Clinical History: A 22-year-old female softball player presented with right shoulder pain. T1-weighted fat-suppressed (T1 FS) coronal (1a and 1b), axial (1c), and sagittal (1d) magnetic resonance arthrographic (MRA) images and a selected video clip from arthroscopy (1e) are provided. What are the findings? What is the diagnosis?

1a
")
1b

1c

1d

1e
Figure 1
Findings
")
2a
")
2b

2c

2d

2e
Figure 2:
Sequential coronal T1 FS MRA images from anterior to posterior (2a and 2b) and axial T1 FS MRA image (2c) demonstrate continuous detachment of the superior and anterosuperior glenoid labrum from the 11 o’clock to the 1 o’clock position (arrows). The sagittal T1 FS MRA image (2d) demonstrates involvement of the long head of the biceps tendon (arrow) (2d). The tear is confirmed on the arthroscopic video, which shows insertion of the probe beneath the bucket-handle tear, with the tear also involving the tendon of the long head of the biceps brachii muscle (2e). Case provided courtesy of Eric Y. Chang, M.D. Click here to watch.
Diagnosis
Bucket-handle tear of the superior labrum with involvement of the long head biceps tendon (SLAP IV lesion).
Introduction
Being able to distinguish anatomic variants of the superior portion of the labrum from pathologic abnormalities, such as superior labrum anterior posterior (SLAP) lesions, can be a diagnostic challenge for radiologists, yet this ability can guide patient care. In this web clinic, we discuss and illustrate the anatomy of the superior labrum, some of its anatomic variations, and patterns of labral failure, emphasizing those MR imaging features that allow differentiation between what is considered normal and what is regarded as pathologic.
The glenoid labrum serves as an anchor for various tendinous and capsuloligamentous structures about the shoulder, significantly contributing to glenohumeral joint stability.1 The labra that are found in the glenohumeral joint and hip are complex fibrocartilaginous structures and function to deepen the concavity of the glenoid fossa and acetabular fossa, respectively, thus increasing the width, depth, and area of the articular surface. Histologically, the glenoid labrum consists of chondrocytes within a proteoglycan matrix.2
The attachment of the glenoid labrum differs superiorly compared to inferiorly. Superiorly, the labrum is loosely adherent to the glenoid rim, and there is a cleft composed of cellular tissue serving as an interface between the labrum and the cartilage and bone, permitting significant mobility of the superior labrum.3 In contrast, the inferior labrum is firmly attached to the glenoid rim with an elevated bone ridge, contributing to its relative immobility.
As demonstrated in the index case, the labrum is particularly susceptible to injury in persons, especially athletes, whose activities include frequent throwing, whether it relates to overhead throwing as in baseball, volleyball, and handball, or to underhand throwing as in softball pitchers, especially those who use the windmill pitching delivery. Because the results of the clinical examination in patients with labral injury are often non-specific, advanced imaging plays an important role in identifying such lesions.1,4 MR imaging and, especially, direct MR arthrography, in which contrast agent is injected into the joint, are recognized as the most effective imaging methods in the assessment of the glenoid labrum.4,5,6
Pertinent Anatomy
Glenoid Cavity
The morphology of the glenoid cavity is commonly described as “pear shaped” given its central narrowing and broad base (Figure 3). Of interest in this regard, one of the authors visited a local grocery store to find a pear that resembled the shape of the glenoid cavity but was unsuccessful in this search (although the store did not sell English pears that may have provided a useful specimen). Rather, nearby in the store, there was a collection of avocados, many of which resembled the shape of the glenoid cavity.

3a

3b
Figure 3:
Glenoid cavity. Schematic depiction (3a) of the glenoid contour with the analogous avocado(3b). ANT: Anterior, POST: Posterior. Please note that the lower two-thirds of the glenoid cavity approaches the shape of a circle. (b, courtesy of Amin Matin, M.D.)

4a
Figure 4:
Glenoid ossification centers. The superior subcoracoid ossification center (blue) and three inferior ossification centers (green) are shown in this illustration.
The glenoid cavity develops from one superior and multiple inferior ossification centers (Figure 4). The superior ossification center, termed the subcoracoid, or infracoracoid, ossification center, originates at the base of the coracoid process and forms the superior one-third of the glenoid articular surface.7 The inferior ossification centers form the lower two-thirds of the glenoid articular surface. The subcoracoid ossification center typically develops between eight and ten years of age with maturation of its development by sixteen to seventeen years of age.8 The inferior ossification centers appear at fourteen to fifteen years of age and typically become mature at seventeen to eighteen years of age.8 The posterior point of fusion of these superior and inferior ossification centers has been associated with the development of an abnormality referred to as a glenoid articular rim divot, or GARD lesion (Figure 5).9 This posterosuperior osteochondral abnormality typically occurs at the 9 – 10 o’clock position (see following discussion of the glenoid clock face), and it may be related to posterior subluxation of the humeral head. The GARD lesion involves the articular rim, distinguishing it from osteochondritis dissecans, which typically involves the glenoid fossa.
")
5a

5b

5c
Figure 5:
Glenoid articular rim divot (GARD) lesion. Sagittal (5a) and coronal (5b) T1 FS MRA images demonstrate an osteochondral abnormality involving the articular rim at the point of fusion of the superior and inferior ossification centers (arrows). The accompanying illustration (5c) depicts the point of fusion (arrow) between the superior (gray) and inferior (turquoise) ossification centers. It is the involvement of the posterior glenoid rim that separates a GARD lesion from osteochondritis dissecans, which generally is more centrally located. ANT: Anterior, POST: Posterior. Figure 5a, 5b, reprinted from Internal Derangements of Joints; 2nd Edition. Resnick D., Kang H.S., Pretterklieber M.L. (2007) with permission from Elsevier.
The glenoid clock face is often used as a method to quickly identify specific regions of the glenoid labrum. Generally, but not invariably, this method assigns the 12 o’clock position as superior, 3 o’clock position as anterior, 6 o’clock position as inferior, and 9 o’clock position as posterior (Figure 6a). As will be detailed later, the clock face analogy is also used to establish labral quadrants (Figure 6b). Of note, in the orthopaedic surgical literature, many surgeons flip the clockface based on right or left, such that 3 o’clock is anterior in the right shoulder but posterior in the left.
")
6a
")
6b
Figure 6:
Glenoid clock face. Sagittal T1 FS MRA image (6a) shows the glenoid clock face, with the 12 o’clock position assigned as superior, 3 o’clock position as anterior, 6 o’clock as inferior, and 9 o’clock as posterior. The six anatomic quadrants of the labrum are applied to the same image in 6b. C: Coracoid process, G: Glenoid, A: Acromion, S: Superior, AS: Anterosuperior, AI: Anteroinferior, PS: Posterosuperior, PI: Posteroinferior, I: Inferior.
Periarticular Fiber System
Within the labrum can be found longitudinal circumferential collagen fibers that encircle the glenoid cavity. Nearby, there is a periarticular fiber system (PAFS), which represents the collagenous framework that connects the collagen within the labrum to the collagen fibers of the multiple structures that attach to the labrum. This framework provides a useful concept in understanding the mechanism of labral tears and detachments. Owing to the collagenous connections between the glenoid labrum and the glenohumeral ligaments and tendons of the long heads of the biceps and triceps brachii muscles, traction forces placed on those structures can be transferred to the labrum itself.3,10,11 Specifically, the PAFS serves as a “tension brace” throughout the glenohumeral joint, and a composite vector force placed on this framework may be transmitted to the labrum, ultimately resulting in a tear or detachment (Figure 7).10 Such a force occurring in the anterosuperior portion of the labrum can cause a superior labral tear or detachment, including variations of a SLAP lesion. In patients with a relatively high labral attachment of the middle glenohumeral ligament (MGHL), nearer the labral attachment of the SGHL, a vector force applied to the superior labrum is of greater magnitude and may result in a more extensive labral abnormality than in patients with a more inferiorly positioned MGHL.
The concept of the peel-back lesion, referring to posterosuperior labral injury related to abduction and external rotation about the shoulder, is another application of the PAFS framework.12 With the shoulder in abduction and external rotation, the biceps tendon rotates posteriorly, causing the composite vector applied to the superior labrum to be transmitted posterosuperiorly rather than anterosuperiorly (see Figure 7c).12 Therefore, in this position, which occurs commonly in the shoulder in the dominant arm of a baseball pitcher, a SLAP lesion of the labrum would be expected to begin posterosuperiorly.

7a

7b

7c
Figure 7:
Periarticular Fiber System (PAFS). Illustration (7a) depicts the PAFS (upper arrows), which is a collagenous framework that connects the circumferential collagen fibers (lower arrow) of the labrum to those ligamentous and tendinous structures that attach to the labrum. Application of tensile forces to the glenohumeral ligaments and long head of the biceps tendon results in an anterosuperior composite vector force transmitted to the labrum, resulting in a tear or detachment (7b). That composite vector has a greater magnitude when the middle glenohumeral (MGHL) has a high attachment to the labrum. With abduction and external rotation of the shoulder as shown in the animation (7c), click here to view, the biceps tendon rotates posteriorly, causing the composite vector to be transmitted posterosuperiorly, which would be expected to cause a SLAP lesion beginning in the posterosuperior portion of the labrum. SGHL: Superior glenohumeral ligament.
Labrum
- Normal MR Appearance of the Labrum
As a fibrocartilaginous structure attached to the glenoid rim, the normal labrum displays low signal intensity on all MR imaging sequences, although in older persons, owing to the presence of labral degeneration, gentle “graying” of the labrum may be visible. The typical normal labral morphology is triangular; however, the normal labrum has also been described as round, flat, cleaved, notched, or absent (Figure 8).13,14 These additional shapes, however, may be indicative of degenerative labral alterations occurring in asymptomatic persons, especially with advancing age, rather than representing the morphology of an entirely normal labrum.

