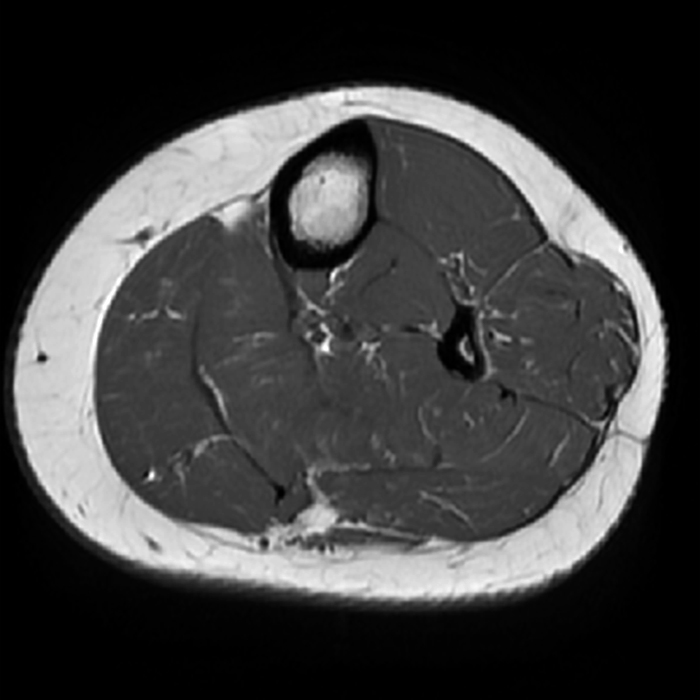
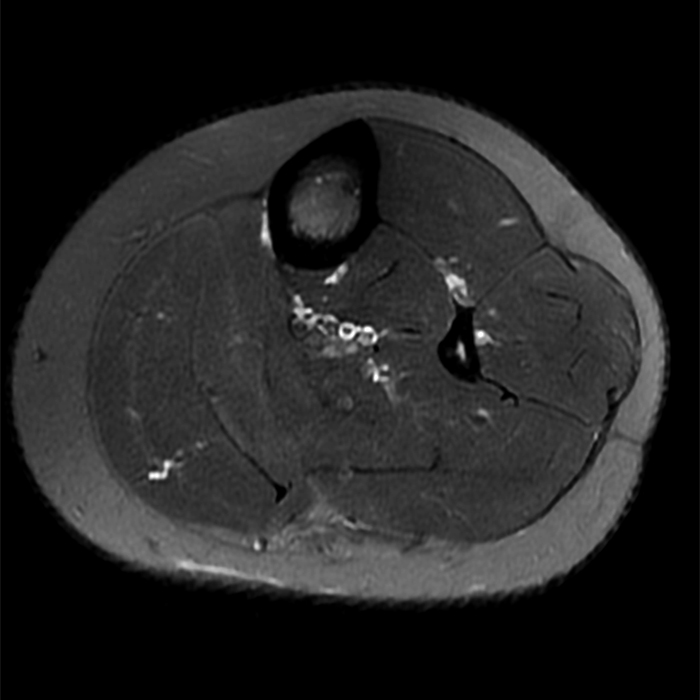
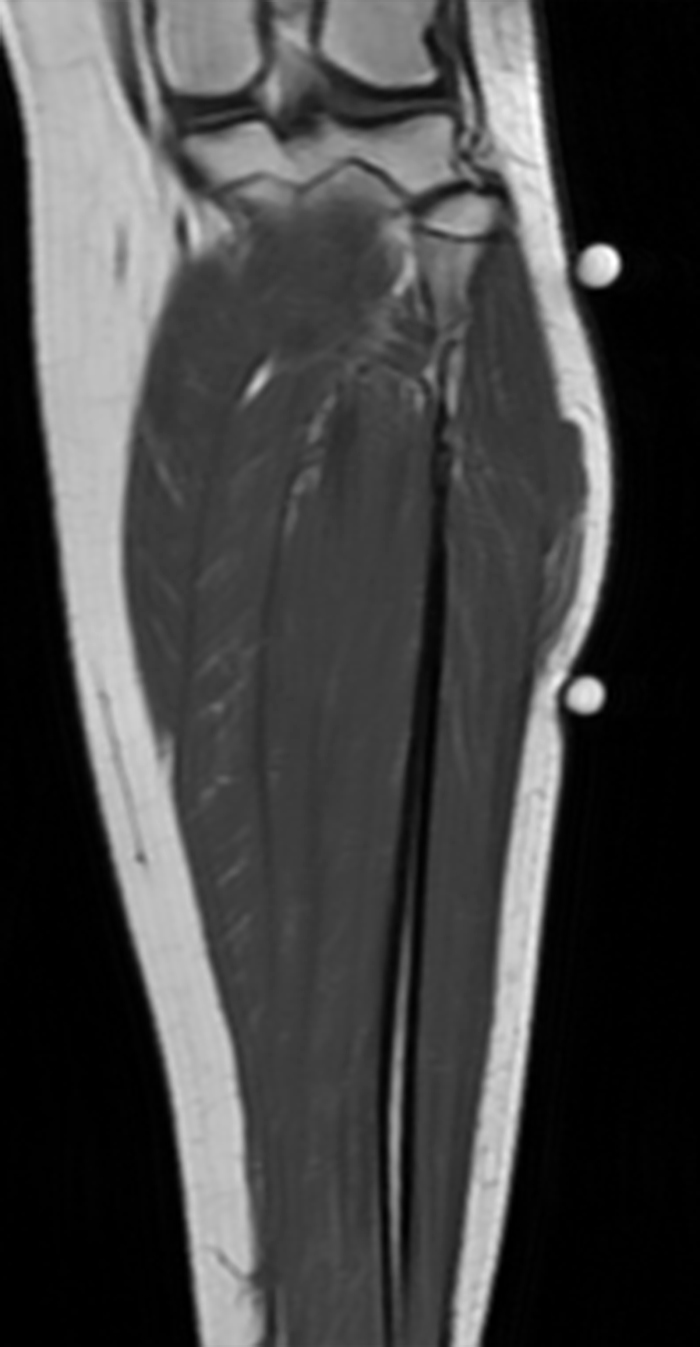
Clinical History: A 13-year-old girl presents with a 10-day history of lateral left leg pain and a palpable mass which persisted after a period of prolonged walking. The patient denies recent injury. Physical exam revealed scar formation overlying the palpable abnormality at the site of a remote dog bite. Axial T1 (1a) and T2-weighted fat suppressed images (1b) are provided with coronal T1-weighted (1c) and STIR (1d) images. What are the findings? What is your diagnosis?

