Clinical History
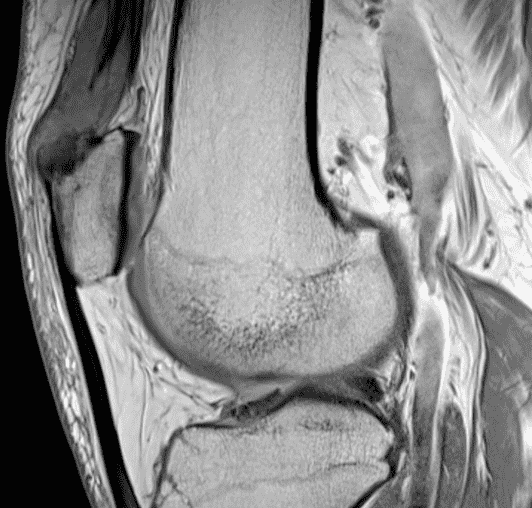
A 65 year-old-man presents with a palpable mass in the anterior knee and generalized pain. Sagittal (1A) fat-suppressed T2-weighted and (1B) proton density-weighted images are shown. What are your findings? What is your diagnosis?

Findings
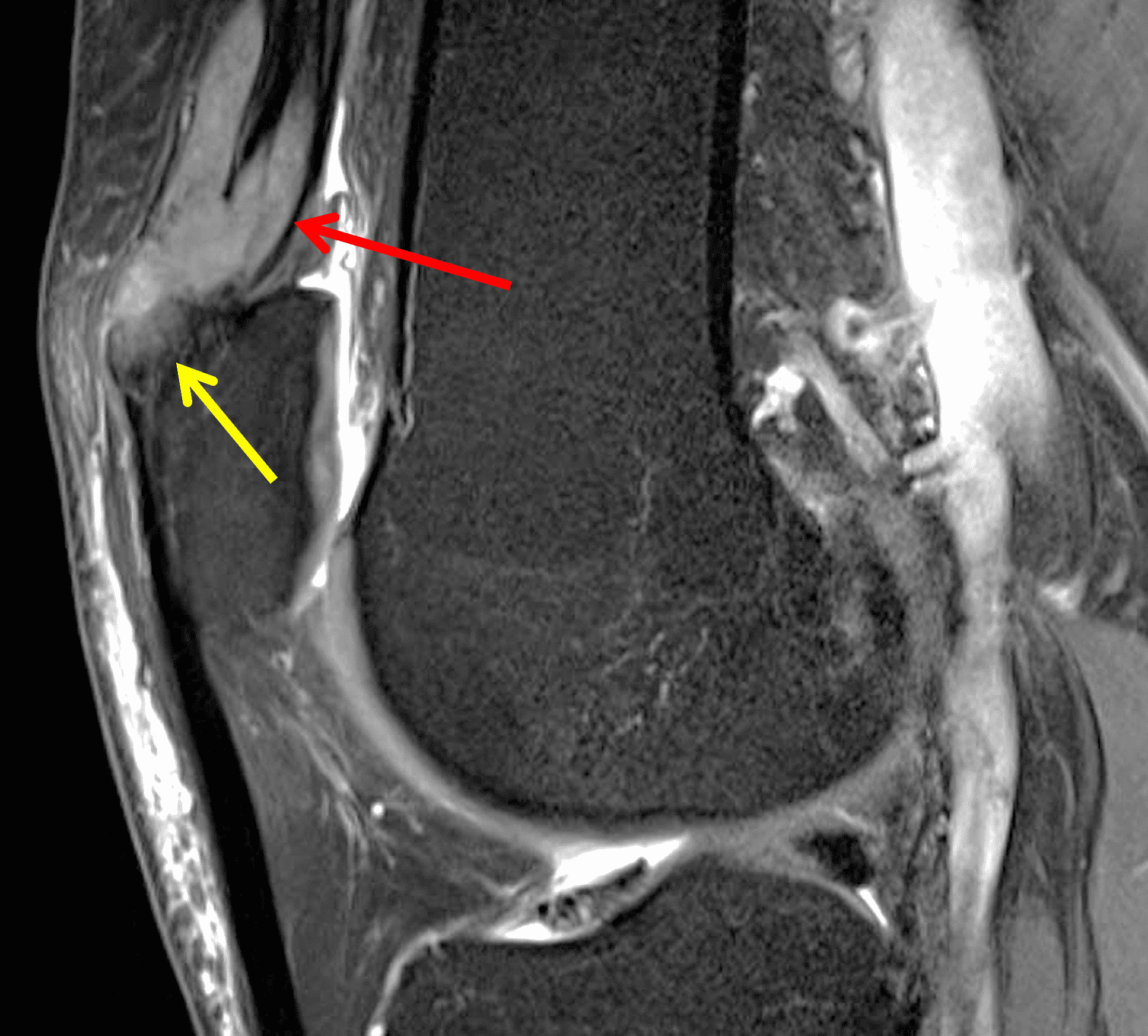
