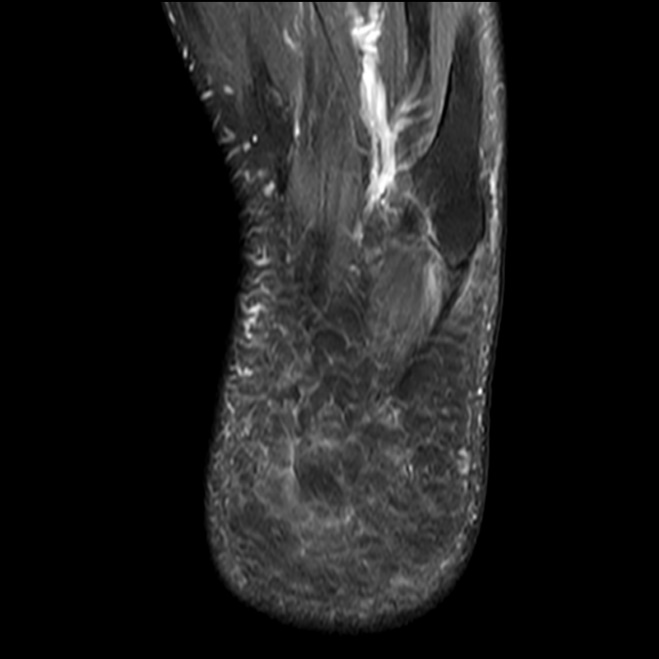
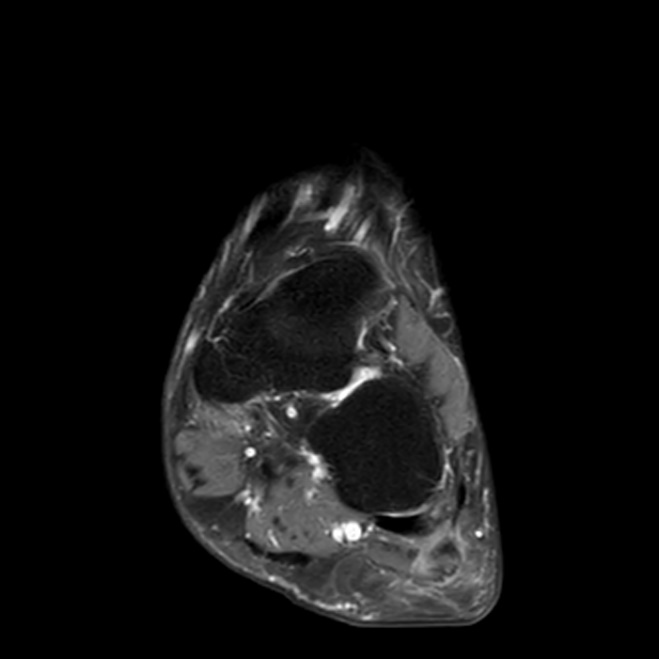
Clinical History: A 69-year-old female presents with a several year history of progressive lateral midfoot pain. There is a clinical concern for peroneal tendon tear. Fat-suppressed T2-weighted axial (1A), T1-weighted sagittal (1B) and fat-suppressed proton density-weighted coronal (1C) images are provided. What are the findings? What is your diagnosis?

Findings
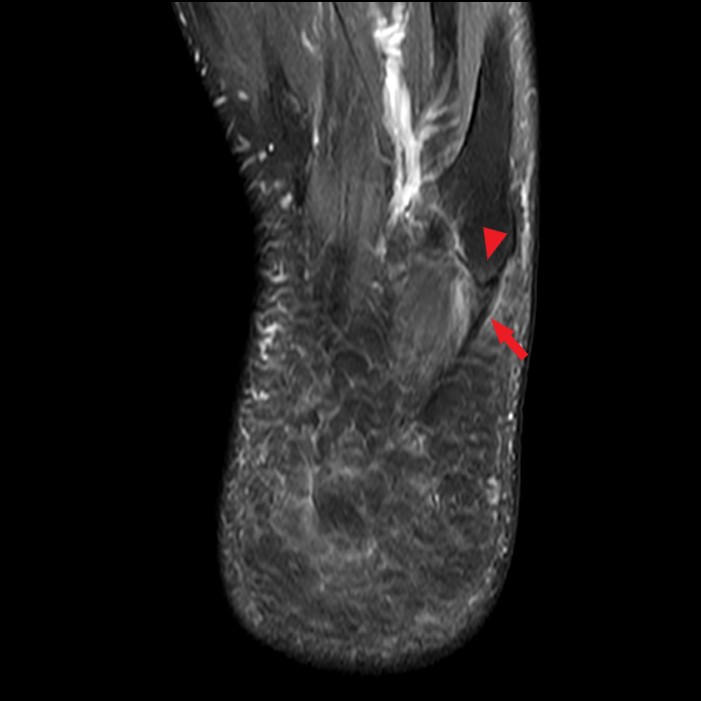

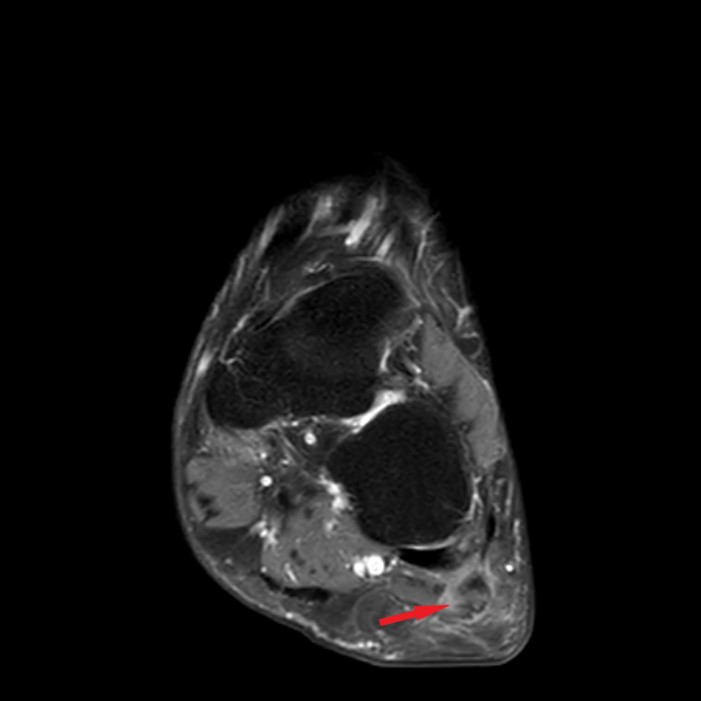
Figure 2: Moderate thickening and edema along the distal lateral cord of the plantar aponeurosis (arrow) with mild insertional bone marrow edema at the fifth metacarpal base attachment (arrowhead) is present on the axial fat-suppressed T2-weighted image (2A). Sagittal T1-weighted image (2B) demonstrates intermediate signal thickening of the distal lateral cord (arrow) with a small enthesophyte at the fifth metatarsal base attachment (arrowhead). The coronal fat-suppressed proton density-weighted image (2C) also shows the thickened lateral cord with a partial thickness intrasubstance tear (arrow).
Diagnosis
Insertional Lateral Cord Plantar Fasciopathy
Introduction
Chronic foot pain is a common and often disabling condition with approximately 40 percent of adults in the United States experiencing foot problems.1 Accurate diagnosis is often difficult because of the broad spectrum of potential causes. Lateral cord insertional fasciopathy is a less commonly discussed etiology of lateral midfoot pain both in clinical and imaging literature. More commonly questioned causes of lateral midfoot pain include fractures of the fifth metatarsal base or cuboid, painful os peroneum syndrome, peroneal tendon pathology, Baxter’s nerve impingement or abductor digiti minimi strain. Misdiagnosis can lead to improper treatment which may result in prolonged and worsening pain.
Plantar fasciitis is a common cause of plantar heel pain and most commonly involves the proximal third of the central cord near the calcaneal attachment.2

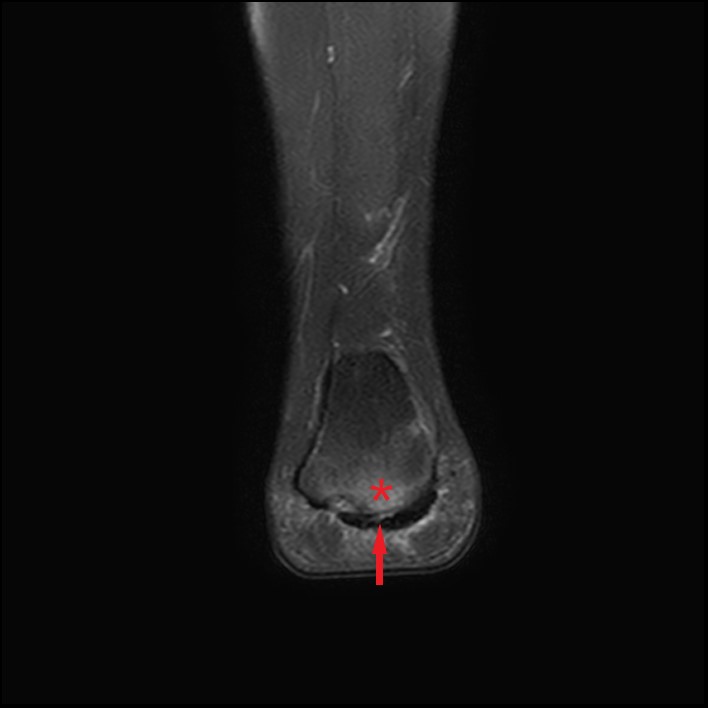
Figure 3: Sagittal (3A) and Coronal (3B) STIR images of the ankle in a 30-year-old female with acute on chronic heel pain. Edematous medial calcaneal tuberosity (asterisks) with adjacent thickening, edema, and partial tearing of the proximal central and lateral cords of the plantar aponeurosis (arrows).