Findings
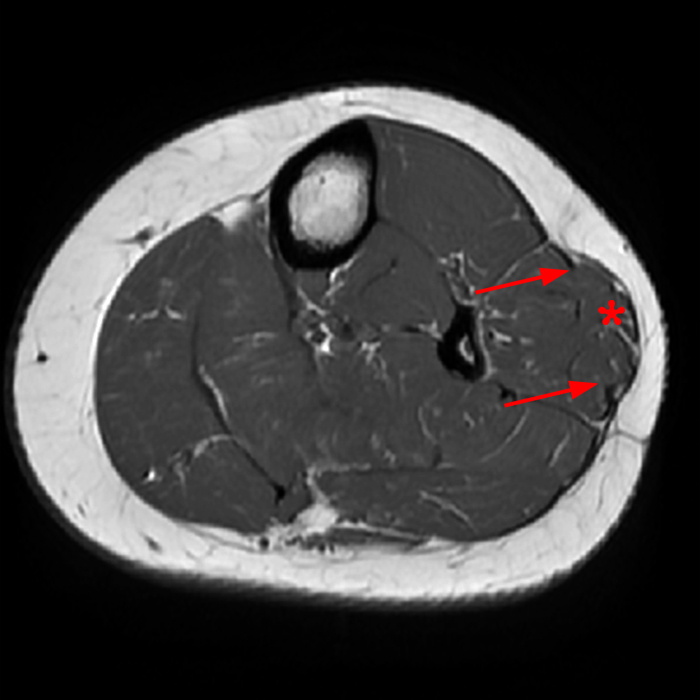
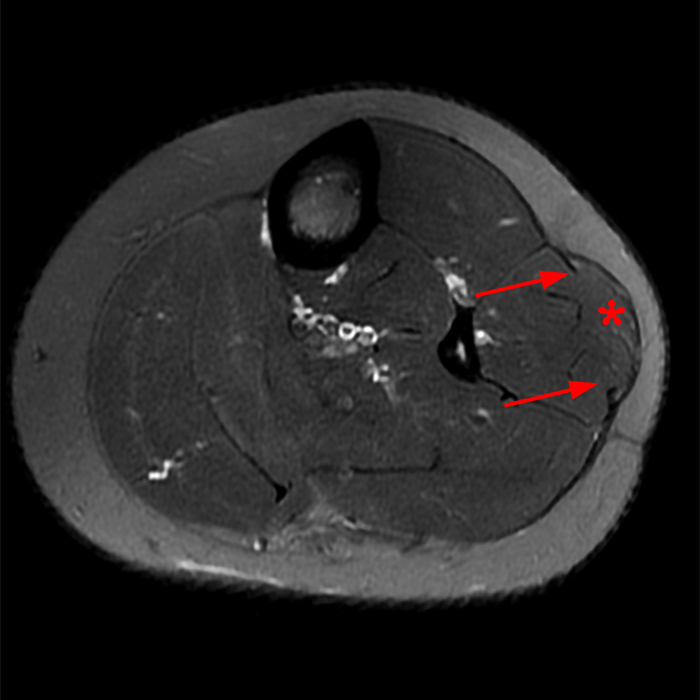


Figure 2: The Axial T1- (2a) and T2-weighted fat suppressed image (2b) demonstrate a defect (arrows) in the superficial layer of the deep fascia of the lateral compartment of the proximal lower leg at the superficial aspect of the peroneus longus muscle belly. The longitudinal extent of the fascial defect (arrows) is appreciated on the coronal T1-weighted (2c) and STIR images (2d). The palpable soft tissue “mass” has the same signal intensity as the adjacent muscle and corresponds to the herniated peroneus longus muscle belly (asterisks). Note the MR compatible cutaneous markers which bracket the palpable abnormality (arrowheads).
Diagnosis
Peroneus Longus Muscle herniation.
Introduction
A muscle hernia occurs when the muscle protrudes through a defect in the deep peripheral fascia, the epimysium, into the subcutaneous fat.1 Ihde divided muscle hernias into post-traumatic and constitutional.2 Post-traumatic muscle hernias occur secondary to a penetrating injury, blunt trauma with contracted muscle, or surgery (Figure 3) that results in a fascial tear which permits herniation of the muscle into the subcutaneous fat.3,4 Constitutional muscle hernias occur due to vigorous exercise, muscle hypertrophy, and elevated intra-compartmental pressure with subsequent muscle herniation at points of fascial weakness, including sites at which the neurovascular bundle traverses the fascia.2,3,4,5,6 Constitutional muscle hernias with secondary nerve compression have been most frequently reported to affect the superficial peroneal nerve in the lower leg as it exits into the subcutaneous fat of the anterolateral aspect of the distal third of the leg (Figure 4).7,8,9
