Clinical History
A 30-year-old male presents with pain at the metacarpophalangeal (MP) joint of the thumb following a bicycle wreck. Coronal proton density-weighted (Figure 1A) and inversion recovery (Figure 1B) images, and consecutive axial proton density-weighted images (Figure 1C and 1D) are provided. What are the findings? What is your diagnosis?




Findings




Figure 2: The coronal images (2A and 2B) reveal a complete tear of the thumb MP joint ulnar collateral ligament (UCL) from its distal insertion. The torn ligament (arrows) is retracted proximal to the adductor aponeurosis (arrowhead), best seen on the proton density-weighted sequence, and the torn ligament points ulnarly rather than distally. The adductor aponeurosis (arrowheads) is fully visualized in the axial plane at the metacarpal head (2C). An axial slice (2D) just proximal the aponeurosis reveals the balled-up, retracted UCL (arrow).
Diagnosis
Complete distal disruption of the ulnar collateral ligament at the MP joint of the thumb, with a Stener lesion.
Discussion
Ulnar collateral ligament (UCL) tears at the metacarpophalangeal (MP) joint of the thumb are a well-known and not uncommon injury, first described as gamekeeper’s thumb by Campbell in a study of 25 Scottish gamekeepers who tore their ligaments due to repetitive valgus stress from breaking the necks of rabbits. 1 Of course, in modern times such activities are frowned upon and UCL tears are now much more commonly encountered after acute trauma. The injury is now often referred to as Skier’s Thumb, as it is known to occur from acute valgus injury to the thumb MP joint when a skier falls onto the outstretched hand while grasping a ski pole.
The Stener lesion, first described by Bertil Stener, 2 occurs when the torn UCL becomes proximally retracted during radial deviation of the joint and the adductor aponeurosis becomes interposed between the joint and the torn retracted ligamentous fibers (Figure 3). The interposed tissue from the adductor aponeurosis prevents the torn end of the UCL from approximating to its insertion point on the proximal phalanx base, and thus healing with conservative therapy such as casting becomes impossible. 3 A Stener lesion is thus felt to be an absolute indication for surgical repair of the UCL.
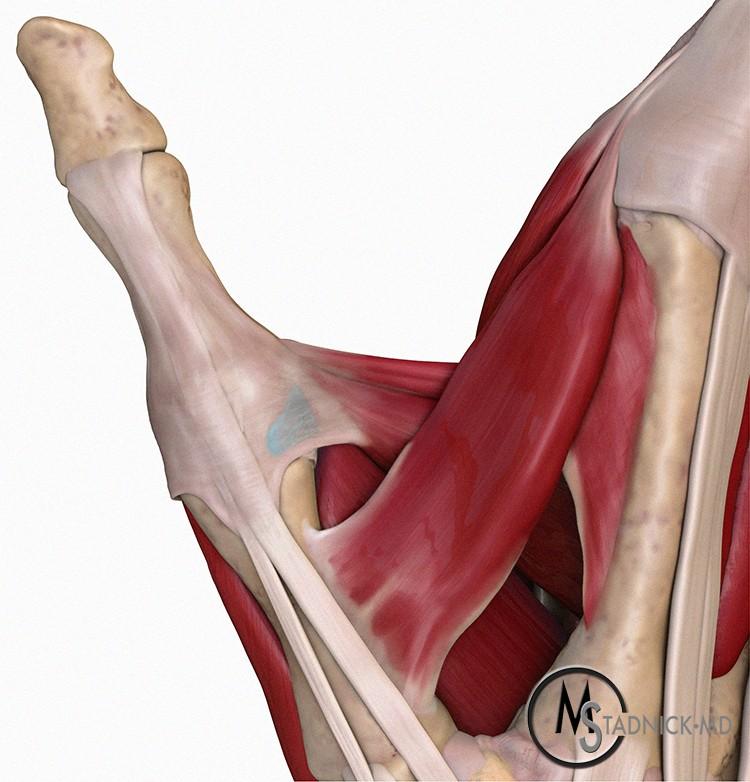
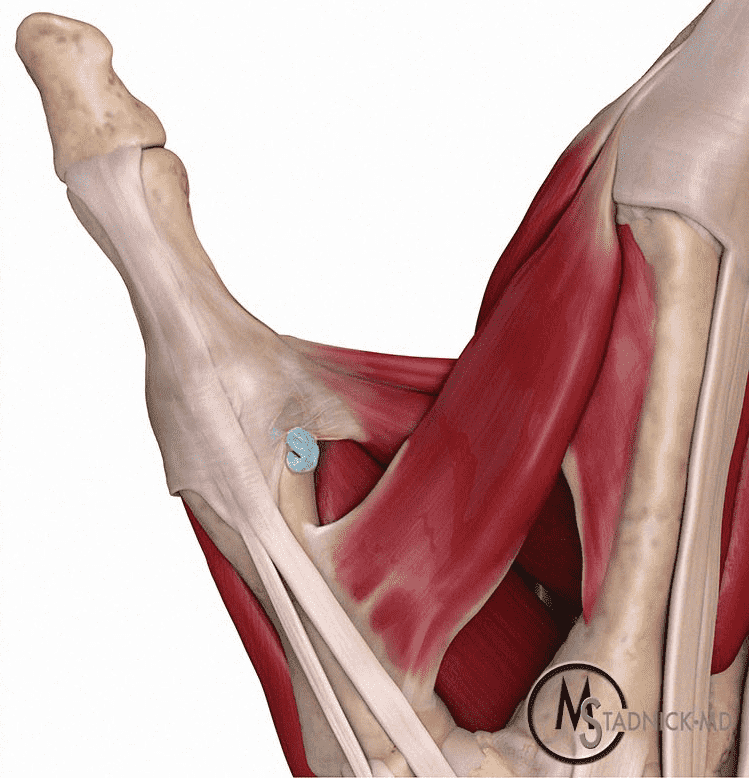
Figure 3: (3A) Dorsal Illustration of the normal thumb MP joint showing the intact UCL (in blue) deep to the fibers of the adductor aponeurosis. (3B) With a Stener lesion, the torn stump of the UCL is retracted proximal to the leading edge of the aponeurosis, which becomes interposed between the torn ligament and its anatomic insertion site.
The thumb Stener lesion is perhaps the best know example of a musculoskeletal finding that requires timely surgery. However, there are multiple other examples of musculoskeletal pathology seen on MRI that also require surgical repair due to interposed tissue. This Web Clinic will review other entities that are “Stener-like”, in which the skilled radiologist is able to provide an accurate diagnosis and therefore guide the referring physician towards appropriate (surgical) treatment.
