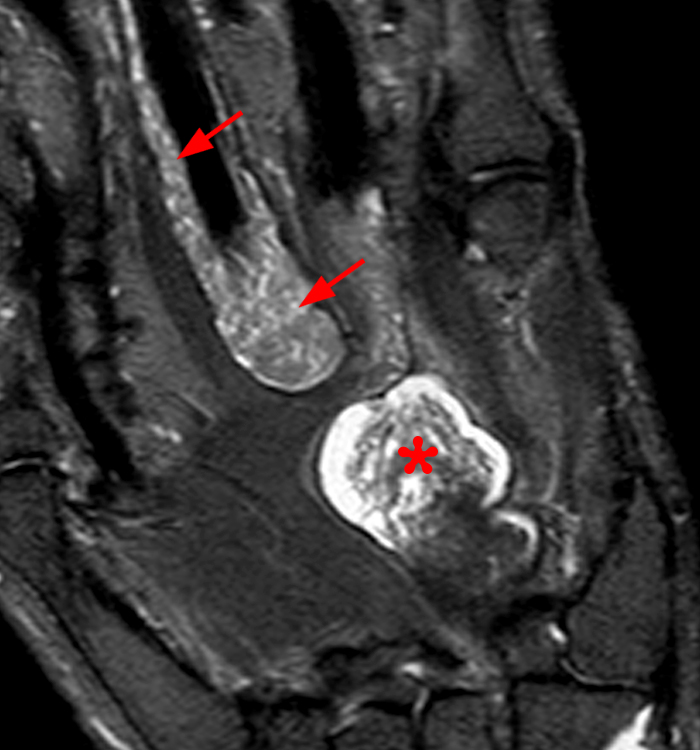
Figure 7: Axial (7a) and coronal (7b) STIR images from a 71-year-old female with a history of prior small finger amputation for mycobacterium avium infection. Generalized flexor tenosynovitis (arrowheads) is apparent on the axial view. The coronal image reveals distal extension of the tenosynovitis to the index finger (arrows) and involvement of the ulnar bursa (asterisk), which is distended. Internal signal consistent with rice bodies is apparent at both sites, and the diagnosis of recurrent mycobacterium avium was confirmed.
Differential diagnosis
Flexor tenosynovitis in the fingers can be infectious or non-infectious (inflammatory). MRI cannot reliably distinguish between the two, and thus, clinical and laboratory correlation are critical. The 4 Kanavel signs, when present, favor an infectious etiology, though inflammatory causes such as rheumatoid arthritis may also result in positive Kanavel signs. A history of penetrating injury should also prompt one to be highly vigilant for infectious tenosynovitis. An intratendinous abscess, such as in our first case, is admittedly quite rare, but there are entities that can present with similar imaging features. Severe tendinosis can result in marked swelling and tenderness, though other signs typical for infection are absent, and tendinosis is usually a chronic, indolent process. Tendon tears may result in fluid-filled splits that mimic an intratendinous abscess, but again, the clinical presentation is not typical for infection. Gout, the great mimicker, can involve tendons and cause adjacent bone erosion that may raise the possibility of osteomyelitis. Overall, as with PFT, clinical and laboratory findings are paramount for making the appropriate diagnosis.


Figure 8: Proton density-weighted (8a) and fat-suppressed proton density-weighted (8b) sagittal images in a 45-year-old female with chronic anterior knee pain reveal severe patellar tendinosis (arrows). Increased signal intensity is seen throughout the tendon, but the signal changes do not suggest fluid.
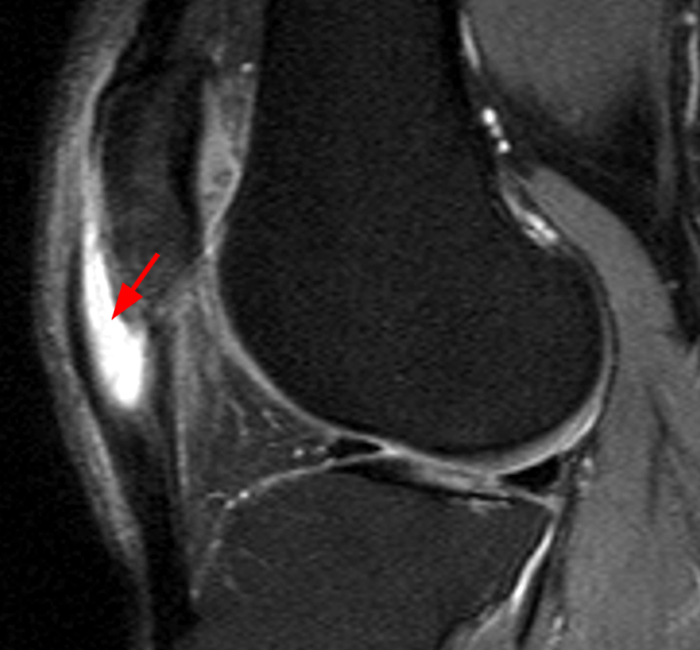
Figure 9: A fat-suppressed proton density-weighted image in a 52-year-old male with anterior knee pain reveal proximal patellar tendinosis with a fluid filled interstitial tear (arrow) involving the proximal tendon. There is minimal associated soft-tissue edema and no clinical signs of infection were present.