8a

8b
Figure 8:
Normal labrum. Coronal (8a) and axial (8b) T1 FS MRA images in a 24-year-old patient show a normal labrum (arrows). H: Humeral Head, G: Glenoid.
- Anatomic Quadrants of the Labrum
The application of the glenoid clock face also delineates six anatomic quadrants, or zones, of the labrum. The six labral quadrants are described as: superior, anterosuperior, anteroinferior, inferior, posteroinferior, and posterosuperior in location (see Figure 6b). Those portions of the labrum, particularly from about 10 o’clock to 3 o’clock, representing the posterosuperior, superior, and anterosuperior quadrants of the clock face, are distinguished as zones of considerable anatomic variability. It is this variability that leads to corresponding MR and MR arthrographic findings that are easily misinterpreted as evidence of labral pathology.
Biceps Tendon and the Biceps-Labral Complex
Four types of biceps tendon attachment to the superior portion of the labrum have been described. These types are distinguished by the proportion of biceps tendon fibers attaching to the posterosuperior versus the anterosuperior region of the labrum (Figure 9).14, 15 In type 1, the entire biceps tendon attaches to the posterosuperior labrum. In type 2, most of the biceps tendon fibers attach to the posterosuperior labrum with a small portion of fibers attaching to the anterosuperior labrum. In type 3, equal portions of the biceps tendon attach to the posterosuperior and anterosuperior regions of the labrum. In type 4, most of the biceps tendon fibers attach to the anterosuperior labrum with only a small portion of fibers attaching to the posterosuperior labrum.

9a
Figure 9:
Biceps-labral attachments. The 4 types of biceps tendon attachment to the superior portion of the labrum are depicted in this illustration: (1) posterosuperior labrum, (2) posterosuperior and a small portion of the anterosuperior labrum, (3) equal portions of the posterosuperior and anterosuperior labrum, and (4) anterosuperior and a small portion of the posterosuperior labrum.
Type 1 and type 2 attachments are most common, occurring in approximately 55% of persons while type 3 occurs in 37% and type 4 in 8%.14
Two major morphologic variations of the glenoid attachment of the biceps-labral complex have been emphasized (Figure 10). In the slab morphology, there is a relatively intimate attachment of the biceps-labral complex to the glenoid margin, with no space or only a small intervening space between these structures. In the meniscoid morphology, there is a larger space between the biceps-labral complex and the glenoid margin, permitting greater labral mobility compared to the mobility associated with the slab morphology. That prominent space is a normal variant that is designated a sublabral recess, or sulcus, and is discussed in detail later.

10a

10b

10c

10d
Figure 10:
Biceps-labral attachments. The 4 types of biceps tendon attachment to the superior portion of the labrum are depicted in this illustration: (1) posterosuperior labrum, (2) posterosuperior and a small portion of the anterosuperior labrum, (3) equal portions of the posterosuperior and anterosuperior labrum, and (4) anterosuperior and a small portion of the posterosuperior labrum.
Rotator Interval
An understanding of the anatomy of the rotator interval is also important in the complete assessment of the structures adjacent to a torn or detached superior labrum. The rotator interval is the triangular space in the anterosuperior aspect of the shoulder through which multiple capsuloligamentous and tendinous structures pass, contributing to normal biomechanical function about the shoulder.15 The superior boundary of the rotator interval is delineated by the anterior margin of the supraspinatus tendon, while the inferior boundary of the interval is marked by the superior margin of the subscapularis tendon, and the coracoid process forms the base of this interval( Figure 11).16 The apex of this interval is at the level of the intertubercular sulcus.17 The glenohumeral joint capsule, coracohumeral ligament, superior glenohumeral ligament, and biceps tendon traverse the rotator interval.16,17

11a
Figure 11:
Rotator interval. Illustration demonstrates the borders of the rotator interval. CAL: coracoacromial ligament, TRA: trapezoid ligament, CON: conoid ligament, RI: rotator interval, A/C: acromioclavicular joint, CP: coracoid process, LHBT: long head of biceps tendon, SGHL: superior glenohumeral ligament.
Glenohumeral Ligaments
The glenohumeral ligaments represent reinforcements of the joint capsule (Figure 12) and contribute to glenohumeral joint stability.18 These ligaments demonstrate variability in how often they are present and their specific course, and they may merge with adjacent structures, contributing to the complexity of the anatomy in this region.10 Indeed, some anatomists believe that these structures are not ligaments at all but, rather, they are capsular folds that become more evident in certain positions of the shoulder. With regard to their visibility on imaging studies, in an investigation of 108 MR arthrograms of the glenohumeral joint, Park and associates found the superior and inferior glenohumeral ligaments to be present in 99% of cases, while the middle glenohumeral ligament was present in only 79% of cases.13

12a

12b

12c

12d
Figure 12:
Glenohumeral ligaments. Sagittal illustration (12a), cadaveric section (12b), and corresponding sagittal T1 FS MRA image (12c) demonstrate the SGHL (arrows), MGHL (arrowheads), and anterior band of the IGHL (dashed arrows). The final illustration (12d) depicts these same glenohumeral ligaments, as well as the fasciculus obliquus (FO), or spiral glenohumeral ligament, which fuses laterally with the MGHL and subscapularis tendon (SSC).
- Superior Glenohumeral Ligament (SGHL)
The SGHL is recognized as a relatively constant anatomic structure in humans, present in 94% to 98% of specimens.19 The SGHL consists of direct and oblique fibers, courses from the glenoid labrum and/or the supraglenoid tubercle in a lateral direction, and attaches to the fovea capitis of the humeral head, which is a small depression of the humeral articular surface just above the lesser tuberosity.15 The SGHL also attaches to the bicipital groove, the upper part of the lesser tuberosity, and the subscapularis tendon, as well as the transverse humeral ligament, further contributing to the stability of the long head of the biceps tendon. There are many variations of the SGHL, however, with possible attachments to the biceps tendon itself or the anterior portion of the labrum, or the SGHL may arise in common with the middle glenohumeral ligament (Figure 13).
")
13a
")
13b

13c
Figure 13:
Variations in SGHL. Axial T1 FS MRA image (13a) demonstrates the SGHL (arrow) that in this patient arises from the long head of the biceps tendon (arrowhead). In an axial T1 FS MRA image from a second patient (13b), the SGHL (straight arrow) arises from the anterior labrum (curved arrow). Sagittal T1 FS MRA (13c) from a third patient demonstrates the SGHL (solid arrow) arising in common with the MGHL (dashed arrow). Figure 13a, 13b, 13c, reprinted from Internal Derangements of Joints; 2nd Edition. Resnick D., Kang H.S., Pretterklieber M.L. (2007) with permission from Elsevier.
- Middle Glenohumeral Ligament (MGHL)
The MGHL is the most variable of the glenohumeral ligaments in its size and position.19 This structure arises from the upper peripheral aspect of the glenoid cavity, intimate and possibly fusing with the coracohumeral ligament, coursing downward to attach onto the lesser tuberosity.15 The MGHL may attach directly to the anterior portion of the labrum or to the scapular neck, the latter pattern simulating a stripped joint capsule when studied with MR imaging or MR arthrography (Figure 14). Regarding its size, this too is variable, appearing thin and veil-like in some people and thick or even cord-like in others. Of all of the glenohumeral ligaments, the MGHL is the one most often absent.
")
14a
")
14b

14c

14d
Figure 14:
Variations in MGHL. Cadaveric axial sectional photograph (14a) and corresponding axial T1 FS MRA image (14b), show that the MGHL (arrows) arises from the base of the anterior labrum (arrowheads). This origin of the MGHL is far more common than the pattern shown in 14c and 14d. In a second cadaver, an axial sectional photograph (14c) and corresponding axial T1 FS MRA image (14d) demonstrate the MGHL (arrows) arising from the anterior scapular periosteum (S), simulating the appearance of periosteal stripping. Figure 14b, reprinted from Internal Derangements of Joints; 2nd Edition. Resnick D., Kang H.S., Pretterklieber M.L. (2007) with permission from Elsevier.
- Inferior Glenohumeral Ligament (IGHL)
The IGHL is likened to a hammock, connecting the inferior glenoid and labrum to the humeral neck. This structure consists of two focal thickenings, termed its anterior and posterior bands, and an intervening axillary pouch.15 While the anterior band typically attaches to the 2 to 4 o’clock position on the glenoid rim and the posterior band attaches between the 7 to 9 o’clock position, there are many variations in these points of attachment. In some cases, for example, the anterior band attaches very high on the glenoid rim, in the region of the SGHL and MGHL, creating diagnostic difficulty in interpreting the MR imaging study. In other cases, the posterior band is entirely absent. The axillary pouch is formed by the fasciculus obliquus medially and by the junction of the anterior and posterior bands laterally (Figure 15).

