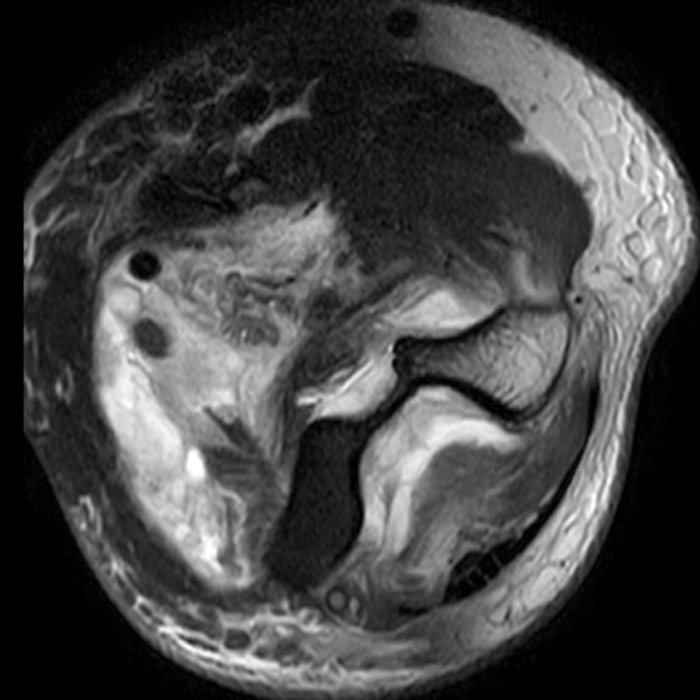
Clinical History: A 35-year-old male presents with pain and swelling in the distal arm and antecubital fossa after an ATV accident. Axial T2-weighted fat-suppressed(1A) and sagittal proton density-weighted fat-suppressed (1B) images are provided. What are your findings? What is your diagnosis?

Findings
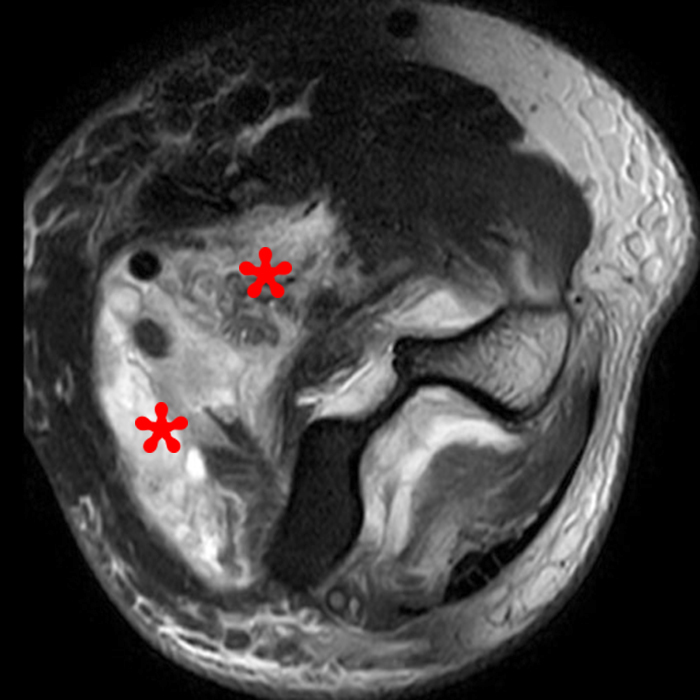
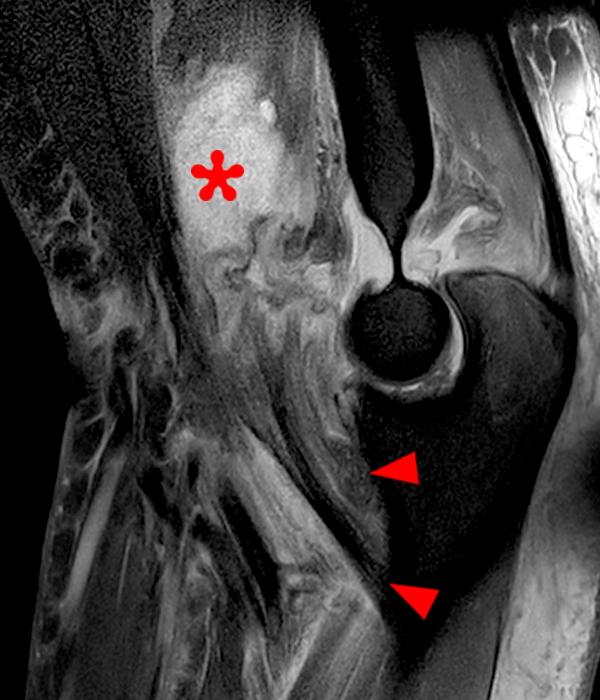
Figure 2: Fat-suppressed axial T2-weighted (2A) and sagittal proton density-weighted (2B) images demonstrate a large brachialis intramuscular defect (asterisks) with diffuse surrounding muscle edema and heterogeneous fluid signal in the muscle gap. Note that the distal insertion of the brachialis onto the ulna is intact (arrowheads).
Diagnosis
High-grade tear of the brachialis muscle with intramuscular hematoma and diffuse muscle and surrounding soft tissue edema.
Introduction
Brachialis muscle injuries may be associated with biceps brachii injuries or may occur in isolation. Isolated brachialis muscle injuries are rare, and brachialis tendon injuries are even more rare when compared to biceps brachii injuries, which make up the majority of elbow flexor injuries.1,2 In fact, the first reported case of an isolated brachialis muscle tear was in 2001, and only a few cases have been reported since.3 Because of the rarity of the reported injury, a timely, accurate diagnosis may be missed when it does occur. MRI is very useful for the diagnosis of the type, location, and severity of brachialis muscle injury, as well as differentiating it from other pathologic entities.