Plantar fasciitis is usually the result of repetitive microtrauma, specifically, prolonged pronation stresses, inducing microtears and eliciting a low-grade inflammatory process. Plantar fasciitis can be seen in athletes, obese patients, or those with work requiring prolonged standing or walking. Alternatively, plantar fasciitis can also be seen as an enthesopathy associated with spondyloarthropathies such as ankylosing spondylitis, psoriatic arthritis, or Reiter’s syndrome.3 The same pathologic process may occur at the insertion of the lateral cord of the plantar aponeurosis at the base of the fifth metatarsal with resultant lateral midfoot pain. Patients with a cavovarus foot are predisposed to excessive supination forces that may increase stress at the fifth metatarsal base and cause lateral cord fasciitis.4
Lateral cord insertional fasciopathy more commonly affects women and obesity is a common underlying factor.5 Affected individuals often report pain that is typically worse after rest, similar to the pain reported for the more common central cord plantar fasciitis at the calcaneal origin. On physical examination, patients usually have pain on direct palpation at the plantar lateral aspect of the fifth metatarsal base. In contrast to peroneus brevis tears, patient’s typically do not have pain with resisted eversion testing.4
Anatomy
The plantar aponeurosis, or plantar fascia, is the most important structure for dynamic longitudinal arch support in the foot.6 The aponeurosis is a sophisticated combination of collagen and elastic fibers creating a strong tendinous layer at the plantar aspect of the foot.7 The fibrous aponeurosis arises from the medial calcaneal tuberosity and divides into central, medial, and lateral components. The thickest central cord extends distally, covering the plantar surface of the flexor digitorum muscle, before dividing into five digitations inserting at the metatarsophalangeal joint capsules. The lateral cord partially blends with the abductor digiti minimi proximally and splits into a smaller medial crux and a larger lateral crux as it courses to the fifth metatarsal base. The medial crux terminates in the plantar forefoot where it blends with the third and fourth metatarsophalangeal joint plantar plates and gives rise to a portion of the transverse component of the abductor hallucis muscle.8 The lateral crux is larger and courses along the plantar lateral aspect of the abductor digiti minimi, finally broadening and inserting along the plantar lateral aspect of the fifth metatarsal tuberosity. The insertion is separate from that of the peroneus brevis tendon which inserts a mean of 5.4 mm dorsal to the lateral cord of the plantar fascia according to a cadaveric study performed by Devries et al.9
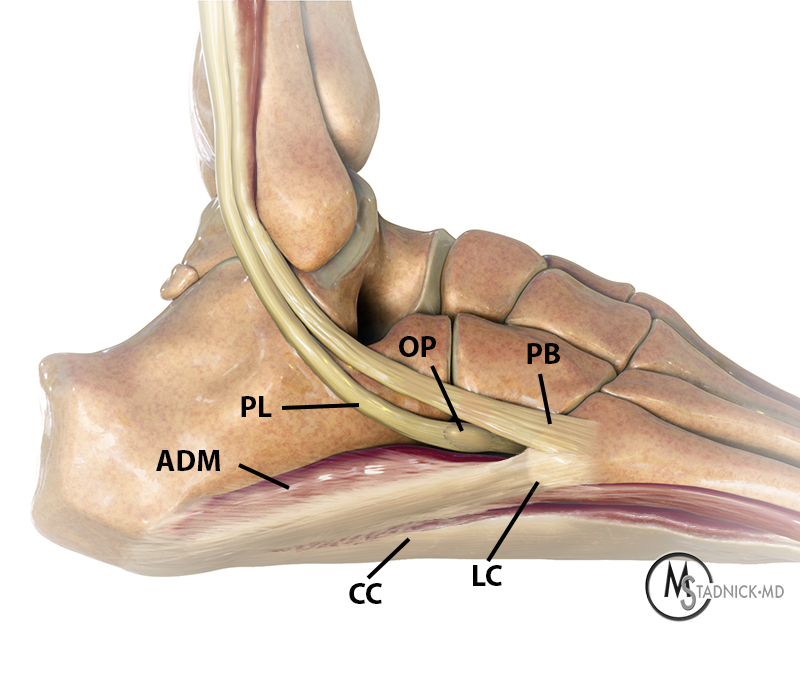
Figure 4: A lateral view of the foot demonstrates the insertion of the lateral cord (LC) of the plantar aponeurosis along the lateral aspect of the base of the fifth metatarsal and the peroneus brevis (PB) attaching more dorsally. Additional pertinent anatomy includes the abductor digiti minimi (ADM), the peroneus longus (PL) containing the os peroneum (OP), and the central cord (CC) of the plantar aponeurosis.
MRI Findings of Lateral Cord Insertional Fasciopathy
Normal MRI appearance of the lateral cord of the plantar fascia insertion includes uniform dark signal on T2-weighted sequences, smooth contour as it fans out to attach to the metatarsal base, no intra- or perifascial edema, and lack of insertional enthesophyte or bone marrow edema at the base of the fifth metatarsal.
Figure 5: Sequential fat-suppressed proton density-weighted coronal images beginning at the level of the calcaneal tuberosity demonstrate the normal relationship of the medial (green), central (red), and lateral (yellow) cords of the plantar aponeurosis. Notice the relationship of the lateral cord with the adjacent abductor digiti minimi muscle (asterisk). Note the normal broadening of the hypointense lateral crux of the lateral cord near its insertion on the plantar lateral fifth metatarsal base and the separate attachment of the peroneus brevis tendon (arrow) dorsal and just distal to the lateral cord insertion.
MRI findings of lateral cord insertional fasciitis are identical to those seen in the more common proximal central cord plantar fasciitis. Plantar fascial thickening, intrafascial edema and surrounding soft tissue edema on T2-weighted sequences are present. Insertional bone marrow edema and an enthesophyte may be present at the plantar lateral aspect of the fifth metatarsal base. In more severe cases, the lateral cord of the plantar aponeurosis may be torn near the fifth metatarsal base.