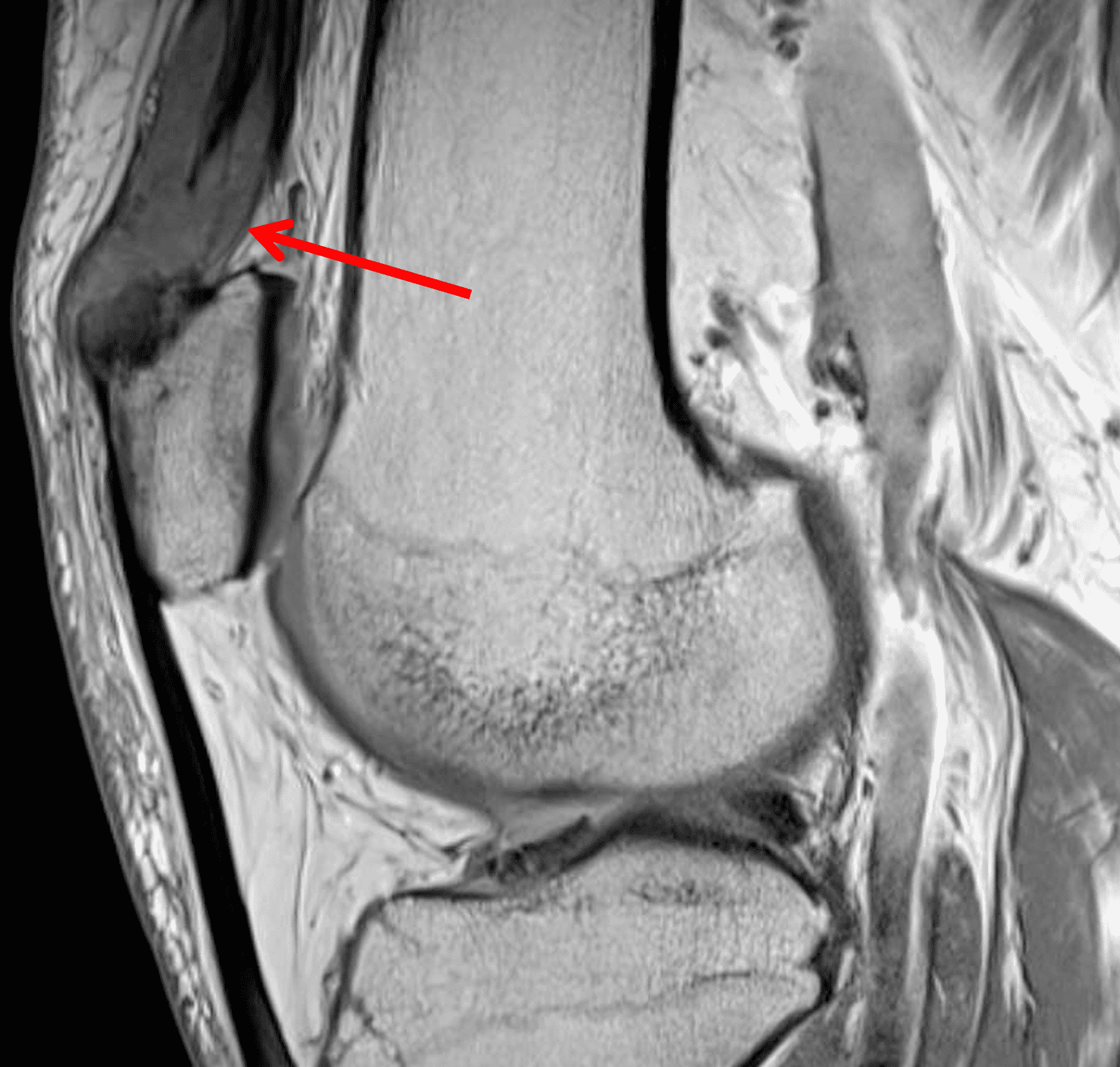
Figure 2: An ill-defined, infiltrative mass superficial to and involving most of the distal quadriceps tendon (red arrows) has intermediate signal on the fat-suppressed fluid-sensitive (2A) and proton density-weighted (2B) images, with faint marrow edema in the adjacent patella (yellow arrow).