Stener-like lesion of the radial collateral ligament of the thumb MP joint
Radial collateral ligament (RCL) tears at the MP joint of the thumb are less common than those of the UCL, typically caused by a fall on the radial aspect of the thumb or by varus stress to the proximal phalanx. MRI has demonstrated high accuracy for detecting RCL injuries at the thumb.4 Stener-like lesions associated with RCL tears of the thumb are recognized though rarely reported. As with true Stener lesions, the soft-tissue interposition of the abductor aponeurosis in such cases (Figure 4) is felt to be an absolute indication for operative repair.


Figure 4: 35-year-old man presents after a hyperextension injury to the thumb while playing basketball. (4A) A fat-suppressed T2-weighted coronal image demonstrates a completely torn and retracted radial collateral ligament (RCL, arrow) lying proximal and superficial to the abductor aponeurosis (arrowheads). Bone bruising is evident within the proximal phalanx (asterisk). (4B) A fat-suppressed proton density-weighted axial image just proximal to the abductor aponeurosis reveals poorly defined retracted ligamentous tissue (arrow). The aponeurosis of the abductor pollicis longus muscle (arrowheads) lies superficial and parallel to the RCL and is unlikely to become interposed.
Stener-like lesions of the fingers
Collateral ligament injuries to the fingers are less common than at the thumb, as these joints are less likely to undergo extreme stress, and dynamic lateral support is provided by the interosseous muscles. 5 Because the most common mechanism of injury is ulnar deviation, RCL tears predominate. Stener-like lesions of the fingers occur when the torn RCL is trapped by an injured or intact radial sagittal band (Figure 5).
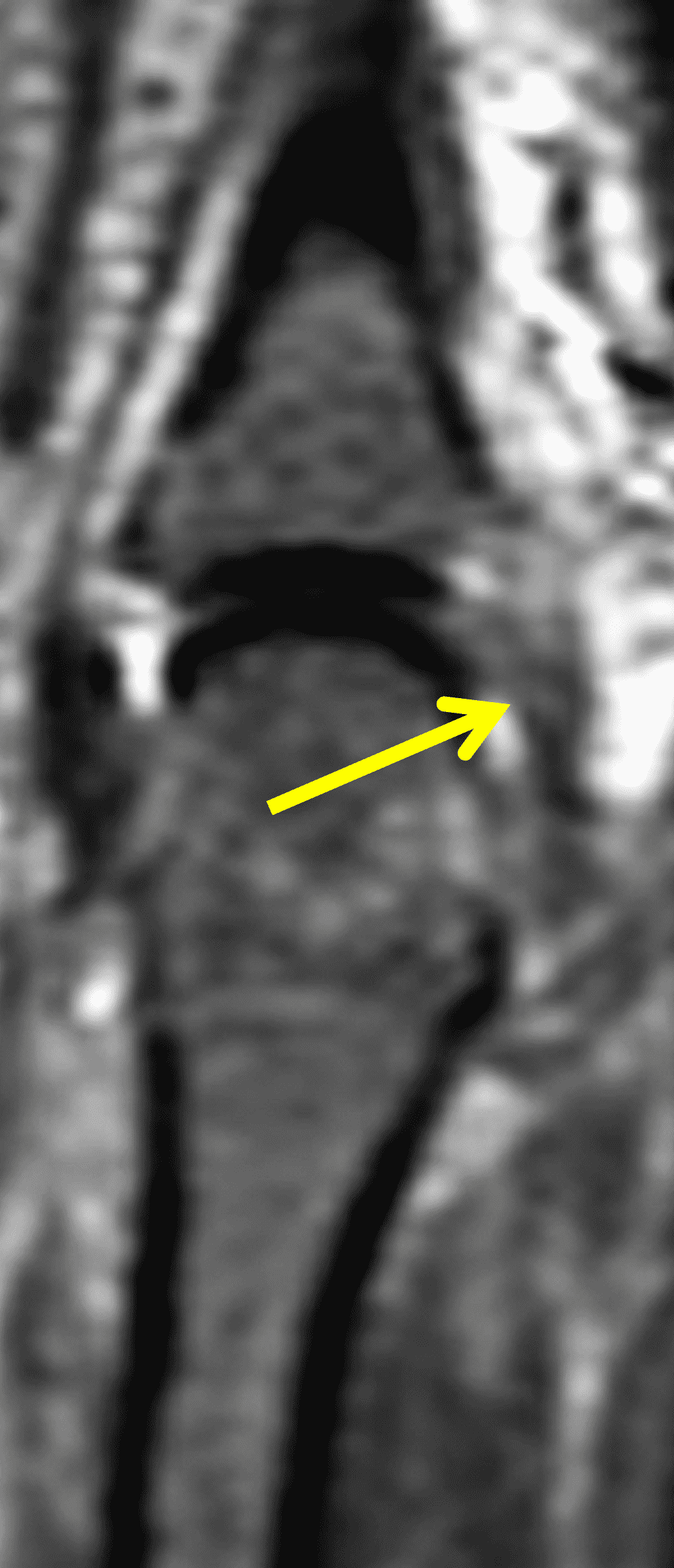


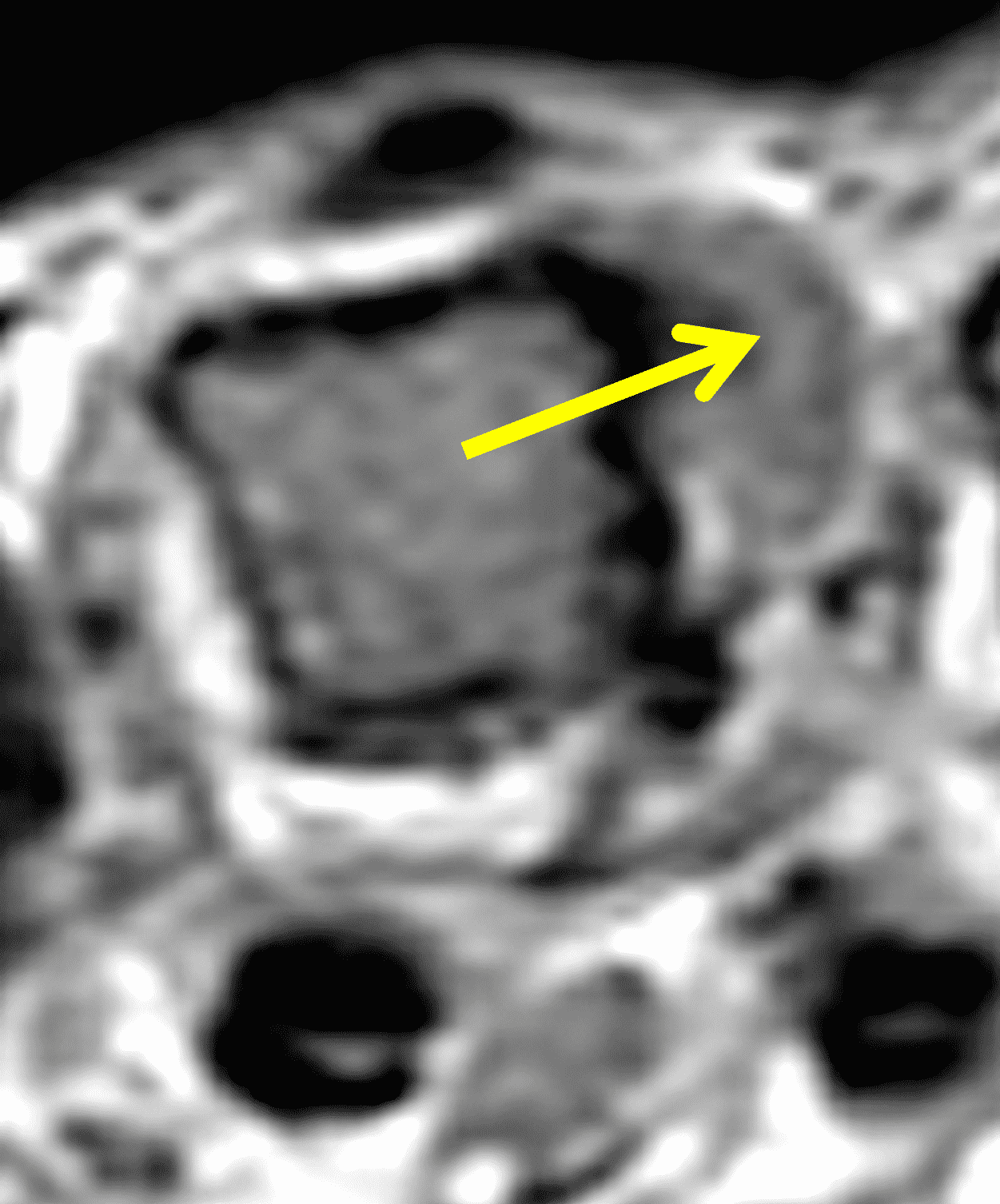
Figure 5: A 52-year-old man presents with pain at the MCP joint of the long finger following a fall. (5A) Consecutive coronal STIR images demonstrate a poorly defined and edematous long finger MCP joint RCL (arrow). (5B) On the next dorsal slice, the balled-up and retracted RCL is apparent (arrow). (5C) Axial STIR image reveals an intact radial sagittal band (arrowheads). (5D) More proximally, retracted ligamentous tissue is apparent (arrow).
The small finger, with no finger protecting its medial side, is the most commonly injured MCP joint other than the thumb. Forced ulnar deviation results in RCL tears. In such cases, patients may present with a palpable mass that in fact represents bunched-up, retracted ligamentous tissue (Figures 6 and 7).6

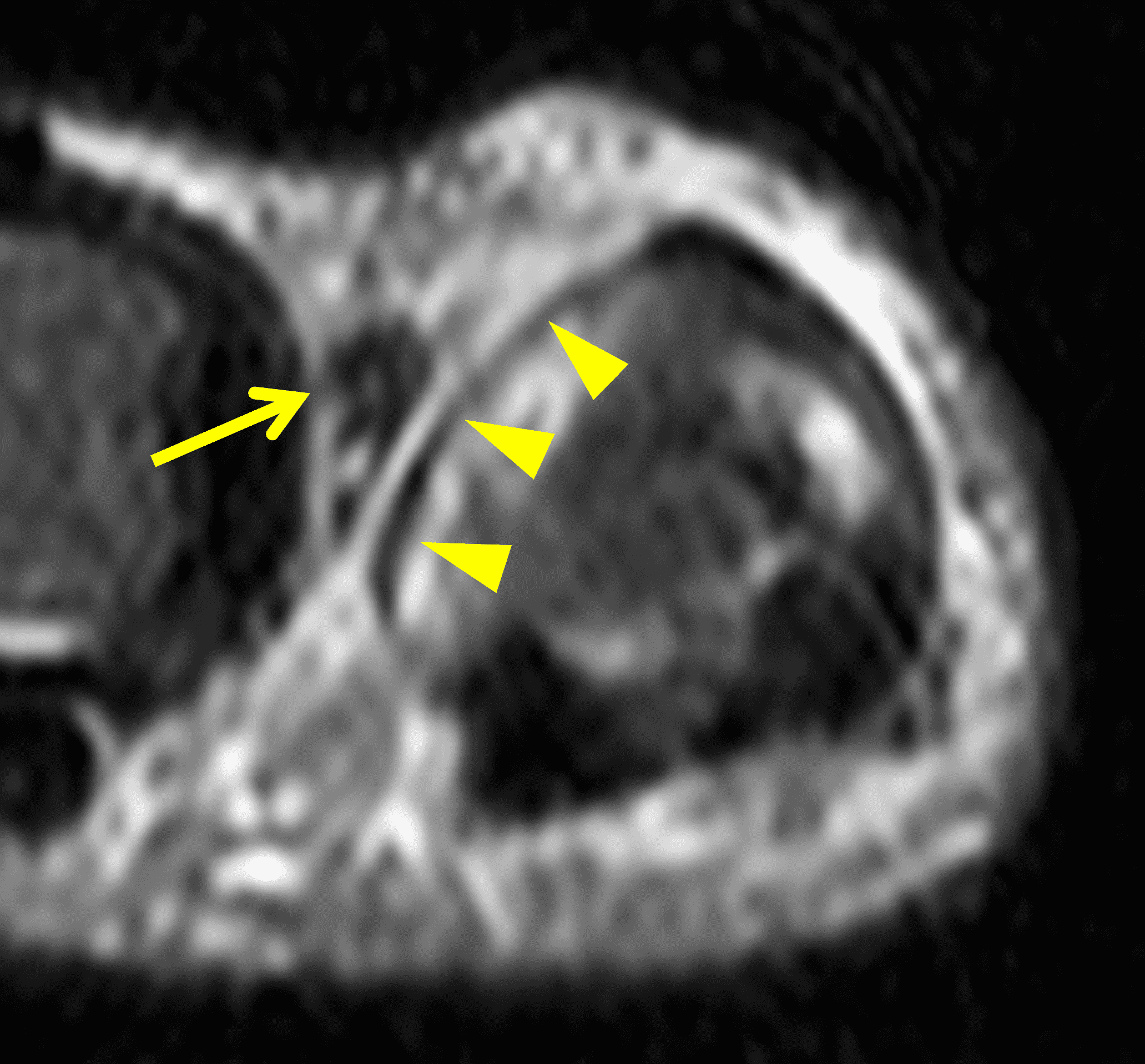
Figure 6: A 75-year-old presents with small finger MCP joint pain following a fall. (6A) A torn and radially displaced RCL (arrow) is evident on the STIR coronal image. (6B) The displaced ligament (arrow) clearly lies superficial to the radial sagittal band (arrowheads) on the corresponding STIR axial image.