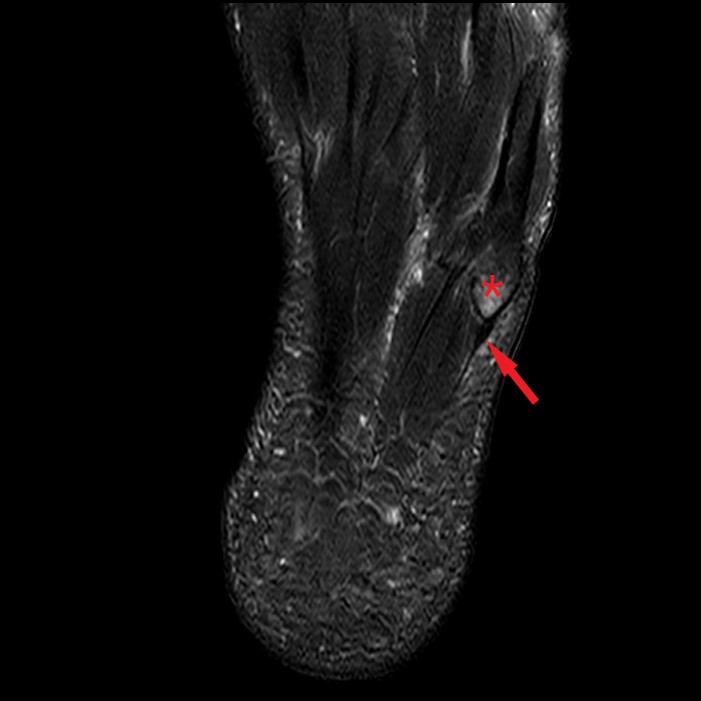
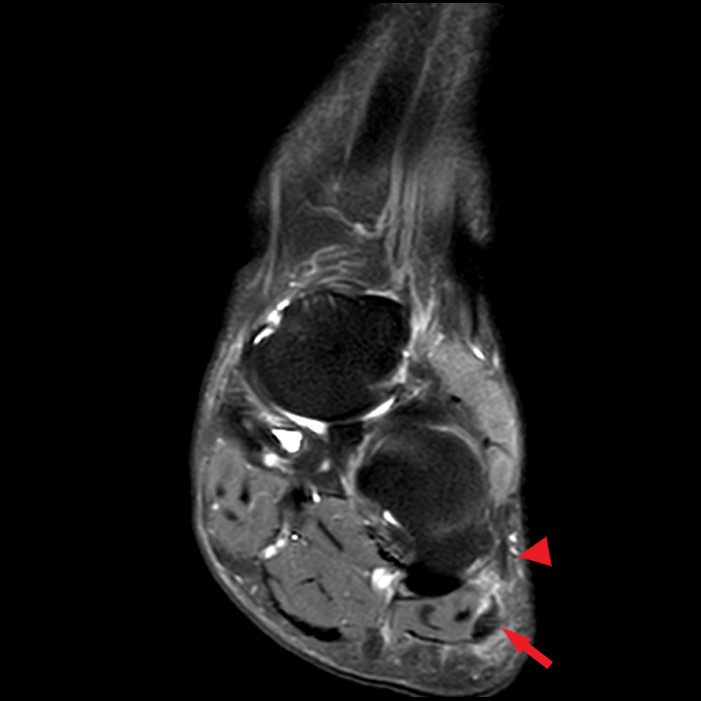
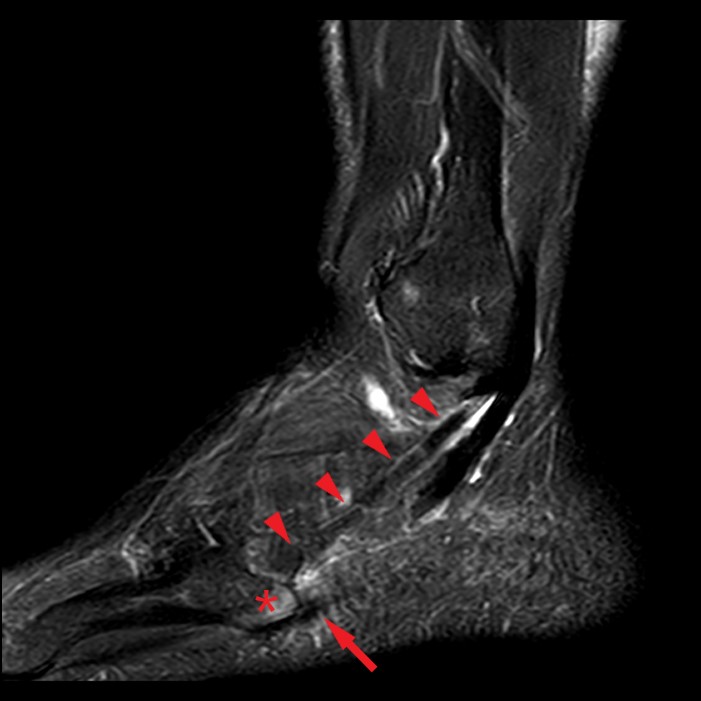
Figure 6: Fat-suppressed T2-weighted axial (6A), coronal fat-suppressed proton density-weighted (6B), and sagittal fat-suppressed T2-weighted (6C) images in another 51-year-old male with acute on chronic midfoot pain near the cuboid tunnel. Moderate thickening and edema along the distal lateral cord of the plantar aponeurosis (arrows) with mild insertional bone marrow edema at the fifth metacarpal base attachment (asterisks) is present on the fat-suppressed T2-weighted images.
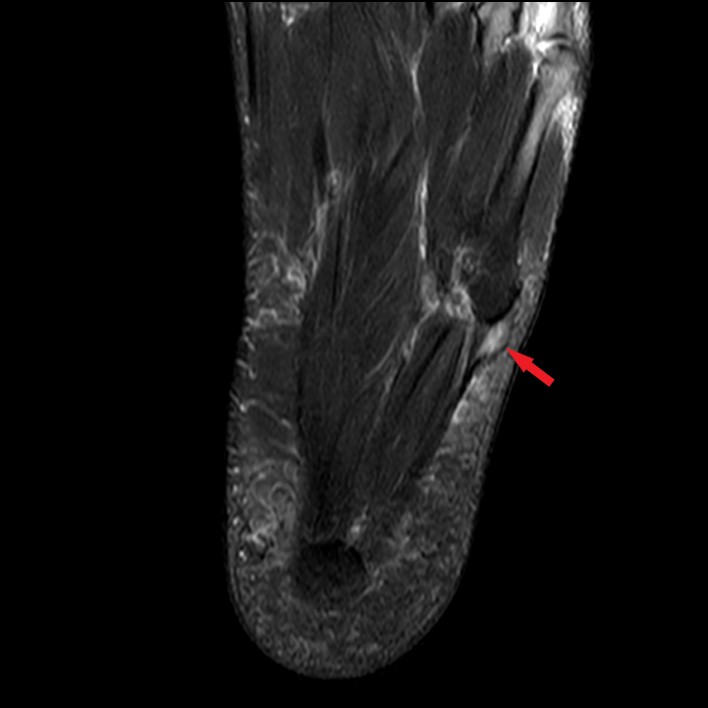
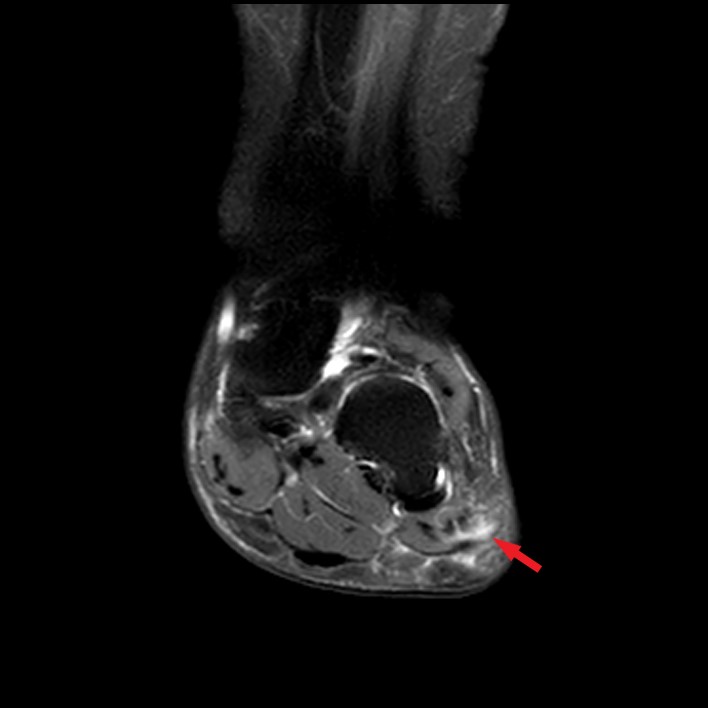
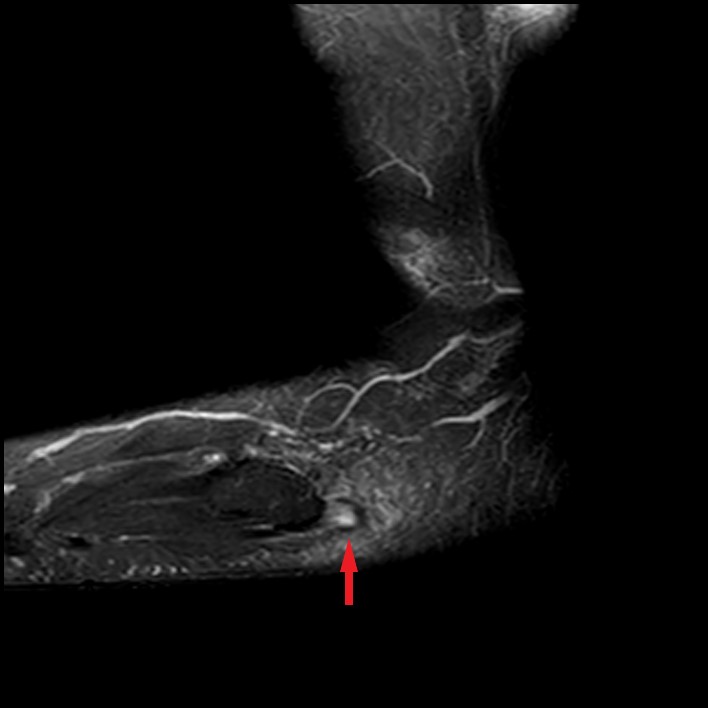
Figure 7: STIR images in the axial fat-suppressed T2-weighted (7A), coronal fat-suppressed proton density-weighted (7B), and sagittal fat-suppressed T2-weighted (7C) images in a 55-year-old female with lateral midfoot pain after recent injury 8 weeks ago with concern for peroneal tendon tear. Moderate thickening and edema along the distal lateral cord of the plantar aponeurosis with a partial tear involving the lateral half of the distal lateral cord at the fifth metatarsal base insertion (arrows).
