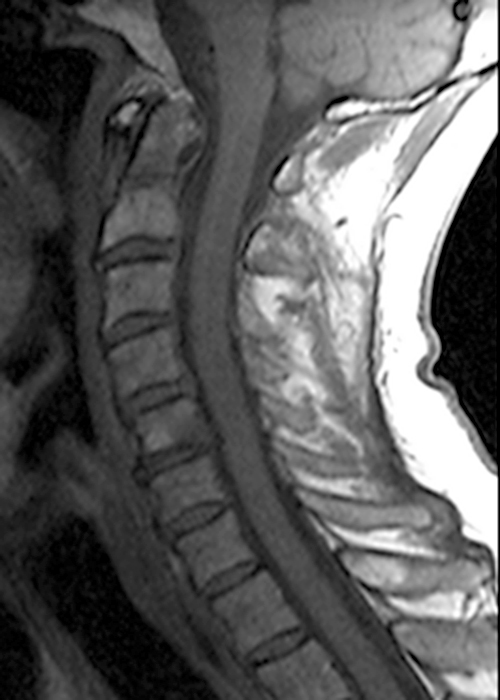
Clinical history: A 69-year-old male presents for MRI after he fell down a set of stairs one week prior. Sagittal T1- and T2-weighted images (1a,b) and a STIR sagittal image (1c) of the cervical spine are provided. What are the findings? What is your diagnosis?


Findings



Figure 2: Sagittal T-weighted (2A) and T2-weighted (2B) images of the cervical spine demonstrate linear horizontal low signal intensity (arrows) at the base of the odontoid process (dens), at the junction with the body of the C2 vertebra compatible with a non-displaced fracture. A sagittal STIR image (2C) of the cervical spine demonstrates marrow edema (short arrows) surrounding the fracture line and associated prevertebral soft tissue edema (arrowheads).
Diagnosis
Type 2 fracture of the odontoid process
Introduction
MRI is a valuable imaging modality for the diagnosis and evaluation of odontoid (dens) fractures due to its detailed visualization of bone marrow and assessment of supporting ligamentous structures. In addition, MRI provides insight into fracture classification and potential pathology of the cervical cord and craniocervical junction, thus aiding clinicians in assessing the neurological implications of injury and guiding conservative vs surgical management.
Anatomy
The atlantoaxial joint facilitates flexion and extension as well as axial rotational movements of the head. It is composed of two articulations: the median atlantoaxial joint and the lateral atlantoaxial joint. The median atlantoaxial joint is formed by the odontoid process of the axis (C2) and the anterior arch of the atlas (C1). The lateral atlantoaxial joint is formed by the inferior articular facets of the atlas and superior articular facets of the axis.1,2 The transverse ligament of the atlas (also known as the transverse atlantal ligament) is the strongest ligament in the spine (Figures 3 and 4).1 The transverse ligament extends posterior to the odontoid process and attaches to tubercles on the medial aspect of the lateral masses of the atlas.1 The transverse ligament prevents excessive anterior