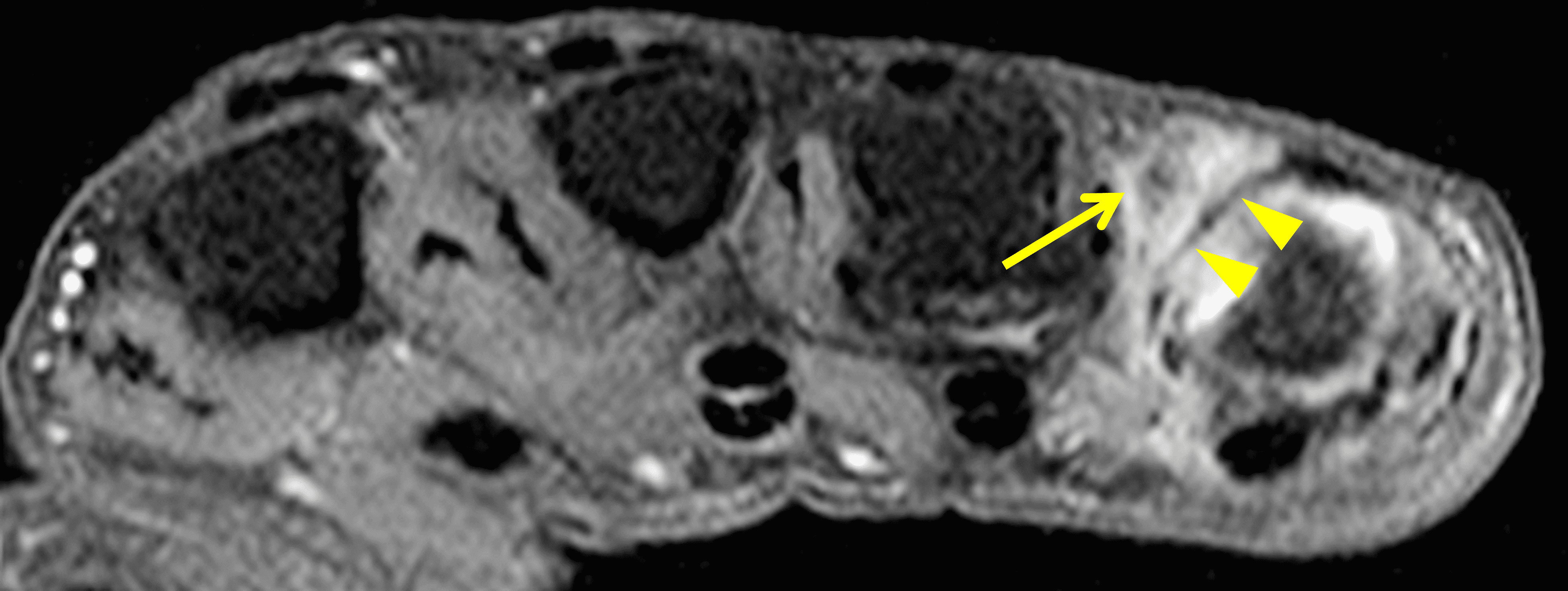
Figure 7: A 47-year-old man presents with complaints of a dorsal webspace mass 2 months following injury and with no relief from splinting. (7A) In the region of clinical concern, a low signal intensity nodular lesion is apparent (arrow) on the STIR axial image. (7B) Given the concern for a mass, intravenous contrast was administered. The subsequent fat-suppressed T1-weighted axial image reveals enhancing granulation tissue surrounding the “mass” (arrow), which lies superficial to the radial sagittal band (arrowheads). Complementary MR images and subsequent surgery confirmed that the mass represented a displaced RCL with a Stener-like lesion.
A unique example of a finger Stener-like lesion occurs in cases of extensor hood disruption at the proximal interphalangeal (PIP) joint. Rarely, the torn extensor hood can be displaced palmar to its typical location, in which case the resultant soft-tissue interposition leads to a non-reducible dislocation (Figure 8), most commonly seen at the PIP joint of the small finger.7



Figure 8: A 16-year-old boy presents with persistent pain and deformity at the small finger proximal interphalangeal (PIP) joint after a basketball injury two months prior. The patient had not improved despite splinting since the injury. (8A) A T1-weighted axial image through the proximal phalangeal neck demonstrates a tear of the extensor hood at its radial aspect with displaced tissue (arrow) from the hood lying palmar to the proximal phalanx. Compare to the intact extensor hood at the ring finger (arrowheads). (8B) A proton density-weighted sagittal image demonstrates the displaced tissue lying radial and palmar to its anatomic position (arrows). (8C) The adjacent slice shows pronounced palmar subluxation of the PIP joint, irreducible due to the soft tissue interposition (arrow), another indication for operative repair.
A rarely reported Stener-like lesion of the fingers can occur in cases of pulley tears, most commonly involving the A2 pulley. When an A2 pulley tear is complete, the torn tissue may become interposed between the flexor tendons and the typical palmar attachment site of the pulley (Figure 9), preventing healing with conservative therapy.

