Clinical History:
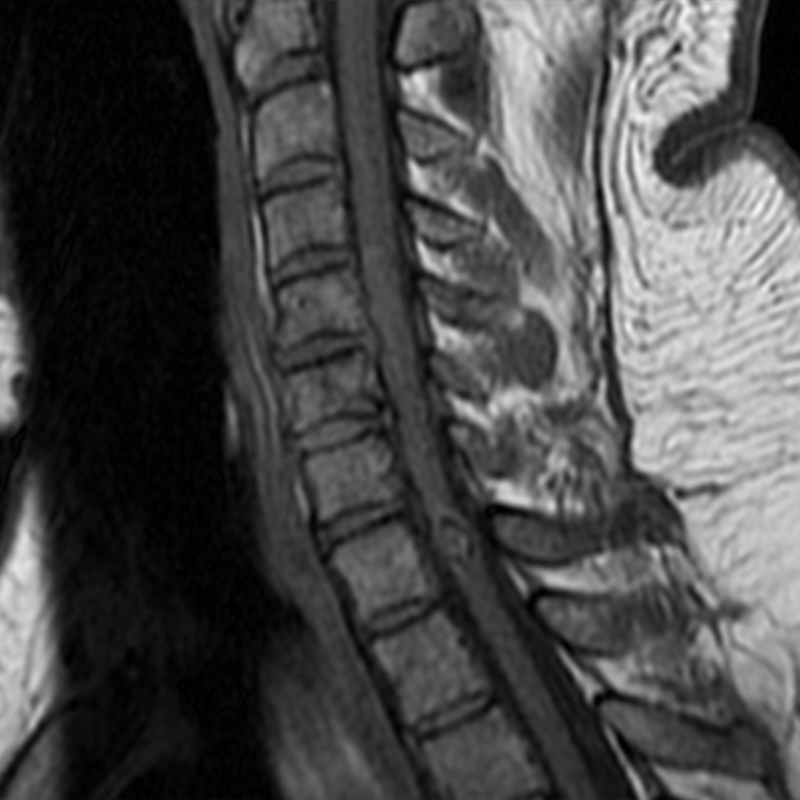
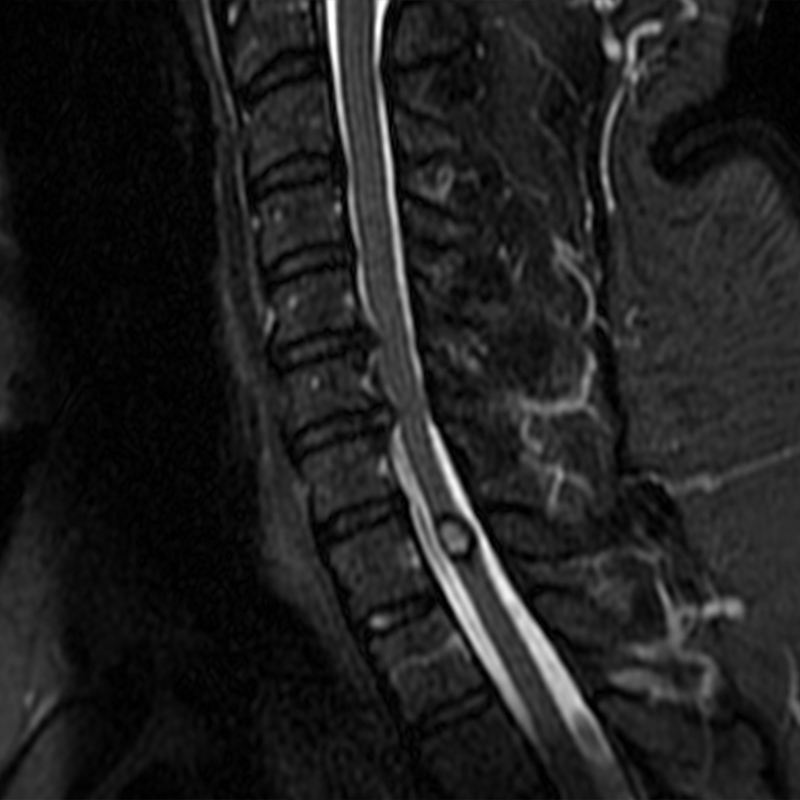
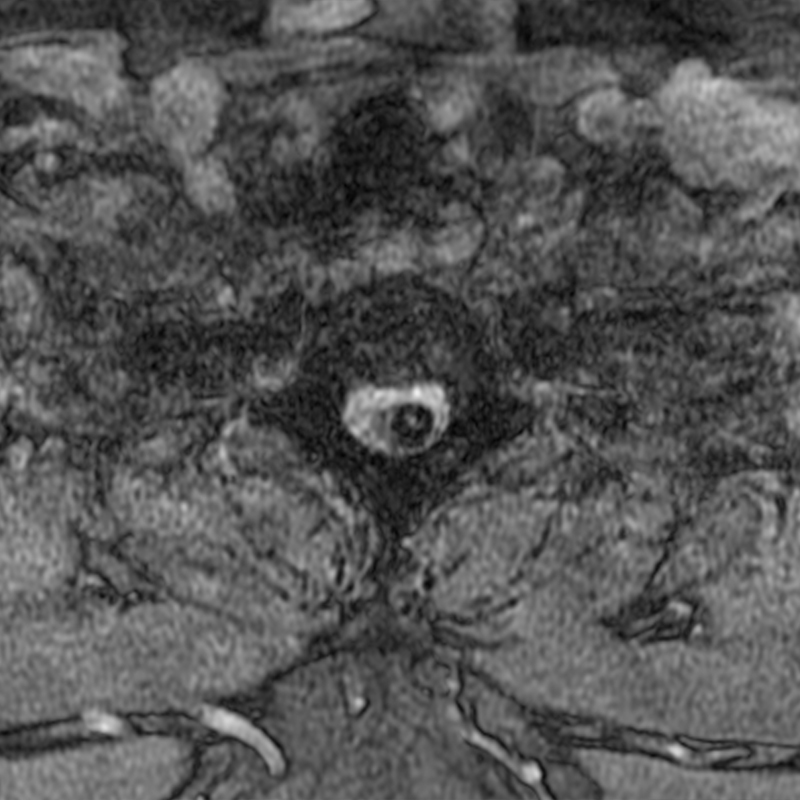
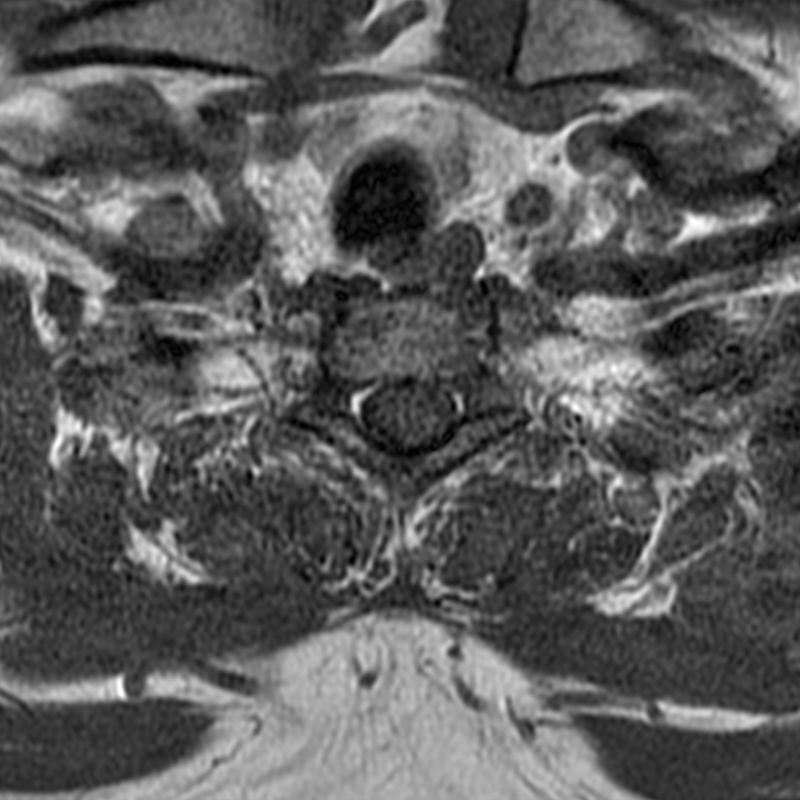
A 51-year-old male presents with pain extending into left shoulder and arm with numbness and tingling. A sagittal T2-weighted (1a), sagittal T1-weighted (1b), sagittal STIR (1c), axial T2-MEDIC gradient-echo (1d), axial T1-weighted (1e), sagittal T1-weighted fat-suppressed post-contrast (1f), and axial T1-weighted post-contrast (1g) image obtained around the time of presentation are provided. What are the findings? What is your diagnosis?