displacement of the odontoid relative to the anterior arch of C1. The cruciform (cruciate) ligament is composed of the transverse ligament and superior and inferior longitudinal bands/fibers (Figures 3 and 4) that allow for controlled rotational movements and promotes stability of the atlantoaxial joint, preventing excessive lateral motion of the atlas over the axis.3
The paired alar ligaments originate from the lateral margins of the odontoid process and attach to medial aspects of the occipital condyles (Figure 4).1 The alar ligaments limit axial rotation and contralateral flexion, and along with the transverse ligament, are a major stabilizer of the craniocervical junction.1
The tectorial membrane consists of superficial and deep layers and is a cephalad continuation of the posterior longitudinal ligament. Inferiorly, it extends from the body of the axis and superiorly, attaches to the clivus after passing through the foramen magnum.1 The tectorial membrane lies deep to the cruciform ligament and superficial to spinal dura mater (to which it is also closely apposed).4
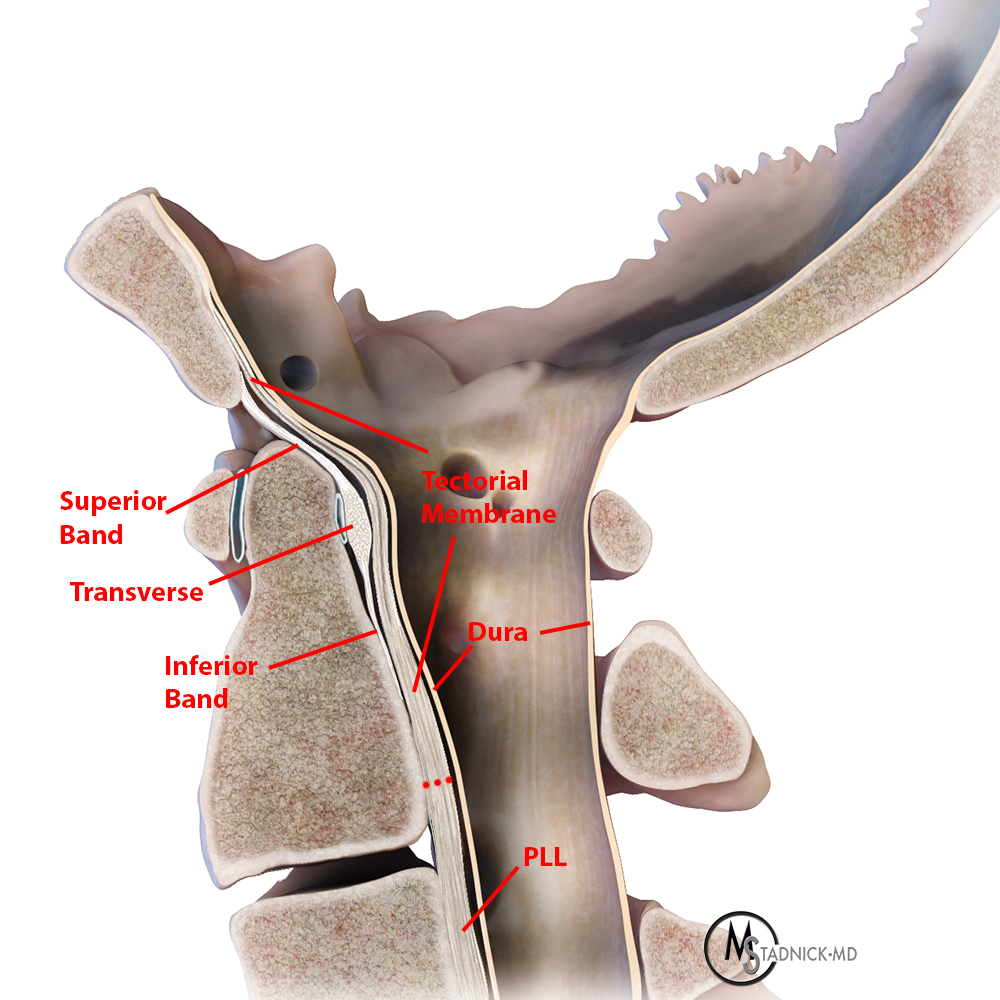
Figure 3: A lateral rendering of the craniocervical junction and atlantoaxial joint demonstrates key ligamentous structures including the transverse ligament posterior to the odontoid which is in continuity with superior and inferior longitudinal bands. The tectorial membrane extends from the body of C2 and is a continuation of the posterior longitudinal ligament (PLL).
Figure 4: To view the interactive series, depress the left mouse key and drag from right to left. The rendering progresses from a lateral to a posterior view of the craniocervical junction with removal of the posterior elements and dura. The tectorial membrane extends from the body of C2 to the clivus. Removal of the tectorial membrane reveals the cruciform ligament composed of the transverse ligament of the atlas and the superior and inferior longitudinal bands. The paired alar ligaments originate at the superior lateral aspect of the odontoid process and attach at the medial aspect of the occipital condyles.