15a

15b

15c

15d

15e

15f

15g
Figure 15:
IGHL. Sequential coronal cadaveric sections (15a-c) and corresponding coronal T1 FS MRA images (15d-f) from anterior (15a, d) to posterior (15c, f) demonstrate the anterior (arrows) and posterior (dashed arrows) bands of the IGHL, separated by the intervening axillary pouch (curved arrows), and the relationship of the anterior band of the IGHL with the fasciculus obliquus (arrowheads). Note that both bands and the axillary pouch have glenoid and humeral attachments. Note, also, in Figure 15g, the crossing of the anterior bundle (AB) of the IGHL with the fasciculus obliquus (FO), or spiral glenohumeral ligament, simulating the crossing bands of a baby bundler.
- Fasciculus Obliquus (FO)
The FO is also referred to as the spiral glenohumeral ligament and attaches to the glenoid from about the 5 o’clock to the 7 o’clock position.15 This ligament attaches to the infraglenoid tubercle and the long head of the triceps tendon and courses obliquely upwards, ultimately merging with the MGHL and the IGHL (see Figure 15a and 15d).15 At its most superior aspect, the FO fuses with the subscapularis tendon on the lesser tubercle of the humerus.15, 19, 20,21 The significance of the FO is related to its impact on glenohumeral joint stability given its influence on the positioning of the MGHL with shoulder motion.21 Indeed, the FO has been termed the holy grail of the glenohumeral joint, with its critical role in providing joint stability likened to the function of a baby bundler (see Figure 15g).
Normal Variants
Most “normal” variants of the glenohumeral joint involve the glenoid labrum, glenohumeral ligaments, or glenoid rim, or combinations of these, and in general, these variations predominate in the posterosuperior, superior, and anterosuperior quadrants, from the 10 to 3 o’clock position. Many of these variations are intimate with the biceps-labral complex. In the following discussion, only some of the more frequently described variants are considered.
Glenoid Notch
The glenoid notch is a normal variant characterized by an indentation of the anterior glenoid cavity and rim in the region of the anterior fusion site of the superior and inferior ossification centers (Figure 16). It has previously been suggested to have an association with a sublabral foramen in as many as 69% of cases, although the significance of this glenoid contour alteration is debated.

16a

16b
Figure 16:
Glenoid notch. Sagittal T2 weighted fat-suppressed (T2 FS) MR image (16a) demonstrates an indentation at the anterior glenoid cavity in the region of the fusion site of the superior and inferior ossification centers of the glenoid (arrow). This indentation can be of variable depth, as outlined in the illustration in 16b. A: Acromion, C: Coracoid process, G: Glenoid.
Sublabral Recess
The most common labral variant is the sublabral recess, or sublabral sulcus, which is described as a normal space between the biceps-labral complex and the superior glenoid cartilage, a space that is more prominent with a meniscoid type attachment of the biceps-labral complex (Figure 17). This variant has a reported incidence of up to 73%. The defining features of a sublabral recess include a narrow gap (< 2 mm) that is uniform in width with smooth margins on axial sequences and medial extension between the superior labrum and glenoid, paralleling the glenoid articular cartilage, on coronal oblique sequences. Furthermore, in general but not invariably, there is minimal to no extension of the sublabral recess posterior to the biceps tendon attachment to the superior labrum.

17a

17b

17c

17d

17e
Figure 17:
Sublabral recess. Coronal T1 FS MRA images (17a and 17b), with 17a anterior to 17b, show a sublabral recess (arrows), separating the biceps-labral complex from the articular cartilage of the glenoid. It is smooth, relatively narrow, and points in a medial direction, toward the patient’s head. In transverse cadaveric sections (17c and 17d), with 17c slightly superior to 17d, and an axial T1 MRA image (17e), the sublabral recess (arrows) is well shown. Note its relationship to the attachment (arrowheads) of the biceps tendon. The recess does not extend posterior to this attachment, and it is uniformly narrow and smooth.
Sublabral Foramen
The sublabral foramen, or sublabral hole, is another anatomic variant similar to the sublabral recess but with a lower incidence (3%-17%) and different location on the glenoid clock face. Whereas the sublabral recess is generally (but not invariably) described as a space located superiorly between the biceps-labral complex and glenoid cartilage, the sublabral foramen is located anterosuperiorly, generally between the 1 to 3 o’clock position (Figure 18). Its pathogenesis is not clear, although it may relate to an embryologic variation (see later discussion) characterized by the development of the labrum at a distance from the glenoid margin. Of diagnostic importance, the anomalous anterosuperior labrum located away from the glenoid margin rejoins the normally positioned labrum along the anterior glenoid rim, usually by the 3 o’clock position, via a labral slip extending between the inferior border of the recess and the glenoid margin. This slip is not apparent in a Buford complex (see following discussion). The sublabral foramen generally is seen in continuity with a sublabral recess, although it may also be seen as an independent finding.

18a

18b

18c

18d

18e

18f
Figure 18:
Sublabral foramen. Illustration (18a) demonstrates a sublabral foramen, a gap between the anterosuperior labrum and the glenoid margin between the 12 o’clock and 3 o’clock position (asterisk). The lower aspect of the foramen reconnects with the glenoid margin via a labral slip (arrow). Sequential cadaveric axial sections from superior to inferior (18b, 18c, and 18d) and corresponding axial proton density fat-suppressed MR images (18e and 18f) demonstrate the sublabral foramen as a smooth space (solid arrows in 18c,18e, and 18f) between the glenoid rim and labrum (arrowheads). MGHL is also displayed in the images (dashed arrows).
Buford Complex
The Buford complex is a less frequently seen anatomic variant characterized by two findings: the absence of the anterosuperior portion of the labrum; and the presence of a cord-like MGHL (Figure 19).3, 4, 13,14 The developmentally thick MGHL attaches superiorly to the glenoid margin and then extends obliquely downward; there is no labral slip passing posteriorly to rejoin the glenoid margin. Rather, the labrum starts anew anteroinferiorly. Some references indicate that in 80% of cases of the Buford complex, there is an associated pathologic lesion of the labrum, especially posterosuperiorly.

19a

19b

19c

19d

19e

19f

19g
Figure 19:
Buford complex. Illustration (19a), sequential cadaveric axial sections from superior to inferior (19b, 19c, and 19d), with axial (19e), sagittal (19f), and coronal (19g) T1 FS MRA images demonstrate the characteristic findings of a Buford complex. Note the absence of the anterosuperior glenoid labrum (dashed arrows) and the presence of a cord-like MGHL (arrowheads). There is no labral slip. The anteroinferior labrum is normal (solid arrow).
Sublabral Foramen with a Cord-Like MGHL
In some reports, a sublabral recess with a cord-like MGHL has been identified as a more frequent anomaly than a Buford complex, a variant whose features include a cord-like MGHL (as seen in a Buford complex) with a labral slip that is typical of a sublabral foramen (Figure 20).22

20a

20b

20c

20d

20e
Figure 20:
Sublabral foramen with a cord-like MGHL. Illustration (20a), sequential axial T1 FS MRA images from superior to inferior (20b and 20c), and sequential sagittal T1 FS MRA images from lateral to medial (20d and 20e) demonstrate a sublabral foramen with a cord-like MGHL, which is differentiated from the Buford complex by the presence of a labral slip (arrows) extending between the thick MGHL (arrowheads) and glenoid margin. As with a Buford complex, the anterosuperior labrum is absent (dashed arrows).
Normal Variants or Prior Pediatric Injury?
Undermining this entire discussion of labral variants is the issue as to whether these variants can even be considered “normal”. Embryologic studies have suggested that the glenoid labrum develops in conjunction with the glenoid rim and, along with the capsule, precedes the development of the glenohumeral joint cavity and its recesses.23 This would subsequently call into question the notion that these labral variants are a result of an arrest in this normal pattern of embryologic development of the labrum and lend credence to the idea that they are sequelae of childhood labral injuries. In this regard, Chauvin and coworkers retrospectively reviewed MR arthrograms in 66 children (mean age 15 years old) and reported two cases of a labral variant (one sublabral recess, one Buford complex), both of which were deemed SLAP lesions at the time of arthroscopy.24 This result would favor the notion that these so-called anatomic variations are, in reality, related to prior labral pathology. Figure 21 highlights this concept, in which a Buford complex was diagnosed in an adolescent patient both with MR arthrography and during arthroscopy; however, closer review of the MR images suggests that a torn labrum intimate with the MGHL may be responsible for this appearance. Alternatively, Fealy et al. and Arregui et al. evaluated cadaveric fetuses (57 total) and discovered “detachment” of the anterosuperior labrum in a small minority of cases.25 The finding of an anomalous “detachment” in a fetus that has yet to experience any external stresses would argue more for the developmental arrest theory. A possible hybrid theory is that these detachments are indeed developmental variants that lead to labral hypermobility that itself predisposes persons to the subsequent development of a pathologic labral lesion.