Anatomy
There is a relative paucity of literature describing the anatomy of the brachialis muscle. Within the available literature, there are discrepancies regarding the anatomic makeup of the muscle and its distal insertion, including controversy regarding the number of muscle heads and the type of distal insertion. Recent anatomic studies in the past few decades have helped clarify some of the controversies.4,5,6,7 It has been established that the brachialis muscle contains two heads: a large superficial head and a smaller deep head. The superficial head originates from the anterolateral aspect of the mid humerus and lateral intermuscular septum, and the deep head originates from the distal third of the anterior aspect of the humerus and medial intermuscular septum.4,5 The muscle belly of the superficial head is anterior and ulnar to the muscle belly of the deep head.4 The superficial head forms a thick circular tendon distally, which inserts onto the distal aspect of the ulnar tuberosity. The deep head muscle fibers converge into a fan-shaped musculotendinous/musculoaponeurotic structure, which attaches more broadly to the coronoid process and proximal aspect of the ulnar tuberosity. The superficial and deep heads attach to the ulnar tuberosity overall as a single contiguous blended structure.4,5,6 Finally, Leonello et al. described some muscle fibers attaching to the anterior elbow, while Resnick et al. saw no discrete muscle attachments.
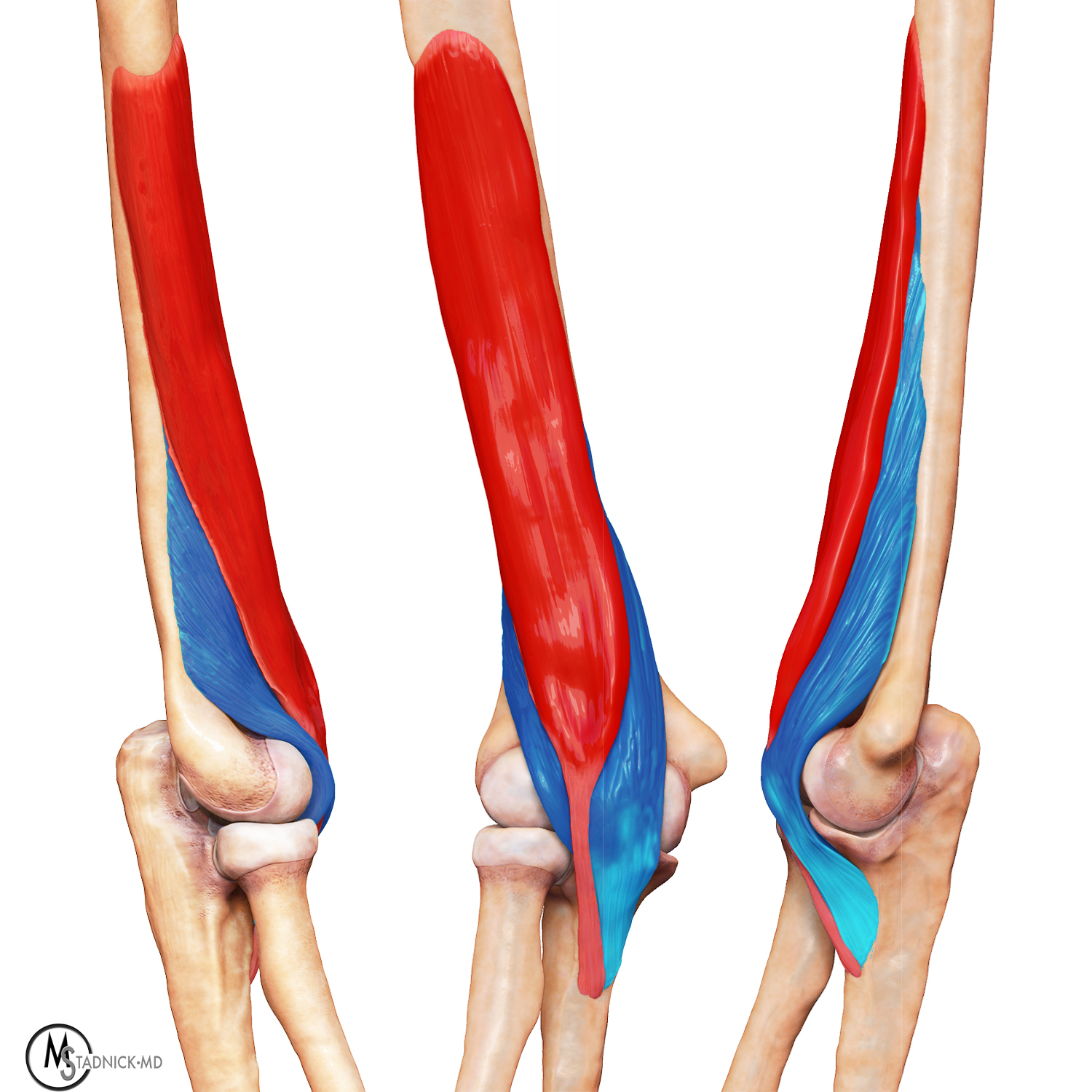
Figure 3: Lateral (left), anterior (middle), and medial (right) 3D views of the elbow demonstrate the superficial (red) and deep (blue) heads of the brachialis muscle.
Function
The biceps brachii, brachialis, and brachioradialis all contribute to elbow flexion. Because the brachialis lies anterior to the elbow joint and inserts onto the ulna, it only contributes to flexion of the elbow, with no role in supination or pronation.5,8 It generates the most contractile force between the three muscles.2,9 The biceps brachii also contributes to supination of the radioulnar joint.6 The brachialis has the poorest mechanical advantage of the elbow flexors due to a small lever arm when the elbow is in full extension as the line of the ulna, humerus, and brachialis fibers are parallel during extension. It has its strongest position when the elbow is in 90-degree flexion as the brachialis fibers are perpendicular to the ulna at this position.5 Leonello et al. postulate that the noticeable morphological differences between the superficial and deep heads suggest they have distinct functions. As the deep fibers insert more anterior to the axis of rotation of the ulnohumeral joint due to partly inserting onto the coronoid process, the deep head is thought to play a more important role in the initiation of flexion from full extension, and the superficial head is thought to generate more power once the elbow is flexed due to an increase in mechanical advantage at this position. 2,5 Leonello et al. also postulate that since the inferolateral deep head fibers of the brachialis and the anconeus are both innervated by the radial nerve and travel in a similar direction parallel to the lateral ulnar collateral ligament, they likely provide dynamic restraint to rotatory instability. Kulig also showed that the brachialis is responsible for maintaining stability of the elbow throughout concentric and eccentric contraction and is preferentially recruited over the biceps brachii when undergoing eccentric contraction.10
Normal MRI Appearance
Axial images are very helpful in identifying the brachialis musculoaponeurotic and tendon insertions. Sagittal images are helpful in delineating the fan-shaped muscle fibers inserted onto the ulna, and sagittal as well as coronal images help identify the tendinous portion.4 The superficial head insertion demonstrates a typical tendinous hypointense linear signal, and the deep head insertion demonstrates a striated muscle pattern (Figure 4).