Differential Diagnosis of Lateral Midfoot Pain
Ordering physicians often query many different causes of lateral midfoot pain and rarely list lateral cord fasciopathy as a potential cause, not unexpected given the relative lack of discussion of this pathology in both orthopaedic and radiology literature. A retrospective study by Newman et al. found that out of 20 patients referred for evaluation of lateral foot pain, the most common suspected diagnoses were fractures of the fifth metatarsal base, cuboid, or anterior calcaneus, painful os peroneum syndrome (POPS), and peroneal tendon tendinosis or tear5. Baxter’s nerve (first branch of the lateral plantar nerve) impingement or an abductor digiti minimi strain may also be considered as potential etiologies given the proximity of the muscle to the lateral cord of the plantar aponeurosis.
Stress injuries are a common cause of foot pain in athletes. Stress injuries of the calcaneus, cuboid, fourth or fifth metatarsal bases cause lateral midfoot pain which may mimic peroneal tendon pathology or lateral cord plantar fasciopathy.
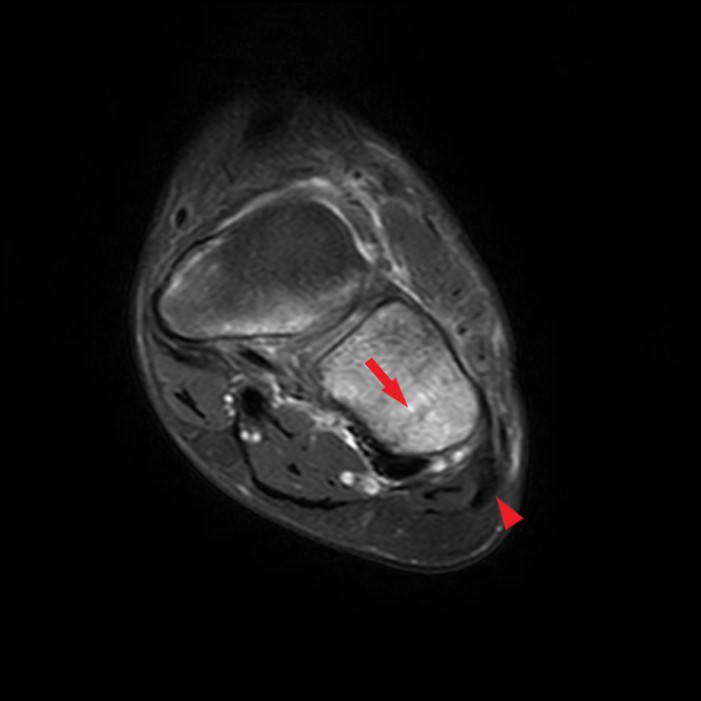


Figure 8: Coronal fat-suppressed T2-weighted image (8A), sagittal (8B) and axial (8C) T1-weighted images in 11-year-old male with 3-week history of lateral midfoot pain. Fracture line noted in the lateral aspect of the cuboid on the T2 and T1-weighted images (arrows) with surrounding marrow edema. Note the proximity of the cuboid fracture to the lateral cord of the plantar fascia located just plantar and lateral to the cuboid (arrowheads).
Fractures of the base of the fifth metatarsal are among the most common skeletal injuries of the foot and can be categorized into stress fractures of the proximal diaphysis, Jones fracture, and avulsion fractures of the metatarsal tuberosity with two thirds of all fifth metatarsal fractures being avulsion fractures.10 There has been much debate as to the exact cause of proximal fifth metatarsal fractures. A cadaveric study by DeVries et al. determined that avulsion fractures are most commonly the result of traction by the lateral cord of the plantar aponeurosis due to inversion and plantar flexion of the forefoot9 rather than a result of traction by the peroneus brevis tendon as previously thought.11 He et al. used a combination of 3D fracture mapping and cadaveric specimens to conclude that both the lateral band of the plantar fascia and peroneus brevis play a major role, either separately or together, in avulsion fractures of the fifth metatarsal base and proposed a novel classification for such fractures based on the fracture pattern and location of the fracture.10



Figure 9: Sagittal T1-weighted (9A), fat-suppressed T2-weighted (9B) images and axial T1-weighted (9C) images of the ankle in a 48-year-old male with 1 month history of pain localized to the base of the fifth metatarsal. A transverse fracture (arrows) is noted through the fifth metatarsal tuberosity with surrounding bone marrow edema. Note the location of the insertion of the lateral cord of the plantar fascia on the plantar lateral aspect of the tuberosity (arrowheads).

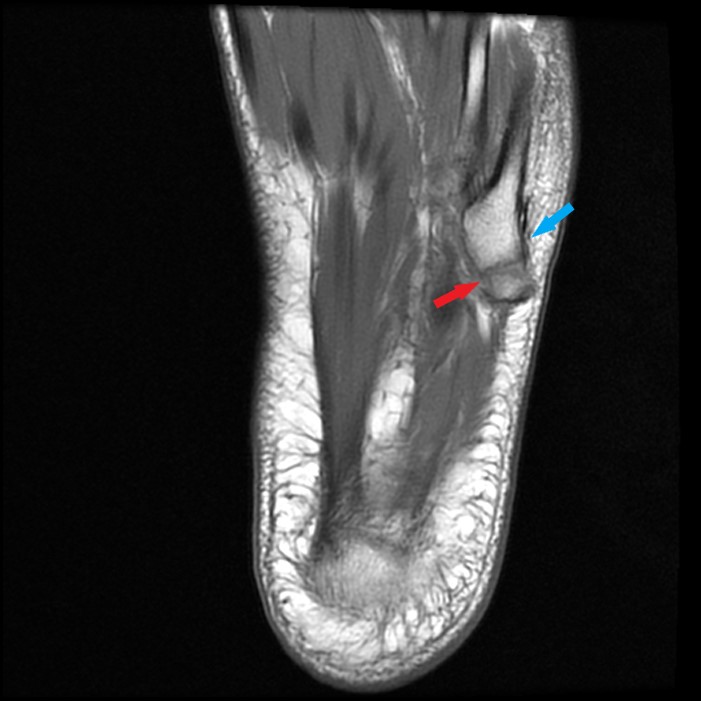
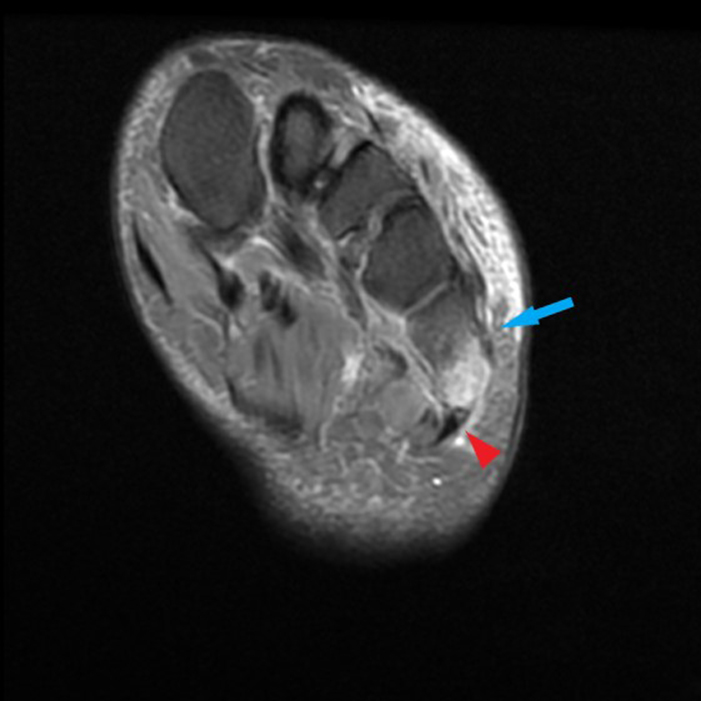
Figure 10: Sagittal (10A) and axial (10B) T1-weighted images in another 61-year-old female with lateral midfoot pain demonstrates a mildly displaced avulsion fracture of the fifth metatarsal base tuberosity (arrows). Oblique coronal fat-suppressed proton density-weighted image (10C) demonstrates bone marrow edema associated with the fracture and the adjacent insertion of the lateral cord of the plantar fascia (arrowhead). Note the peroneus brevis insertion spans the fracture (blue arrow) and thus is unlikely to be the primary contributing factor to the avulsion fracture.
An os vesalianum pedis is an uncommon accessory ossicle that resides adjacent to the fifth metatarsal base and involves the insertion of the peroneus brevis tendon. It may be mistaken for an acute or chronic avulsion fracture, apophysitis, or chronically ununited apophysis. An os vesalianum is typically rounded or triangular12, whereas an unfused apophysis is usually ovoid and oriented with its long axis parallel to the long axis for the fifth metatarsal shaft.13 Painful os vesalianum is relatively uncommon cause of foot pain. MRI will show stress related changes at the synchondrosis with the parent bone.