21a

21b

21c
Figure 21:
Buford complex or pediatric labral tear? This adolescent patient was noted by the surgeon on arthroscopy to have findings consistent with a Buford complex. Axial T1 FS MRA image (21a) demonstrates what appears to be a developmentally thick MGHL (curved arrow) with an absent anterosuperior labrum. On a more inferior axial T1 FS MRA image (21b) with a magnified view (21c), the “thick MGHL” appears to consist of a detached labrum (arrows) and MGHL (arrowheads), separated by a thin cleft (dashed arrow). (Courtesy of Jerry Dwek, M.D.)
SLAP Lesions
The term SLAP lesion is an abbreviation for superior labrum, anterior and posterior lesion; the term was introduced by Snyder and his associates based on observations during arthroscopic examinations.26 It refers to a detachment or tear of the superior portion of the labrum. This lesion can occur owing to a single traumatic event, repetitive stress, or labral degeneration. In Snyder’s study, the most common traumatic mechanism was a compression force applied to the shoulder during a fall onto the arm with the shoulder abducted in slight forward flexion.26 Abrupt traction applied to the arm from a pulling force or related to repetitive overhead throwing motion represents another potential mechanism.26, 27
Clinical manifestations of SLAP lesions include shoulder pain exacerbated with overhead activities and a “catching” or “popping” sensation with overhead motion. As SLAP lesions often co-exist with other pathologic abnormalities of the shoulder, findings discovered at the time of physical examination can be nonspecific and challenging to interpret. A combination of at least three positive clinical tests has been found to be more sensitive than a single positive physical maneuver for the diagnosis of SLAP lesions.28 Key clinical tests include the O’Brien active compression test and the Speed and Yergason tests, each reported with varying sensitivity and specificity for the diagnosis of SLAP lesions.
Key Clinical Tests
- O’Brien Active Compression Test
A positive O’Brien active compression test is commonly associated with SLAP lesions, with up to 67% sensitivity but only approximately 37% specificity.29 In the O’Brien test, the patient attempts to resist the examiner’s downward force when the shoulder is in 90 degrees of flexion with the arm adducted approximately 15 degrees and with the elbow in extension and the forearm in internal rotation and pronation.29 A positive result is defined as the sensation of deep or anterior shoulder pain during this maneuver.
- Speed Test
Regarding the Speed test, the patient attempts to elevate the arm against the examiner’s force when the elbow is extended with the forearm in full supination and the shoulder slightly flexed. A positive result is defined as eliciting anterior shoulder pain. There is a reported sensitivity for the Speed test of 48% and specificity of approximately 67%.29
- Yergason Test
In the Yergason test, the patient attempts to supinate the arm against the examiner’s resistance when the forearm is pronated and the elbow is flexed to ninety degrees. A positive result is defined as pain localized to the long head of the biceps tendon. For this test, there is a reported sensitivity of 13% and specificity of 93%.29
SLAP Lesion Classification System and Prevalence
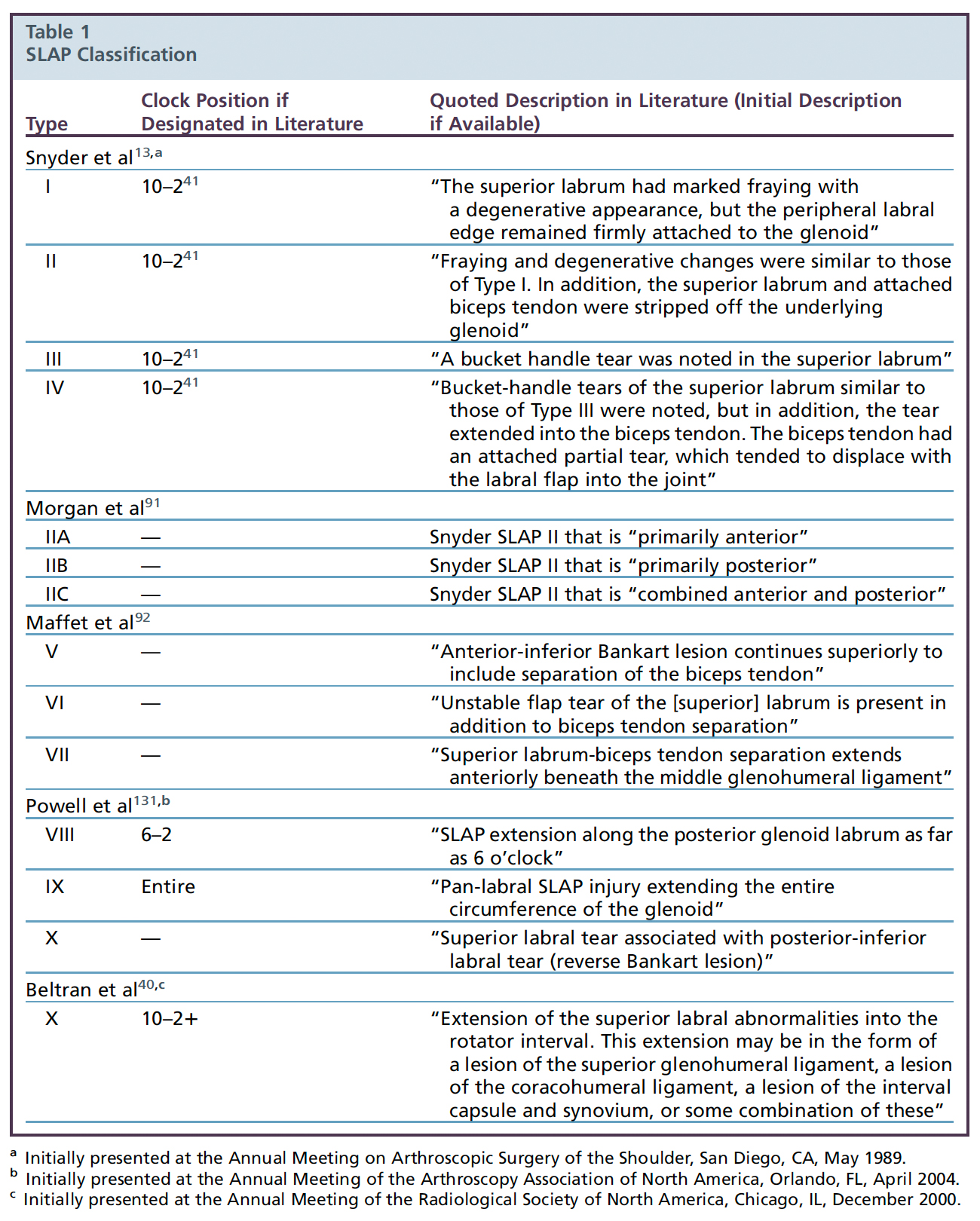
While Snyder and collaborators originally proposed four types of SLAP lesions, their classification system has subsequently been expanded and revised on multiple occasions. Currently, ten types of SLAP lesion have been recognized, although the inclusion of types VIII and IX remains controversial.30 The SLAP lesions are distinguished by three factors: 1) the morphology, or pattern, of labral abnormalities; 2) the location, or extent, of labral abnormalities; and 3) the presence or absence of involvement of adjacent structures including the biceps tendon, glenohumeral ligaments, and rotator interval (Table 1). Although there is variability in the prevalence of the various types of SLAP lesion, type II SLAP lesions are recognized as the most common form, not considering degenerative SLAP I lesions.
- Morphology of the Labral Lesion
The morphology of labral failure that can be found with SLAP lesions is highly variable. As described by Snyder and his coworkers, one such pattern is simply labral fraying.26 In some ways, the inclusion of this pattern created diagnostic problems, as well as the probable overuse of the term SLAP lesion. Labral fraying is generally degenerative in nature and, further, it is almost universally present in middle-aged and elderly persons, dominating in the posterosuperior, superior and anterosuperior portions of the labrum.
Additional morphologic variations relate to the pattern of labral detachment or labral tearing, although both detachment and tearing may occur together. Labral detachments may be partial or complete, and labral tears can be described as longitudinal vertical, horizontal, radial, flap-type, or bucket-handle (Figure 22).

22a
Figure 22:
Patterns of labral failure. Illustrations demonstrate the morphology of a number of patterns of labral failure, including labral detachment (22A) and labral tears (22B, 22C, 22D, 22E, and 22F).
- Lesion Location and Involvement of Adjacent Structures
Additionally, characterization of SLAP lesions includes localization of the labral tear or detachment, which can refer to the involved quadrant or quadrants or, alternatively, the position or “hours” on the glenoid clock face that are affected. Although the typical and most frequently reported location of the SLAP lesion is the 11 o’clock to the 1 o’clock position, involvement of the labrum elsewhere on the glenoid face in combination with superior labral involvement is well recognized. Although the term “extension” is often used to describe the propagation of superior quadrant labral lesions to other quadrants, there are little reported data that confirm how multiquadrant lesions develop (see later discussion).
With regard to involvement of adjacent structures in cases of SLAP lesions, this too is well documented. As noted previously, one or more of the following structures may be involved in combination with labral abnormalities: long head of the biceps tendon, SGHL, MGHL, IGHL, and rotator interval. In the complete description of a SLAP lesion, any evidence of involvement of adjacent structures, as well as the morphology and location of the glenoid labral abnormalities, should be included, as each of these features impacts the way SLAP lesions are managed.30
Definitions of SLAP Lesions
- Type I Lesion
A type I SLAP lesion refers to fraying without detachment of the labrum, involving the 11 o’clock to the 1 o’clock position (Figure 23). As noted previously, this is a degenerative lesion that is almost universal in middle-aged and elderly persons and, in the opinion of the authors of this clinic, its inclusion as a SLAP lesion accounts, in part, for the overutilization of this term in clinical practice.