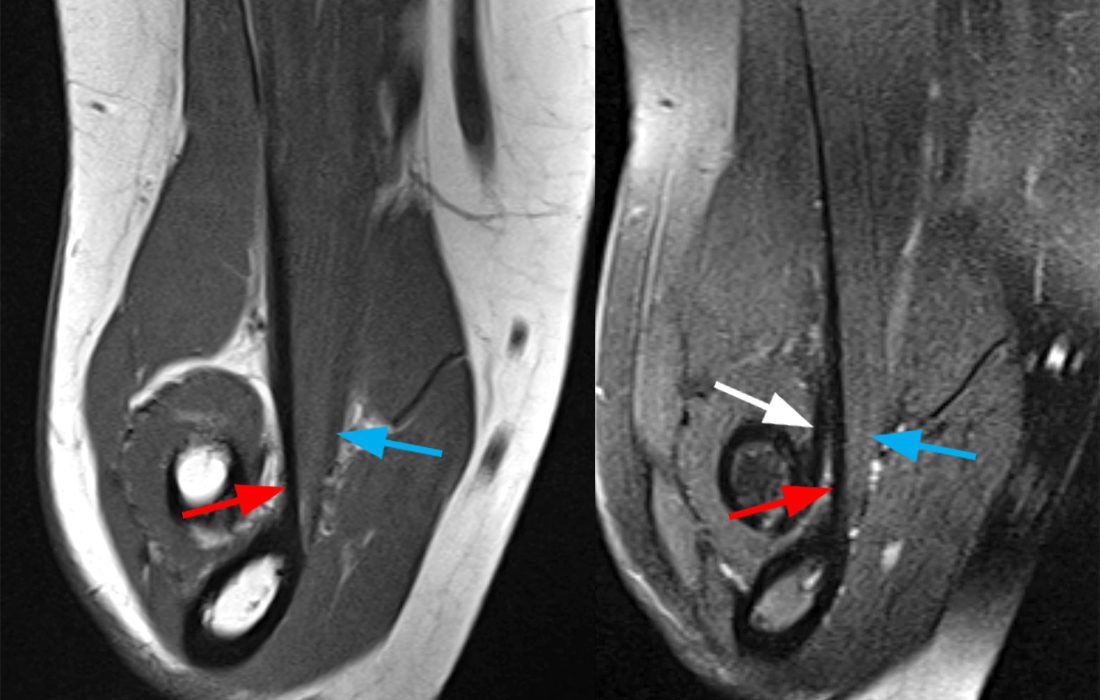
Figure 4A: Coronal T1-weighted and fat-suppressed T2-weighted Flexed Abducted Supinated Views (FABS) (4A) demonstrate the distal tendinous insertion (red arrows), which arises from the superficial head and the more broadly attaching distal musculotendinous/musculoaponeurotic insertion (blue arrows), which originates from the deep head of the brachialis muscle. The distal biceps brachii tendon is also indicated (white arrow). Image courtesy of Varand Ghazikhanian, MD
Figure 4B: This is an interactive image series. To scroll through the series, left click and hold on the image, then drag down over the image. Note: The image will not open in a separate window when clicked. Sequential axial T1-weighted FABS images (4B) demarcate the tendinous portion of the brachialis superficial head insertion onto the ulnar tuberosity (red arrows) and the adjacent musculotendinous/musculoaponeurotic deep head portion inserting onto the ulna (blue arrows). The distal biceps brachii tendon insertion is also indicated (white arrow).
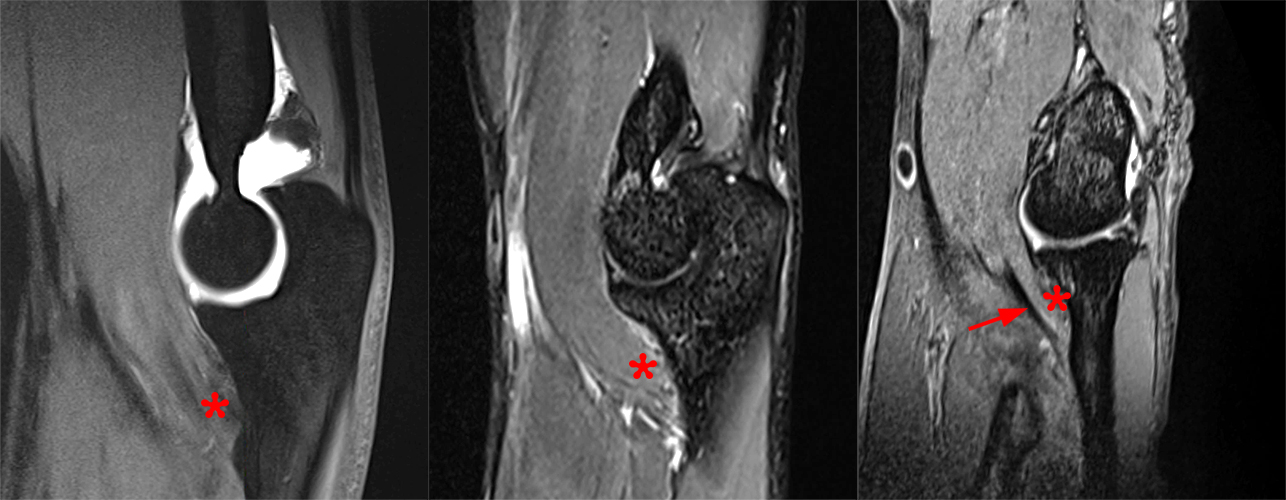
Figure 4C: Sagittal T1-weighted with fat-suppression arthrogram (left), T2-weighted fat-suppressed (middle), and sagittal gradient echo (right) images from different patients demonstrate the combined insertion of the distal brachialis (asterisks). The tendinous portion is more clearly visible in some patients than others (arrow).