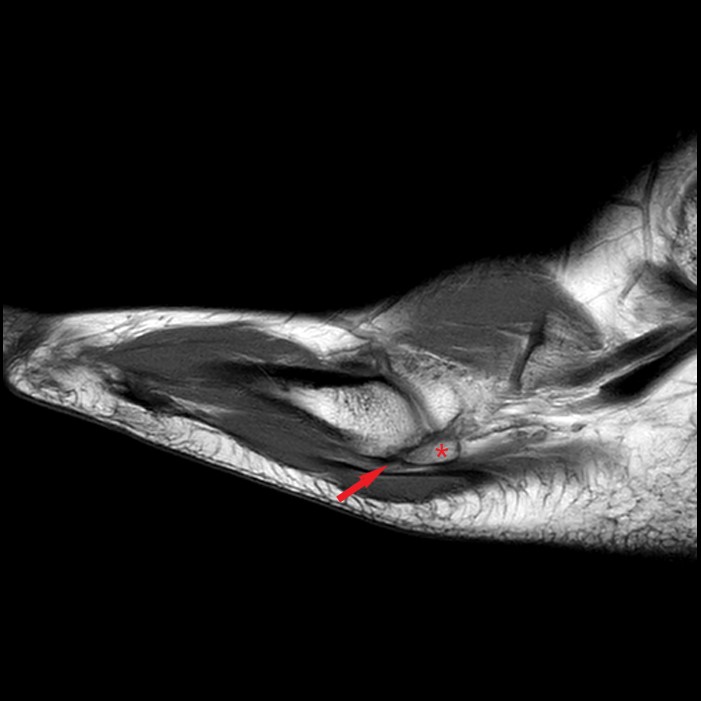
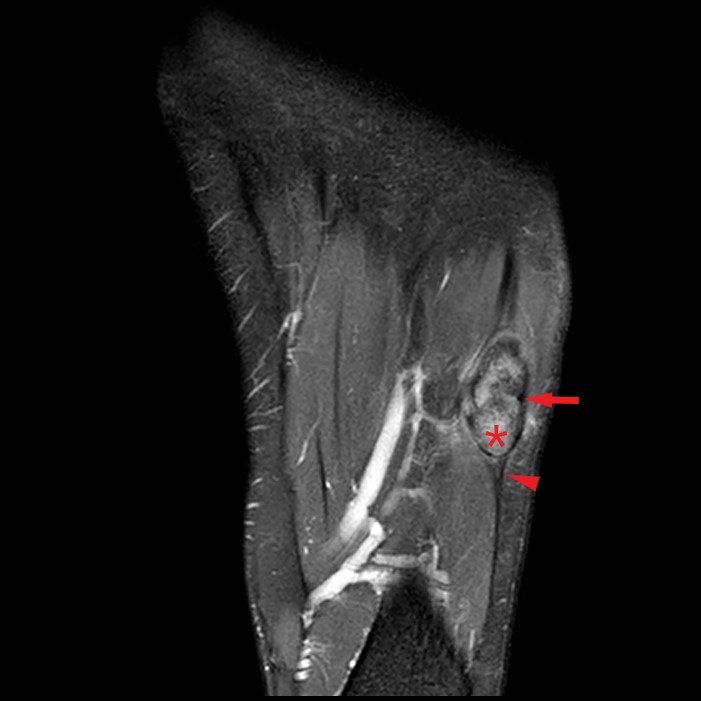

Figure 11: Sagittal proton density-weighted image (11A) and axial fat-suppressed proton density-weighted image (11B) in a 21-year-old male with chronic pain at the base of the fifth metatarsal demonstrates a hypertrophied, triangular-shaped ossicle (asterisks) adjacent to the fifth metatarsal base. Edema surrounds the synchondrosis (arrows) suggestive of micromotion. Lateral cord of the plantar aponeurosis (arrowhead) inserts on the ossicle. Oblique radiograph of the foot (11C) demonstrates the accessory ossicle at the fifth metatarsal base (arrowhead).
An os peroneum is one of the most common ossicles of the foot and present in up to 26% of the population.14 The ossicle is usually located at the calcaneocuboid joint and near the entrance to the cuboid tunnel. Painful os peroneum syndrome (POPS) refers to a wide spectrum of conditions that may present after local acute trauma or chronic overuse. Acute presentation results from sudden trauma, such as a supination injury and/or inversion of the ankle. An acute os peroneum fracture or diastasis of multipartite ossicle may result in disruption of the peroneus longus tendon. Chronic repetitive stress injuries of the foot may lead to hypertrophy and/or callus formation. This may result in local friction with the cuboid and regional impingement symptoms.15 Chronic partial or complete tearing of the peroneus longus tendon either proximal or distal to the ossicle may occur. Mechanical symptoms may lead to stenosing tenosynovitis surrounding the peroneus longus tendon.

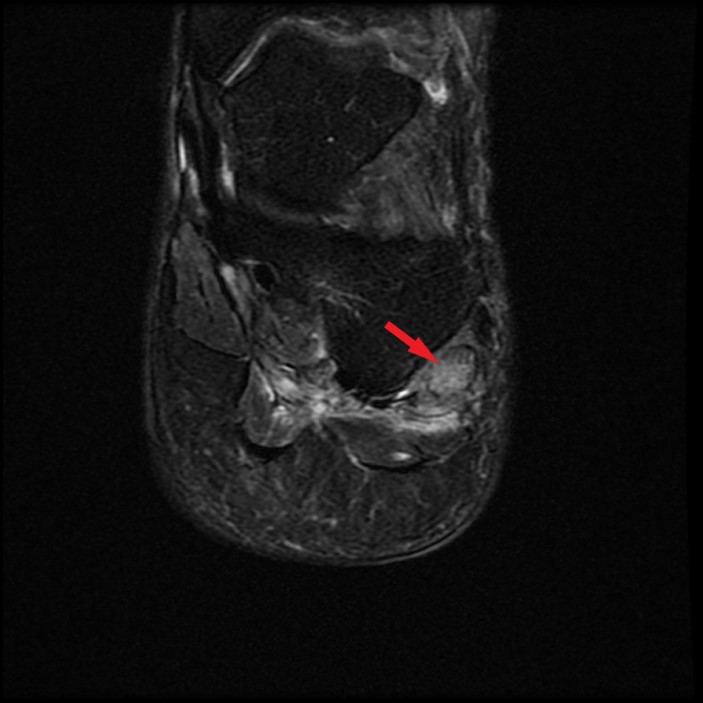


Figure 12: Axial (12A), coronal (12B), and sagittal (12C) fat-suppressed T2-weighted images in a 53-year-old with lateral midfoot pain after twisting injury 5 weeks ago demonstrates a hypertrophied, edematous os peroneum (arrows) located near the level of the calcaneocuboid joint within the peroneus longus tendon. The adjacent peroneus longus tendon (arrowheads) is moderately tendinopathic between the os peroneum and the cuboid tunnel. Oblique radiograph of the foot (12D) shows the corresponding enlarged os peroneum (arrow) with mild irregularity along the distal margin.
Peroneus longus tears may also occur in the absence of an os peroneum. Most often tearing of the peroneus longs occurs at the level of the lateral malleolus, usually following peroneus brevis tears. Isolated peroneus longus tendinosis and tearing typically occurs more distally at the midfoot16 where increased stress is placed on the tendon as it courses in the cuboid tunnel or at the level of the peroneal tubercle, particularly when it is hypertrophied.
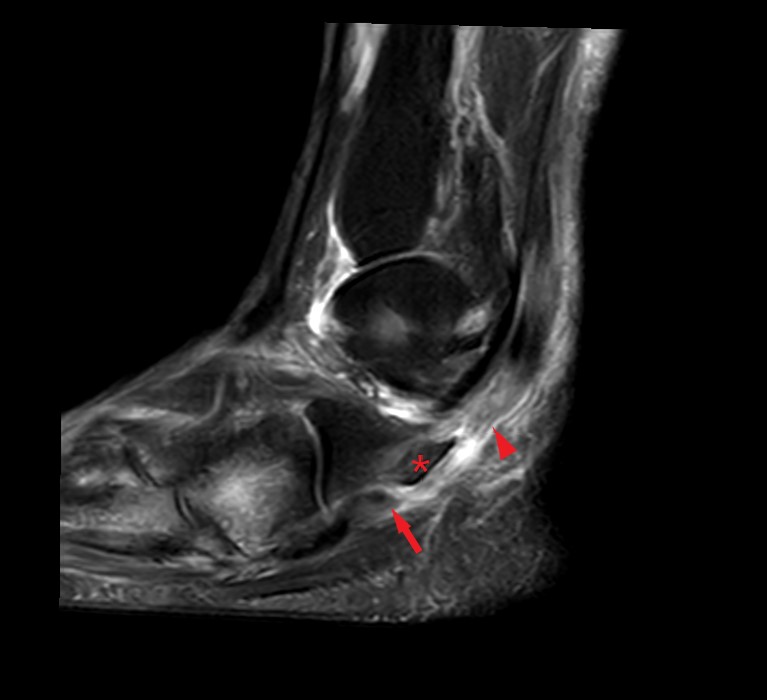
Figure 13: Sagittal STIR image demonstrates complete tear of the moderately tendinopathic peroneus longus tendon in a 62-year-old woman with 1 year of lateral foot pain. The distal tendon stump (arrow) is located between a hypertrophied peroneal tubercle (asterisk) and the cuboid tunnel. The proximal tendon stump (arrowhead) is retracted just proximal to the peroneal tubercle.