Findings



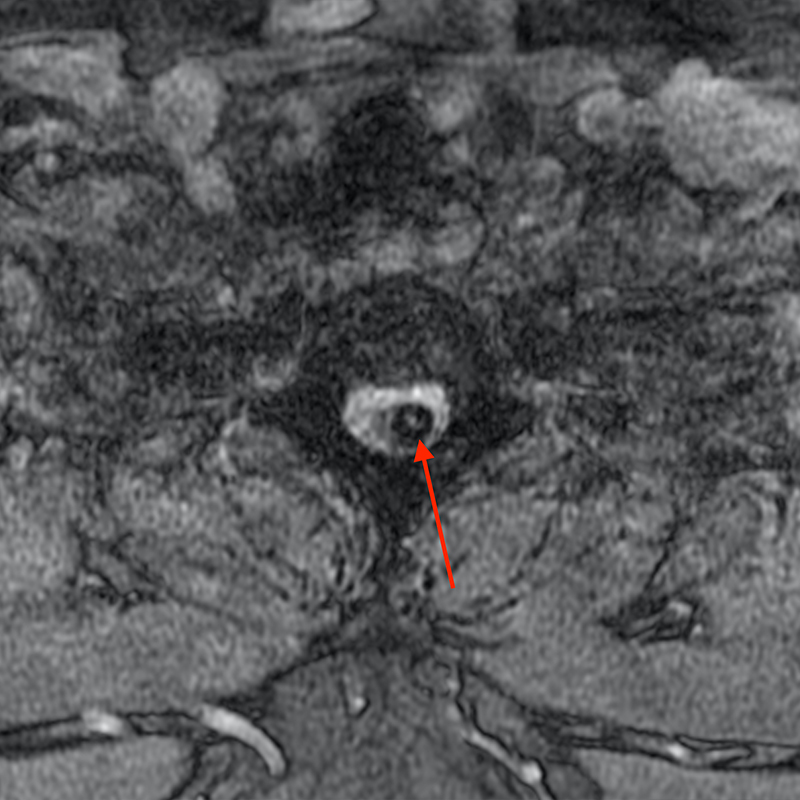
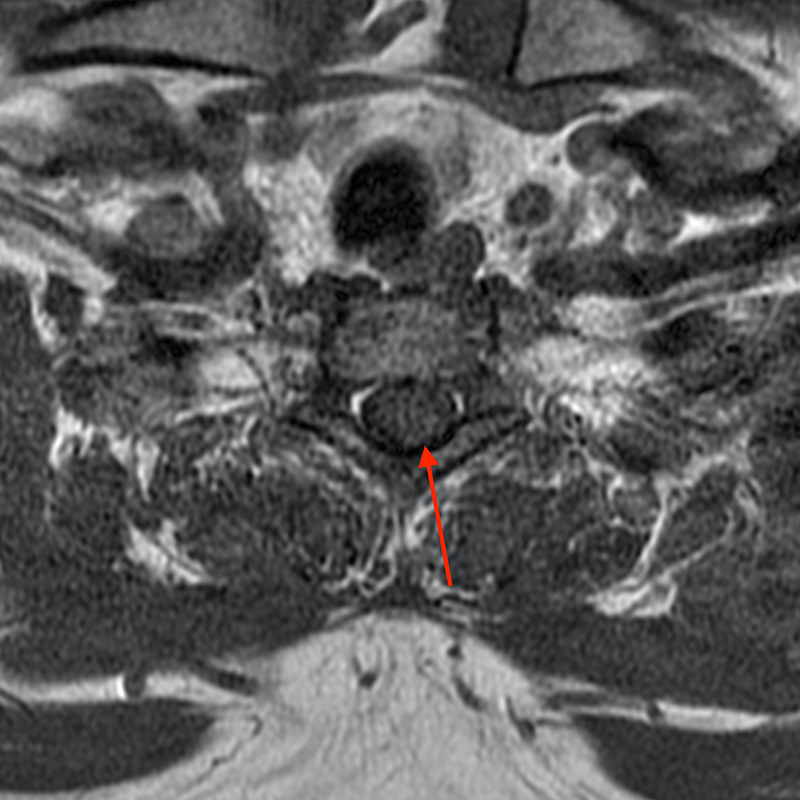

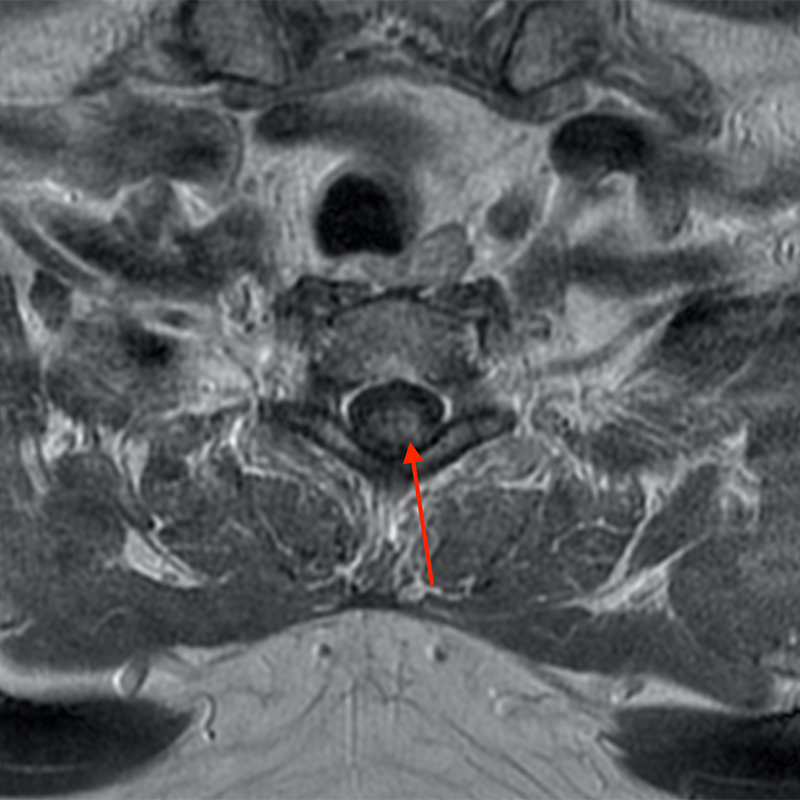
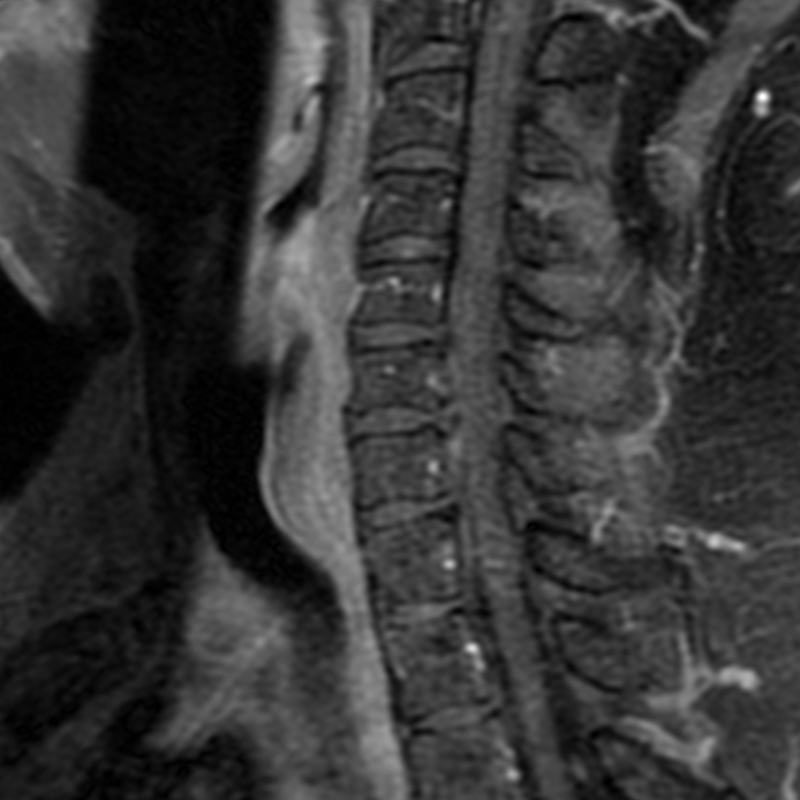
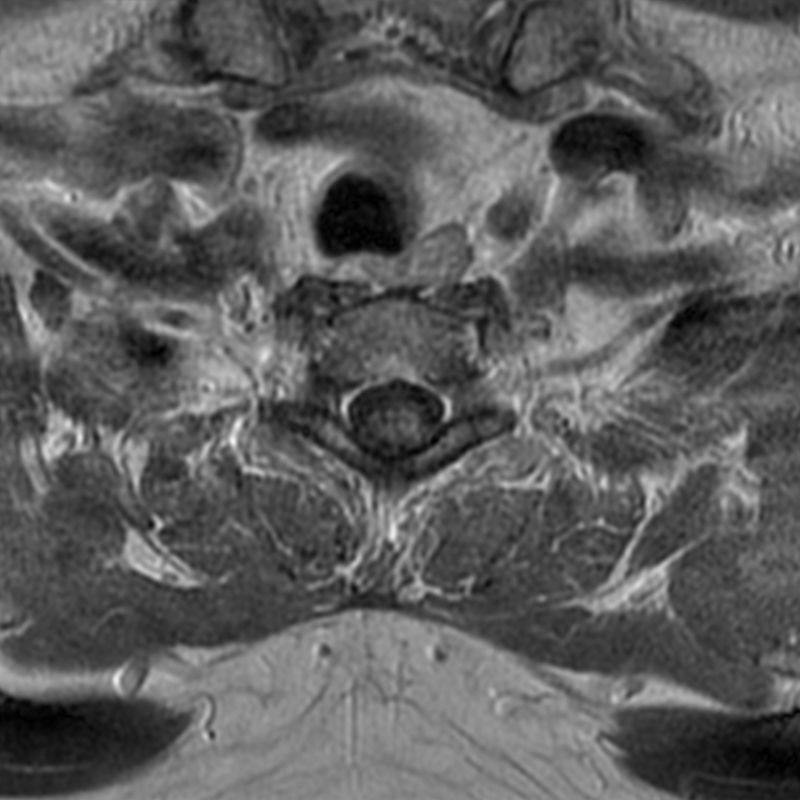
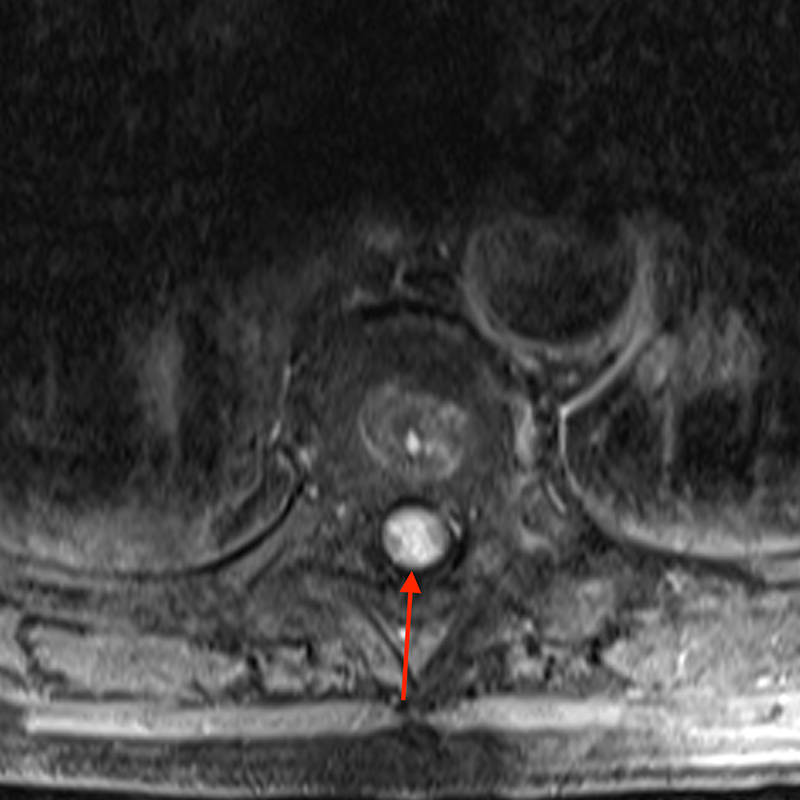
Figure 2: An ovoid T2 hyperintense and mildly T1 hyperintense lesion (red arrow) in the cervical cord with T1/T2 hypointense hemosiderin ring on sagittal T2-weighted (2a), sagittal T1-weighted (2b), and axial T1-weighted (2e) image without associated adjacent cord edema on sagittal STIR (2c) image. Blooming of hemosiderin is seen on hemorrhage sensitive axial T2-MEDIC GRE (2d) image. There is little to no enhancement on sagittal T1-weighted fat- suppressed post-contrast (2f) and axial T1-weighted post-contrast (2g) images.