Clinical Presentation and Pathophysiology
Acute brachialis injuries are postulated to occur with eccentric contraction during pronation and resistance of hyperextension.1,11,12 They have been described in hockey, rugby, football, and lifting of heavy objects.3,13,11,14,15,16,17,2,1,12 Most, if not all, reported cases in the literature describe muscle tears as opposed to insertional tears, although in our practice, we have seen insertional tears. On physical exam, there is pain and swelling anteriorly and proximal to the elbow without discernible bruising or neurologic deficit. There is also pain with flexion and extension, including inability to fully extend the elbow. There is no finger motion restriction, and there is usually normal range of motion in pronation and supination. A palpable mass may be felt. In general, it is difficult to palpate the brachialis due to its deep location. Of note, a biceps brachii tendon gap is not present on physical exam, which can be a helpful clue.1,11,14 More chronically, repetitive pull-ups, especially in climbers, which involve the use of arms predominantly in the pronated semi-flexed position, can result in strain and tendinopathy of the brachialis, called “climber’s elbow.” 18
MRI Findings
MRI is an excellent tool for the characterization of brachialis injuries, including location and severity, and for simultaneously evaluating the remainder of the elbow for additional or alternative pathology. Acute muscle tears are easily seen on fluid-sensitive images, demonstrating discontinuity of the muscle fibers with architectural distortion, intervening fluid and/or hemorrhagic signal collection, muscle edema, and surrounding soft tissue edema, with or without evidence of insertional signal abnormality. Lower-grade muscle strains will demonstrate feathery edema signal in the muscle belly on fluid-sensitive sequences without muscle fiber disruption (Figure 5).
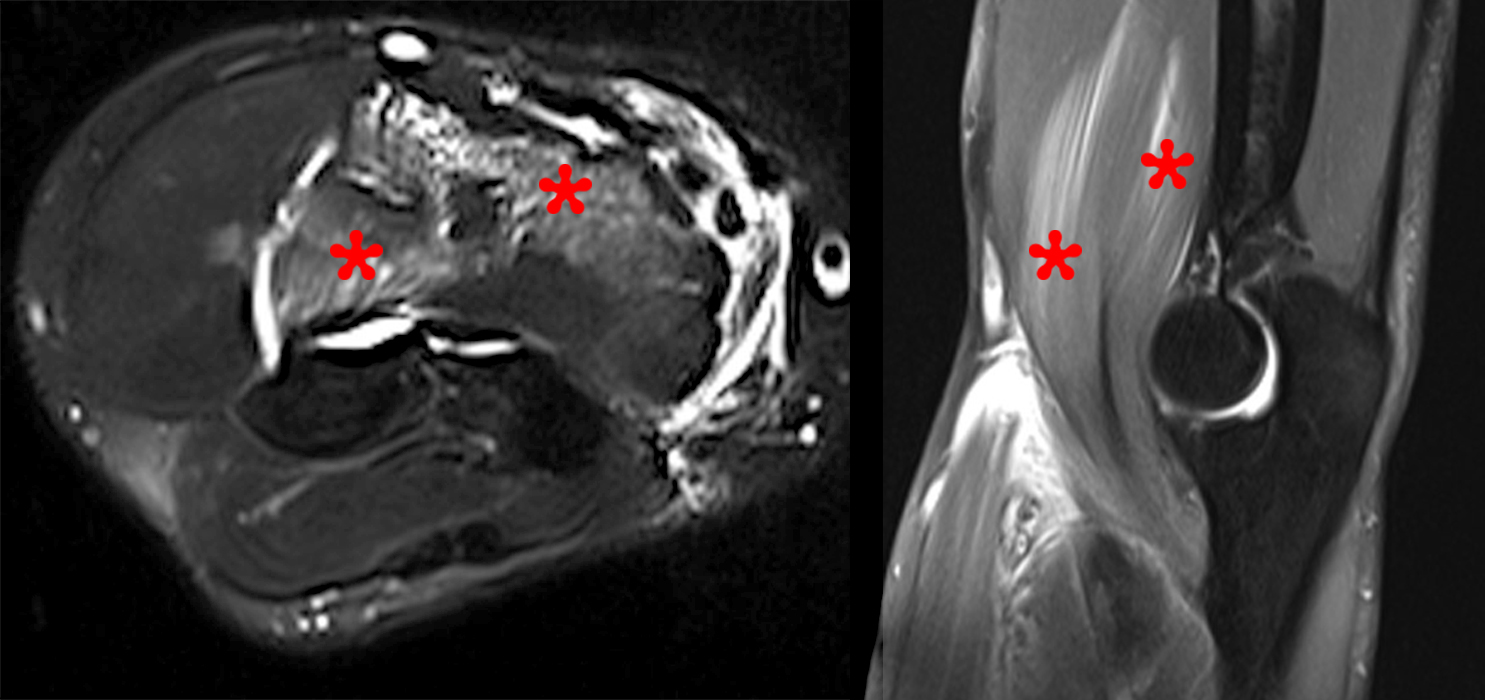
Figure 5: Axial T2-weighted fat-suppressed (left) and sagittal proton density-weighted fat-suppressed (right) images demonstrate diffuse feathery edema throughout the brachialis muscle (asterisks) without focal muscle or tendon disruption, compatible with a low-grade strain.