Diagnosis
Tophaceous gout.
Introduction
Intra-articular and peri-articular masses are commonly encountered on imaging and encompass many localized and diffuse processes. These include benign and malignant tumors as well as infectious and non-infectious, non-neoplastic synovial proliferative conditions. While most intra-articular processes are benign, malignant entities rarely do occur within the joint and should be considered in the right scenarios. The etiology of some lesions will be indeterminate on imaging and require tissue sampling; however, many lesions have a characteristic appearance, especially on MRI, due to its excellent soft tissue contrast and its ability to reliably delineate the anatomic location and origin of the mass. This information, along with radiography and clinical history, can help arrive at a specific diagnosis or a short differential diagnosis confidently, greatly aiding clinical management. When evaluating an articular process, the entities can be divided into focal and diffuse processes.1,2,3,4
Relevant Anatomy
Diarthrodial joints consist of articulating hyaline cartilage and a surrounding fibrous/ligamentous capsule. An inner synovial lining covers the majority of the joint. In more complex joints such as the knee, additional structures such as fat pads, bursae, recesses, fibrocartilage, and tendons may also be intra-articular and as such can be a source of intra-articular pathology.1-4
Diffuse Processes
Tenosynovial Giant Cell Tumor, Diffuse Type
Tenosynovial giant cell tumor (TSGCT, previously called pigmented villonodular synovitis and giant cell tumor of the tendon sheath) is a locally aggressive mesenchymal neoplasm arising from joints, bursae and tendon sheaths. It is characterized by aberrations in CSF1, which is not a requirement for pathologic diagnosis.5,6 TSGCTs are divided into localized (nodular) and diffuse types. Unlike the local type, the diffuse form demonstrates extensive infiltration of the synovium and can extend through the joint capsule into the extra-articular tissues; hemarthrosis and joint destruction. Diffuse type TSGCT most commonly involves the knee, ankle and hip, typically in the third and fourth decades of life, with slight female predilection. Local recurrences after treatment are more common compared to the focal type. While not fatal, diffuse type TSGCT may cause significant morbidity. Malignant TSGCT (and metastases) are very rare and can occur de novo or following multiple recurrences of conventional TSGCT.5
