Clinical History: A 35 year-old man sustained a hyperextension injury to his right knee while playing football. (1a,1b) Sagittal proton-density and (1c) coronal fat-suppressed T2-weighted images from the MR examination are provided. What are the findings? What is your diagnosis?

1a

1b

1c
Figure 1:
(1a,1b) Sagittal proton-density and (1c) coronal fat-suppressed T2-weighted images.
Findings

2a
Figure 2:
A sagittal proton density-weighted image demonstrates a complete proximal tear of the anterior cruciate ligament (arrow).

3a
Figure 3:
An additional sagittal proton density-weighted image demonstrates elongation and altered signal intensity of the posterior cruciate ligament consistent with high-grade partial-thickness intrasubstance tearing (red arrow). A nondisplaced tibial intercondylar eminence fracture (yellow arrow) and a joint effusion are also seen.

4a
Figure 4:
The coronal fat-suppressed T2-weighted image demonstrates complete tearing of the distal biceps femoris tendon with retraction to the joint line (arrow).
Diagnosis
Multi-ligamentous and tendon injury suggesting knee dislocation.
Discussion
Additional fat-suppressed T2-weighted coronal images from the above case:

5a
Figure 5:
A fat-suppressed T2-weighted coronal image demonstrates high-grade partial-thickness intrasubstance tearing of the proximal portion of the tibial collateral ligament (red arrow). Marrow edema is present in the medial femoral condyle (blue arrow) and medial tibial plateau, extending into the medial tubercle of the intercondylar eminence (yellow arrow). Extensive edema is present in the surrounding soft tissues.

6a
Figure 6:
A more posterior coronal view reveals a complete tear of the popliteus tendon near the popliteal sulcus (arrow). The fibular collateral ligament is not visualized, a finding that is consistent with a complete tear of this structure as well.
In the medical literature, the term “knee dislocation” is commonly used to describe a knee either with multiple injured ligaments or with multi-directional instability, findings that can result from either knee subluxation or a complete knee dislocation1. Although knee dislocations are rare, their true prevalence is unknown because of missed diagnoses or misdiagnosis. The prevalence has been reported to be as high as 0.11% in one series that reviewed over 17,000 consecutive knee MRI examinations2. Most commonly knee dislocations are associated with high-velocity trauma related to motor vehicle accidents1; however, in some reports low-velocity injuries from sports activities have been the predominate cause of knee dislocation2,3.
Evaluation of the remainder of the images in this case also demonstrated disruption of the peroneal nerve (surgically proven) and intact popliteal vessels. Given the involvement of all four major ligamentous complexes, the findings are consistent with a recent knee dislocation.
Classification
The most commonly utilized classification system to describe knee dislocations is based on the direction of displacement of the tibia relative to the femur: anterior (7a,8a), posterior, lateral, medial, or rotatory4. In most reported series, anterior dislocations are the most common followed by posterior dislocations1,4,5. Anterior knee dislocations are most frequently due to hyperextension, which first tears the posterior joint capsule and then the anterior and posterior cruciate ligaments 4,6. Posterior knee dislocations require considerably more force compared with anterior dislocations, can occur from crushing injuries to the leg, and most commonly occur with disruption of both cruciate ligaments4. Lateral and medial knee dislocations are far less common than anterior and posterior dislocations, can be seen with motor vehicle accidents4, and are invariably associated with damage to the collateral ligaments7. Rotatory knee dislocations are historically considered one of the more rare forms5 with numerous subdivisions1.

7a
Figure 7:
24 year old man with spontaneously reduced anterior knee dislocation. A T1-weighted sagittal image demonstrate complete disruption of the ACL (arrow).

8a
Figure 8:
An adjacent sagittal images reveals complete disruption of the PCL as well (red arrow). A displaced meniscal fragment from a bucket handle tear of the medial meniscus (blue arrow) is also present, creating the so-called "double PCL" sign.
Imaging Findings
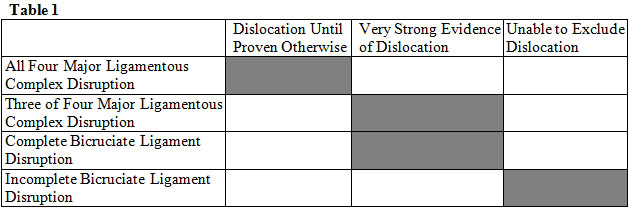
The MR findings associated with knee dislocations are often profound with high-grade injuries of multiple ligaments and other supporting structures (9a,10a). The specific pattern of ligamentous disruption is influenced but not dictated by the direction of dislocation; however, the diagnosis of a knee dislocation and certainly its direction may not be evident at the time of examination8. Therefore, the radiologist must remain alert for this entity and based on the findings suggest the diagnosis. Involvement of both cruciate ligaments and one or both of the collateral ligamentous complexes is common9. Bicruciate ligament injury alone is very strong evidence for a prior knee dislocation10. Less commonly, knee dislocations have been described with sparing of the PCL11,12 and ACL6. Based on previous descriptions of prior knee dislocations, the following principles can be outlined13, as summarized in Table 1.

9a
Figure 9:
46 year old female with rotatory type knee dislocation. A coronal T2-weighted fat suppressed image demonstrates a retracted fibular head avulsion fracture (arrow), the so-called "arcuate sign".