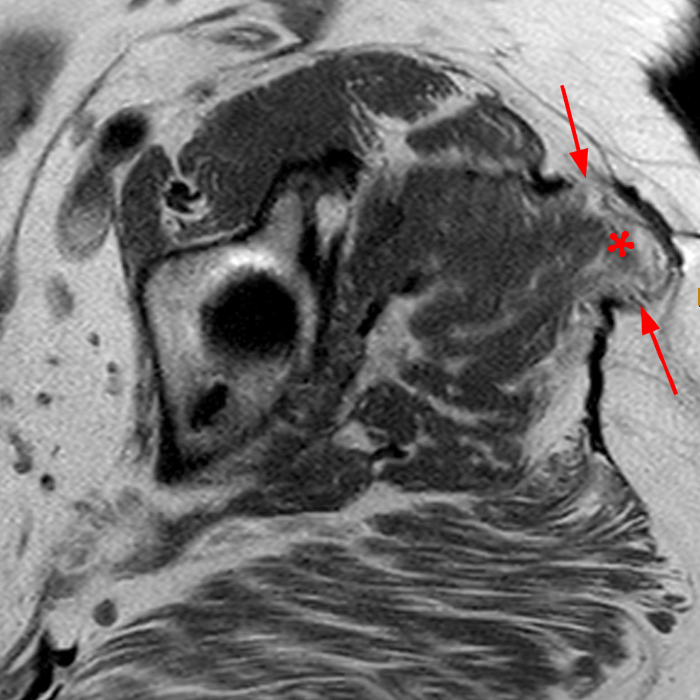
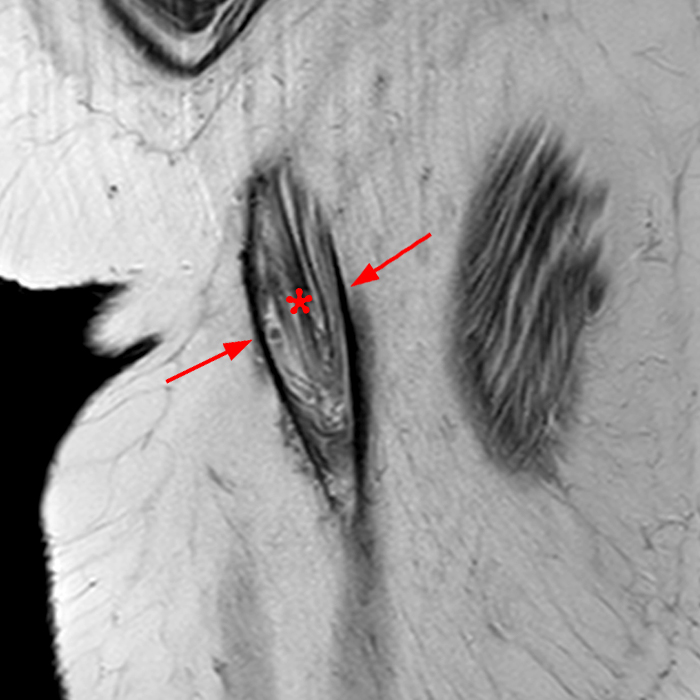
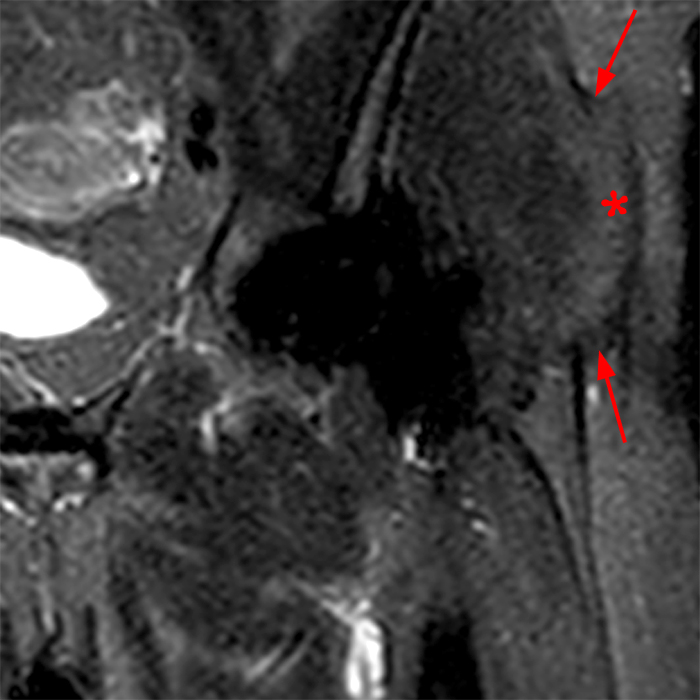
Figure 3: 64-year-old woman with generalized left hip pain since total hip arthroplasty 1 year prior. Axial T1-weighted image (3a), T2-weighted sagittal image (3b), and coronal STIR image (3c) show a post-operative defect in the iliotibial band and superficial fascia of the gluteus medius (arrows) with herniation of the gluteus medius muscle (asterisk) through the defect into the adjacent subcutaneous fat. Note the signal and architecture of the herniated muscle is equivalent to the adjacent muscle.
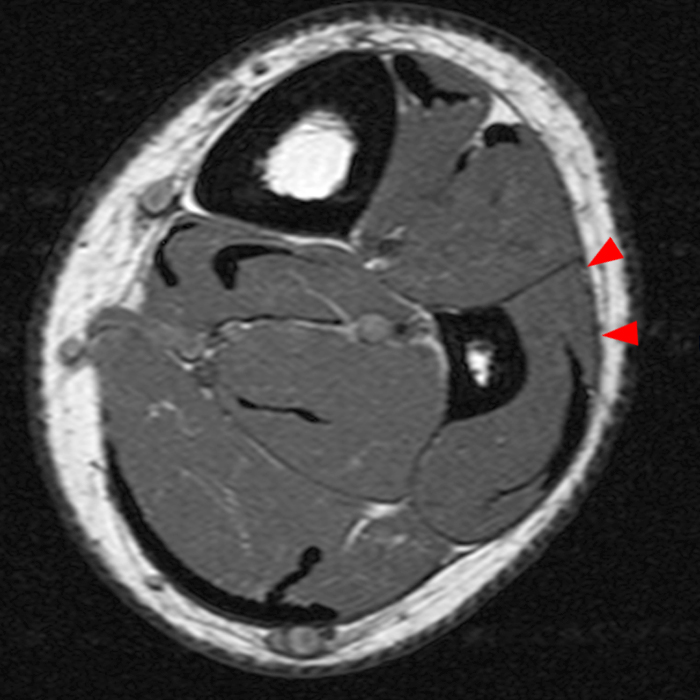
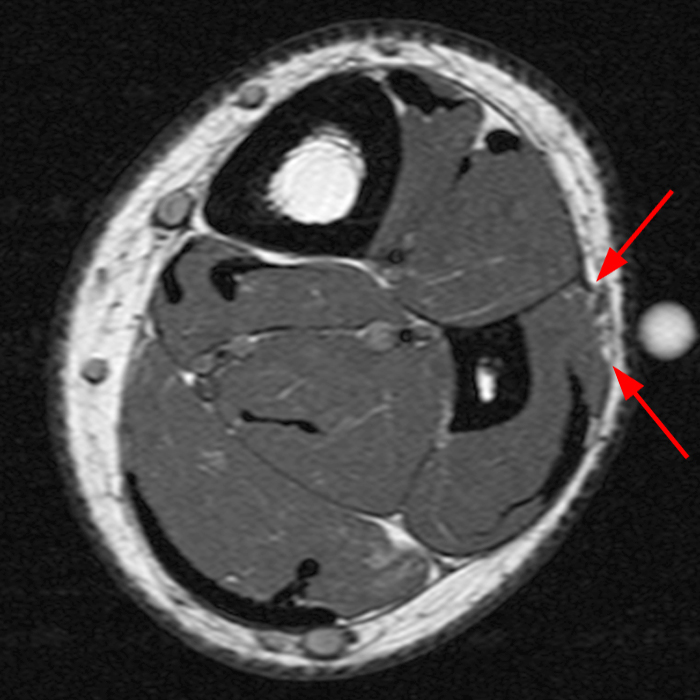
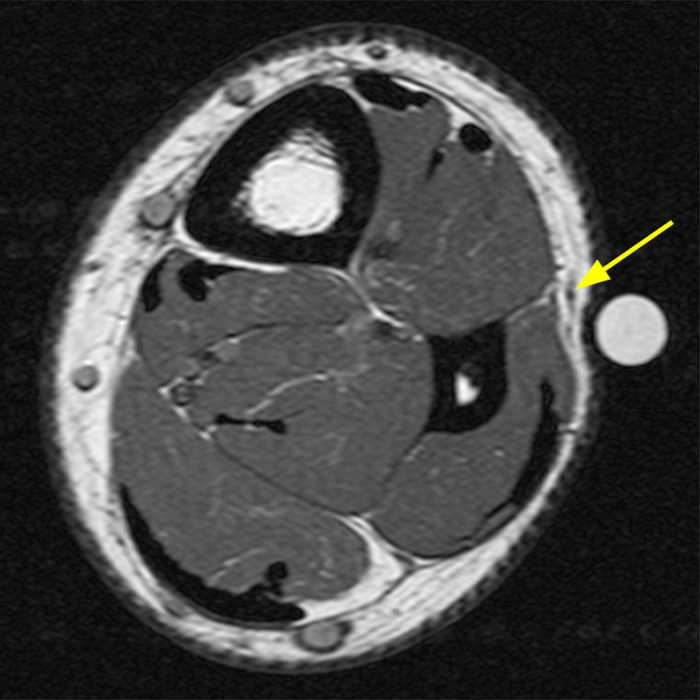
Figure 4: 23-year-old man presents with parasthesias in the ankle and foot and a mass above the ankle for years that is painful with running. Consecutive T1-weighted axial images of the lower leg. Cranial most axial image (4a) demonstrates the intact T1 dark fascia of the peroneus brevis (arrowheads). The middle image (4b) demonstrates a defect in the fascia (arrows), with slight bulge in the contour of the adjacent muscle, where the superficial peroneal nerve exits the lateral compartment, a constitutional muscle hernia. On the caudal most image (4c) the superficial peroneal nerve is well identified in the adjacent superficial subcutaneous fat (yellow arrow).