23a

23b

23c
Figure 23:
Type 1 SLAP lesion. Illustration (23a) and coronal fat-suppressed T2-weighted MR images from two different patients (23b and 23c) demonstrate fraying of the superior labrum (red arrows), likely degenerative. In 23b, note the accompanying glenohumeral osteoarthrosis characterized by subchondral cysts in the glenoid with cartilage loss. Mild supraspinatus tendinosis is also shown (yellow arrow). In 23c, there is a lesser degree of cartilage loss in the glenohumeral joint. Also note the articular-sided fraying of the supraspinatus tendon (white arrow).
- Type II Lesion
Snyder and his colleagues originally described the second type of SLAP lesion as a detachment of the superior labrum from the peripheral aspect of the glenoid in addition to labral fraying.26 This original defining feature of detachment in this subcategory raises the recurrent question, should a tear, in addition to detachment, of the superior labrum be designated a SLAP II lesion? In the current definition, the type II lesion indicates a detachment (or tear) involving the biceps-labral complex and is subcategorized into three patterns. In type IIa lesions, the tear is localized anterosuperiorly and involves the 12 o’clock to 3 o’clock position, while type IIb lesions are localized posterosuperiorly involving the 9 o’clock to 12 o’clock position. Type IIc lesions exhibit anterosuperior, superior, and posterosuperior labral involvement, affecting the 9 o’clock to 3 o’clock position (Figure 24).

24a

24b

24c
Figure 24:
Type IIc SLAP lesion. Illustration (24a) demonstrates detachment of the labrum from the 11 o’clock to 1 o’clock position. Coronal (24b) and sagittal (24c) T1 FS MRA images confirm detachment of the labrum from the 9 o’clock to 3 o’clock position (arrows).
- Types III and IV Lesions
The type III and IV SLAP lesions involve the 11 o’clock to the 1 o’clock position and are defined as bucket-handle tears of the superior labrum. These two lesions are distinguished by the presence or absence of involvement of the biceps tendon. In type III lesions, the biceps tendon is intact and uninvolved (Figure 25), while in type IV lesions, the bucket-handle tear also involves the biceps tendon.
The “double oreo” sign on MR arthrography and the “cheerio” sign on CT arthrography and MR arthrography, have been described in SLAP III lesions.31,32 In the oreo cookie analogy, the white center represents fluid (intra-articular contrast agent during MR arthrography) and the two black layers correspond to the fibrocartilaginous labrum and the glenoid cortex. Note that when the “single oreo” sign is present adjacent to the biceps tendon, this is consistent with a sublabral recess, as the fluid or contrast agent is located between the labrum and the glenoid.31 In contrast, with the “double oreo” sign (Figure 26), there is a configuration of two oreo cookies next to each other, and the two white columns indicate two different fluid collections; in this context, the more medial fluid collection is between the labrum and the glenoid representing a sublabral recess, and the more lateral fluid collection is within the substance of the superior labrum, indicative of a superior labral bucket-handle tear (SLAP III lesion). The “cheerio” sign visible during MR arthrography refers to a peripheral rim of contrast agent outlining a central core of soft tissue adjacent to the labrum. The central core usually has a lower attenuation, which results from the folded edge of the labrum of the bucket-handle tear, as well as some trapped air.32 Rarely, type III and IV SLAP lesions may be degenerative in pathogenesis (Figure 27).

25a

25b

25c

25d

25e
Figure 25:
Type III SLAP lesion. Illustration (25a) demonstrates a bucket-handle tear of the superior labrum involving the 11 o’clock to the 1 o’clock position (arrow). Coronal cadaveric section (25b) and corresponding coronal T1 FS MRA image (25c) show the bucket-handle tear (red arrows) of the superior labrum. Coronal T1 FS MRA images (25d and25e) in a patient with a similar SLAP lesion (arrows) are also shown to compare the appearance of the labrum with the arm first in traction (25d) and then without traction (25e). Note that the bucket-handle tear is accentuated when traction is applied to the arm, as in 25d. The same labral abnormality is visible only as altered signal (arrow) and altered morphology inferiorly when the arm is not under traction (25e). Figure 25b, 25c, 25d, 25e, reprinted from Internal Derangements of Joints; 2nd Edition. Resnick D., Kang H.S., Pretterklieber M.L. (2007), with permission from Elsevier.

26a

26b

26c

26d
Figure 26:
Type III SLAP lesion. Coronal (26a) and axial (26b) T1 FS MRA images demonstrate the “double oreo” sign, with the more medial white column representing a sublabral recess (dashed arrows), and the more lateral white column representing a tear within the substance of the superior labrum (arrows). Axial (26c) and coronal (26d) fat-suppressed T2-weighted MR images in a different patient demonstrate the “cheerio” sign, with fluid in the center of the labrum corresponding to the labral tear (arrows).

27a

27b

27c

27d

27e

27f

27g
Figure 27:
Type IV SLAP lesion. Illustration (27a) demonstrates a bucket-handle tear of the superior labrum from the 11 o’clock to 1 o’clock position with involvement of the biceps tendon. Cadaveric axial sections (27b and 27c) and corresponding axial T1 MRA (27d and 27e) and coronal T1 FS MRA (27f and 27g) images demonstrate a bucket-handle tear of the superior labrum (arrows) with additional involvement of the biceps tendon (arrowheads). As these abnormalities are observed in a cadaver derived from an elderly person at the time of death, they may be degenerative in pathogenesis.
- Type V Lesion
A type V SLAP lesion is associated with involvement of both the superior and the anterior portions of the labrum, typically between the 11 o’clock and 5 o’clock position, and this lesion may be accompanied by anterior or anteroinferior dislocation of the humeral head relative to the glenoid (Figure 28). In this type of lesion, an injury to the anteroinferior labrum, the so-called Bankart lesion, coexists with a superior labral tear or detachment. Most descriptions of this lesion show continuous labral abnormalities involving the superior, anterosuperior, anterior, and anteroinferior portions of the glenoid labrum, although it is probable that the labral involvement may be discontinuous, with intervening regions of normal appearing labrum.4, 27 Also, in contrast to those SLAP lesions that are confined to the superior portion of the labrum, in which macro-instability of the glenohumeral joint is generally not encountered, those SLAP lesions that also affect other quadrants of the glenoid labrum can clearly be associated with such macro-instability.

28a

28b

28c

28d

28e

28f

28g

28h
Figure 28:
Type V SLAP lesion. Illustration (28a) demonstrates detachment / tearing of the superior and anterior labrum involving the 11:30 to 6 o’clock position. Sequential cadaveric axial sections at the 12 o’clock (28b), 1 o’clock (28c), and 3 o’clock (28d) positions demonstrate superior labral detachment (arrow, 28b) with tearing at the base of the labrum anterosuperiorly (arrow, 28c) and anteriorly (arrow, 28d). Sequential axial T1 FS MRA images from a patient show similar detachment / tearing of the labrum superiorly (arrow, 28e), anterosuperiorly (arrow, 28f), and anteriorly (arrow, 28g). The same labral abnormalities (arrows) are displayed on the accompanying sagittal T1 FS MRA image (28h).
- Type VI Lesion
The type VI SLAP lesion is defined as an unstable labral flap tear, occurring in the 11 o’clock to 1 o’clock position (Figure 29). Given its proximity to the biceps tendon, this type of SLAP lesion can be associated with stripping of the biceps tendon. The type VI SLAP lesion can be conceptualized as a type II SLAP lesion combined with a component of instability clinically owing to the separation of the biceps tendon superiorly.

29a

29b

29c
Figure 29:
Type VI SLAP lesion. Illustration (29a) demonstrates a displaced flap tear of the superior labrum (arrow). Axial (29b) and coronal (29c) T1 FS MRA images show a labral flap tear (arrows) with a large transverse dimension.
- Types VII-X Lesions
SLAP types VII, VIII, IX and X lesions are defined by the association of the torn or detached superior labrum with additional lesions of key adjacent structures. Type VII lesions also involve the MGHL with the labral abnormalities most commonly located in the 11 o’clock to 3 o’clock position (Figure 30). Type VIII lesions involve both the superior and posterior portions of the labrum (from the 7 o’ clock to the 1 o’clock position), and these lesions can be conceptualized as particularly extensive type IIb lesions (Figure 31 and Figure 32). Type IX lesions involve almost the entire labrum, typically from the 7 o’clock to the 5 o’clock position (Figure 33). Most reported descriptions of these patterns of labral involvement show labral lesions that are continuous, not separated by areas in which the labrum appears normal, but it is highly likely that discontinuous forms of these types of SLAP lesion exist. Finally, the type X SLAP lesion refers to labral involvement combined with involvement of the rotator interval, the labral abnormalities affecting typically the 11 o’clock to (at least) the 1 o’clock position (Figure 34).

30a

30b

30c
Figure 30:
Type VII SLAP lesion. Illustration (30a) demonstrates detachment / tearing of the superior and anterosuperior labrum involving the 12 o’clock to 2 o’clock position, combined with a tear of the MGHL. Axial (30b) and sagittal (30c) T1 FS MRA images show a tear of the anterosuperior labrum (arrow) with involvement of the MGHL (arrowheads).