10a
Figure 10:
The avulsion fracture of the fibular head is confirmed on the corresponding plain radiograph.
Associated Complications
Traumatic knee dislocations are devastating injuries and even cases with spontaneous or easy reduction demonstrate the same frequency and extent of complications such as vascular injury14 (11a,12a). Due to the relatively fixed position of the popliteal artery between its origin at the hiatus of the adductor magnus muscle and its termination as it passes beneath the tendinous arch of the soleus muscle, this artery is prone to injury, a complication that is seen in approximately one-third of knee dislocations4,5,15. If this vascular injury is not emergently corrected, amputation is often required with reported rates as high as 86% at 8 hours5. The peroneal nerve is also prone to injury, a complication that occurs in approximately one-third of patients (13a,14a)16. Injury to the popliteus tendon denotes a more severe mechanism of injury and may be predictive of injury to the peroneal nerve9.

11a
Figure 11:
A lateral radiograph demonstrates an non-reduced anterior dislocation of the knee.

12a
Figure 12:
An image from a conventional angiogram on the same patient after reduction demonstrates occlusion of the popliteal artery at the joint line (arrow).

13a
Figure 13:
A 53 year old man who was hit by a truck with reduced rotatory type knee dislocation and clinical findings of peroneal neuropathy. MR images (not shown) revealed complete tears of the ACL and the fibular collateral ligament. An axial fat suppressed proton-density weighted image demonstrates increased signal within and edema surrounding the peroneal nerve (arrow).

14a
Figure 14:
A corresponding coronal T2 fat suppressed T2-weighted image confirms increased peroneal intraneural signal and perineural edema at the level of the joint line over a length of approximately 2.5 cm (arrow), consistent with the clinical findings of peroneal neuropathy.
Treatment
Years ago, non-operative treatment with prolonged immobilization was the standard treatment for knee dislocation17. With modern surgical techniques, early repair often utilizing multi-ligamentous reconstruction and aggressive physical therapy has resulted in more favorable outcomes17. When present, vascular or neural injuries often require the most expeditious treatment, after which ligamentous injuries may be addressed. Prior to surgery MRI allows accurate characterization of the extent of injuries to supporting structures of the knee, as well as identification of meniscal tears which may require partial meniscectomy or repair. MR thus provides a valuable roadmap towards determining the appropriate surgical approach.
Conclusion
Knee dislocation commonly involves injuries to many of the soft-tissue stabilizing structures of the knee. Reduction may occur prior to imaging and the radiologist must remain vigilant to this diagnosis and to the potential for devastating associated complications that may occur with this entity.
References
1 Brautigan, B. and D.L. Johnson, The epidemiology of knee dislocations. Clin Sports Med, 2000. 19(3): p. 387-97.
2 Bui, K.L., et al., Knee dislocations: a magnetic resonance imaging study correlated with clinical and operative findings. Skeletal Radiol, 2008. 37(7): p. 653-61.
3 Shelbourne, K.D., M.S. Haro, and T. Gray, Knee dislocation with lateral side injury: results of an en masse surgical repair technique of the lateral side. Am J Sports Med, 2007. 35(7): p. 1105-16.
4 Kennedy, J.C., Complete Dislocation of the Knee Joint. J Bone Joint Surg Am, 1963. 45: p. 889-904.
5 Green, N.E. and B.L. Allen, Vascular injuries associated with dislocation of the knee. J Bone Joint Surg Am, 1977. 59(2): p. 236-9.
6 Bratt, H.D. and A.P. Newman, Complete dislocation of the knee without disruption of both cruciate ligaments. J Trauma, 1993. 34(3): p. 383-9.
7 Mills, W.J. and R.J. Nowinski, Dislocation of the knee with lateral dislocation of the patella. A report of four cases. J Bone Joint Surg Br, 2001. 83(4): p. 530-2.
8 Walls, R.M. and P. Rosen, Traumatic dislocation of the knee. J Emerg Med, 1984. 1(6): p. 527-31.
9 Yu, J.S., et al., Complete dislocation of the knee: spectrum of associated soft-tissue injuries depicted by MR imaging. AJR Am J Roentgenol, 1995. 164(1): p. 135-9.
10 Wascher, D.C., P.C. Dvirnak, and T.A. DeCoster, Knee dislocation: initial assessment and implications for treatment. J Orthop Trauma, 1997. 11(7): p. 525-9.
11 Cooper, D.E., et al., Complete knee dislocation without posterior cruciate ligament disruption. A report of four cases and review of the literature. Clin Orthop Relat Res, 1992(284): p. 228-33.
12 Toritsuka, Y., S. Horibe, and A. Hiro-oka, Knee dislocation following anterior cruciate ligament disruption without any other ligament tears. Arthroscopy, 1999. 15(5): p. 522-6.
13 Resnick, D., H.S. Kang, and M.L. Pretterklieber, Internal derangements of joints. 2nd ed2007, Philadelphia, Pa.: Saunders/Elsevier.
14 Varnell, R.M., et al., Arterial injury complicating knee disruption. Third place winner: Conrad Jobst award. Am Surg, 1989. 55(12): p. 699-704.
15 Reckling, F.W. and L.F. Peltier, Acute knee dislocations and their complications. 1969. Clin Orthop Relat Res, 2004(422): p. 135-41.
16 Meyers, M.H. and J.P. Harvey, Jr., Traumatic dislocation of the knee joint. A study of eighteen cases. J Bone Joint Surg Am, 1971. 53(1): p. 16-29.
17 Taylor, A.R., G.P. Arden, and H.A. Rainey, Traumatic dislocation of the knee. A report of forty-three cases with special reference to conservative treatment. J Bone Joint Surg Br, 1972. 54(1): p. 96-102.