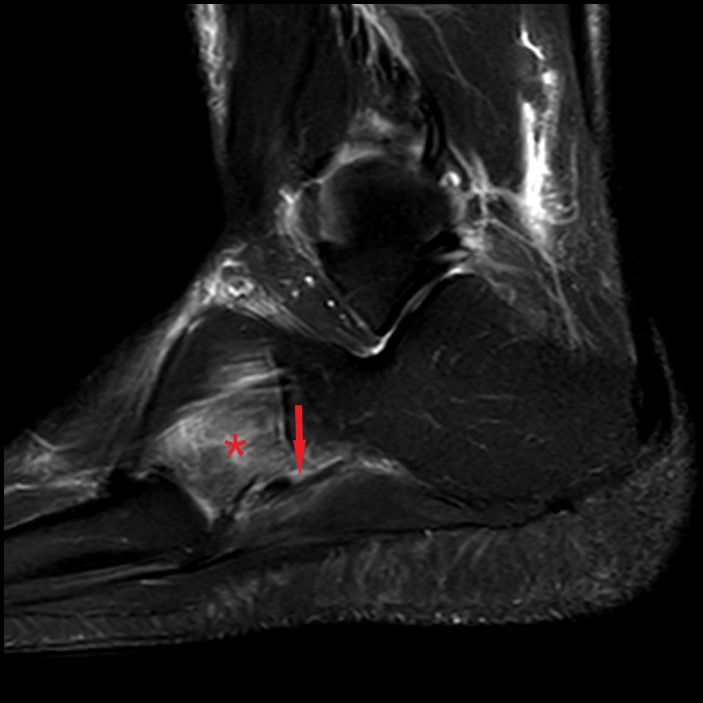
Figure 14: Sagittal STIR image in 42-year-old male with 2 weeks of lateral midfoot pain demonstrates high-grade partial tearing of the peroneus longus tendon just proximal to the cuboid tunnel (arrow). Stress-related edema is also present in the cuboid (asterisk).
Injuries of the peroneus brevis tendon are more common than those of the peroneus longus.17 Peroneus brevis tears may be acute and the result of trauma, most often a lateral ankle sprain18, or related to a chronic degenerative process. Most often, peroneus brevis tears occur in the retromalleolar groove and just beyond the lateral malleolus, where the tendon is predisposed to injury by mechanical wear or anatomic variances, such as a low-lying peroneus brevis muscle or presence of a variant peroneus quartus muscle. Less commonly, the peroneus brevis tendon may tear at the fifth metatarsal base insertion either due to acute trauma or chronic repetitive forces. In these cases, the pain associated with the distal peroneal tendon pathology may be confused with lateral cord insertional fasciopathy. Occasionally, distal peroneus brevis tendinosis and tearing may occur with lateral cord insertional fasciopathy.

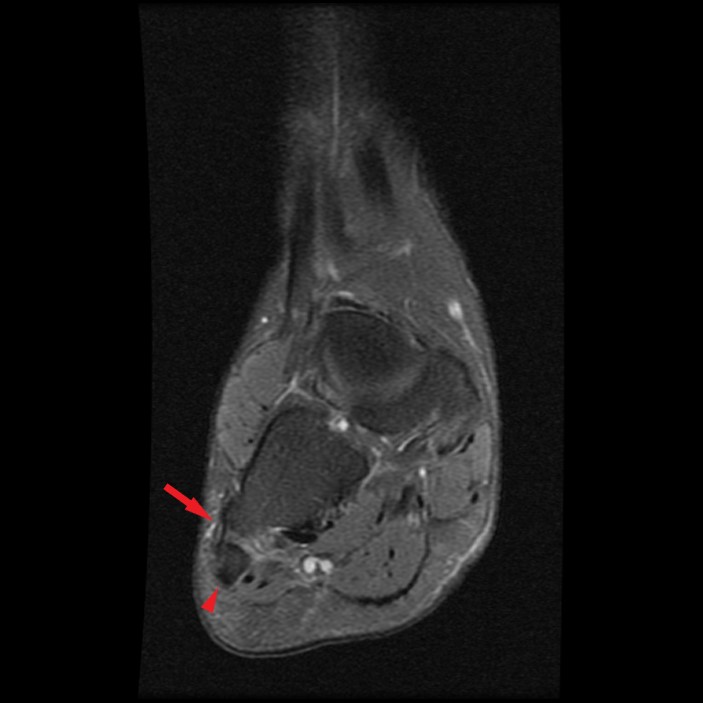
Figure 15: Oblique axial (15A) and coronal (15B) fat-suppressed T2-weighted images in a 25-year-old female with pain at the fifth metatarsal base demonstrate mild tendinosis and low grade interstitial tear of the peroneus brevis tendon (arrows) at the insertion on the lateral aspect of the fifth metatarsal base. The distal lateral cord of the plantar aponeurosis (arrowhead) is unremarkable.

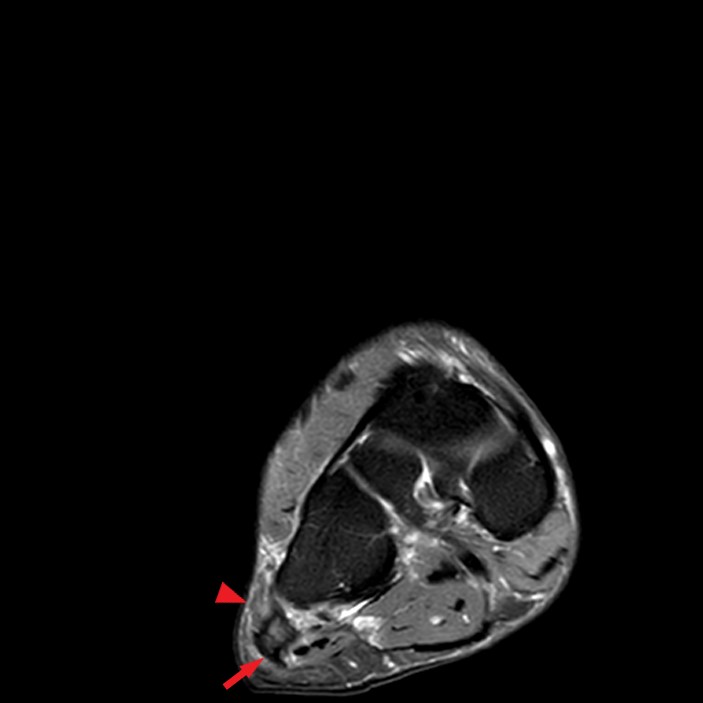
Figure 16: Sagittal (16A) and coronal (16B) fat-suppressed T2-weighted images of the ankle in a 55-year-old male with lateral foot pain demonstrates moderate tendinosis of the distal peroneus brevis tendon (arrowheads) with surrounding edema. There is also mildly increased signal and thickening of the lateral cord of the plantar aponeurosis (arrow) near the insertion on the plantar lateral aspect of the fifth metatarsal base consistent with accompanying lateral cord insertional fasciopathy.
Baxter’s nerve (first branch of the lateral plantar nerve) impingement may produce symptoms similar to plantar fasciitis and lateral midfoot pain, and it is often overlooked.19 Baxter’s nerve (also known as the inferior calcaneal nerve) is a mixed sensory and motor nerve, providing motor innervation to the abductor digiti minimi muscle.20 Entrapment of the nerve may occur as the nerve passes between the deep fascia of the abductor hallucis muscle and the medial margin of the quadratus plantae muscle or more distally as the nerve passes anterior to the medial calcaneal tuberosity20. Most commonly a plantar calcaneal enthesophyte21 and/or soft tissue changes related to plantar fasciitis may contribute to impingement.22 MRI may show typical findings of denervation selectively within the abductor digiti minimi muscle, and potentially within the flexor digitorum brevis and quadratus plantae muscles, depending on the innervation pattern. During acute/subacute muscle denervation, fluid sensitive sequences, such as T2-weighted imaging with fat suppression or STIR imaging will exhibit diffusely increased signal within the muscle belly compared to normal muscle, related to neurogenic muscular edema.23 While it may be challenging to differentiate, the edema typically seen in an abductor digiti minimi muscle strain will not be as diffuse and should extend along the myotendinous junction of the tendon. Chronic denervation results in volumetric atrophy and subsequently irreversible fatty infiltration, best depicted on non-fat-suppressed T1-weighted images.23

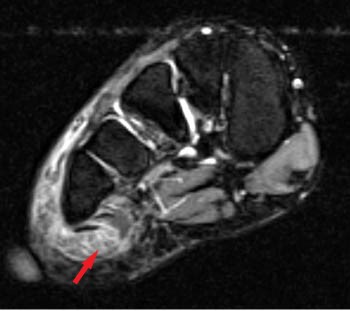
Figure 17: Axial T2-weighted image (17A) and coronal fat-suppressed T2-weighted image (17B) in a patient with lateral heel and midfoot pain demonstrates diffusely increased signal throughout the abductor digiti minimi muscle (arrows) consistent with subacute denervation in the setting of Baxter’s neuropathy. No atrophy of the muscle was present to suggest chronic denervation.