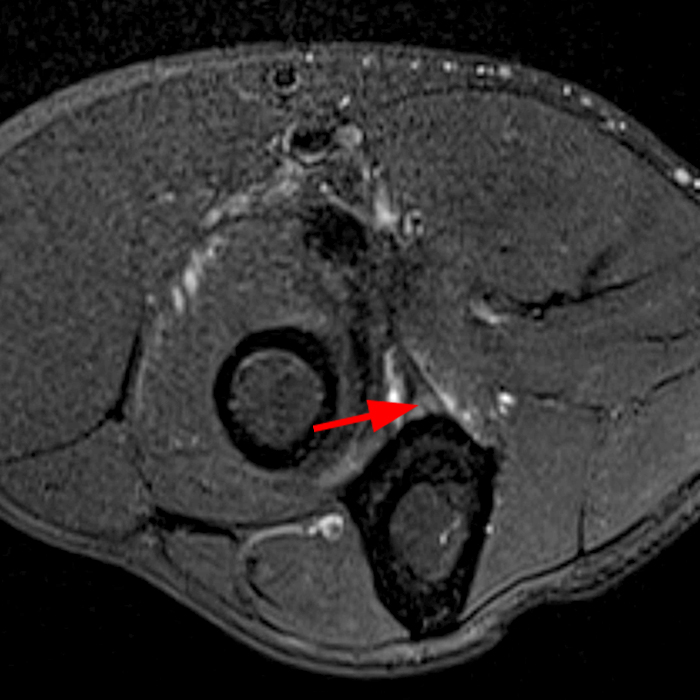
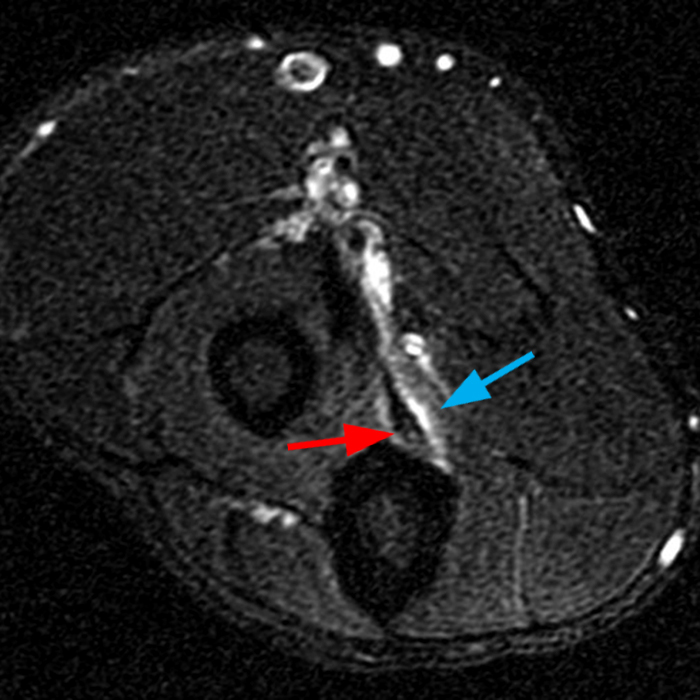
Figure 6: Axial T2-weighted fat-suppressed image (6a) demonstrates intermediate T2 signal at the tendinous insertion (red arrow) of the brachialis compatible with mild tendinosis. Axial T2-weighted fat-suppressed image in a different patient (6b) demonstrates mild tendinosis at the brachialis tendon insertion (red arrow) as well as edema in the deep head (blue arrow) consistent with strain.
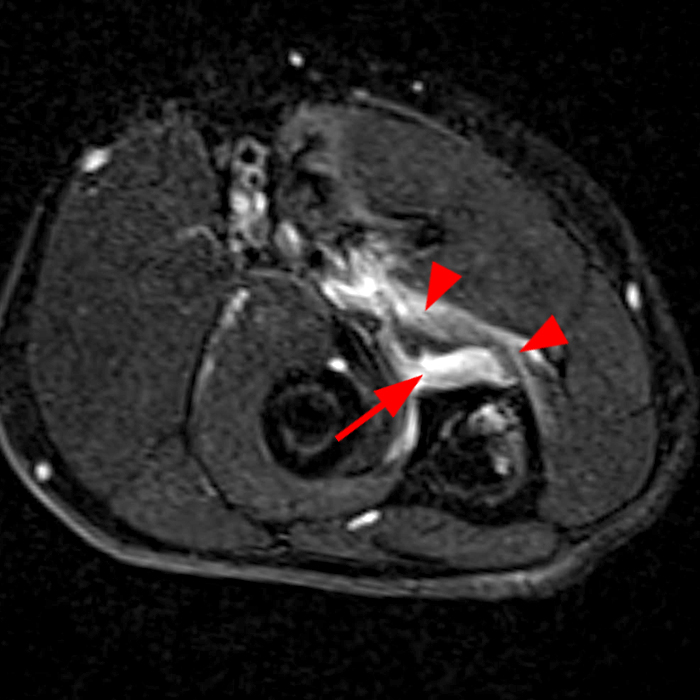
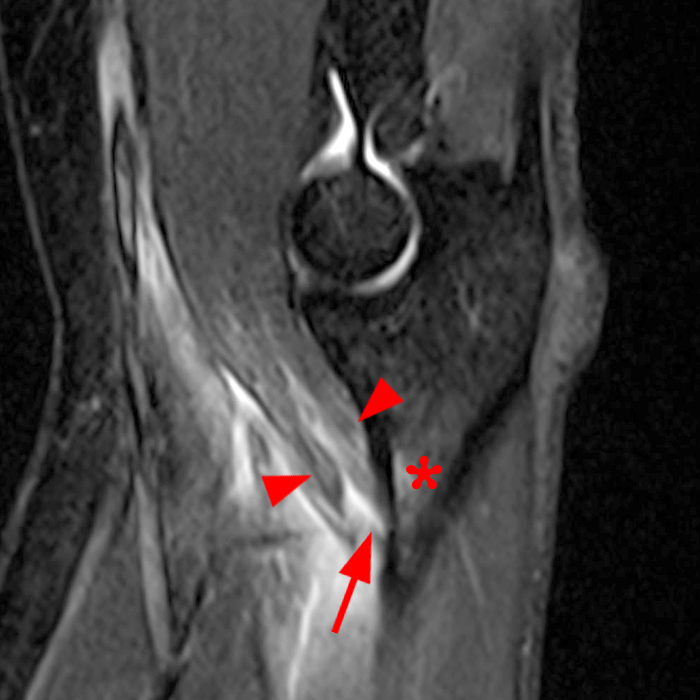
Figure 7: Axial T2-weighted fat-suppressed (7A) and sagittal STIR (7B) images demonstrate a partial tear of the distal brachialis insertion with a small fluid gap at the tendinous insertion (arrow), mild subjacent marrow edema (asterisk) and edema in the remainder of the musculotendinous/musculoaponeurotic insertion (arrowheads).
Differential Considerations
Distal biceps tendon rupture: Distal biceps tendon injuries are much more common than brachialis injuries. Distal biceps tendon injuries most commonly occur in the dominant arm of males over the age of 40 or in younger athletes sustaining a heavy load on the distal biceps during flexion.19,20 Distal biceps tendon ruptures account for 3-10% of biceps injuries. Distal biceps tendon ruptures are readily demonstrated by MRI (Figure 8).