31a

31b

31c
Figure 31:
Type VIII SLAP lesion. Illustration (31a) demonstrates detachment of the superior and posterior labrum involving the 7 o’clock to 1 o’clock position. Coronal (31b) and axial (31c) T1 FS MRA images show a tear of the superior (arrow, 31b), and posterior (arrow, 31c) labrum.

32a

32b
Figure 32:
Type VIII SLAP lesion. Coronal (32a) and axial (32b) T1 FS MRA images demonstrate detachment of the superior labrum (blue arrow in 32a) with additional tearing / detachment of the posteroinferior and posterior labrum (red arrows in 32a and 32b). Note that this is a multiquadrant lesion in continuity as there is no normal intervening labrum between the lesions. (Courtesy of Karen C. Chen, M.D.)

33a

33b

33c

33d
Figure 33:
Type IX SLAP lesion. Illustration (33a) demonstrates near global detachment of the labrum. Axial (33b), and two sagittal (33c and 33d) T1 FS MRA images, c medial to d, demonstrate detachment of the labrum superiorly, anteriorly, and posteriorly (arrows). The extent of the anterior and posterior labral abnormalities is especially well shown in the sagittal images (33c and 33d, arrows).

34a

34b

34c
Figure 34:
Type X SLAP lesion. Illustration (34a) demonstrates detachment of the superior labrum with associated tearing of the SGHL. Axial (34b) and coronal (34c) T1 FS MRA images demonstrate the superior labral detachment (arrowhead) and tearing of the SGHL (arrows). Note the target appearance in the coronal plane.
- Other Types of SLAP Lesion
It is not surprising or unexpected that some SLAP lesions simply do not conform to any of these previously reported patterns. Their features may not match those described in the literature (e.g., the presence of a labral tear rather than labral detachment or of discontinuous rather than continuous labral abnormalities). Further, the pattern of involvement of adjacent structures may not match any that has previously been described (Figure 35). Rather than report further types of SLAP lesion to the ever-growing list of such lesions that already exists in the literature (each with its own Roman numeral and many of which, are not known by orthopaedic surgeons, even shoulder surgeons), a complete report containing the location and morphology of the labral abnormalities and the pattern of involvement of additional structures should suffice.

35a

35b

35c

35d
Figure 35:
Combined Type VII and Type X SLAP lesions. Illustration (35a) demonstrates detachment / tearing of the superior labrum with involvement of the SGHL and MGHL. Axial (35b and 35c) and sagittal (35d) T1 FS MRA images demonstrate the labral tears (arrowheads) and involvement of the SGHL (solid arrow) and MGHL (dashed arrows).
Multiquadrant Labral Abnormalities
The current classification system for SLAP lesions includes those labral abnormalities that are isolated to the superior quadrant and those that involve more than one labral quadrant (i.e., multiquadrant labral abnormalities). Although the terms anterior extension and posterior extension of the superior labral abnormalities are often applied to these multiquadrant lesions, there are few or any comprehensive investigations that have long periods of observation in cases of SLAP lesion such that the identification of the initial site of involvement and subsequent sites of involvement, that is the precise progression of the process, is not clear. Do these multiquadrant instances indicate a process that starts in one place and then extends into another as a continuous region of labral abnormality, or do they commence in multiple quadrants and then remain discontinuous or even collide over time? The answer to this question remains elusive.
What seems to be clear is that when labral abnormalities involve multiple quadrants, the sites of pathology may be in continuity or there may be an intervening region between sites of abnormal labrum in which the labrum is normal (Figure 36). In these multiple quadrant scenarios, we recommend describing the sites and features of the abnormalities without necessarily invoking whether one of these abnormalities “extends” to another site unless sequential imaging over a prolonged period of time documents the course of the labral alterations. Further, clinical findings in cases of multiquadrant involvement may differ from those associated with superior quadrant involvement alone. Glenohumeral joint macro-instability is not a characteristic finding in cases of superior quadrant involvement alone, but with multiple quadrant abnormalities, such instability may exist. Therefore, in describing the labral abnormalities in cases of SLAP lesion, the quadrants of involvement, their continuity or discontinuity, the pattern of labral abnormality (e.g., tear versus detachment, nondisplaced versus bucket-handle or flap tear), and the involvement of other structures (e.g., biceps tendon, rotator interval, SGHL, MGHL, and/or IGHL) should be included.

36a

36b
Figure 36:
Multiquadrant lesions. Illustration of multiquadrant labral lesions in discontinuity (36a) on the glenoid clock face. Note the region of normal labrum (in red, from approximately 1 o’clock to approximately 3 o’clock) located between two regions of labral abnormality (in blue, depicted from approximately 11 o’clock to 1 o’clock and from approximately 3 o’clock to 5 o’clock). Thus, these two labral lesions are discontinuous. Alternatively, multiquadrant labral lesions can occur in continuity (36b). Observe the multiquadrant abnormality involving the labrum in continuity from approximately 11 o’clock to 5 o’clock (in blue). ANT: Anterior, POST: Posterior.
Distinguishing Normal Variants of SLAP Lesions
Although MR arthrography appears to be the best imaging technique to investigate the glenoid labrum and adjacent structures, the differentiation of anatomic variants from SLAP lesions remains difficult in many cases. Careful analysis of the location, morphology, and signal intensity of the labrum, combined with additional analysis of the glenohumeral ligaments, tendon of the long head of the biceps brachii muscle, and rotator interval, is required for accurate diagnosis. Specific diagnostic dilemmas include the following:
Sublabral Recess Versus SLAP II Lesion
The sublabral recess is a smooth space located superiorly between the biceps-labral complex and the glenoid articular cartilage, no more than 1-2 mm in width, of equal width anterosuperiorly and posterosuperiorly, and rarely involving that portion of the superior labrum that is located posterior to the biceps tendon anchor. A SLAP II lesion is often associated with a wider space between the superior labrum and glenoid margin, frequently with an unequal width anterosuperiorly and posterosuperiorly, best displayed in the axial plane. In the coronal plane, a sublabral recess often extends superomedially, paralleling the glenoid articular cartilage, whereas a SLAP II lesion may extend superolaterally (Figure 37).

37a

37b

37c

37d
Figure 37:
Distinguishing a sublabral recess from a Type II SLAP lesion. Upper Illustration of the biceps-labral complex in the coronal plane (37a) and a coronal T1 FS MRA image (37b) demonstrate a sublabral recess. Note that in the coronal plane, a sublabral recess is a smooth and thin space that is located between the biceps-labral complex and the glenoid articular cartilage (arrow in 37b). It is obliquely oriented, paralleling the surface of the articular cartilage and pointing toward the patient’s head (arrow in 37a). Lower illustration (37c), again in the coronal plane, and coronal T1 FS MRA image (37d) demonstrate a Type II SLAP lesion, which has irregular margins and is oriented laterally in the coronal plane (dashed arrow in 37d), pointing toward the humeral head (solid arrow in 37c).
Occasionally, one encounters a very prominent sublabral recess whose imaging characteristics are almost identical to a SLAP II lesion. In these cases, does it really matter if one accurately distinguishes between the two? A prominent sublabral recess may be indicative of a hypermobile superior labrum that, theoretically, could lead to clinical manifestations identical to those of a SLAP lesion. This idea may be akin to the hypermobile lateral meniscus described in the knee, in which abnormal translation, specifically of the posterior horn, has been responsible for symptoms of pain and/or intermittent locking with no meniscal tear identified on either pre-operative MR images or during arthroscopy.33
Sublabral Foramen Versus SLAP V Lesion
The sublabral foramen can be differentiated from a SLAP V lesion by identifying the location of the “reconnection” of the labrum to the glenoid rim. With a sublabral foramen, there generally is a reconnection of the “malpositioned” anterosuperior labrum with the glenoid margin that occurs no more inferiorly than the 3 o’clock position whereas the SLAP V lesion is often characterized by a detached anterosuperior labrum that remains separated from the anterior margin of the glenoid more anteroinferiorly, often rejoining the normal labrum at about the 4 or 5 o’clock position (Figure 38).

38a

38b
Figure 38:
Distinguishing a sublabral foramen from a Type V SLAP lesion. Sagittal T1 FS MRA image (38a) demonstrates a sublabral foramen with a “reconnection” of the “malpositioned” anterosuperior labrum with the glenoid margin by the 3 o’clock position (arrows). Sagittal T1 FS MRA image in a different patient (38b) demonstrates a SLAP V lesion with detachment of the anterosuperior labrum continuing more anteroinferiorly and rejoining the normal labrum at the 4 o’clock position (dashed arrows).
Sublabral Foramen, Buford Complex, and Sublabral Foramen with a Cord-Like MGHL
The sublabral foramen, Buford complex, and sublabral foramen with a cord-like MGHL are all characterized by absence of the anterosuperior portion of the labrum. Unlike the Buford complex, the sublabral foramen demonstrates a labral slip that extends from the malpositioned labrum and the anterior glenoid rim, usually by the 3 o’clock position. The sublabral foramen with a cord-like MGHL is a hybrid variation with features of both a sublabral foramen and Buford complex (Figure 39), in which the MGHL is developmentally thick (as in a Buford complex) and a labral slip is present (as in a sublabral foramen).