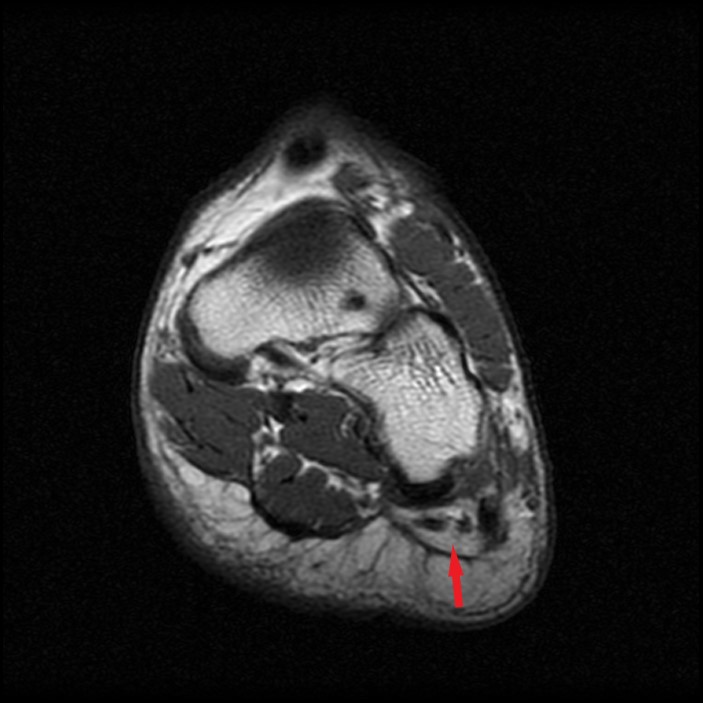
Figure 18: Coronal T1-weighted image in a different patient demonstrates diffuse fatty infiltration of the abductor digiti minimi muscle (arrow) suggestive of chronic denervation in the setting of Baxter’s neuropathy.
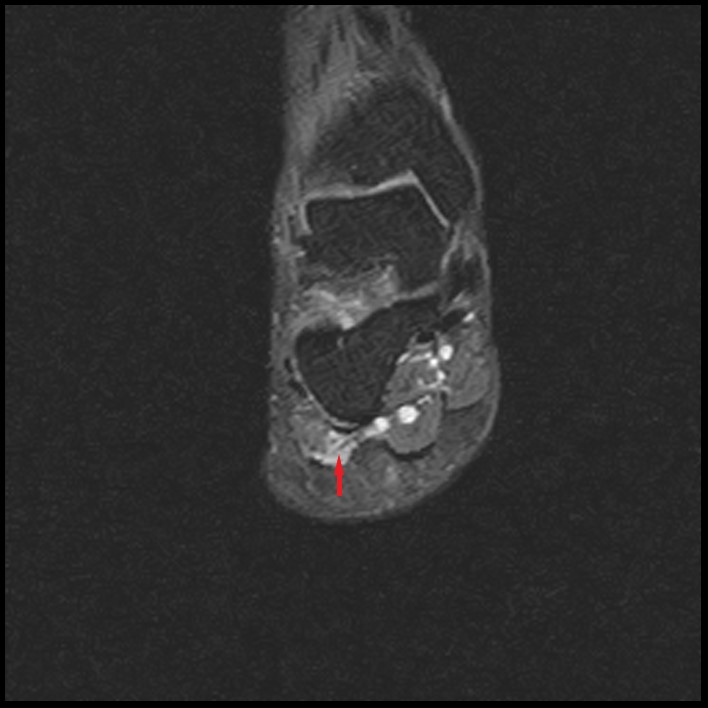
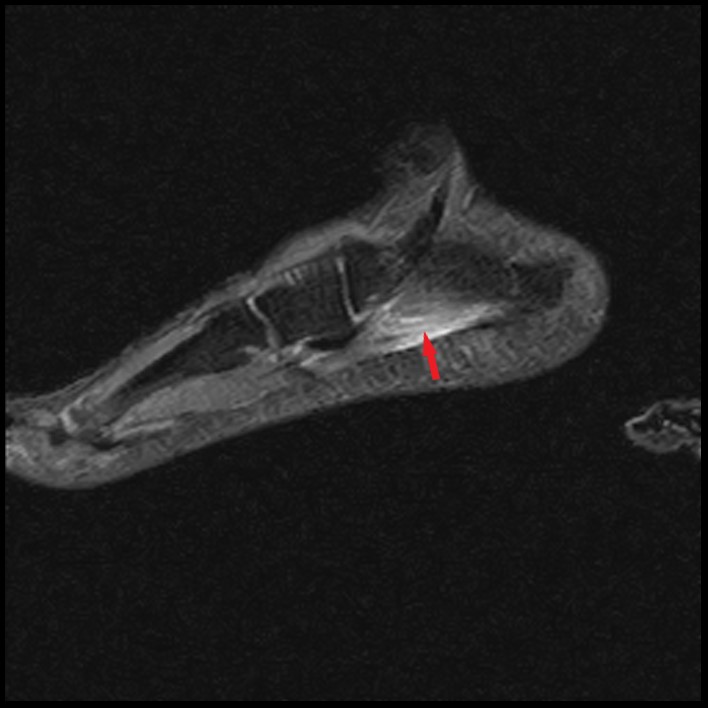

Figure 19: Coronal (19A) and sagittal (19B) fat-suppressed T2-weighted images in a different patient with acute lateral heel and midfoot pain demonstrate edema within the abductor digiti muscle that extends along the myotendinous junction (arrows) suggestive of myotendinous strain rather than diffusely involving the muscle as in subacute denervation. Coronal T1-weighted image (19Cc) demonstrates preserved muscle bulk of the abductor digiti minimi muscle (asterisk) without fatty infiltration.
Finally, thickening of the lateral cord of the plantar aponeurosis should be differentiated from more focal nodularity of the cord associated with plantar fibromatosis. As noted above, lateral cord plantar fasciitis most commonly occurs at the insertion of the lateral cord on the fifth metatarsal base. Plantar fibromatosis is a benign fibroblastic proliferative disorder associated with replacement of elements of the plantar aponeurosis with abnormal fibrous tissue.24 Typically, plantar fibromatosis is multinodular and most commonly occurs along the medial aspect of the central part of the plantar aponeurosis, most commonly near the level of the great toe metatarsal base.25 On MRI imaging, plantar fibromas appear as well-defined nodules of low signal intensity on T1-weighted and low-to-intermediate signal intensity on T2-weighted MR images.
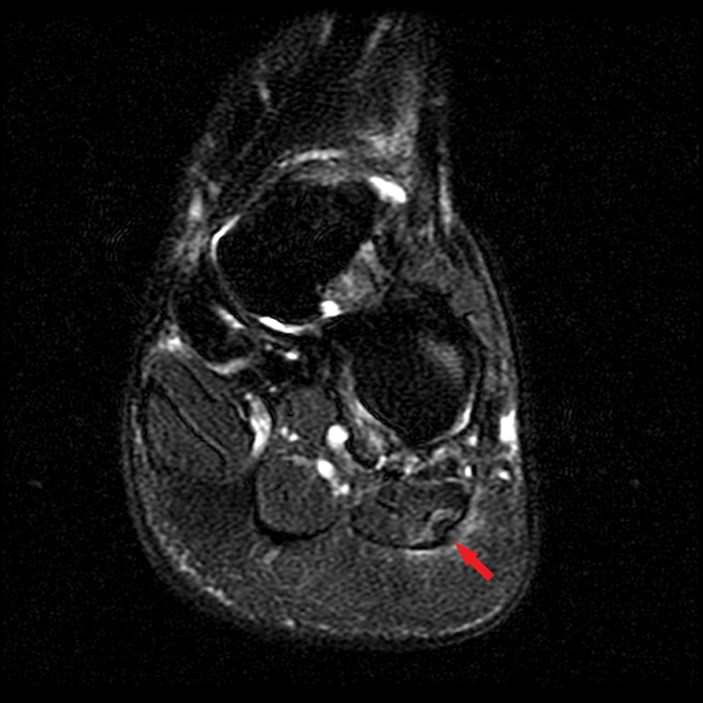

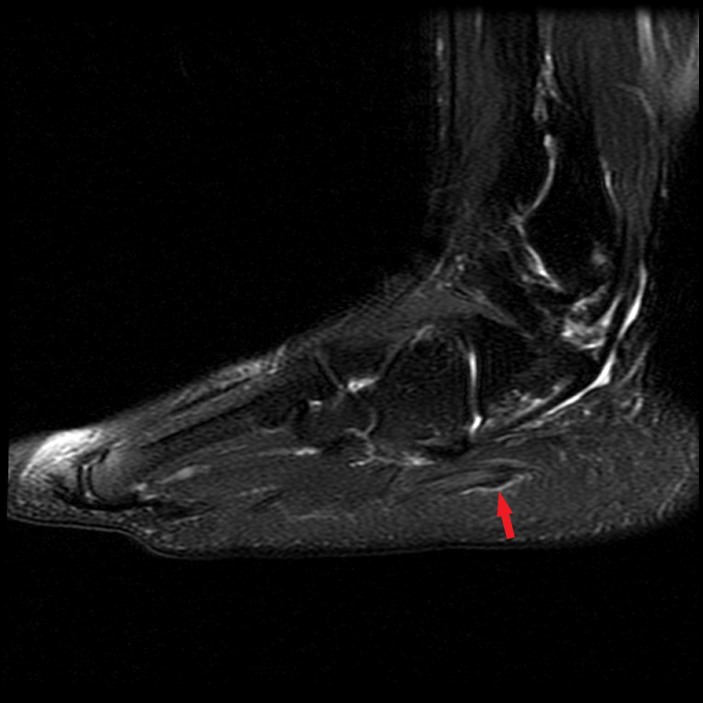
Figure 20: Fat-suppressed2-weighted (20A) and T1-weighted (20B) images in the coronal plane and a sagittal fat-suppressed T2-weighted image (20C) of the ankle in a 47-year-old female with lateral heel pain demonstrates focal nodular intermediate signal thickening along the lateral cord of the plantar aponeurosis proximal to the insertion suggestive of a plantar fibroma (arrows). This patient also had chronic denervation of the abductor digiti minimi muscle (asterisk).