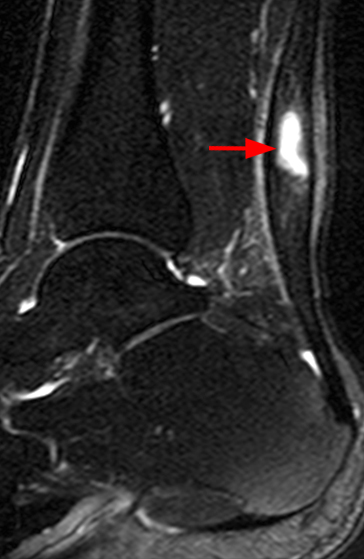
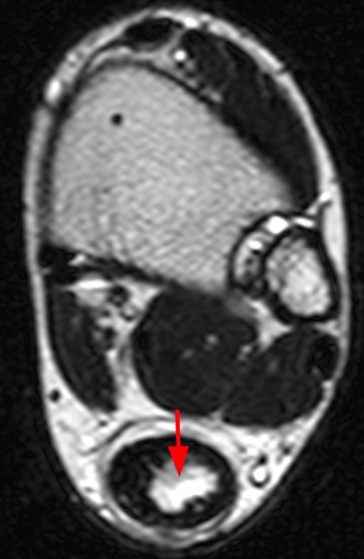
Figure 10: Fat-suppressed T2-weighted sagittal (10a) and T2-weighted axial (10b) images from a 47-year-old male who presented with a history of a palpable Achilles nodule that arose after a fall one year earlier. The sagittal image reveals fusiform swelling of the tendon compatible with chronic tendinosis. A fluid-filled interstitial tear is present within the mid tendon (arrows) on both images. The history and clinical presentation were not consistent with infection.
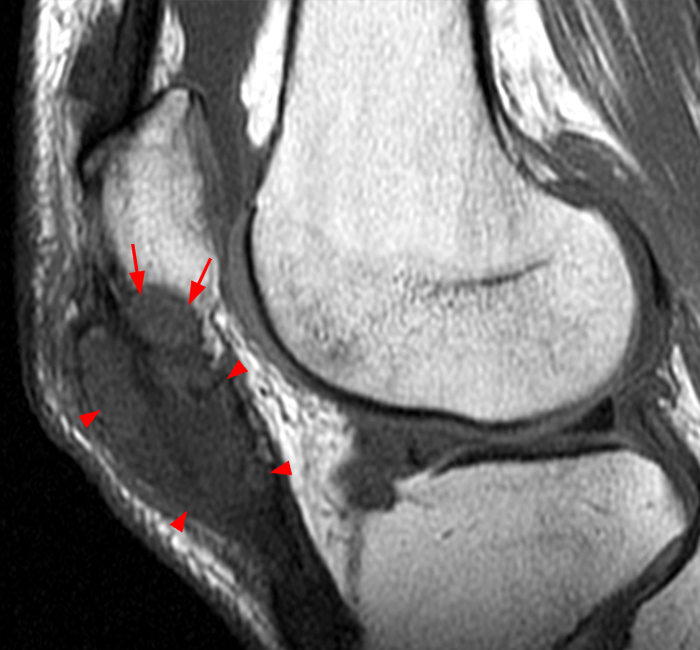
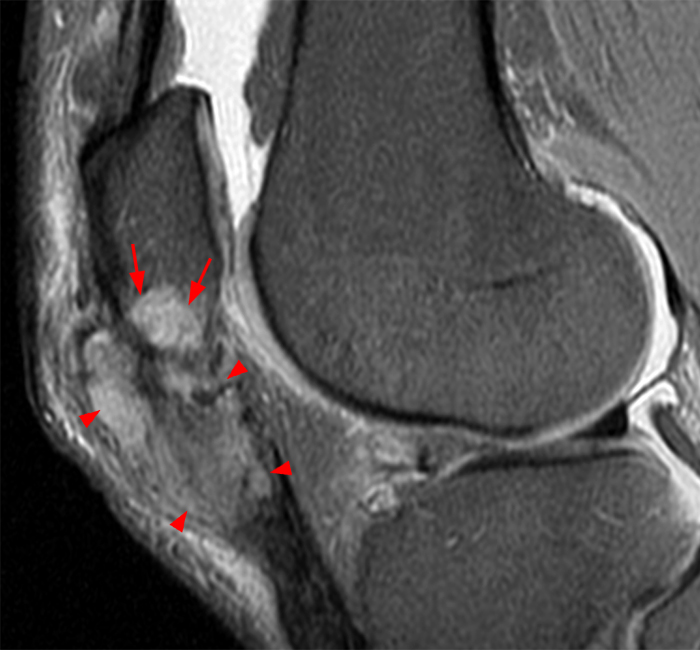
Figure 11: T1-weighted (11a) and fat-suppressed proton density-weighted (11b) sagittal images from a 58-year-old male with chronic anterior knee pain and swelling. Bulky heterogeneous enlargement of the proximal patellar tendon is present due to an infiltrating process (arrowheads), and there is extension into the caudal aspect of the patella (arrows). Gout was diagnosed at surgery.