39a

39b

39c

39d
Figure 39:
Distinguishing a sublabral foramen with a cord-like MGHL from a Buford complex. Initial illustration (39a) and sagittal T1 FS MRA image (39b) demonstrate a sublabral foramen (between arrowheads), with a labral slip (solid red arrow) extending from the “malpositioned” anterosuperior labrum to the anterior glenoid rim. The MGHL is prominent and cord-like (dashed red arrow). These findings indicate a sublabral foramen with a cord-like MGHL. Next illustration (39c) and sagittal T1 MRA image (39d) demonstrate a Buford complex, with an absent anterosuperior labrum (between arrowheads) and a cord-like MGHL (dashed arrow). No labral slip is present in a Buford complex.
Developmentally Duplicated MGHL Versus SLAP VII Lesion
There have been reported cases in which the MGHL has a duplicated appearance, presumably on a developmental basis, with two parallel lines on oblique sagittal MR images and a U-shape on axial MR images.34 This appearance overlaps with that of a SLAP VII lesion, in which the labral abnormality is combined with an abnormal MGHL, often characterized by a longitudinal “split” tear. Methods allowing differentiation between these two entities have not been well described, with some investigators even suggesting that what is described as a developmental duplication of the MGHL simply reflects a remote partially healed SLAP VII lesion.
Coexistence of Normal Variants and SLAP Lesions
Differentiation of many of the so-called normal variants from SLAP lesions at the time of MR imaging or even during arthroscopy is made even more difficult owing to the presence of many reports that have confirmed the association of such variants with a variety of pathologic labroligamentous abnormalities. One example of this relates to the Buford complex. Some reports indicate that labral pathology, especially posterosuperiorly, occurs in 80% of cases of the Buford complex.
Additional Abnormalities Associated with SLAP Lesions
Paralabral Ganglion Cyst
Paralabral ganglion cysts have been found to be highly associated (59%-88%) with an underlying labral tear or detachment, often a SLAP lesion. Such cysts may be single or multiple, may contain gas, and are of variable size and, when large, may erode the adjacent bone, especially the scapula (Figure 40). In certain locations, paralabral ganglion cysts may lead to an entrapment neuropathy, particularly of the suprascapular nerve, with denervation changes in the supraspinatus or infraspinatus muscle, or both muscles (Figure 41). Using MR imaging or MR arthrography, ganglion cysts are often seen as uniloculated or multiloculated cystic lesions in close proximity to the glenoid margin. They represent strong, although not certain, evidence of an adjacent glenoid labral abnormality.35

40a

40b

40c

40d
Figure 40:
Paralabral ganglion cyst with scapular erosion. AP radiograph (40a), axial CT (40b), and coronal (40c) and sagittal fat-suppressed T2-weighted (40d) MR images demonstrate a paralabral ganglion cyst (arrows in 40c and 40d) that has eroded the posterior surface of the adjacent scapula, with deepening of the spinoglenoid notch (arrows in 40a and 40b). (Courtesy of Mini N. Pathria, M.D.)

41a

41b

41c
Figure 41:
Paralabral ganglion cyst with denervation muscle edema. Coronal (41a), sagittal (41b), and more posterior coronal fat-suppressed T2-weighted (41c) MR images demonstrate a paralabral ganglion cyst (arrows) intimate with a superior labral tear (not shown), extending into the spinoglenoid notch, with resultant denervation edema of the infraspinatus muscle (asterisks).
Paralabral ganglion cysts often do not communicate with the joint lumen even when accompanied by an extensive labral tear. Therefore, with MR arthrography, contrast material may not enter the ganglion cysts. Because of this, it is important that fluid-sensitive sequences are included in the MR arthrographic imaging protocols, as images from those sequences may show the clearest or, sometimes, only evidence of such cysts.
Bone and Cartilage Abnormalities Associated with SLAP Lesions
- Chondral Print
Abnormalities of the articular cartilage and/or the subchondral bone plate of the humeral head may be associated with superior labral tears. These sites of chondral injury are referred to as a chondral print and may be seen with superior labral tears as well as with biceps tendon instability.36 The chondral print sign refers to the presence of this abnormality arthroscopically.36 Regarding the pathogenesis of this finding, abnormal pressure placed on the articular cartilage and subchondral bone plate can result in mechanical erosion. In an analysis of shoulder arthroscopic examinations demonstrating the chondral print sign, Patzer and colleagues found that types II through VII SLAP lesions were associated with an increased likelihood of such chondral print abnormalities.37 A subsequent study by Domos and colleagues found that when type I SLAP lesions are included, there is a statistically significant association of the chondral print sign with SLAP lesions (67% versus 37%, with a p-value of 0.01); however, if type 1 SLAP lesions are excluded, there is no statistically significant association of the chondral print sign with SLAP lesions.36 Finally, a lesion simulating a chondral print may be identified occasionally in MR images in persons with adhesive capsulitis of the glenohumeral joint, perhaps related to friction owing to the presence of adhesions involving the biceps tendon and humeral head.
- Labrochondral and Labro-osseous Avulsion and the “Pitcher’s Mound”
In rare instances, tensile force transmitted by the biceps tendon may lead to avulsive injuries that contain cartilage alone or both cartilage and bone together, in addition to labral tissue (Figure 42). As expected, these involve the superior portion of the labrum at the biceps tendon anchor, and the degree of displacement of the avulsed tissue is variable. Such avulsions do not fit into the traditional classification system for SLAP lesions.

42a

42b
Figure 42:
Labrochondral and labro-osseous avulsion. Rarely, labral avulsions are accompanied by additional avulsion of glenoid cartilage (42a, left) or glenoid cartilage and bone (42a, right) in the region of the biceps tendon anchor. Coronal T1 FS MRA (42b, left) and fat-suppressed T2-weighted MRA (42b, right) images show a large avulsive lesion of the superior glenoid articular surface (arrows), containing both cartilage and bone, occurring at the anchor of the biceps tendon. Note the large size of the resulting glenoid defect. (Courtesy of Diego F. Lemos, M.D.)