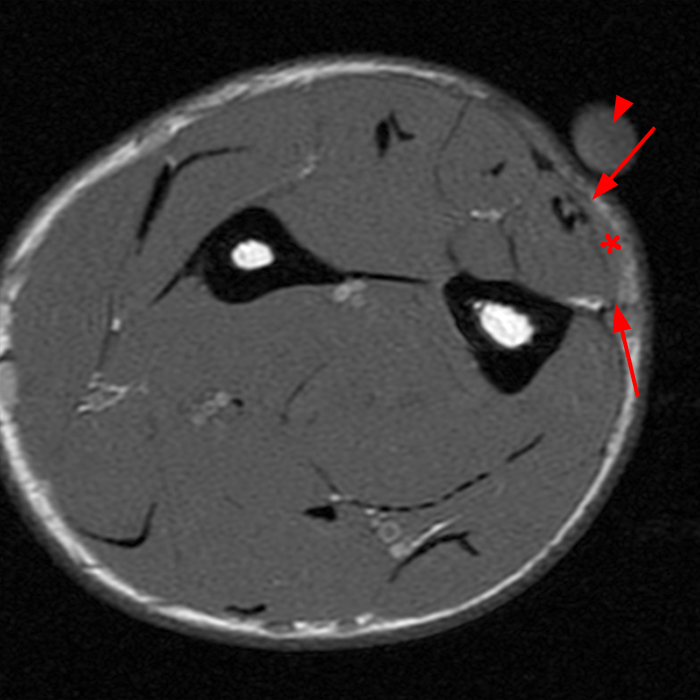
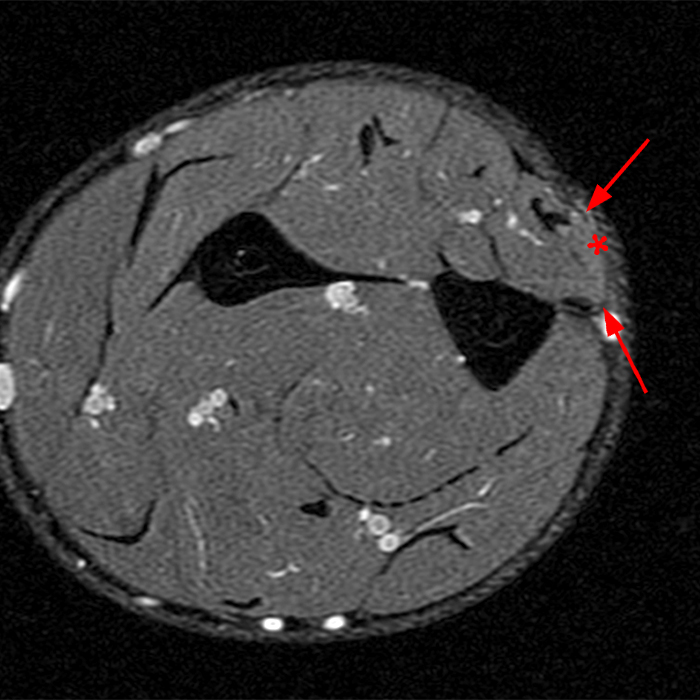
Figure 5: 29-year-old man presents with focal pain and swelling at the ulnar aspect of the mid forearm. He reports a remote history of laceration with exploratory surgery. Axial T1 (5a) and fat suppressed proton density-weighted (5b) images show a short segment bulge in the contour of the extensor carpi ulnaris muscle (asterisk), extending into the adjacent subcutaneous fat between a focal defect in the overlying fascia (arrows). A cutaneous marker (arrowhead) was included to facilitate assessment of the mass.