Treatment
Tendon and peritendinous infections, the most common being pyogenic flexor tenosynovitis (PFT) in the hand, require prompt appropriate treatment in order to avoid complications. If the patient presents within 48 hours of penetrating injury, non-operative treatment including antibiotics, arm elevation, and splinting may be provided. If there is no clinical improvement or if symptoms worsen, operative intervention is required. Various surgical approaches have been described. Flexor sheath irrigation can be performed through two small incisions13. However, severe PFT or delayed presentation of PFT often requires more invasive surgical treatment and open irrigation14 The rare intratendinous abscesses, when encountered, are unlikely to heal with conservative therapy, and indeed permanent damage to the affected tendon would likely occur in the absence of operative intervention. Both the patient from the other reported case of patellar tendon abscess and the initial patient in this web clinic had successful treatment of their patellar tendon abscesses via the use of incision and drainage, followed by targeted antibiotic therapy.
Conclusion
Peritendinous infections are not uncommon, with the most likely site of involvement being the flexor tendons of the wrist and hand, in the entity known as pyogenic flexor tenosynovitis. Intrinsic tendon infection such as a patellar tendon abscess is much more rare, but both of these entities require prompt diagnosis and treatment in order to avoid permanent injury to the involved tendon(s) and adjacent structures. MRI is useful to suggest the appropriate diagnosis and to guide operative intervention, though appropriate laboratory and clinical correlation are also vital in evaluation of such patients.
References
- Glass M, Everist B, Nelson D, Spencer J. Methicillin-resistant Staphylococcal aureus patellar tendon abscess and septic prepatellar bursitis in an injection drug user. Radiology Case Reports 14 (2019): 238-241. ↩
- Merschin D, Ekkernkamp A, Seifert J. The Vulnerable Heel of Achilles: Intratendinous Abscess Following a Cat Bite. Z Orthop Unfall. 2017 Jun;155(3):324-327. ↩
- S. Konda, S. Gyftopolous, A. Dayan. Late intratendinous abscess of the Achilles tendon complicating surgical repair: a case report. Foot Ankle Int, 31 (12) (2010), pp. 1118-1121. ↩
- Saglam N, Akpinar F. Intratendinous Septic Abscess of the Achilles Tendon after Local Steroid Injection. The Journal of Foot and Ankle Surgery, 48 (5) 2009: 565-568. ↩
- Mistry K. Triceps abscess. Case study, Radiopaedia.org. https://doi.org/10.53347/rID-34772. ↩
- Glass KD. Factors related to the resolution of treated hand infections. J Hand Surg Am. 1982;7:388–394. ↩
- Kanavel A B. 1st ed. Philadelphia: PA: Lea & Febiger; 1912. The symptoms, signs, and diagnosis of tenosynovitis and major fascial space abscesses; pp. 201–226. ↩
- Kennedy CD, Lauder AS, Pribaz JR, Kennedy SA. Differentiation Between Pyogenic Flexor Tenosynovitis and Other Finger Infections. Hand (N Y). 2017 Nov;12(6):585-590. ↩
- Pang H N, Teoh L C, Yam A K, Lee J Y, Puhaindran M E, Tan A B. Factors affecting the prognosis of pyogenic flexor tenosynovitis. J Bone Joint Surg Am. 2007;89(08):1742–1748. ↩
- Fowler J R, Greenhill D, Schaffer A A, Thoder J J, Ilyas A M. Evolving incidence of MRSA in urban hand infections. Orthopedics. 2013;36(06):796–800. ↩
- han E, Roberson BF, Johnson SM. Kanavel signs of flexor sheath infection: a cautionary tale. British Journal of General Practice 2019; 69 (683): 315-316. ↩
- Pang HN, Teoh LC, Yam AKT et al. Factors Affecting the Prognosis of Pyogenic Flexor Tenosynovitis. J Bone Joint Surg Am. 2007;89:1742-8. ↩
- Carter SJ, Burman SO, Mersheimer WL. Treatment of digital tenosynovitis by irrigation with peroxide and oxytetracycline: review of nine cases. Ann Surg. 1966 Apr;163(4):645-50. ↩
- Bruner JM. The zig-zag volar-digital incision for flexor-tendon surgery. Plast Reconstr Surg. 1967 Dec;40(6):571-4. ↩