Diagnosis
Spinal cavernous malformation
Introduction
Cavernous malformations are vascular malformations of the central nervous system and are uncommon, estimated to be found in 0.4-0.6% of the general population.1,2 Spinal intramedullary cavernous malformations are rare comprising only 3-5% of cavernous malformations and 5-12% of all intraspinal vascular malformations 3,4 They are comprised of endothelial lined vascular spaces of varying sizes embedded in a connective tissue matrix with no intervening normal nervous tissue though there may be gliotic and hemosiderin-stained neural parenchyma around the lesion facilitating resection.2,5,6,7 Cavernous malformations are prone to repeated hemorrhage and growth over time.
The majority of cavernous malformations are sporadic with a large meta-analysis finding associated cerebral cavernous malformations in 16.5% of patients and a family history of cavernous malformations in 11.9% of patients.8 Similarly, 80% of cerebral cavernous malformations, which have been more extensively studied, have been found to be sporadic while 20% are familial/syndromic with autosomal dominant inheritance. Several studies in patients with familial cerebral cavernous malformations have been performed and have demonstrated a prevalence of spinal intramedullary cavernous malformations in up to 70% of these patients.9 Unlike cerebral cavernous malformations, spinal cord cavernous malformations have been less well studied particularly with regards to treatment and management and tend to follow a more aggressive clinical course compared to lesions in the brain due to a lower degree of tolerance for mass lesions in the spine.10
Clinical Presentation
There is a reported equal distribution of spinal intramedullary cavernous malformations in the cervical and thoracic spine and a mean age at presentation between the 3rd-5th decade of life.2,8,11,12 A slightly higher male predominance is noted7,8,12 as opposed to higher female predominance in cerebral cavernous malformations. The majority of spinal intramedullary cavernous malformations are symptomatic at presentation and tend to present with a chronic progressive myelopathy2,8 with 5 types of clinical presentations described2:
- Type A: discrete episodes of neurological deterioration with varying degrees of recovery between episodes,