Pathology and Treatment
Odontoid fractures are usually due to significant trauma, including falls (particularly in the elderly), motor vehicle accidents or high impact sports injuries. Odontoid process fractures are classified by location as Type I, Type II, and Type III (Anderson and D’Alonzo classification).5 Surgical management is based on the type of fracture, the degree of displacement, associated ligamentous injury, spinal cord compression, patient neurological deficits and general health of the patient.6
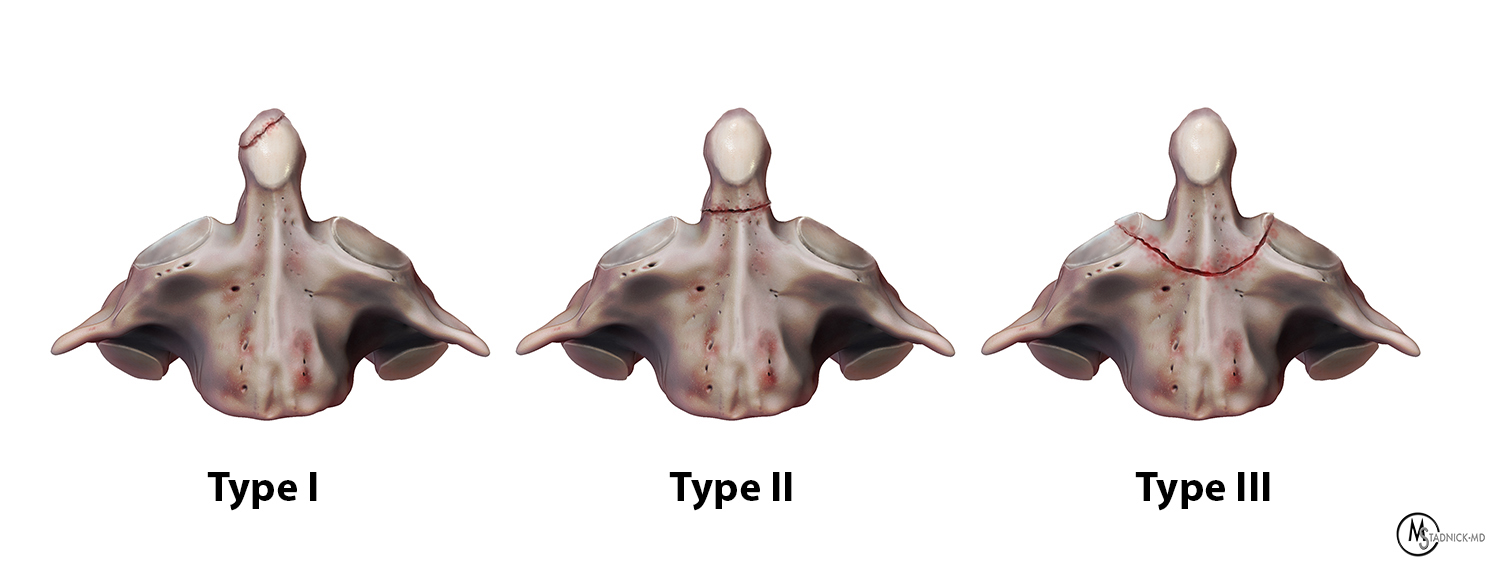
Figure 5: Fracture types according to the Anderson and D’Alonzo classification.