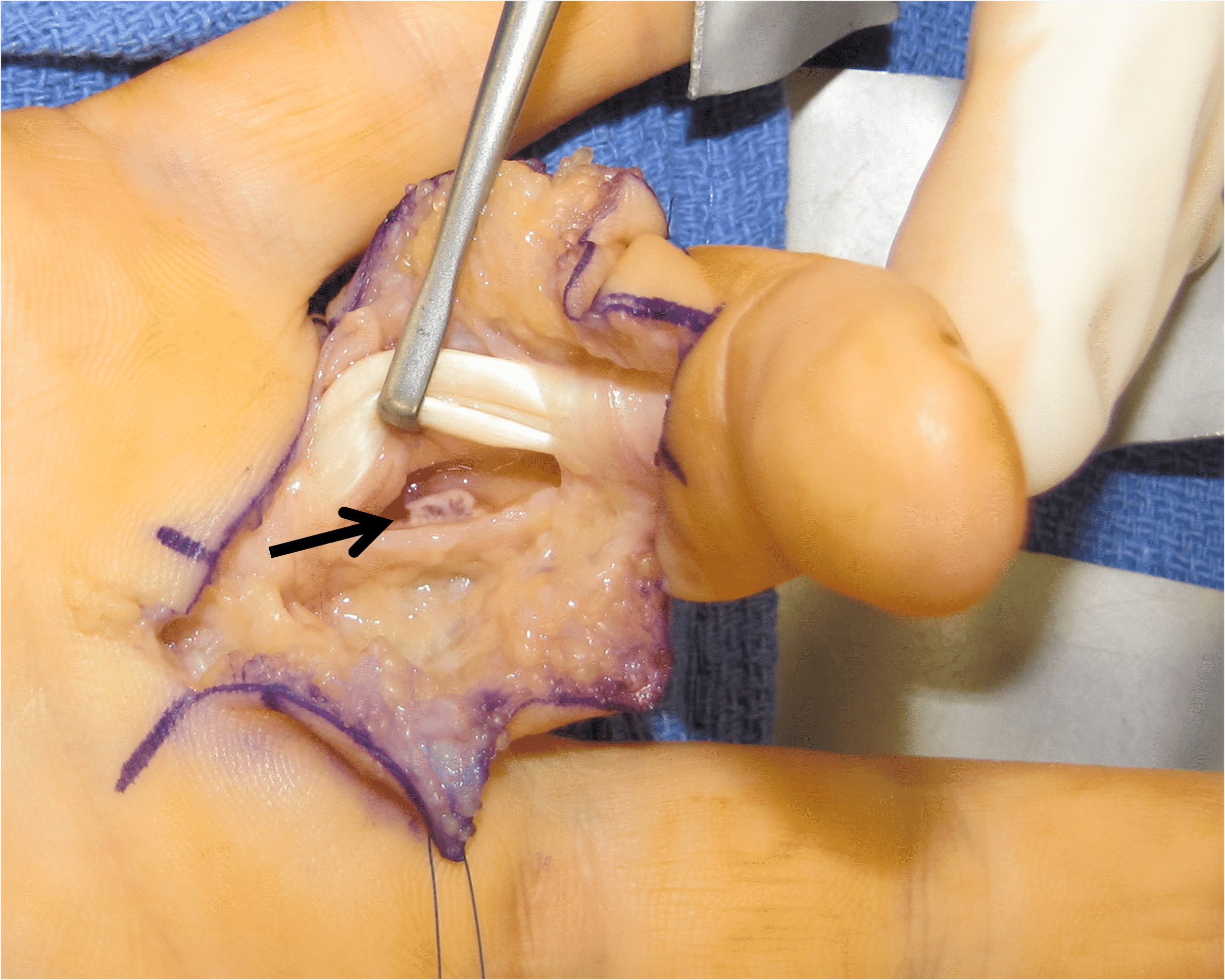
Figure 9: A 40-year-old man felt a pop in his ring finger while lifting a heavy box. (9A) An axial fat-suppressed T2-weighted image shows a portion of the torn A2 pulley interposed between the ring finger proximal phalanx and the palmarly displaced flexor tendons (t). (9B) At surgery, the torn pulley fragment (arrow) was revealed once the flexor tendons were elevated. Subsequent repair was done using a graft composed of retinacular tissue.
Stener-like lesion of the great toe
Stener-like lesions of the great toe are thought to be quite rare. A single reported case discusses findings involving the lateral collateral ligament (LCL) at the metatarsophalangeal (MT) joint of the great toe.8 This report described how the ruptured LCL became trapped by the extensor hood and the adductor tendon. The single available example in the Radsource files is of a Stener-like lesion of the great toe MT joint which involved the medial collateral ligament (Figure 10).
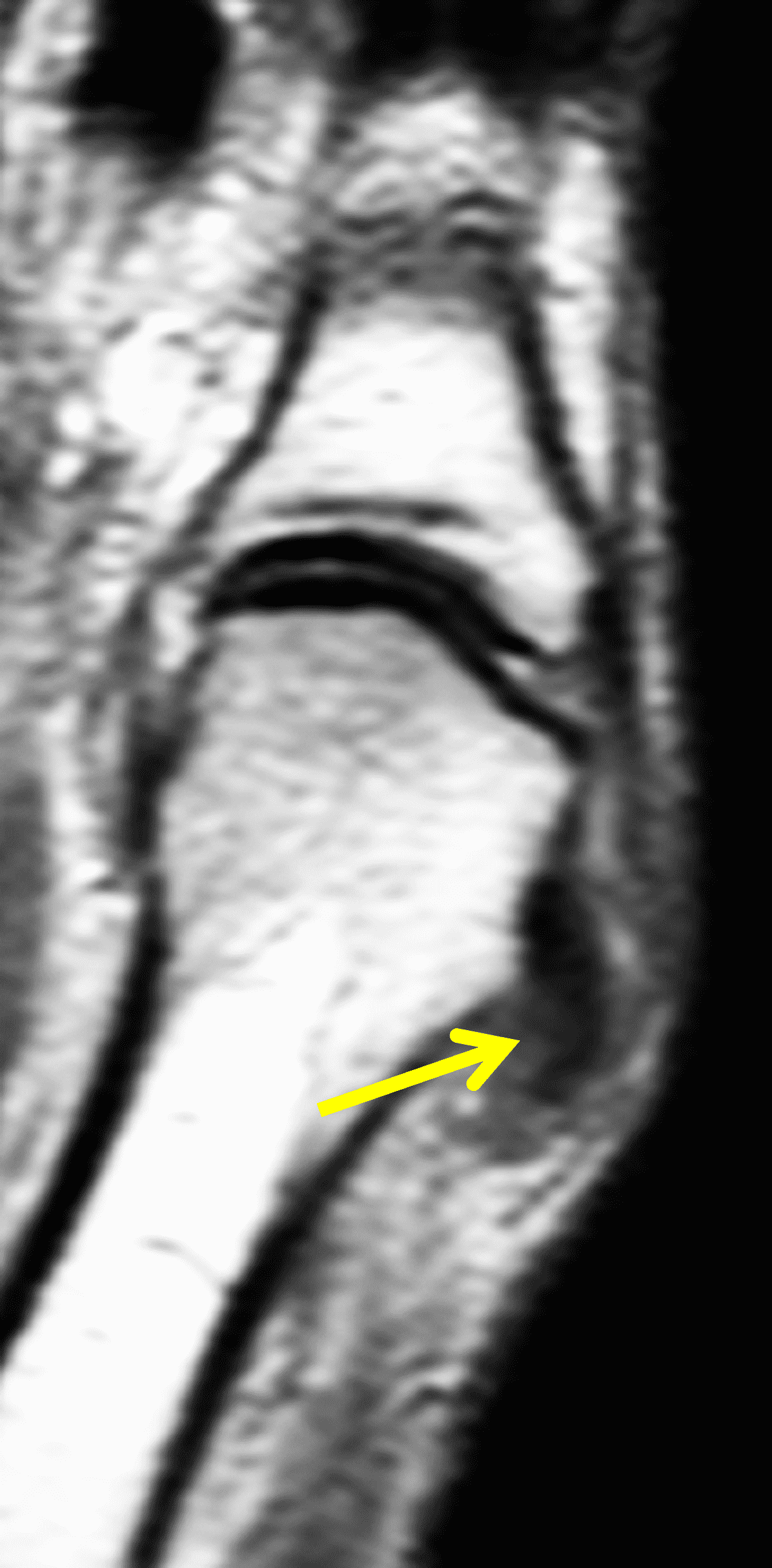


Figure 10: A 50-year-old woman presents with persistent great toe metatarsophalangeal (MP) joint pain 6 weeks following a fall down stairs. (10A) Proton density-weighted and (10B) STIR coronal images demonstrate complete tearing and retraction of the medial collateral ligament (MCL, arrows) adjacent to the metatarsal neck. (10C) The corresponding STIR axial image confirms the torn and retracted MCL (arrow), which lies proximal and superficial to the extensor hood (arrowheads). Such injuries are thought to require surgical repair.