- Type B: slow progression of neurological decline,
- Type C: acute onset of symptoms with rapid decline,
- Type D: acute onset of mild symptoms with subsequent gradual decline lasting weeks to months and (5) Type E: asymptomatic incidentally detected lesions.
A combination of motor/sensory/pain/sphincter symptoms is most common at presentation.12 The annual retrospective rate of hemorrhage is calculated to be 1.4-6.8% per person per year.1,7,8,11,12
Imaging Findings
Spinal intramedullary cavernous malformations are best imaged by MRI. These lesions can be seen by CT with hemorrhage in the cord but smaller lesions may be occult. The finding of popcorn morphology classically described for cerebral cavernous malformations is not typically seen for spinal intramedullary cavernous malformations.13 Cavernous malformations in the cord most commonly demonstrate a T2 hypointense rim due to hemosiderin with heterogenous T1 and T2 hyperintensity.14 Adjacent intramedullary hemorrhage is common, most commonly bidirectional and eccentric (Figure 3). Perilesional edema or significant mass effect is not commonly seen, as opposed to other intramedullary masses. There is typically no significant enhancement on contrast-enhanced images.


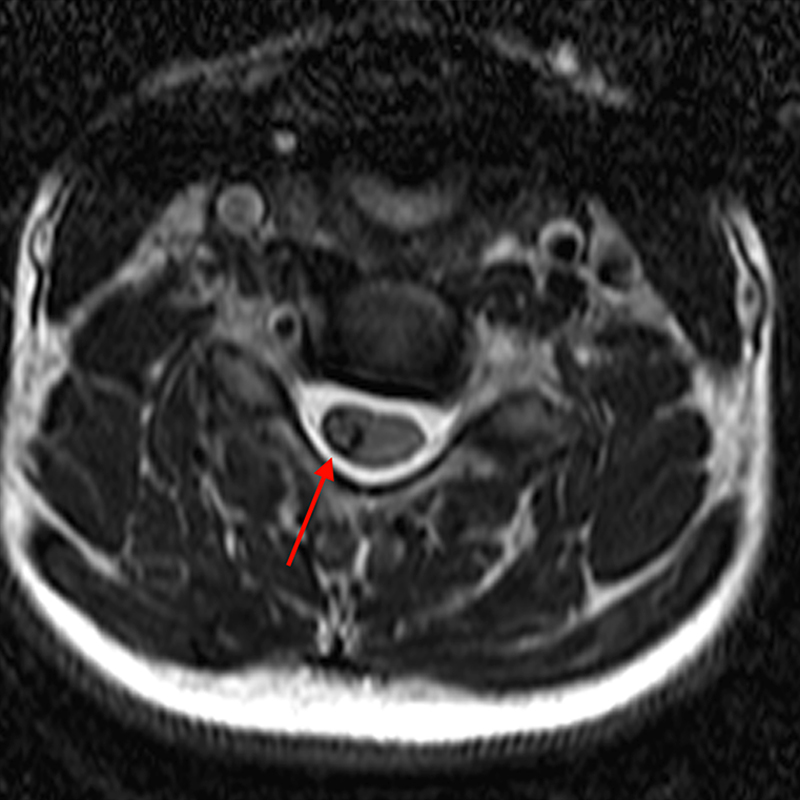
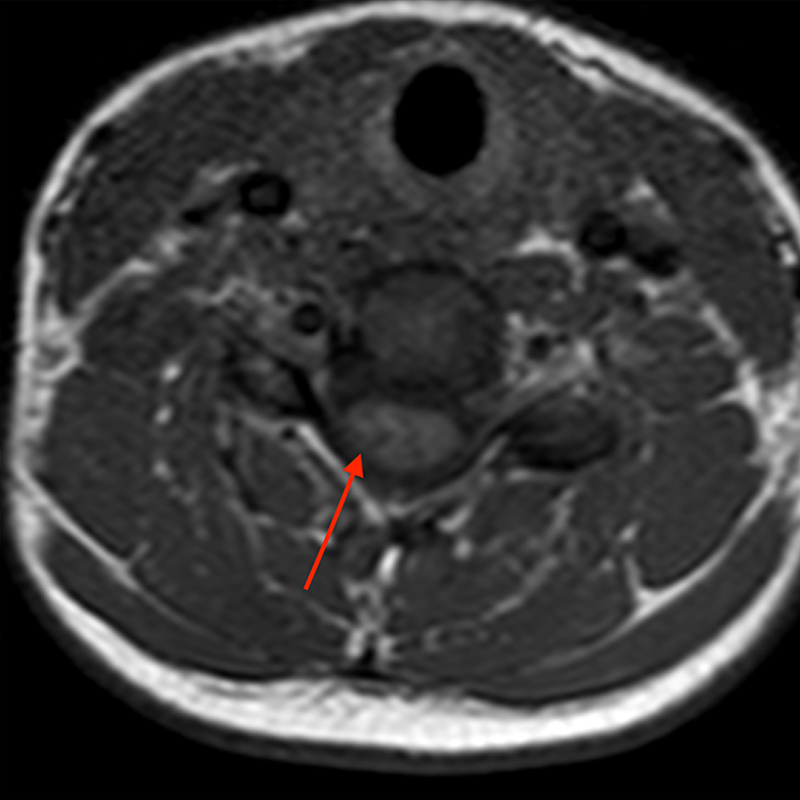
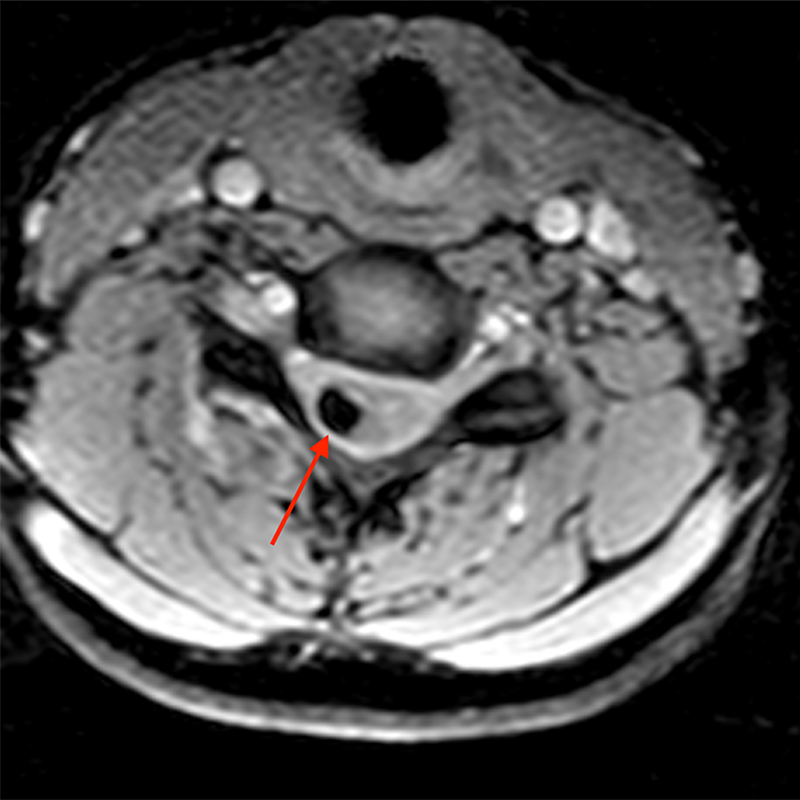

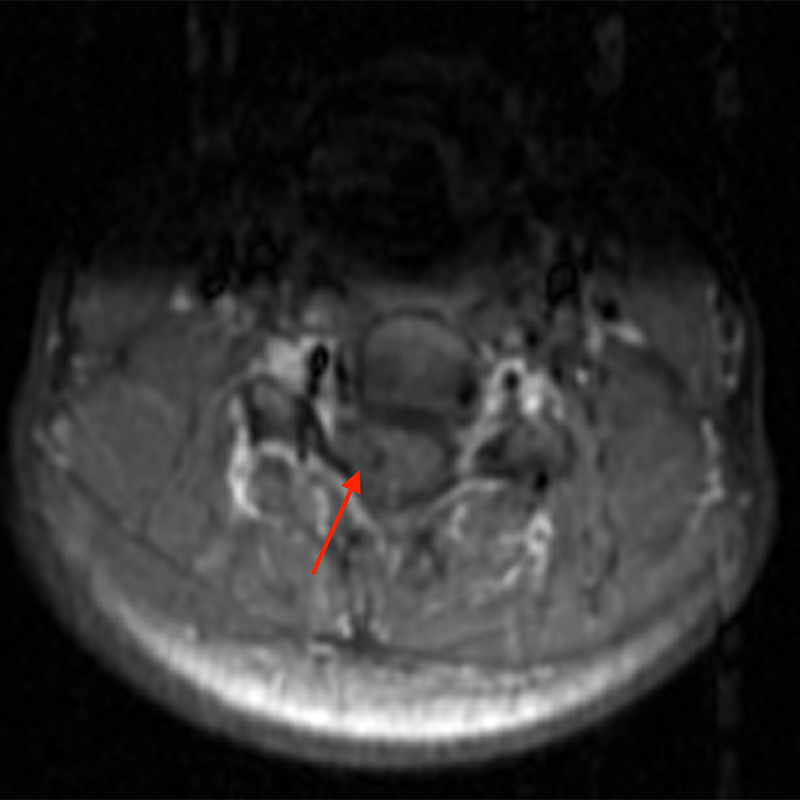
Sagittal T2-weighted (3a) and axial T2-weighted image (3c) of the cervical spine demonstrate a T2 hyperintense lesion (red arrow) with a hypointense hemosiderin rim that extends cranially and caudally. The lesion is mostly isointense to cord on sagittal T1-weighted (3b) and axial T1-weighted (3d) images. Axial FFE (3e), a hemorrhage sensitive sequence, demonstrates significant blooming of hemosiderin. There is no demonstrable enhancement on post-contrast sagittal T1-weighted fat- suppressed (3f) and axial-T1-weighted fat- suppressed (3g) images.
Appropriately sensitive sequences should be used in imaging, since additional lesions may be found at other levels of the spinal cord or within the brain (Figure 4), and may change the presumptive diagnosis from sporadic to genetic disease, and thereby the overall management.