Clinical Presentation
Patients with muscle hernias most commonly present with a history of trauma and a palpable mass which may be asymptomatic or painful with exertion.4,12,13 On physical exam the mass is typically soft and reducible. The fascial defect can often be palpated.4,12,14 When the muscle is contracted the palpable abnormality may enlarge.11,14,15 The swelling may decrease with rest or, for those in the lower extremity, supine positioning.15 With constitutional hernias, occurring at sites where nerves traverse the fascia, patients may present with numbness, paresthesia, and/or hyperalgesia and have a positive Tinel’s sign on physical examination.7–9
Imaging
Appropriate imaging is critical to confirm and assess the extent of muscle injuries, exclude soft tissue masses and mimics, and help guide appropriate treatment. In cases where there is an appropriate clinical history, physical exam, and high index of suspicion for muscle hernia, ultrasound is an appropriate initial imaging exam.11 In addition to a high accuracy in the assessment of muscle hernia it offers the advantage of dynamic imaging, including imaging muscle contraction or in an upright position, and at a lower cost and increased availability.3,11,14,16 A targeted ultrasound exam should be performed with a high frequency linear probe. Both sides should be prepped for imaging as comparison with the contralateral side may increase diagnostic confidence in subtle cases. At ultrasound the thin superficial layer of the deep fascia at the interface of the subcutaneous fat and muscle is visualized as a thin echogenic, bright, line superficial to the muscle. A muscle hernia appears as a discontinuity in the echogenic fascia with muscle protruding into the defect (Figure 5).15 The muscle may be less echogenic than the adjacent non-herniated muscle.15 One pitfall to be mindful of when performing ultrasound is that excessive pressure with the ultrasound probe may reduce the hernia and result in a false negative exam.8,15

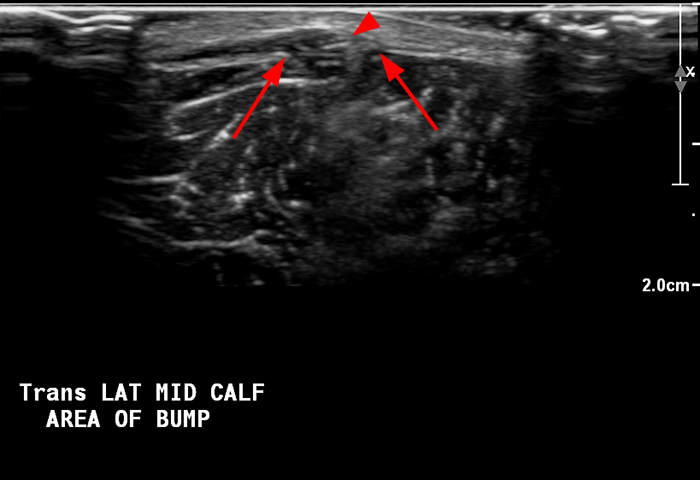

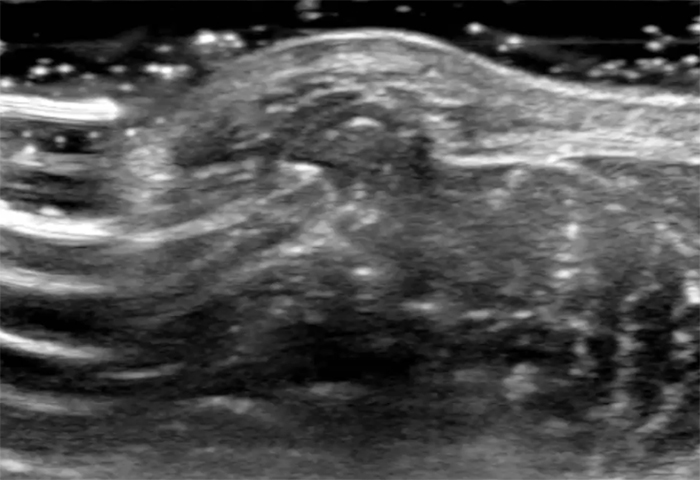
Figure 6: 54-year-old man with a history of chronic venous stasis presents with a persistent “bump” anteriorly at the mid lower leg. Longitudinal grey scale ultrasound image at site of palpable abnormality with the patient supine (6a) shows a focal bulge in the contour of the adjacent muscle (arrowhead). Transverse, axial image (6b) again shows an abnormal protrusion of the muscle (arrowhead) into the subcutaneous fat through a defect in the echogenic fascia (arrows). On longitudinal image with the patient in the upright position (6c) the muscle protrusion enlarges (arrowhead) and the fascial defect is visible (red arrows) diagnostic of a muscle hernia. Transverse cine (6d) ultrasound of the fascial defect demonstrates reduction of the muscle hernia with increasing compression with the ultrasound probe.
Click here to view video of figure 6D.