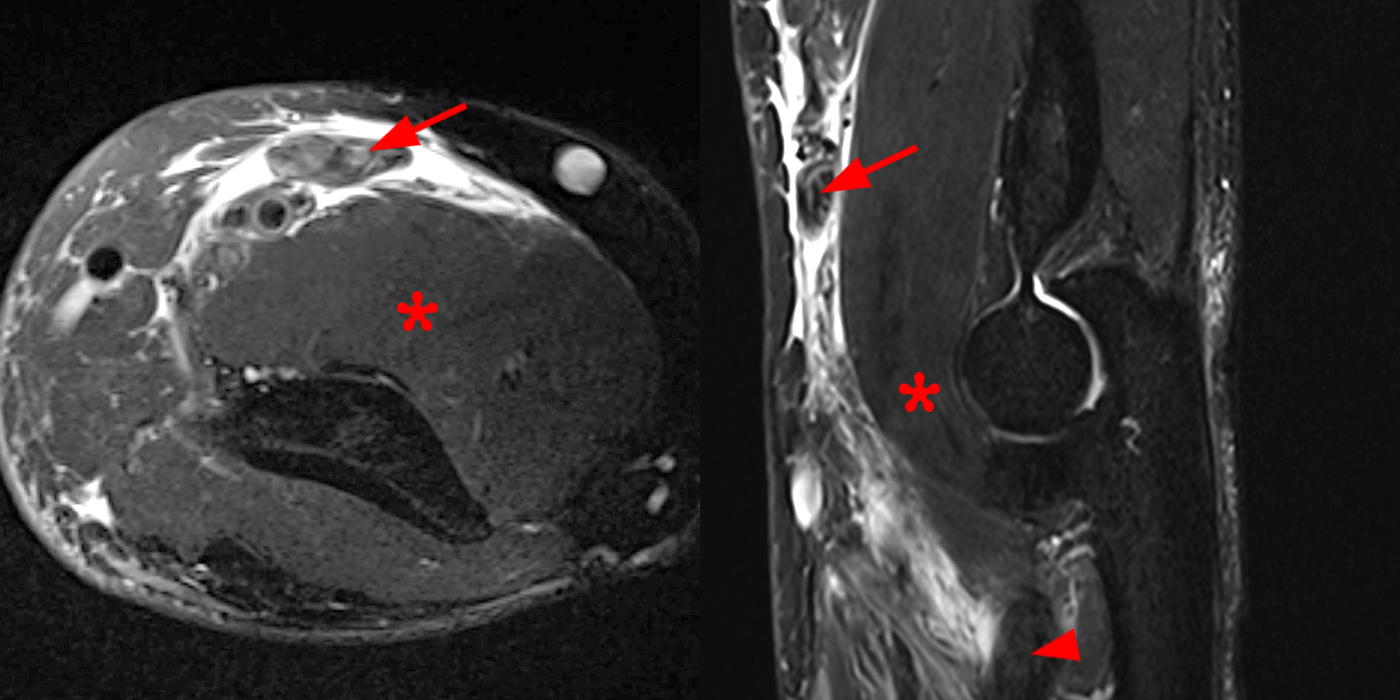
Figure 8A: Axial T2-weighted fat-suppressed axial (left) and sagittal STIR (right) (8A) ultrasound images demonstrate complete rupture of the distal biceps brachii tendon with retraction of the torn tendon (arrows) from the bicipital tuberosity (arrowhead) and surrounding fluid and hematoma with a normal appearing subjacent brachialis muscle (asterisks). Images courtesy of Varand Ghazikhanian, MD
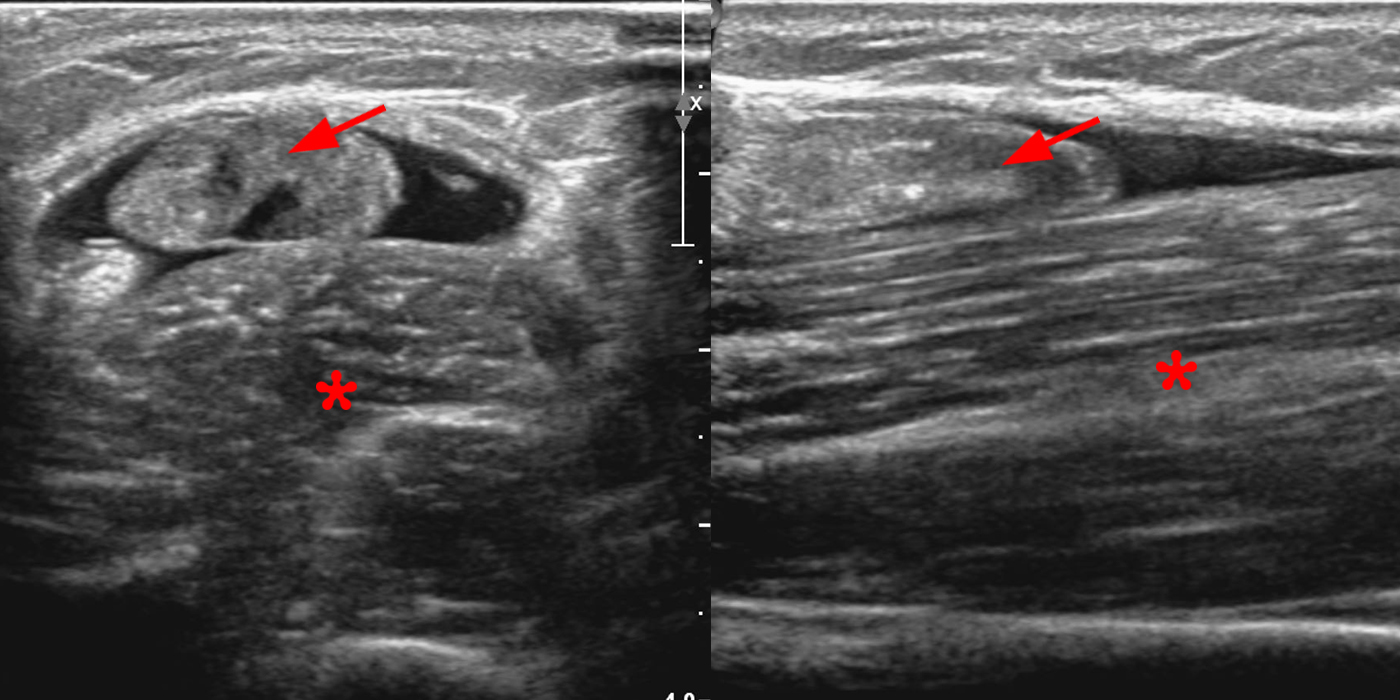
Figure 8B: Short-axis (left) and long-axis (right) (8B) ultrasound images demonstrate complete rupture of the distal biceps brachii tendon with retraction of the torn tendon (arrows) from the bicipital tuberosity (arrowhead) and surrounding fluid and hematoma with a normal appearing subjacent brachialis muscle (asterisks). Images courtesy of Varand Ghazikhanian, MD