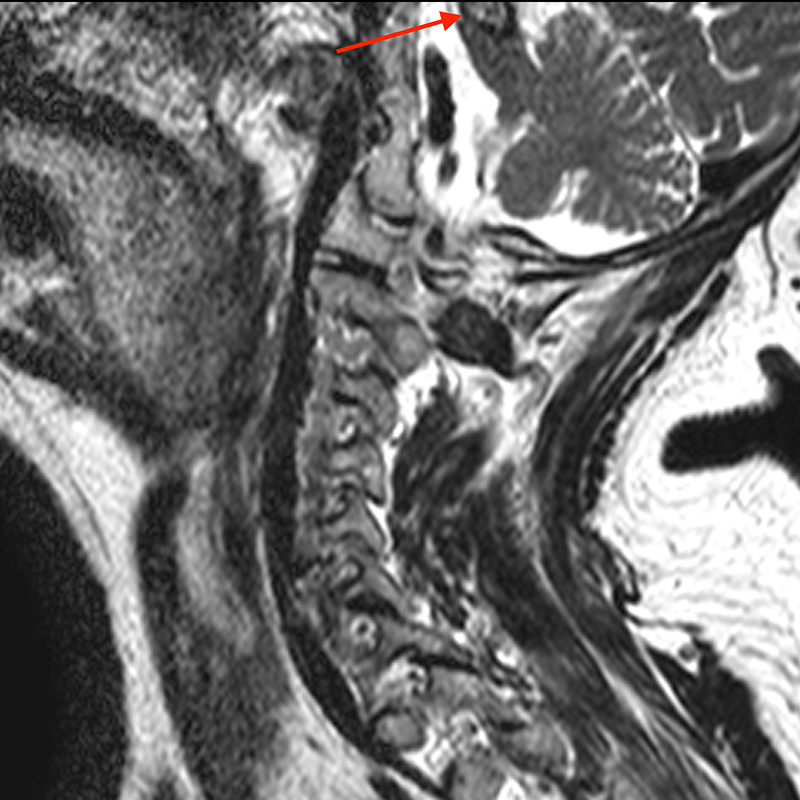
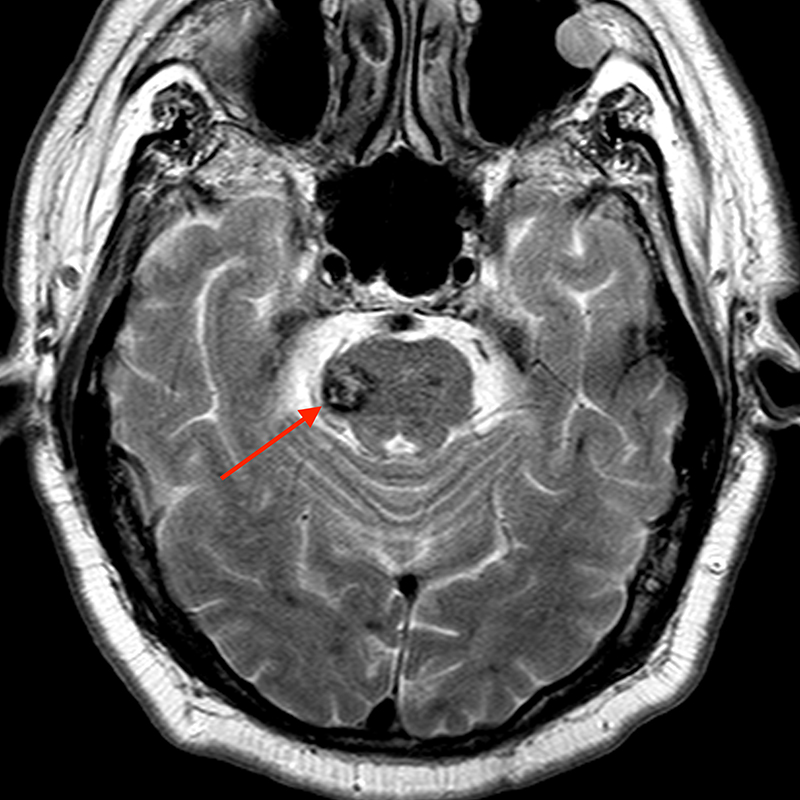
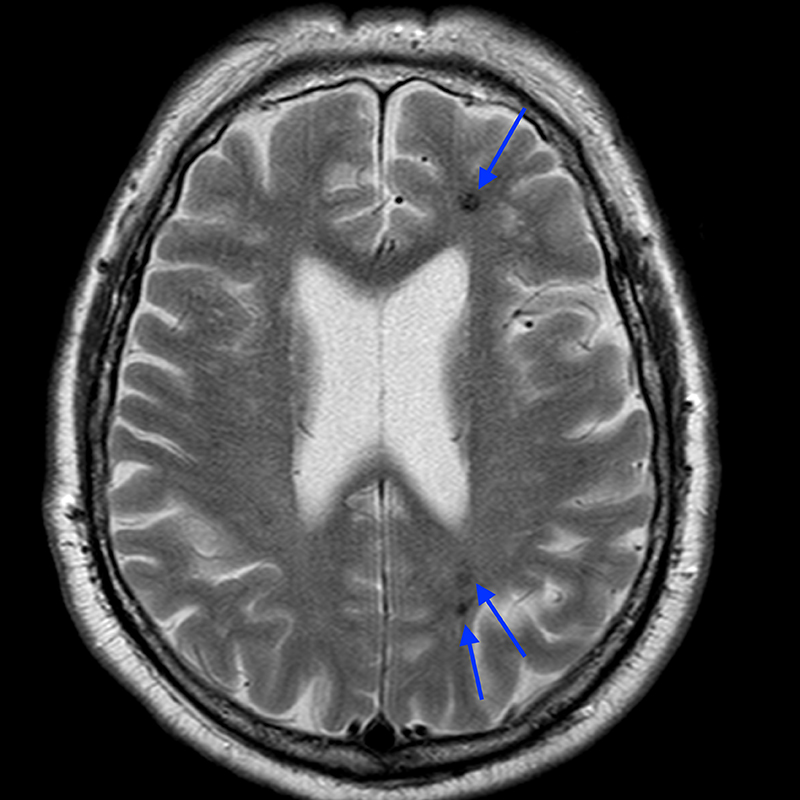
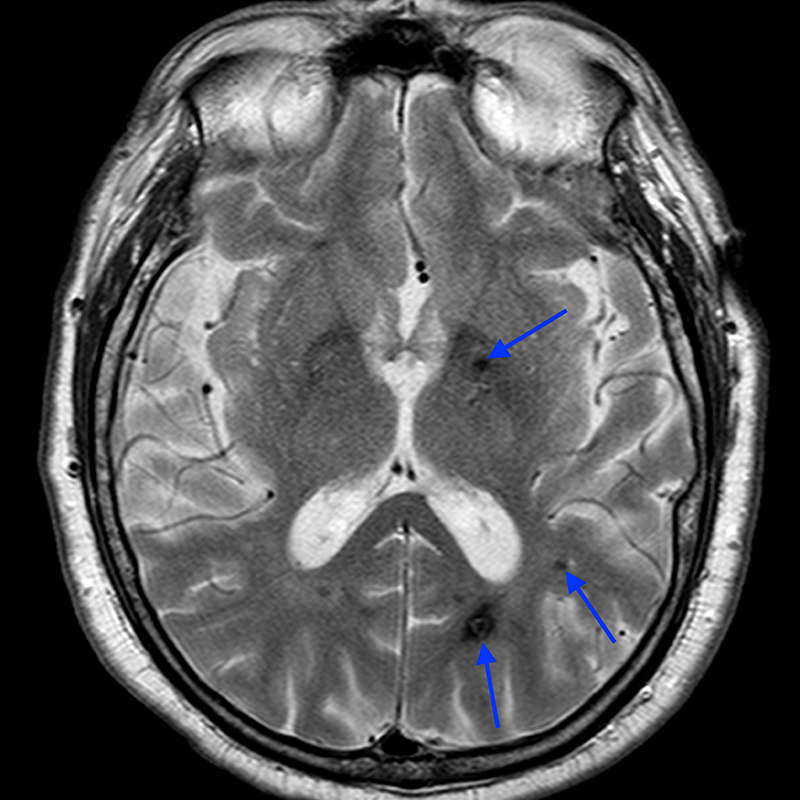
Sagittal T2-weighted image (4a) of the cervical spine incidentally demonstrating a partially visualized T2 heterogenous lesion with hypointense hemosiderin ring (red arrow). Additional brain imaging with axial T2-weighted (4b) image of the lesion partially seen on cervical spine exam demonstrates a popcorn-appearing lesion in the right aspect of the pons (red arrow) with a hemosiderin ring. Numerous additional T2 hypointense hemosiderin (blue arrow) stained lesions are seen throughout the supratentorial and infratentorial brain (4c and 4d). Fortunately, these could be seen on axial T2-weighted images even though GRE or SWI sequences were not performed.