Type I fractures are avulsion fractures that extend through the apex of the odontoid process. Type I fractures are usually stable and are typically only minimally displaced. Therefore, they are most commonly conservatively managed with a cervical collar or halo vest.6
Type II fractures extend through the base of the odontoid process and are more commonly associated with instability and non-union (Figure 5). Type II fractures represent the most common type of odontoid fracture and have varying degrees of displacement and diastasis. Anterior screw fixation across the fracture site is more commonly employed for fractures with minimal displacement and comminution.6 Posterior fusion with screws, rods and bone grafts can be utilized to treat more complex Type II fractures to obtain stabilization (Figure 6).6,7 Occasionally, an os odontoideum can mimic a Type II odontoid fracture. In contrast to a Type II fracture, an os odontoideum has more well-circumscribed/smoother margins, a developmentally smaller odontoid process and is associated with a hypertrophied and rounded C1 anterior arch.8,9
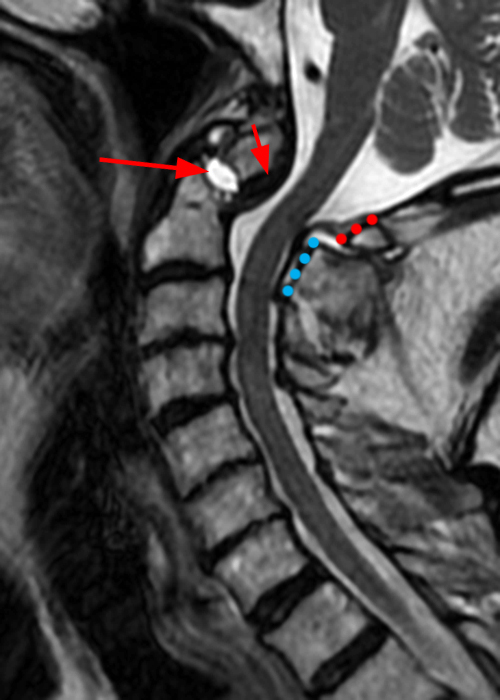
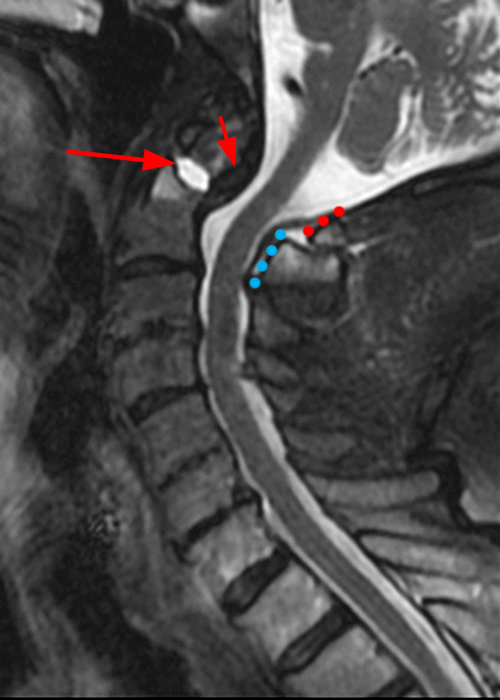
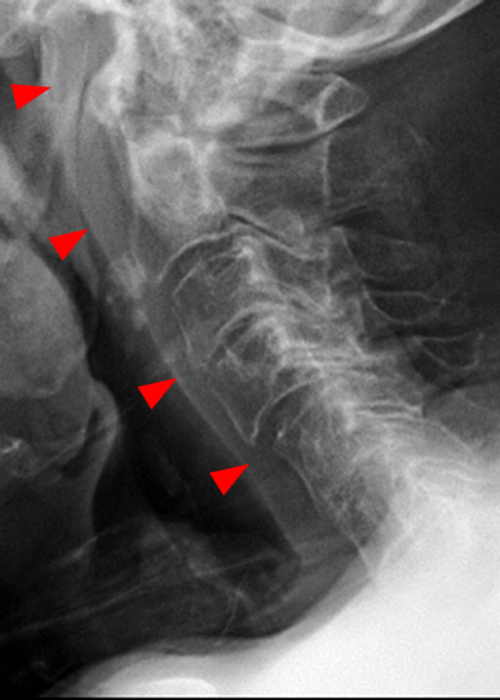

Figure 6: 84-year-old male with a history of a fall one month prior presents with headaches. Sagittal T2-weighted (6A) and STIR (6B) images show a subacute Type II odontoid fracture with posterior displacement and diastasis at the fracture site (arrows), thickening of the transverse ligament (short arrows) and posterior translation of the C1 posterior arch (red dotted line) relative to the posterior arch of C2 (blue dotted line). Pre- (6C) and post-operative (6D) x-radiographs demonstrate interval posterior instrumented fusion and reduction in the prevertebral soft tissue swelling present in 6C (arrowheads).
Type III odontoid fractures involve the body of the axis and demonstrate variable degrees of displacement (Figure 5). Surgery is associated with favorable outcomes in patients under the age of 70,10 whereas more conservative treatment with external mobilization is usually indicated in older patients.