The excellent soft tissue contrast and high spatial resolution of MRI makes it well suited to evaluate muscle injury, muscle hernia, and the alternative differential considerations in the assessment of a soft tissue mass. The diagnostic accuracy of MRI and US for evaluation of muscle hernia are comparable.11 MRI offers the advantage of better identifying which muscle is involved and characterizing any identified soft tissue mass.10 As with other small soft tissue masses, high resolution MR images should be acquired with a small field of view and thin sections with MRI compatible skin markers bracketing the palpable abnormality. At MRI muscle hernias appear as an abnormal bulge in the contour of the muscle or protrusion of the muscle into the subcutaneous fat.10,13,14 The T1 and T2 signal and architecture of the herniated muscle is usually normal, though increased T2 signal, indicative of edema, has been attributed to muscle tearing, impingement, or altered perfusion.10,16 A defect in the fascia is not always visualized, though it can be inferred from the abnormal muscle contour.11 Axial images typically better demonstrate the muscle hernia and fascial defect, while orthogonal images better characterize the longitudinal location and extent (Figure 2).10
Differential
The differential diagnosis for a palpable soft tissue mass is broad and varies by location. In locations where muscle hernias are commonly encountered the primary differential considerations include post-traumatic foreign body (Figure 7), hematoma, and muscle tear; and neoplastic entities including lipoma (Figure 8) and nerve sheath tumor (Figure 9).8,17,18 In the forearm the differential includes congenital accessory muscles, which can mimic a muscle hernia both clinically and on imaging exams (Figure 10).12
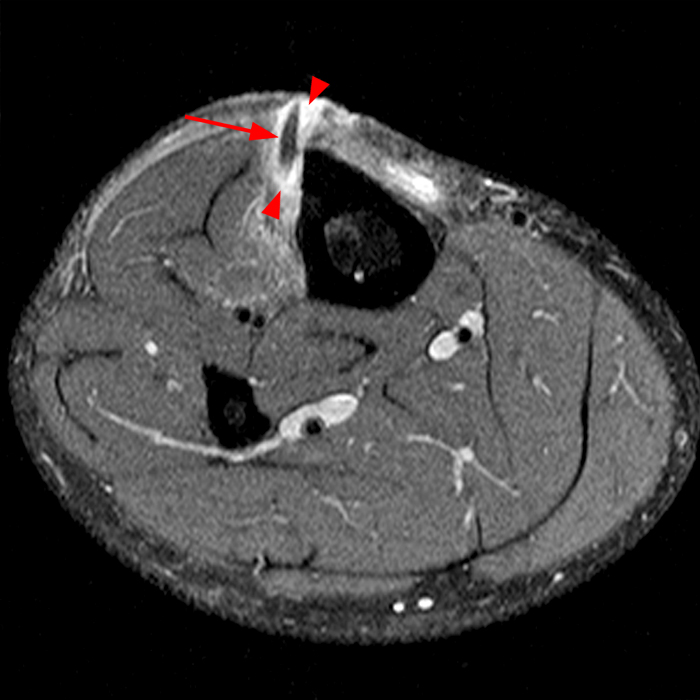
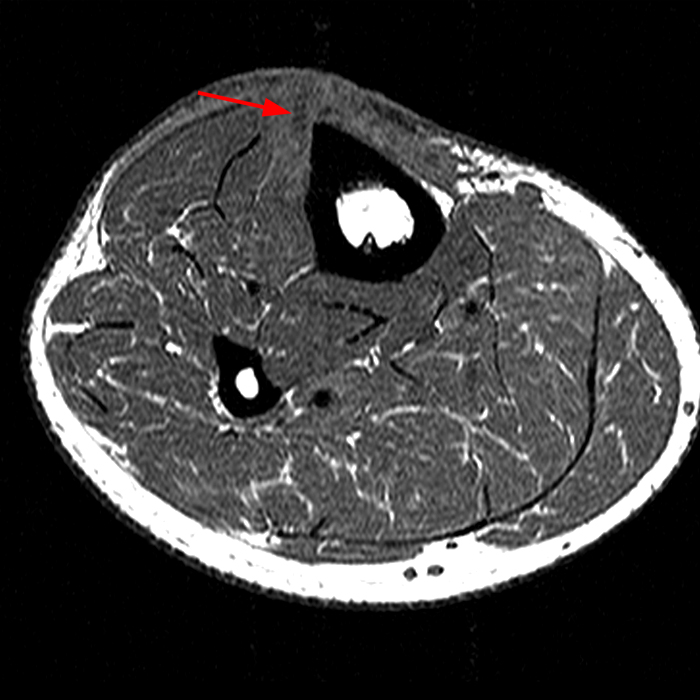
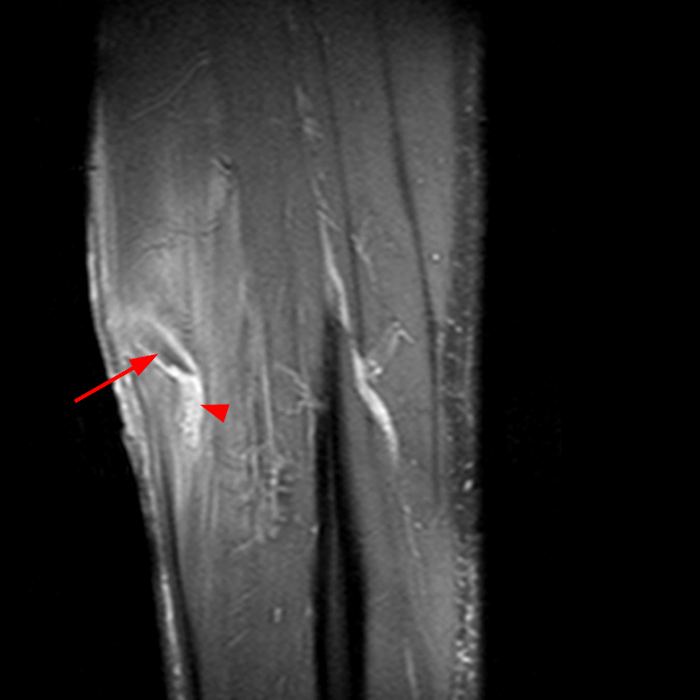

Figure 7: 40-year-old man presents with 1 month history of mid anterior tibial pain and swelling. History of fall one month prior with penetrating injury. Axial fat-suppressed proton density-weighted axial (7a), axial T1-weighted (7b), and sagittal STIR (7c) images demonstrate a sharply marginated linear foreign body (arrows) hypointense to muscle on T1 and T2-weighted images. The foreign body extends through the subcutaneous fat of the anteromedial leg, through the superficial layer of the deep fascia, and into the anterior tibialis muscle. Phlegmon or foreign body granulomatous reaction (arrowheads) surrounds the foreign body. Anterior soft tissue swelling (asterisk) without a radiodense foreign body is identified on lateral radiograph of the tibia-fibula (7d).


Figure 8: 67-year-old woman presents with non-painful, atraumatic, dorsal forearm mass for several years. Sagittal T1-weighted image (8a) shows a mass (asterisk) in the subcutaneous fat of the proximal forearm abutting the superficial layer of the deep fascia with a thin T1 dark capsule (arrows). The mass is isointense to subcutaneous fat and its signal homogenously suppresses on an axial STIR image (8b) without soft tissue nodule or thick septations. The findings are diagnostic of a simple lipoma.
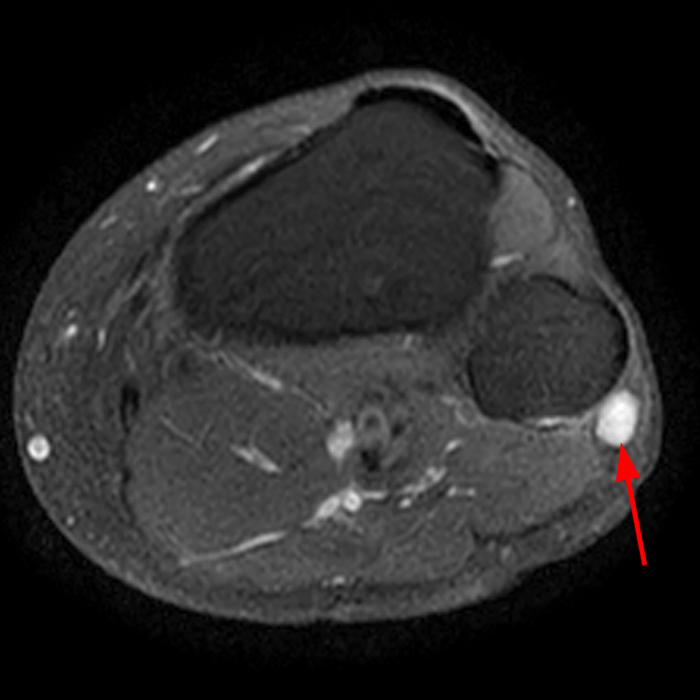
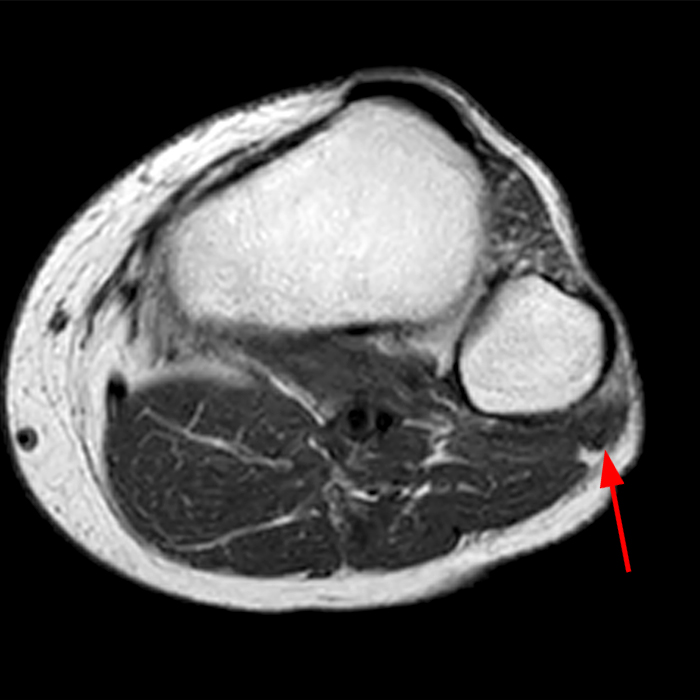
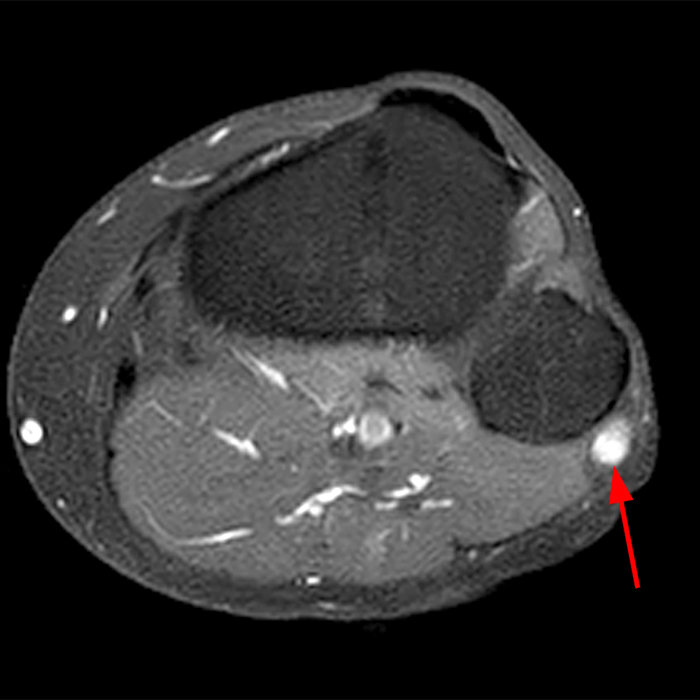
Figure 9: 57-year-old man presents with pain and lump superficial to the fibular head. Axial fat-suppressed proton density-weighted weighted image (9a) demonstrates a T2 hyperintense soft tissue nodule superficial to the fibula (arrow). On coronal and sagittal images, not shown, it did not extend to the joint and was contiguous with the common peroneal nerve. Pre-contrast T1-weighted axial image (9b) and fat suppressed T1-weighted post contrast image (9c) show homogeneous enhancement which in combination with the location is diagnostic of a nerve sheath tumor.