43a

43b

43c
Figure 43:
Pitcher’s mound. An oblique radiograph of the shoulder (43a) reveals a bone excrescence (arrow) arising from the superior articular surface of the glenoid, consistent with a pitcher’s mound. The bone excrescence is located near the posterosuperior aspect of the glenoid (arrows) as shown on the corresponding coronal (43b) and sagittal T1-weighted images from a non-contrast MRI study. (Courtesy of Diego F. Lemos, M.D.)
Treatment
Conservative measures with NSAIDs, physical therapy, and steroid injections are generally pursued initially for the treatment of SLAP lesions, along with physical therapy focusing on stretching the capsule and strengthening the rotator cuff muscles. While surgical management of SLAP lesions is a debatable subject, with the literature indicating mixed outcomes, thereby creating variability in the chosen surgical intervention, some general principles apply for each SLAP type.
SLAP I lesions are often subclinical, incidentally detected on arthroscopy and debrided only if significant labral fraying is visualized. SLAP II lesions were historically treated with suture anchors, though no consensus existed in terms of the number of anchors and suturing technique chosen for this treatment strategy. More recently, biceps tenodesis has been proposed in multiple studies to address SLAP II lesions, particularly for older and less active patients.39 Of note, Schroder and coworkers performed a double blinded randomized control study on patients with SLAP II lesions to compare outcomes between sham surgery and labral repair or biceps tenodesis, and these investigators found no significant difference between the sham surgery group and either the labral repair or biceps tenodesis group.40
Resection of the bucket-handle tear is performed for SLAP III and IV lesions, with careful attention to preserve the MGHL in order to minimize the development of anterior glenohumeral joint instability. For SLAP IV lesions, biceps tenodesis or tenotomy is performed if greater than 30 % of the biceps tendon is affected, with labral repair also performed for younger patients.
SLAP V and VI lesions are treated with labral repair and biceps tenodesis. SLAP VII to X lesions sometimes coincide with injuries of additional structures that require surgical evaluation in addition to the need to address the labral injury. MGHL repair, in addition to biceps tenodesis, is performed for SLAP VII lesions. SLAP VIII lesions are addressed with capsulolabral reconstruction, while debridement and shoulder stabilization are performed for SLAP IX and X lesions.4, 39
Conclusion
The differentiation of what have been designated as normal variations in the superior quadrants of the glenohumeral joint and SLAP lesions using MR imaging or MR arthrography represents a frequent diagnostic dilemma for radiologists. Knowledge of regional anatomy and the imaging characteristics of these so-called normal variants and pathologic lesions allows accurate diagnosis in many cases, although controversy persists regarding whether some variants are truly developmental and clinically insignificant or whether they are acquired and accompanied by clinical findings. With regard to SLAP lesions, the inclusion of degenerative fraying of the superior labrum as a SLAP lesion has clearly resulted in a perceived overutilization of the term in clinical practice. Complete characterization of true SLAP lesions requires the analysis of the precise location and morphology of the labral abnormalities and the determination if additional structures, including the tendon of the long head of the biceps brachii muscle, glenohumeral ligaments, and rotator interval, are involved. Including a Roman numeral as part of the description of a SLAP lesion is of far less clinical importance. The treatment of SLAP lesions is not uniform, ranging from conservative measures to surgical intervention, with reports of mixed outcomes for differing surgical approaches.
References
- Chang, E. Y., Fliszar, E., & Chung, C. B. (2012). Superior labrum anterior and posterior lesions and microinstability. Magnetic Resonance Imaging Clinics of North America, 20(2), 277–294. ↩
- Loredo, R., Longo, C., Salonen, D., Yu, J., Haghighi, P., Trudell, D., Clopton, P., & Resnick, D. (1995). Glenoid labrum: MR imaging with histologic correlation. Radiology, 196(1), 33–41. ↩
- Cooper, D. E., Arnoczky, S. P., OʼBrien, S. J., Warren, R. F., DiCarlo, E., & Allen, A. A. (1992). Anatomy, histology, and vascularity of the glenoid labrum. an anatomical study. The Journal of Bone & Joint Surgery, 74(1), 46–52. ↩
- Modarresi, S., Motamedi, D., & Jude, C. M. (2011). Superior labral anteroposterior lesions of the shoulder: Part 2, mechanisms and classification. American Journal of Roentgenology, 197(3), 604–611. ↩
- De Coninck, T., Ngai, S. S., Tafur, M., & Chung, C. B. (2016). Imaging the Glenoid Labrum and Labral Tears. RadioGraphics, 36(6), 1628–1647. ↩
- Beltran J, Rosenberg ZS, Chandnani VP, Cuomo F, Beltran S, Rokito A. (1997). Glenohumeral instability: evaluation with MR arthrography. Radiographics.17(3):657-73. ↩
- Zember, J. S., Rosenberg, Z. S., Kwong, S., Kothary, S. P., & Bedoya, M. A. (2015). Normal Skeletal Maturation and Imaging Pitfalls in the Pediatric Shoulder. RadioGraphics, 35(4), 1108–1122. ↩
- Kothary, S., Rosenberg, Z.S., Poncinelli, L.L. et al. (2014). Skeletal development of the glenoid and glenoid–coracoid interface in the pediatric population: MRI features. Skeletal Radiol 43, 1281–1288. ↩
- Ruiz Santiago F, Martínez Martínez A, Tomás Muñoz P, Pozo Sánchez J, Zarza Pérez A. (2017). Imaging of shoulder instability. Quant Imaging Med Surg. Aug;7(4):422-433. ↩
- Huber, W. P., & Putz, R. V. (1997). Periarticular fiber system of the shoulder joint. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 13(6), 680–691. ↩
- The Glenoid Labrum. Shoulderdoc.co.uk. (2023). https://www.shoulderdoc.co.uk/article/1340 ↩
- Burkhart, S. S., & Morgan, C. D. (1998). The peel-back mechanism: its role in producing and extending posterior type II slap lesions and its effect on SLAP repair rehabilitation. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 14(6), 637–640. ↩
- Park, Y. H., Lee, J. Y., Moon, S. H., Mo, J. H., Yang, B. K., Hahn, S. H., & Resnick, D. (2000). MR arthrography of the labral capsular ligamentous complex in the shoulder. American Journal of Roentgenology, 175(3), 667–672. ↩
- Modarresi, V., Motamedi, D., Jude, C. (2011). Superior Labral Anteroposterior Lesions of the Shoulder: Part 1, Anatomy and Anatomic Variants. American Journal of Roentgenology.197:3, 596-603 ↩
- Giacomo, D. (2011). Atlas of Functional Shoulder Anatomy. Springer. ↩
- Petchprapa, C. N., Beltran, L. S., Jazrawi, L. M., Kwon, Y. W., Babb, J. S., & Recht, M. P. (2010). The rotator interval: A review of anatomy, function, and normal and abnormal MRI appearance. American Journal of Roentgenology, 195(3), 567–576. ↩
- Chung, C. B., Dwek, J. R., Cho, G. J., Lektrakul, N., Trudell, D., & Resnick, D. (2000). Rotator cuff interval: evaluation with MR Imaging and MR arthrography of the shoulder in 32 cadavers. Journal of Computer Assisted Tomography, 24(5), 738–743. ↩
- Pouliart N, Gagey OJ. (2005). The arthroscopic view of the glenohumeral ligaments compared with anatomy: fold or fact? J Shoulder Elbow Surg. 14(3):324-8. ↩
- Bencardino JT, Beltran J. (2004). MR imaging of the glenohumeral ligaments. Magnetic Resonance Imaging Clinics of North America.12:11-24. ↩
- Merila, M., Leibecke, T., Gehl, HB. et al. (2004). The anterior glenohumeral joint capsule: macroscopic and MRI anatomy of the fasciculus obliquus or so-called ligamentum glenohumerale spirale . Eur Radiol 14, 1421–1426. ↩
- Merila, M., Heliö, H., Busch, L. C., Tomusk, H., Poldoja, E., Eller, A., Kask, K., Haviko, T., & Kolts, I. (2008). The spiral glenohumeral ligament: an open and arthroscopic anatomy study. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 24(11), 1271–1276. ↩
- Williams MM, Snyder SJ, Buford D Jr. (1994). The Buford complex–the “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex: a normal anatomic capsulolabral variant. Arthroscopy. Jun;10(3):241-7. ↩
- Hita-Contreras F, Sanchez-Montesinos I, Martınez-Amat A, Cruz-Dıaz D, Barranco RJ, and Roda O. (2018). Development of the human shoulder joint during the embryonic and early fetal stages: anatomical considerations for clinical practice. J. Anat. 232, pp422—430. ↩
- Chauvin NA, Jaimes C, Ho-Fung V, Wells L, Ganley T, Jaramillo D. (2013). Diagnostic performance of magnetic resonance arthrography of the shoulder in children. Pediatr Radiol. 43:1309–1315 ↩
- Tena-Arregui J, Barrio-Asensio C, Puerta-Fonollá J, Murillo-González J. (2005). Arthroscopic study of the shoulder joint in fetuses. Arthroscopy: The Journal of Arthroscopic and Related Surgery, Vol 21, No 9 (September). pp 1114-1119. ↩
- Snyder SJ, Karzel RP, Del Pizzo W, Ferkel RD, Friedman MJ. (1990). SLAP lesions of the shoulder. Arthroscopy. 6:274-279. ↩
- Maffet MW, Gartsman GM, Moseley B. (1995). Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med, 23:93-98. ↩
- Clark RC, Chandler CC, Fuqua AC, Glymph KN, Lambert GC, Rigney KJ. (2019). Use of clinical test clusters versus advanced imaging studies in the management of patients with a suspected SLAP tear. Int J Sports Phys Ther. Jun;14(3):345-352. ↩
- Familiari F, Huri G, Simonetta R, McFarland EG. (2019). SLAP lesions: current controversies. EFORT Open Rev. Jan 28;4(1):25-32. ↩
- Mohana-Borges AV, Chung CB, Resnick D. (2003). Superior labral anteroposterior tear: classification and diagnosis on MRI and MR arthrography. AJR; 181:1449-1462. ↩
- Smith, D. K., Chopp, T. M., Aufdemorte, T. B., Witkowski, E. G., & Jones, R. C. (1996). Sublabral recess of the superior glenoid labrum: study of cadavers with conventional nonenhanced MR imaging, MR Arthrography, anatomic dissection, and limited histologic examination. Radiology, 201(1), 251–256. ↩
- Hunter, J. C., Blatz, D. J., & Escobedo, E. M. (1992). SLAP lesions of the glenoid labrum: CT arthrographic and arthroscopic correlation. Radiology, 184(2), 513–518. ↩
- Van Steyn, M.O., Mariscalco, M.W., Pedroza, A.D. et al. (2016). The hypermobile lateral meniscus: a retrospective review of presentation, imaging, treatment, and results. Knee Surg Sports Traumatol Arthrosc 24, 1555–1559. ↩
- Dunham KS, Bencardino JT, Rokito AS. (2012). Anatomic variants and pitfalls of the labrum, glenoid cartilage, and glenohumeral ligaments Magn Reson Imaging Clin N Am 20. 213–228. ↩
- Tung GA, Entzian D, Stern JB, and Green A. (2000). MR imaging and MR arthrography of paraglenoid labral cysts. American Journal of Roentgenology.74: 1707-1715. ↩
- Domos P, Neogi DS, Longo UG, Ahrens PM. (2017). The chondral print sign: what does it really mean? J Shoulder Elbow Surg.Jun;26(6):e188-e192. ↩
- Patzer, T., Lichtenberg, S., Kircher, J., Magosch, P., & Habermeyer, P. (2010). Influence of SLAP lesions on chondral lesions of the glenohumeral joint. Knee Surgery, Sports Traumatology, Arthroscopy, 18(7), 982–987. ↩
- Pearce CE, Burkhart SS. (2000). The pitcher’s mound: a late sequela of posterior type II SLAP lesions. Arthroscopy. Mar;16(2):214-6. ↩
- Bijayendra Singh, N Baktl. (2017). The Diagnosis and Management of Superior Labral (SLAP) Tears of the Shoulder: A Review Article. Acta of Shoulder and Elbow Surgery; 2(1): 15-21. ↩
- Schrøder CP, Skare Ø, Reikerås O, et al. (2017). Sham surgery versus labral repair or biceps tenodesis for type II SLAP lesions of the shoulder: a three-armed randomized clinical trial. British Journal of Sports Medicine. 51:1759-1766. ↩