In rare cases with significant displacement, cord compression and severe neurological deficits, a transoral odontoidectomy may be performed.11
Transverse ligament pathology can result in ligament disruption, or more commonly, ligament laxity. Trauma (especially C1 Jefferson fractures), degenerative changes, inflammatory arthropathies (including rheumatoid arthritis) and congenital predispositions (particularly Down Syndrome) can result in ligament laxity. Atlantoaxial instability, whether symptomatic or asymptomatic, is present in approximately 10-20% of patients with Down Syndrome (Figure 7).12 Injury to the transverse ligament can result in cord compression and severe neurological deficits, including paralysis. Treatment of transverse ligament injury is targeted at stabilizing the atlantoaxial joint. Posttraumatic disruption of the substance of the transverse ligament is treated with early internal fixation whereas fractures or avulsions at the C1 lateral mass insertion tend to heal with immobilization/rigid cervical orthosis.13
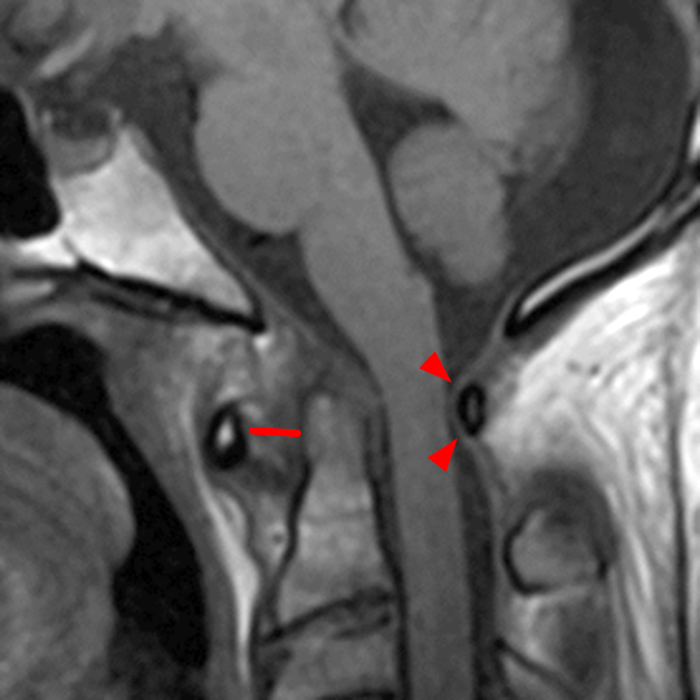
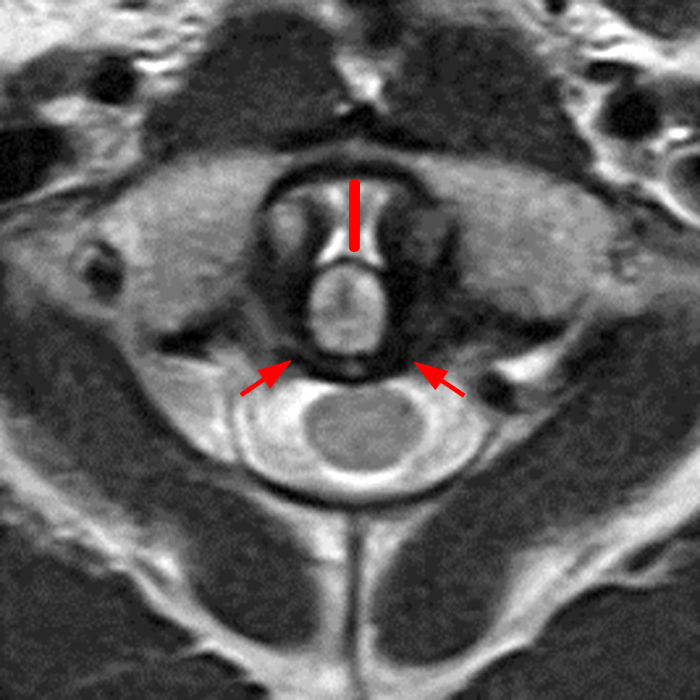
Figure 7: 15-year-old male with a history of Down Syndrome presents with seizures. Sagittal T1-weighted (7A) and axial T2-weighted (7B) images demonstrate an increased atlantodental interval to 7 mm (lines) associated with laxity of the transverse ligament (short arrows). Anterior subluxation of the C1 arch results in mild spinal canal stenosis with indentation of the thecal sac (arrowheads).