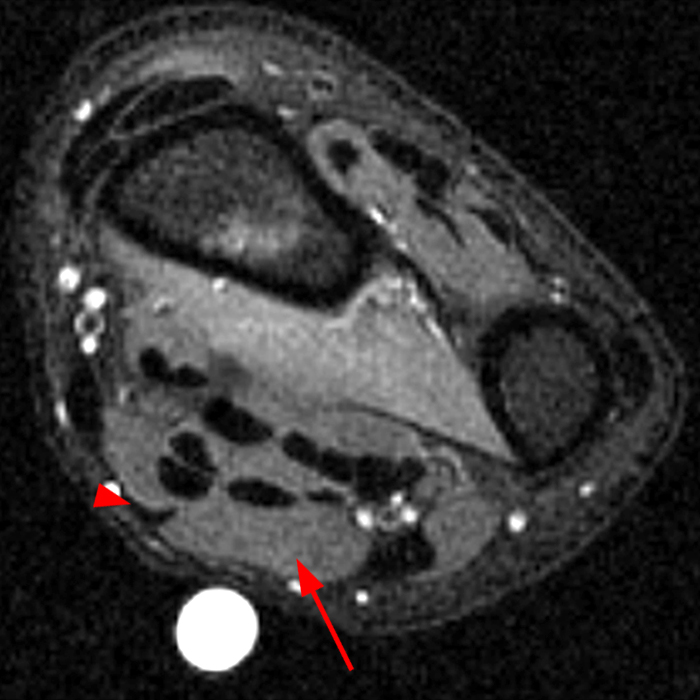
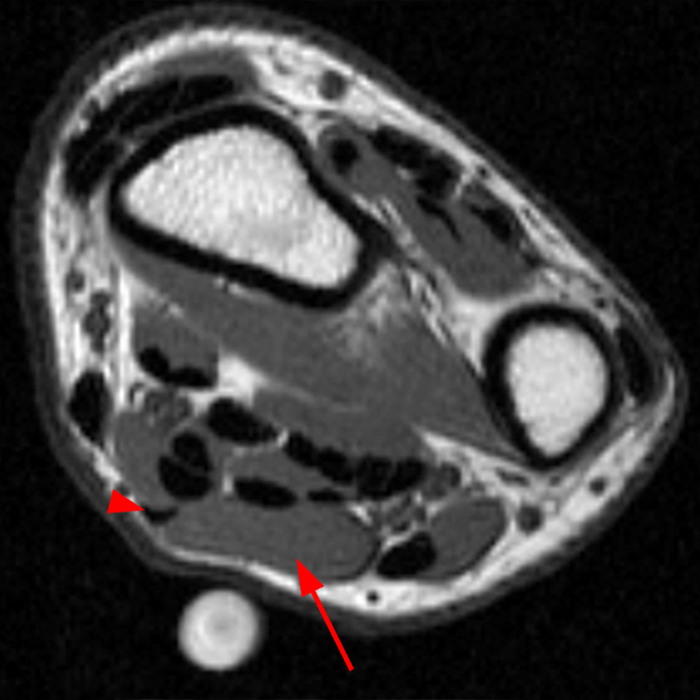
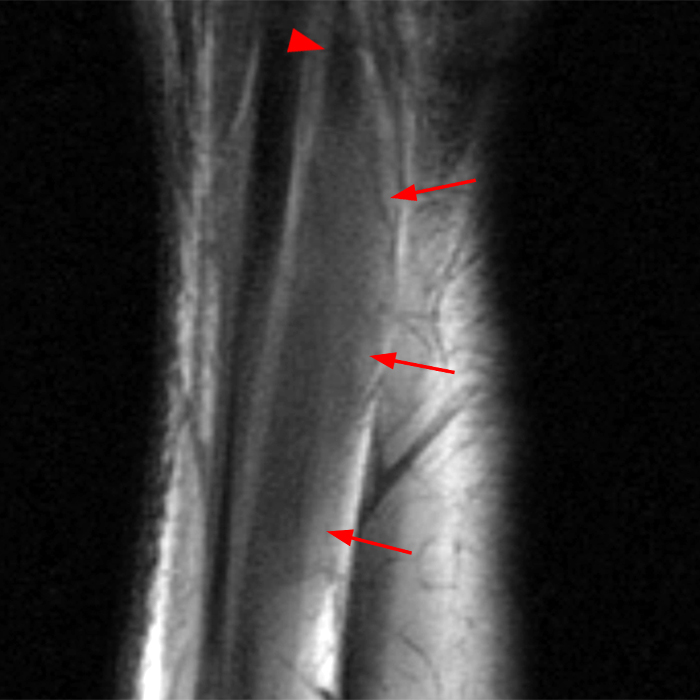
Figure 10: 42-year-old man presents with soft tissue mass in the volar aspect of the distal forearm. Axial T2-weighted fat suppressed image (10a), axial (10b) and coronal T1-weghted images (10c) demonstrate a long segment fusiform mass (arrow) which has the same architecture and signal intensity as muscle on both T1- and T2-weighted images. The muscle is contiguous with the palmaris longus tendon (arrowhead) consistent with a reversed or digastric palmaris longus muscle, a normal variant.