Differential Diagnosis
- Intramedullary AVM
- Spinal cord neoplasms
- Post-traumatic sequelae
- Post-infectious sequelae
The presence of flow voids are typical of intramedullary arteriovenous malformations (AVM), which are high flow lesions, and not seen with low flow cavernous malformations, although a thrombosed or partially thrombosed intramedullary arteriovenous malformation may not be excluded. Intramedullary neoplasms may be associated with hemorrhage, particularly ependymomas and hemangioblastomas, but they rarely demonstrate a mix of subacute and chronic hemorrhage (Figure 5). Ependymomas can be associated with a hemosiderin cap that may have a similar appearance to the hemosiderin ring seen with cavernous malformations. But, in contrast, cavernous malformations often lack significant cord expansion and edema despite the fact that they can result in mass effect when associated with acute hemorrhage.
A good history and a range of labs should exclude traumatic and infectious etiologies. In most cases contrast-enhanced MRI should be performed and if needed, an MRA or DSA can be performed to exclude other vascular malformations.
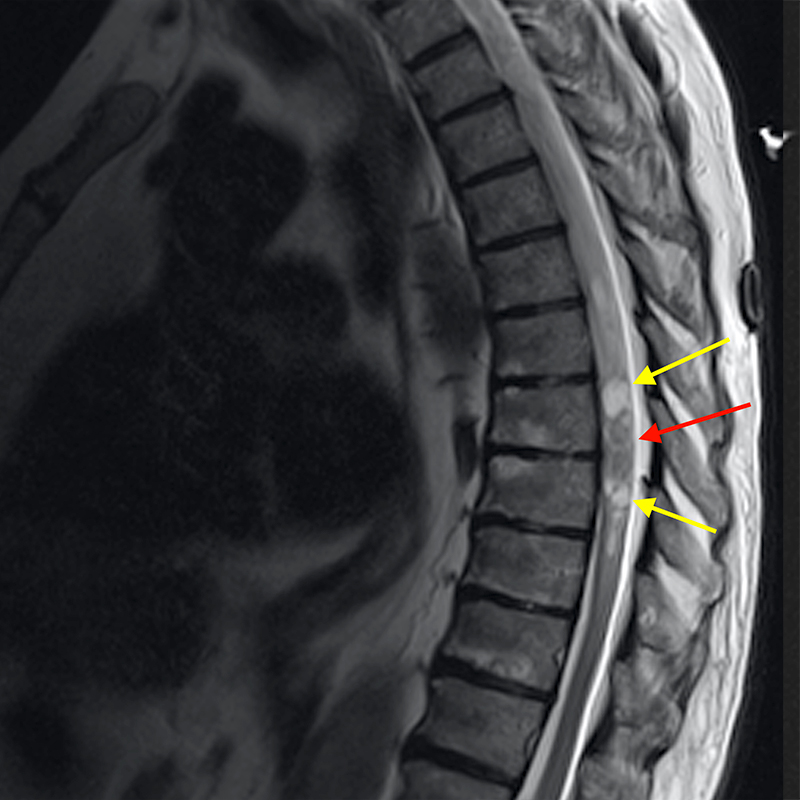
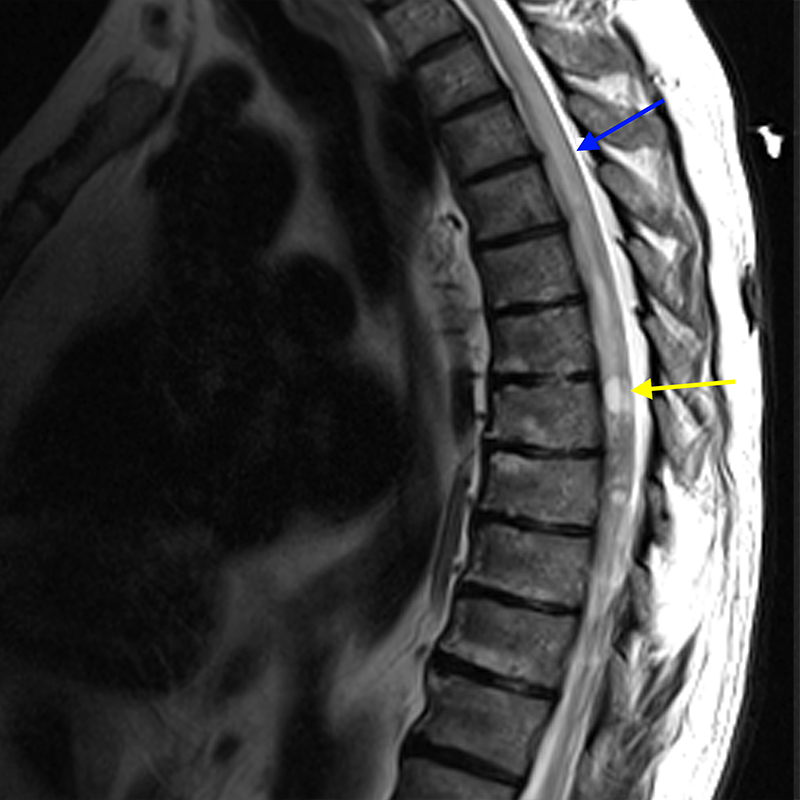
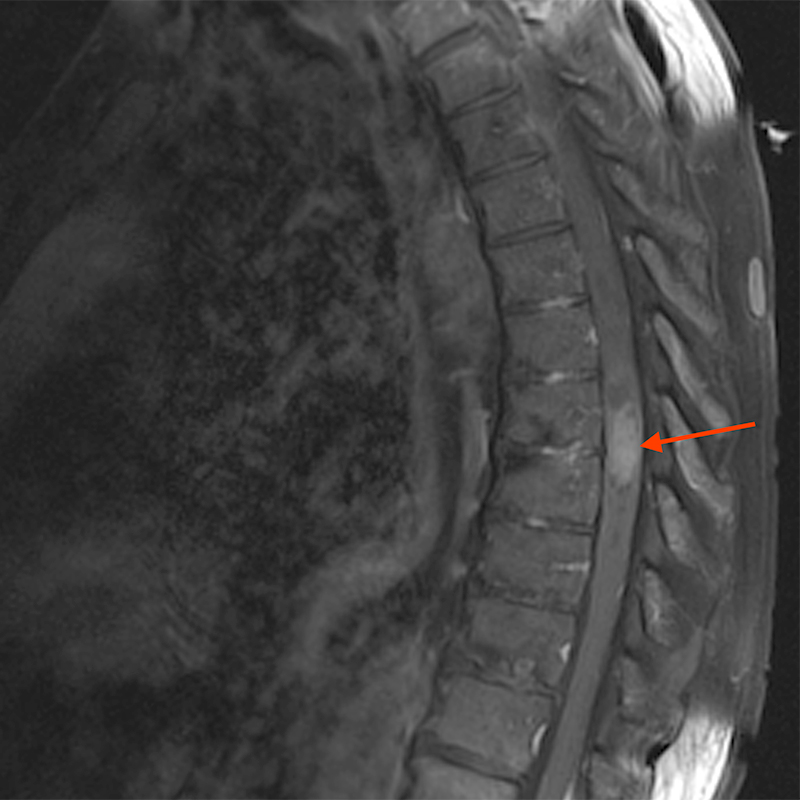
Sagittal T2-weighted images (5a, 5b) in a 72-year-old male patient with presumed spinal ependymoma versus astrocytoma presenting with numbness and tingling in both legs without pain. A large heterogenous T2 hyperintense cord lesion (red arrow) is seen expanding the cord with associated cord edema (blue arrow) and intratumoral/peritumoral cysts (yellow arrows). There is avid enhancement of the central solid-appearing lesion (red arrow) on post-contrast sagittal T1-weighted fat-suppressed (5c) and axial T1-weighted fat- suppressed (5d) images.