Conclusion
MRI plays an integral role in the evaluation of odontoid fractures and associated soft tissue injuries. The ability of MRI to identify transverse ligament injury makes it an invaluable tool to evaluate associated atlantoaxial instability and potential cervical cord pathology. The diagnostic accuracy of MRI makes it an invaluable tool to guide treatment decisions and improve patient outcomes.
References
- Offiah CE, Day E. The craniocervical junction: embryology, anatomy, biomechanics and imaging in blunt trauma. Insights into imaging. 8 (1): 29-47. doi:10.1007/s13244-016-0530-5. ↩
- Jarvis M, Yap J, Hacking C, et al. Atlanto-axial articulation. Reference article, Radiopaedia.org (Accessed on 16 Sep 2023) https://doi.org/10.53347/rID-35480. ↩
- Wong A, Knipe H, Bell D, et al. Cruciate ligament of the atlas. Reference article, Radiopaedia.org (Accessed on 16 Sep 2023) https://doi.org/10.53347/rID-36585. ↩
- Wong A, El-Feky M, Hacking C, et al. Tectorial membrane of the spine. Reference article, Radiopaedia.org (Accessed on 16 Sep 2023) https://doi.org/10.53347/rID-36587. ↩
- Hsu WK, Anderson PA. Odontoid fractures: update on management. J Am Acad Orthop Surg. 2010 Jul;18(7):383-94. doi: 10.5435/00124635-201007000-00001. ↩
- Gonschorek O, Vordemvenne T, Blattert T, Katscher S, Schnake KJ; Spine Section of the German Society for Orthopaedics and Trauma. Treatment of Odontoid Fractures: Recommendations of the Spine Section of the German Society for Orthopaedics and Trauma (DGOU). Global Spine J. 2018 Sep;8(2 Suppl):12S-17S. doi: 10.1177/2192568218768227. ↩
- Elgafy H, Dvorak MF, Vaccaro AR, Ebraheim N. Treatment of displaced type II odontoid fractures in elderly patients. Am J Orthop. Belle Mead NJ0029. 2009;38:410–416. ↩
- Gaillard F, Leong Y, El-Feky M, et al. Os odontoideum. Reference article, Radiopaedia.org (Accessed on 17 Sep 2023) https://doi.org/10.53347/rID-1784 ↩
- Smoker WR. Craniovertebral junction: normal anatomy, craniometry, and congenital anomalies. Radiographics. 1994;14 (2): 255-77. doi:10.1148/radiographics.14.2.8190952 ↩
- Fan, Lei MDa; Ou, Dingqiang MDb; Huang, Xuna MDc; Pang, Mao MDa; Chen, Xiu-Xing MDd; Yang, Bu MDa; Wang, Qi-You MDa,∗. Surgery vs conservative treatment for type II and III odontoid fractures in a geriatric population: A meta-analysis. Medicine 98(44):p e10281, November 2019. doi: 10.1097/MD.0000000000010281. ↩
- Elbadrawi AM, Elkhateeb TM. Transoral Approach for Odontoidectomy Efficacy and Safety. HSS J. 2017 Oct;13(3):276-281. doi: 10.1007/s11420-016-9535-3. ↩
- Ali FE, Al-Bustan MA, Al-Busairi WA, Al-Mulla FA, Esbaita EY. Cervical spine abnormalities associated with Down syndrome. Int Orthop. 2006 Aug;30(4):284-9. doi: 10.1007/s00264-005-0070-y. ↩
- Dickman CA, Greene KA, Sonntag VK. Injuries involving the transverse atlantal ligament: classification and treatment guidelines based upon experience with 39 injuries. Neurosurgery. 1996 Jan;38(1):44-50. doi: 10.1097/00006123-199601000-00012. ↩