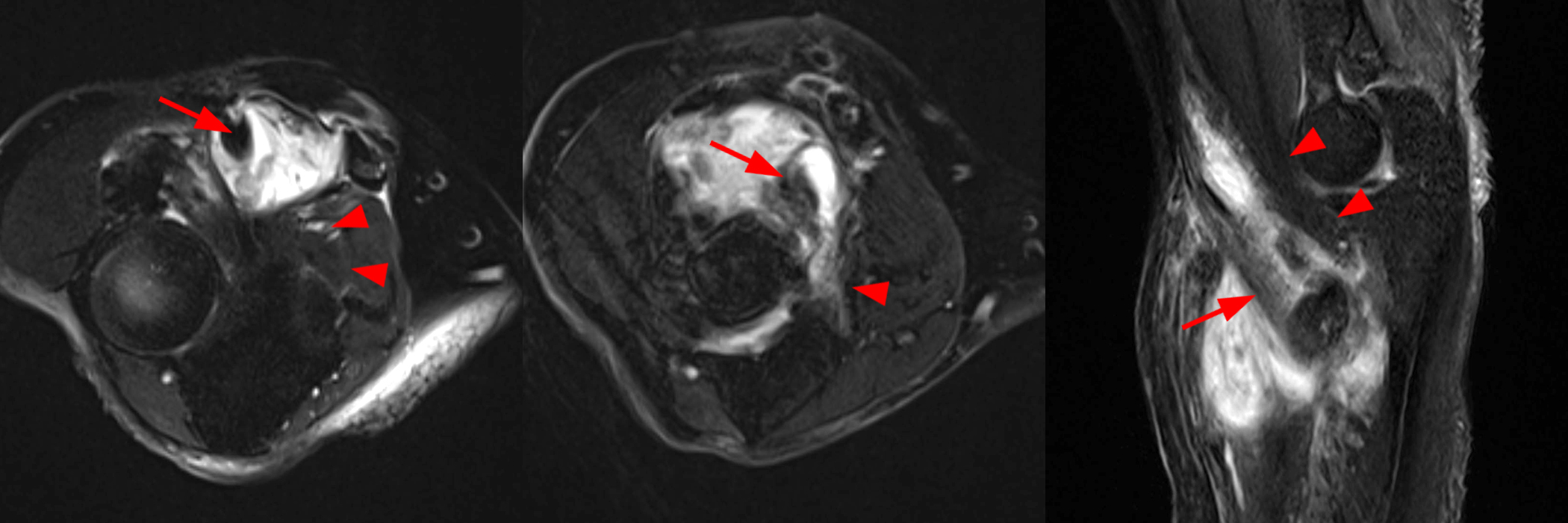
Figure 9: Axial T2-weighted fat-suppressed (left and middle) and sagittal STIR (right) images demonstrate marked distension of the bicipitoradial bursa containing extensive synovitis and debris. There is underlying distal biceps tendinosis (arrows) with an intact flattened distal brachialis musculotendinous insertion (arrowheads).
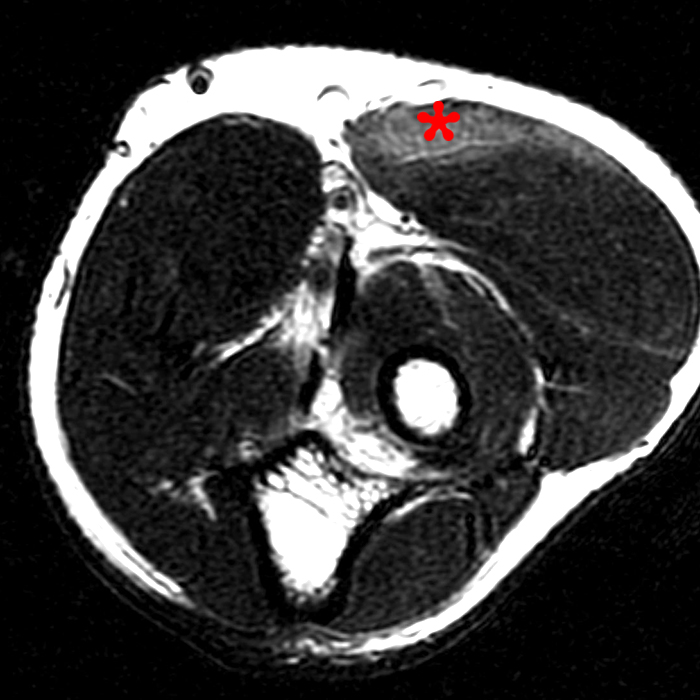
Figure 10: Axial T2-weighted image demonstrates mild feathery edema in the brachioradialis muscle (asterisk) compatible with low-grade strain.
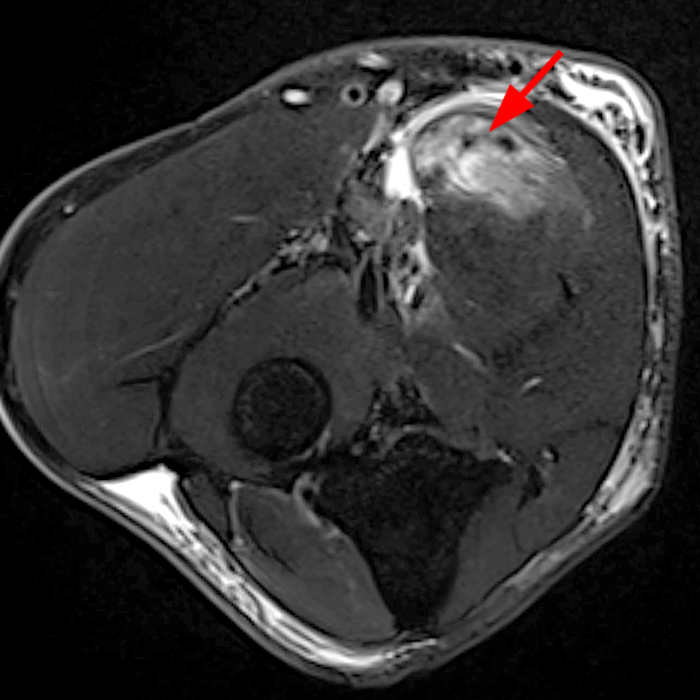
Figure 11: Axial T2-weighted fat-suppressed image demonstrates a focal myotendinous partial tear of the pronator teres (arrow) with focal muscle edema and partial myotendinous disruption.