Treatment
Treatment strategies for lateral cord insertional fasciopathy are not well established. Similar to the more common proximal central cord plantar fasciitis, initial modalities should include rest, orthotics/shoe modification, and activity modification.26 Persistent pain often responds to sonographically guided perifascial injection therapy with corticosteroid. When conservative treatment fails, transection of the lateral cord at the fifth metatarsal base may be effective.8
Conclusion
In conclusion, midfoot pain is a common problem with many potential causes. It is important to include lateral cord insertional fasciopathy as a potential cause of pain when pain is centered near the plantar lateral base of the fifth metatarsal. MRI is a useful tool in identifying lateral cord insertional fasciopathy and differentiating from multiple other potential causes, including fractures or peroneal tendon pathology.
References
- Karasick D, Wapner KL. Hallux valgus deformity: preoperative radiologic assessment. AJR Am J Roentgenol. 1990; 155:119-23. ↩
- Riddle DL, Schappert SM. Volume of ambulatory care visits and patterns of care for patients diagnosed with plantar fasciitis: a national study of medical doctors. Foot Ankle Int 2004; 25:303–310 ↩
- J. A. Narvaez, J. Narvaez, R. Ortega, C. Aguilera, A. Sanchez, and E. Andia Painful Heel: MR Imaging Findings RadioGraphics, March 1, 2000; 20(2): 333 – 352 ↩
- Schoene LM, Kincaid BR. When lateral band injury leads to plantar fasciopathy. Podiatry Today 2008; 21:56–60 ↩
- Newman E, Umans H, Elsinger E, Tobin KS. Not One of the Usual Suspects: MRI Features of Insertional Lateral Cord Plantar Fasciopathy. AJR Am J Roentgenol. 2018 Nov;211(5): W252-W256. doi: 10.2214/AJR.17.19218. Epub 2018 Sep 21. PMID: 30240290. ↩
- Thordarson DB, Schmotzer H, Chon J, Peters J. Dynamic support of the human longitudinal arch: a biomechanical evaluation. Clin Orthop 1995; 316:165-172 ↩
- Stecco C, Corradin M, Macchi V, Morra A, Porzionato A, Biz C, De Caro R. Plantar fascia anatomy and its relationship with Achilles tendon and paratenon. J Anat. 2013 Dec;223(6):665-76. doi: 10.1111/joa.12111. Epub 2013 Sep 12. PMID: 24028383; PMCID: PMC3842207. ↩
- Moraes do Carmo CC, Fonseca de Almeida Melão LI, Valle de Lemos Weber MF, Trudell D, Resnick D. Anatomical features of plantar apo-neurosis: cadaveric study using ultrasonography and magnetic resonance imaging. Skeletal Radiol 2008; 37:929–935 ↩
- DeVries JG, Taefi E, Bussewitz B, Hyer C, Lee T. The fifth metatarsal base: anatomic evaluation regarding fracture mechanism and treatment algorithms. J Foot Ankle Surg 2015; 54:94–98 ↩
- He W, Zhou H, Zhang Y, Yu T, Xia J, Zhao Y, Yang Y, Li B. Classification of avulsion fractures of the fifth metatarsal base using three-dimensional CT mapping and anatomical assessment: a retrospective case series study. J Foot Ankle Res. 2022 Aug 31;15(1):65. doi: 10.1186/s13047-022-00571-2. PMID: 36045449; PMCID: PMC9429432. ↩
- Richli WR, Rosenthal DI. Avulsion fracture of the fifth metatarsal: experimental study of pathomechanics. AJR Am J Roentgenol. 1984 Oct;143(4):889-91. doi: 10.2214/ajr.143.4.889. PMID: 6332501. ↩
- Inoue T, Yoshimura I, Ogata K, Emoto G. Os vesalianum as a cause of lateral foot pain: a familial case and its treatment. J Pediatr Orthop B 1999; 8:56–58 ↩
- Forrester RA, Eyre-Brook AI, Mannan K. Iselin’s disease: a systematic review. J Foot Ankle Surg 2017; 56:1065–1069 ↩
- Peacock KC, Resnick EJ, Thoder JT. Fracture of the os peroneum with rupture of the peroneus longus tendon. Clin Orthop 1986; 202:223-226 ↩
- Bashir WA, Lewis S, Cullen N, Connell DA. Os peroneum friction syndrome complicated by sesamoid fatigue fracture: a new radiological diagnosis? Case report and literature review. Skeletal Radiol. 2009;38(2):181–186. doi: 10.1007/s00256-008-0588-3. ↩
- Rademaker J, Rosenberg ZS, Delfaut EM, Cheung YY, and Schweitzer ME. Tear of the Peroneus Longus Tendon: MR Imaging Features in Nine Patients. Radiology, Mar 2000; 214: 700 – 704. ↩
- Giza E, Mak W, Wong SE, Roper G, Campanelli V, Hunter JC. A clinical and radiological study of peroneal tendon pathology. (2013) Foot & ankle specialist. 6 (6): 417-21. doi:10.1177/1938640013501544 ↩
- Dombek MF, Lamm BM, Saltrick K, Mendicino RW, Catanzariti AR. Peroneal tendon tears: a retrospective review. The Journal of Foot and Ankle Surgery. 42 (5): 250-258. Doi:10.1016/S1067-2516(03)00314-4 ↩
- Delfaut EM, Demondion X, Bieganski A, Thiron MC, Mestdagh H, Cotten A. Imaging of foot and ankle nerve entrapment syndromes: from well-demonstrated to unfamiliar sites. Radiographics. 2003; 23:613-623. ↩
- Recht MP, Groof P, Ilaslan H, Recht HS, Sferra J, Donley BG. Selective Atrophy of the Abductor Digiti Quinti: An MRI Study. AJR 2007; 189:123-127. ↩
- Chundru U, Liebeskind A, Seidelmann F, Fogel J, Franklin P, Beltran J. Plantar fasciitis and calcaneal spur formation are associated with abductor digiti minimi atrophy on MRI of the foot. Skeletal Radiol. 2008; 37:505-10. ↩
- Donovan A, Rosenberg ZS, Cavalcanti CF. MR imaging of entrapment neuropathies of the lower extremity. Part 2. The knee, leg, ankle, and foot. Radiographics. 2010; 30:1001-1019. ↩
- Kim SJ, Hong SH, Jun WS, et al. MR imaging mapping of skeletal muscle denervation in entrapment and compressive neuropathies. Radiographics. 2011; 31:319-32. ↩
- Theodorou DJ, Theodorou SJ, Farooki S, Kakitsubata Y, Resnick D. Disorders of the plantar aponeurosis: a spectrum of MR imaging findings. AJR Am J Roentgenol. 2001 Jan;176(1):97-104. doi: 10.2214/ajr.176.1.1760097. PMID: 11133545. ↩
- Lee TH, Wapner KL, Hecht PJ. Plantar fibromatosis: current concepts review. J Bone Joint Surg Am 1993; 75-A:1080-1083 ↩
- Latt LD, Jaffe DE, Tang Y, Taljanovic MS. Evaluation and Treatment of Chronic Plantar Fasciitis. Foot Ankle Orthop. 2020 Feb 13;5(1):2473011419896763. doi: 10.1177/2473011419896763. PMID: 35097359; PMCID: PMC8564931. ↩