Treatment and Prognosis
The treatment of muscle hernias is guided by the patient’s presenting symptoms. In patients presenting with concern for soft tissue mass without focal pain, muscle hernias can be treated with reassurance.15,19 For patients with mild symptoms, including cramping, aching pain, and exertional discomfort the initial treatment is conservative with rest, activity modification, and support hose.10,19 In patients with moderate to severe pain, or for patients that fail conservative treatment, there are a variety of surgical options, with fasciotomy being the most widely accepted.5,12,19 Fasciotomy enlarges the fascial defect, allows unhindered muscle excursion, and eliminates the risk of future muscle ischemia or strangulation.6,8,12 Alternative surgical treatments include direct repair, muscle excision, fascial grafting, and mesh grafting.10,19 Direct repair is typically avoided in the lower leg due to the possibility of post-operative compartment syndrome.19,20 In a survey of athletes who underwent fasciotomy for symptomatic muscle hernia, Kramer et al. found that 82% of patients were satisfied with the results and 65% had returned to sports.5
Summary
Muscle hernias are the uncommon result of a direct muscle injury which results in a fascial defect through which the underlying muscle can herniate. Patients with muscle hernia most frequently present with a palpable soft tissue mass which may be reducible on physical exam. Imaging is essential to assess the extent of muscle injury and to exclude other causes of a palpable soft tissue masses. On MR imaging, careful assessment of the muscle contour and the thin superficial fascia at the site of a palpable abnormality are essential for diagnosis. The most commonly accepted treatment for patients with severe or persistent pain attributed to muscle hernias is fasciotomy with extension of the fascial defect allowing unhindered muscle excursion and preventing muscle ischemia.
References
- Kirchgesner T, Tamigneaux C, Acid S, et al. Fasciae of the musculoskeletal system: MRI findings in trauma, infection and neoplastic diseases. Insights Imaging. 2019;10(1):47. doi:10.1186/s13244-019-0735-5 ↩
- Ihde H. On muscular hernia of the leg. Acta Chir Scand . 1929;65:97-120. ↩
- Kendi TK, Altinok D, Erdal HH, Kara S. Imaging in the diagnosis of symptomatic forearm muscle herniation. Skeletal Radiol. 2003;32(6):364-366. doi:10.1007/s00256-002-0615-8 ↩
- Zeiss J, Ebraheim NA, Woldenberg LS. Magnetic resonance imaging in the diagnosis of anterior tibialis muscle herniation. Clin Orthop Relat Res. 1989;(244):249-253. ↩
- Kramer DE, Pace JL, Jarrett DY, Zurakowski D, Kocher MS, Micheli LJ. Diagnosis and management of symptomatic muscle herniation of the extremities: a retrospective review. Am J Sports Med. 2013;41(9):2174-2180. doi:10.1177/0363546513493598 ↩
- Mellado JM, Pérez del Palomar L. Muscle hernias of the lower leg: MRI findings. Skeletal Radiol. 1999;28(8):465-469. doi:10.1007/s002560050548 ↩
- Tong O, Bieri P, Herskovitz S. Nerve entrapments related to muscle herniation. Muscle Nerve. 2019;60(4):428-433. doi:10.1002/mus.26643 ↩
- Foresti M. Superficial peroneal nerve compression due to peroneus brevis muscle herniation. J Radiol Case Rep. 2019;13(11):10-17. doi:10.3941/jrcr.v13i11.3757 ↩
- Paolasso I, Cambise C, Coraci D, et al. Tibialis anterior muscle herniation with superficial peroneal nerve involvement: Ultrasound role for diagnosis and treatment. Clin Neurol Neurosurg. 2016;151:6-8. doi:10.1016/j.clineuro.2016.09.019 ↩
- Naffaa L, Moukaddam H, Samim M, Lemieux A, Smitaman E. Semimembranosus muscle herniation: a rare case with emphasis on muscle biomechanics. Skeletal Radiol. 2017;46(3):373-378. doi:10.1007/s00256-016-2553-x ↩
- Zhou X, Zhan W, Chen W, et al. The value of ultrasound in the preoperative diagnosis of muscle herniation: A comparison with magnetic resonance imaging. Eur J Radiol. 2017;94:191-194. doi:10.1016/j.ejrad.2017.06.026 ↩
- Olch CL, Watson HK. Symptomatic forearm fascial hernia. J Hand Surg Am. 1996;21(4):693-695. doi:10.1016/s0363-5023(96)80030-x ↩
- Guermazi A, Roemer FW, Robinson P, Tol JL, Regatte RR, Crema MD. Imaging of Muscle Injuries in Sports Medicine: Sports Imaging Series. Radiology. 2017;282(3):646-663. doi:10.1148/radiol.2017160267 ↩
- Flores D V, Mejía Gómez C, Estrada-Castrillón M, Smitaman E, Pathria MN. MR Imaging of Muscle Trauma: Anatomy, Biomechanics, Pathophysiology, and Imaging Appearance. Radiographics. 2018;38(1):124-148. doi:10.1148/rg.2018170072 ↩
- Beggs I. Sonography of muscle hernias. AJR Am J Roentgenol. 2003;180(2):395-399. doi:10.2214/ajr.180.2.1800395 ↩
- Dierickx J, Vanhoenacker F. Muscle Herniation: An Often-Missed Pseudotumor. J Belg Soc Radiol. 2020;104(1):62. doi:10.5334/jbsr.2294 ↩
- Sara L. Foreign body misdiagnosed as myofascial herniation of tibialis anterior muscle. Journal of orthopaedics for physician assistants. 2021;9(2). doi:10.2106/jbjs.jopa.20.00038 ↩
- Kotha KMR, Tandra VS, Murthy GVS, Vutukuri SR, Vyjayanthi Y. Tibialis anterior partial rupture mimicking muscle hernia: a rare case report. J Clin Diagn Res. 2014;8(10):LD08-9. doi:10.7860/JCDR/2014/10410.5056 ↩
- Dönmez G, Evrenos MK, Cereb M, Karanfil Y, Doral MN. Double layer repair of tibialis anterior muscle hernia in a soccer player: a case report and review of the literature. Muscles Ligaments Tendons J. 2015;5(4):331-334. doi:10.11138/mltj/2015.5.4.331 ↩
- Wolfort GF, Mogelvang C, Filtzer HS. Anterior tibial compartment syndrome following muscle hernia repair. Arch Surg. 1973;106(1):97-99. doi:10.1001/archsurg.1973.01350130095022 ↩