Treatment and Management
A consensus management is not established as it is for cerebral cavernous malformations.15 Most articles report results following surgical resection and may be biased. There is limited data on the history and outcomes of conservative management7, 12 though intramedullary cavernous malformation tend to follow a more aggressive course than cerebral cavernous malformations. As noted above, calculated retrospective annual hemorrhage rates are 1.4-6.8% per person per year but based on clinical profile, symptomatic patients and those with prior history of hemorrhage, have higher annual rates of hemorrhage of 9.9% and 9.7%, respectively.12 Overall hemorrhage rates may be low but the cumulative risk in younger patients may justify surgical resection. A positive association has been found between favorable post-surgical outcome and larger size of the lesion (>1 cm). Thus, larger lesions may benefit from early surgery to prevent subsequent hemorrhage and neurological worsening.8, 12 In addition to size, time to surgery <3 months, surgical technique via hemilaminectomy, gross total resection and predominantly motor symptoms have been noted to be predictive of an improved neurological outcome following surgery. Preoperative pain and sensory symptoms are suggested to be predictive of poor postoperative neurological recovery. Most authors are skeptical of the efficacy of lesion resection to improve pain. Standard guidelines with respect to diagnostic and follow-up imaging, surgical treatment and medical management, and genetic testing have not been established for spinal cavernous malformations.
Conclusion
Intramedullary cavernous malformations are an uncommon benign entity that can be found in the spinal cord, sometimes incidentally on spine imaging or during acute presentation for a combination of motor, sensory, and pain symptoms. On acute presentation, they can be mistaken for more aggressive lesions such as malignant neoplasms with acute hemorrhage and perilesional edema, but they typically also have combined findings of chronic hemorrhage (hemosiderin ring) and lack significant enhancement or edema relative to the size of the lesion. The natural course of cavernous malformations in the cord is not as well established as it is for cerebral cavernous malformations but due to higher propensity for symptomatic mass effect in the spine, most of the available literature on management and treatment is based on surgical outcomes. There may be a certain subset of patients for which surgery is beneficial such as lesions > 1cm in size or those presenting with motor symptoms. More studies are needed to establish the optimal protocol for follow-up and management.
References
- Gross Ba, Lin N, Du R, et al. The natural history of intracranial cavernous malformations. Neurosurg Focus 2011;26. ↩
- Ogilvy CS, Louis DN, Ojemann RG: Intramedullary cavernous angiomas of the spinal cord: clinical presentation, pathological features, and surgical management. Neurosurgery 1992, 31:219–229. ↩
- Ghogawala Z, Ogilvy CS. Intramedullary cavernous malformations of the spinal cord. Neurosurg Clin N Am. 1999 Jan;10(1):101-11. PMID: 9855652. ↩
- Gross Ba, Du R, popp aJ, et al. Intramedullary spinal cord cavernous malformations. Neurosurg Focus 2010;40. ↩
- Lanzino G. Cavernous malformations of the brain and spinal cord. Thieme, 2011. ↩
- Duke BJ, Levy AS, Lillehei KO. Cavernous angiomas of the cauda equina: case report and review of the literature. Surg Neurol. 1998 Nov;50(5):442-5. doi: 10.1016/s0090-3019(97)00354-6. PMID: 9842868. ↩
- Zhang L, Yang W, Jia W, et al. comparison of outcome between surgical and conservative management of symptomatic spinal cord cavernous malformations. Neurosurgery 2016;78:552–61. ↩
- Badhiwala Jh, Farrokhyar F, alhazzani W, et al. surgical outcomes and natural history of intramedullary spinal cord cavernous malformations: a single- center series and meta-analysis of individual patient data. J Neurosurg Spine 2014;26:662–76. ↩
- Mabray MC, Starcevich J, Hallstrom J, Robinson M, Bartlett M, Nelson J, Zafar A, Kim H, Morrison L, Hart BL. High Prevalence of Spinal Cord Cavernous Malformations in the Familial Cerebral Cavernous Malformations Type 1 Cohort. AJNR Am J Neuroradiol. 2020 Jun;41(6):1126-1130. ↩
- Deutsch H, Jallo GI, Faktorovich A, Epstein F. Spinal intramedullary cavernoma: clinical presentation and surgical outcome. J Neurosurg. 2000 Jul;93(1 Suppl):65-70. doi: 10.3171/spi.2000.93.1.0065. PMID: 10879760. ↩
- Zevgaridis D, Medele RJ, Hamburger C, Steiger HJ, Reulen HJ. Cavernous haemangiomas of the spinal cord. A review of 117 cases. Acta Neurochir (Wien). 1999;141(3):237-45. ↩
- Goyal A, Rinaldo L, Alkhataybeh R, Kerezoudis P, Alvi MA, Flemming KD, Williams L, Diehn F, Bydon M. Clinical presentation, natural history and outcomes of intramedullary spinal cord cavernous malformations. J Neurol Neurosurg Psychiatry. 2019 Jun;90(6):695-703. ↩
- Panda A, Diehn FE, Kim DK, Bydon M, Goyal A, Benson JC, Carr CM, Rinaldo L, Flemming KD, Lanzino G. Spinal Cord Cavernous Malformations: MRI Commonly Shows Adjacent Intramedullary Hemorrhage. J Neuroimaging. 2020 Sep;30(5):690-696. ↩
- Weinzierl MR, Krings T, Korinth MC, Reinges MH, Gilsbach JM. MRI and intraoperative findings in cavern- ous haemangiomas of the spinal cord. Neuroradiology 2004;46(1):65–71. ↩
- Akers A, Al-Shahi Salman R, A Awad I, Dahlem K, Flemming K, Hart B, Kim H, Jusue-Torres I, Kondziolka D, Lee C, Morrison L, Rigamonti D, Rebeiz T, Tournier-Lasserve E, Waggoner D, Whitehead K. Synopsis of Guidelines for the Clinical Management of Cerebral Cavernous Malformations: Consensus Recommendations Based on Systematic Literature Review by the Angioma Alliance Scientific Advisory Board Clinical Experts Panel. Neurosurgery. 2017 May 1;80(5):665-680. ↩