Stener-like lesions beyond the digits:
Injuries of the medial collateral ligament complex of the knee are common. In cases of Grade 3 injuries (complete tears), the tibial collateral ligament may be stripped from its distal attachment. In some of these cases, the torn ligament is displaced to lie superficial to the pes anserine tendons (Figure 11).9 This configuration prevents anatomic healing with conservative management and is thus an indication for operative repair.10
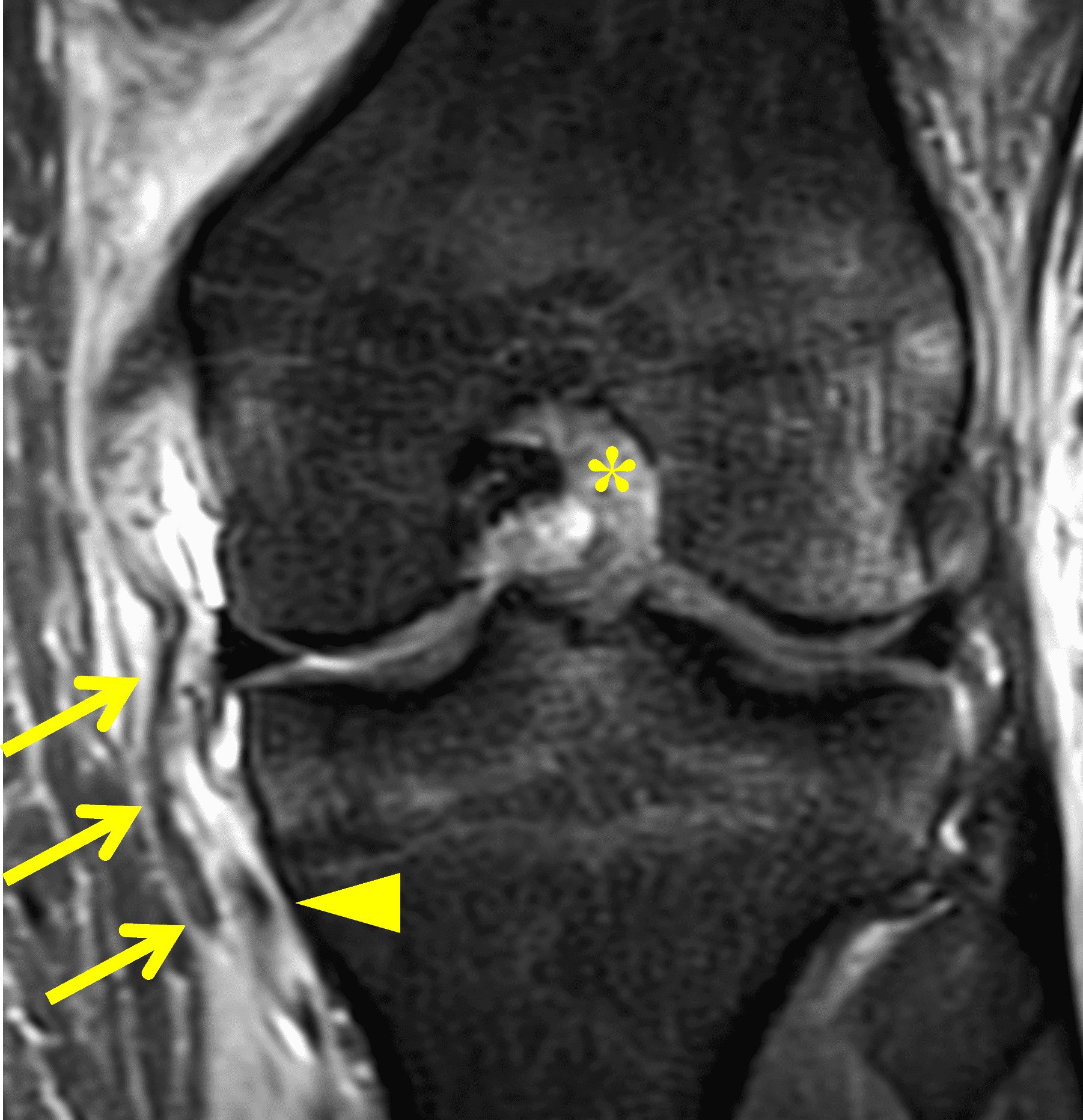
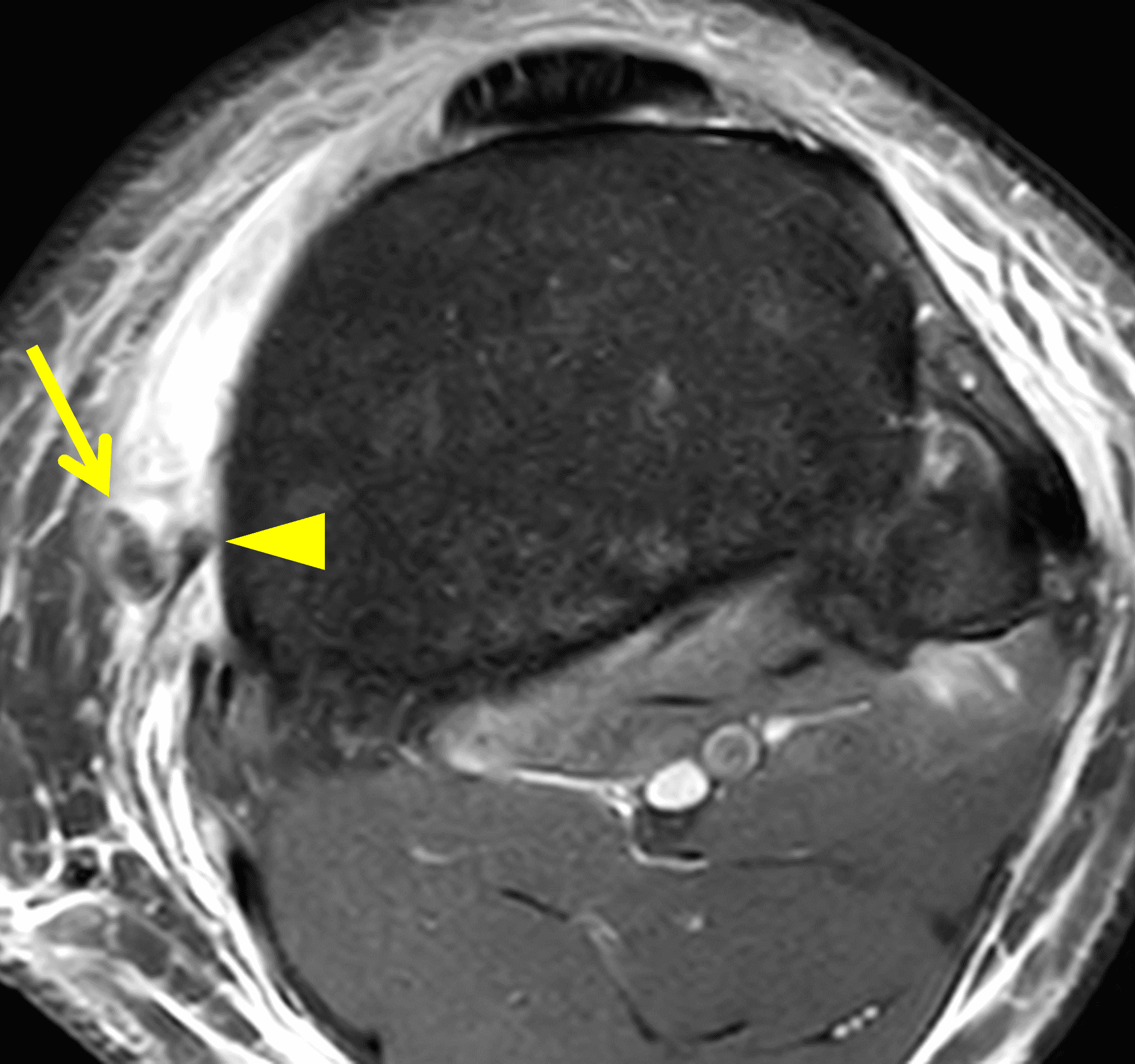
Figure 11: 17-year-old boy injured in a football game. Fat-suppressed proton density-weighted coronal (11A) and axial (11B) knee images show distal disruption and stripping of the tibial collateral ligament (arrows). The torn ligament lies superficial to sartorius tendon (arrowheads), preventing anatomic healing. A concurrent ACL tear (asterisk) is also visible on the coronal view.
In adolescent patients with Salter 1 or 2 type fractures, periosteum is frequently stripped along the distraction side of the injury. The stripped periosteum may then be displaced into the disrupted physis. Trapped periosteum is a known complication that prevents adequate fracture reduction and