Treatment
There is no standard treatment protocol. Both surgical and non-surgical treatments have been described, but most brachialis injuries have been treated conservatively in the literature, with report of one high-level athlete undergoing surgical repair to facilitate early return to sport.14 Conservative therapy in acute injuries involves cast immobilization with flexion to bring the torn brachialis muscle fibers in close approximation for 1-3 weeks, followed by progressive range of motion exercises to regain function and range of motion.1,14,15
Conclusion
The diagnosis of brachialis muscle or insertional tear may be difficult clinically due to its rare nature and deep location in the anterior elbow, precluding a thorough physical exam. MRI allows evaluation of the brachialis muscle and its insertion, can assist in differentiation of muscle belly or insertional tears, and exclude pathology in the adjacent structures.
References
- Winblad JB, Escobedo E, Hunter JC. Brachialis Muscle Rupture and Hematoma. Radiol Case Reports. 2008;3(4):251. doi:10.2484/rcr.v3i4.251 ↩
- Forsythe CM, Burtis MT, Pfeiffer DC, Spurling GR, Ashby DB. Acute brachialis muscle tear in a pediatric patient. Radiol Case Reports. 2020;15(5):498-501. doi:10.1016/j.radcr.2020.01.041 ↩
- Van den Berghe GR, Queenan JF, Murphy DA. Isolated rupture of the brachialis: A case report. J Bone Jt Surg. 2001;83(7):1074-1075. doi:10.2106/00004623-200107000-00015 ↩
- Sanal HT, Chen L, Negrao P, Haghighi P, Trudell DJ, Resnick DL. Distal attachment of the brachialis muscle: Anatomic and MRI study in cadavers. Am J Roentgenol. 2009;192(2):468-472. doi:10.2214/AJR.08.1150 ↩
- Leonello DT, Galley IJ, Bain GI, Carter CD. Brachialis muscle anatomy: A study in cadavers. J Bone Jt Surg. 2007;89(6):1293-1297. doi:10.2106/JBJS.F.00343 ↩
- Mistry PN, Rajguru J, Dave MR. An Anatomical Insight into the Morphology of the Brachialis Muscle and its Clinical Implications. Int J Anat Radiol Surg. 2021;10(2):16-20. doi:10.7860/ijars/2021/46128.2625 ↩
- Kamineni S, Bachoura A, Behrens W, Kamineni E, Deane A. Distal Insertional Footprint of the Brachialis Muscle: 3D Morphometric Study. Anat Res Int. 2015;2015:1-6. doi:10.1155/2015/786508 ↩
- Plantz MA, Bordoni B. Anatomy, Shoulder and Upper Limb, Brachialis Muscle. StatPearls. 2020:1-7. http://www.ncbi.nlm.nih.gov/pubmed/31869094. ↩
- Kawakami Y, Nakazawa K, Fujimoto T. Specific tension of elbow flexor and extensor muscles base on magnetic resonance imaging. Eur J Appl Physiol Occup Physiol. 1994;(68):139-147. ↩
- Kulig K, Powers CM, Shellock FG, Terk M. The effects of eccentric velocity on activation of elbow flexors: Evaluation by magnetic resonance imaging. Med Sci Sports Exerc. 2001;33(2):196-200. doi:10.1097/00005768-200102000-00004 ↩
- Nishida Y, Tsukushi S, Yamada Y, Hosono K, Ishiguro N. Brachialis Muscle Tear Mimicking an Intramuscular Tumor: A Report of Two Cases. J Hand Surg Am. 2007;32(8):1237-1241. doi:10.1016/j.jhsa.2007.06.002 ↩
- Krych AJ, Kohen RB, Rodeo SA, Barnes RP, Warren RF, Hotchkiss RN. Acute brachialis muscle rupture caused by closed elbow dislocation in a professional American football player. J Shoulder Elb Surg. 2012;21(7):1-5. doi:10.1016/j.jse.2011.11.007 ↩
- Wasserstein D, White L, Theodoropoulos J. Traumatic brachialis muscle injury by elbow hyperextension in a professional hockey player. Clin J Sport Med. 2010;20(3):211-212. doi:10.1097/JSM.0b013e3181df1ed4 ↩
- Yamaji A, Uesugi M, Kamada H, Ichimura H, Yamazaki M. Brachialis Muscle Rupture in a Pediatric Patient Followed Up by Ultrasound Examinations: A Rare Case Report. Case Rep Orthop. 2022;2022:1-5. doi:10.1155/2022/3391350 ↩
- Lam JCY, Lee KLR, Griffith JF. Brachialis periosteal avulsion injury: case report with magnetic resonance imaging findings. Skeletal Radiol. 2016;45(11):1561-1564. doi:10.1007/s00256-016-2459-7 ↩
- Sharma P, Mehta N, Narayan A. Isolated Traumatic Brachialis Muscle Tear: A Case Report and Review of Literature. Bull Emerg Trauma. 2017;5(4):307-310. doi:10.18869/acadpub.beat.5.4.476 ↩
- Murugappan KS, Mohammed K. Acute traumatic brachialis rupture in a young rugby player: A case report. J Shoulder Elb Surg. 2012;21(6):12-14. doi:10.1016/j.jse.2011.10.009 ↩
- Bollen SR. Soft tissue injury in extreme rock climbers. Br J Sports Med. 1988;22(4):145-147. doi:10.1136/bjsm.22.4.145 ↩
- Pinas M, Nijs S, Shahabpour M. Distal Biceps Brachii Tendon Injuries: An Imaging Update. J Belgian Soc Radiol. 2021;105(1):1-5. doi:10.5334/jbsr.2696 ↩
- Giuffrè BM, Moss MJ. Optimal Positioning for MRI of the Distal Biceps Brachii Tendon: Flexed Abducted Supinated View. Am J Roentgenol. 2004;182(4):944-946. doi:10.2214/ajr.182.4.1820944 ↩
- Yap SH, Griffith JF, Lee RKL. Imaging bicipitoradial bursitis: a pictorial essay. Skeletal Radiol. 2019;48(1):5-10. doi:10.1007/s00256-018-2970-0 ↩