may result in premature physeal closure.11 Such abnormalities are most common at the distal femur (Figure 12), though trapped periosteum may occur at any physeal location. Other periarticular structures may also become entrapped, with reported abnormalities including the tibial collateral ligament, the pes anserine tendons, the deltoid muscle, the biceps tendon, the pronator quadratus muscle, and the posterior tibial tendon. The treatment for significantly trapped periosteum consists of open reduction and internal fixation of the fracture with removal of the entrapped periosteum.


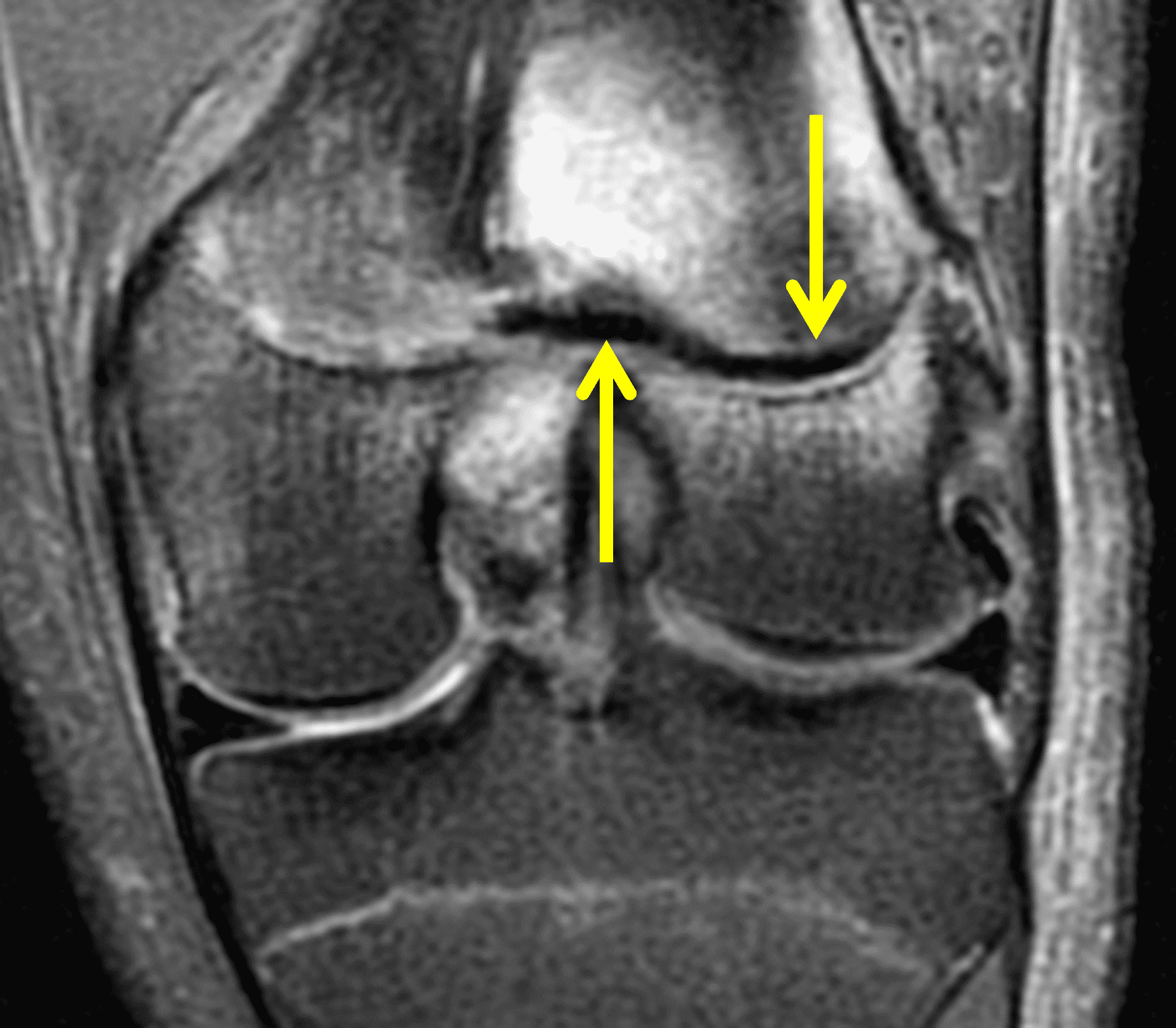
Figure 12: A 15-year-old boy presents with a distal femur Salter 2 fracture following a football injury. (12A) A fat-suppressed proton density-weighted axial image demonstrates extensive periosteal stripping along the distal femoral physis (arrowheads). An adjacent subacute hematoma (asterisk) is also present at a site where periosteum appears missing. (12B) A proton density-weighted sagittal image shows the entrapped periosteum (arrows) within the posterolateral physis. (12C) A fat-suppressed proton density-weighted coronal image also shows the entrapped periosteum (arrows) and associated marrow edema.
Extensor carpi ulnaris (ECU) subsheath injuries are very common, and often chronic injuries due to stripping of the subsheath are asymptomatic and are encountered incidentally on wrist MRI studies performed for other reasons. In the setting of acute subsheath tears, however, the tendon subluxation/dislocation is typically symptomatic with patients reporting immediate searing pain. Three typical patterns of ECU subsheath injury have been described.12 The most common pattern is a stripping pattern from the palmar attachment, resulting in a false pouch into which the tendon can chronically sublux. True subsheath ruptures are most often found along the ulnar side, in which case the tendon usually relocates beneath the subsheath. With radial sided subsheath tears, the tendon may relocate superficial to the residual subsheath (Figure 13), thus preventing anatomic healing and resulting in a Stener-like lesion.

Figure 13: Fat-suppressed proton density-weighted axial image from a 45-year-old after an acute tennis-related injury. The extensor carpi ulnaris tendon (asterisk) is subluxed in a palmar direction relative to the ulnar groove. The lax and edematous ECU subsheath components (arrowheads) lie along the floor of the ulnar groove and prevent anatomic relocation, compatible with an ECU subsheath Stener-like lesion.
Conclusion
In the over 60 years since the initial Stener lesion was described, our knowledge of anatomy and pathology in the musculoskeletal system has certainly grown, and many of radiology’s advances in this area have been fostered by the exquisite visualization of pathology provided by MRI. Numerous Stener-like abnormalities are now recognized and can be accurately diagnosed with MRI. It is exceedingly important to recognize Stener-like lesions, as they share a requirement for surgical repair, and delays in diagnosis and repair may result in long term patient morbidity.
References
- Campbell CS. Gamekeeper’s thumb. J Bone Joint Surg Br 1955 Feb;37-B(1):148-9. doi: 10.1302/0301-620X.37B1.148 ↩
- Tsiouri C, Hayton MJ, Baratz M. Injury to the ulnar collateral ligament of the thumb. Hand (NY) 2009;4(1):12-18. doi:10.1007/s11552-008-9145-8 ↩
- Beutel BG, Melamed E, Rettig ME. The Stener Lesion and Complete Ulnar Collateral Ligament Injuries of the Thumb A Review. Bull Hosp Jt Dis (2013). 2019 Mar;77(1):11-20. ↩
- Shin Y-E, Kim S-J, Kim J-S, Kwak K-Y, Kim J-H, Kim J-P. Efficiency of magnetic resonance imaging for diagnosing unstable ligament injuries around the thumb metacarpophalangeal joint: a comparison to arthroscopy. J Orthop Surg (Hong Kong) 2020 Sep-Dec;28(3):2309499020978308. doi: 10.1177/2309499020978308 ↩
- Carneiro BC, Araujo FF, Buimaraes JB, et al. Stener-like lesions in the hand, knee and foot: a review of anatomy, mechanism of injury and imaging evaluation. Clinical Imaging 2021 Aug;76:235-246. doi: 10.1016/j.clinimag.2021.05.001 ↩
- Ishizuki M, Sugihara T, Wakabayashi Y et al. Stener-like lesions of collateral ligament ruptures of the metacarpophalangeal joint of the finger. J Orthop Sci 2009 Mar;14(2):150-4. doi: 10.1007/s00776-008-1301-z ↩
- Ho WLS and Chew YCW. Irreducible radial dislocation of the proximal interphalangeal joint of a finger. Journal of Orthopaedics, Trauma and Rehabilitation 2015;19(1): 52-54. doi: 10.1016/j.jotr.2012.11.002 ↩
- Braspenningx S, Rezaie W, Simons P. Stener-like lesion of the lateral collateral ligament of the first metatarsophalangeal joint. Skeletal Radiol 2018;47(3):413-7. doi: 10.1007/s00256-017-2790-7 ↩
- Brimmo OA, Senne JA, Crim J. MRI findings of Stener-like lesion of the knee: a case series with surgical correlation. Eur J Radiol 2019 Dec;121:108709. doi: 10.1016/j.ejrad.2019.108709 ↩
- Keyhani S, Mardani-Kivi M. Anatomical repair of Stener-like lesion of medial collateral ligament: a case series and technical note. Arch Bone Jt Surg 2017;5(4): 255-8. ↩
- Barmada A, Gaynor T, Mubarak SJ. Premature physeal closure following distal tibia physeal fractures: a new radiographic predictor. J Pediatr Orthop 2003 Nov-Dec;23(6):733-9. doi: 10.1097/00004694-200311000-00010 ↩
- Inoue G, Tamura Y. Surgical treatment for recurrent dislocation of the extensor carpi ulnaris tendon. J Hand Surg Br 2001 Dec;26(6):556-9. doi: 10.1054/jhsb.2001.0615 ↩