The treatment for diffuse type TSGCT is evolving, with medical therapies starting to play a larger role. Standard treatment is arthroscopic or open synovectomy, if it can be accomplished without significant morbidity. However, surgery is generally associated with high risk and complications, including risk of recurrence, especially if entirely clearing the tumor burden is not possible. Arthroplasty is considered in the presence of advanced osteoarthrosis. In cases where surgery is not a good option, systemic therapy in the form of CSF1R inhibitors can be used. Radiotherapy in various settings and cryotherapy have also been described.5
Patients may present with pain, swelling and limited range of motion.1 Radiographic findings are nonspecific, and are primarily used to exclude calcifications, which are exceedingly rare in TSGCT. Other diagnoses should be pursued if calcifications are present, including primary synovial chondromatosis and synovial sarcoma.1,5
MRI demonstrates lobular mass-like synovial proliferation with scattered areas of hemosiderin deposition, which is usually intermediate to hypointense on all sequences, with variable post-contrast enhancement (Figure 3).1-3 Blooming artifact can also be seen on gradient echo sequences due to hemosiderin deposition, which is the result of recurrent tumoral bleeding and hemarthrosis, although the lack of this finding does not exclude TSGCT. Additionally, other synovial processes such as hemophilic arthropathy and synovial hemangioma can also demonstrate hemosiderin deposition. The clinical history is usually sufficient to differentiate hemophilic arthropathy and the presence of prominent vascular channels can help distinguish synovial hemangiomas.1,2 Inflamed synovium may demonstrate T2 hyperintensity and enhancement following intravenous contrast administration.1-3,5 Uncommonly, areas of intra-lesional fat with T1 hyperintensity may be present.7 Erosions may be seen, usually in small joints or those with a tight joint capsule, such as the hip. A joint effusion is usually present.1
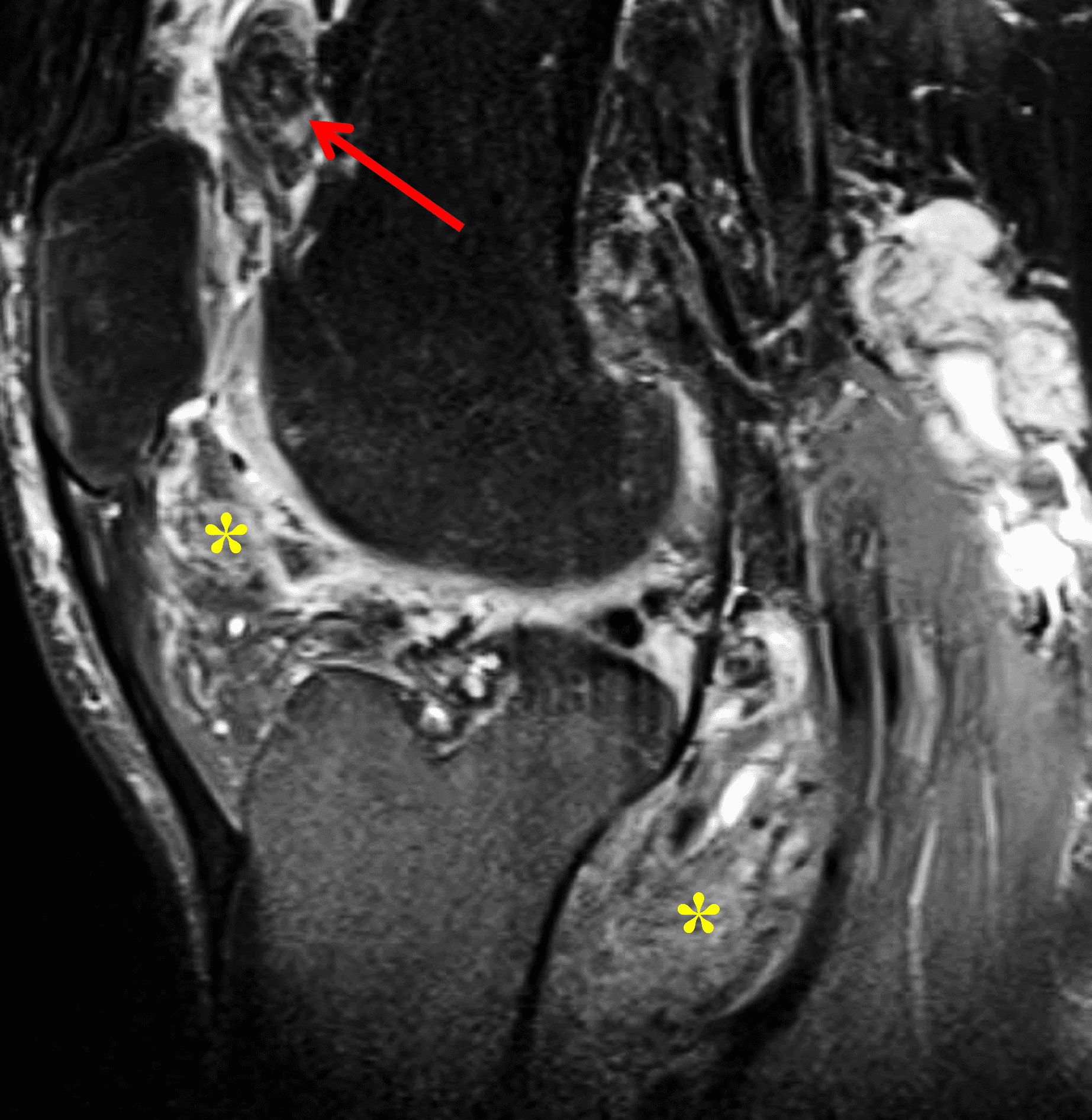
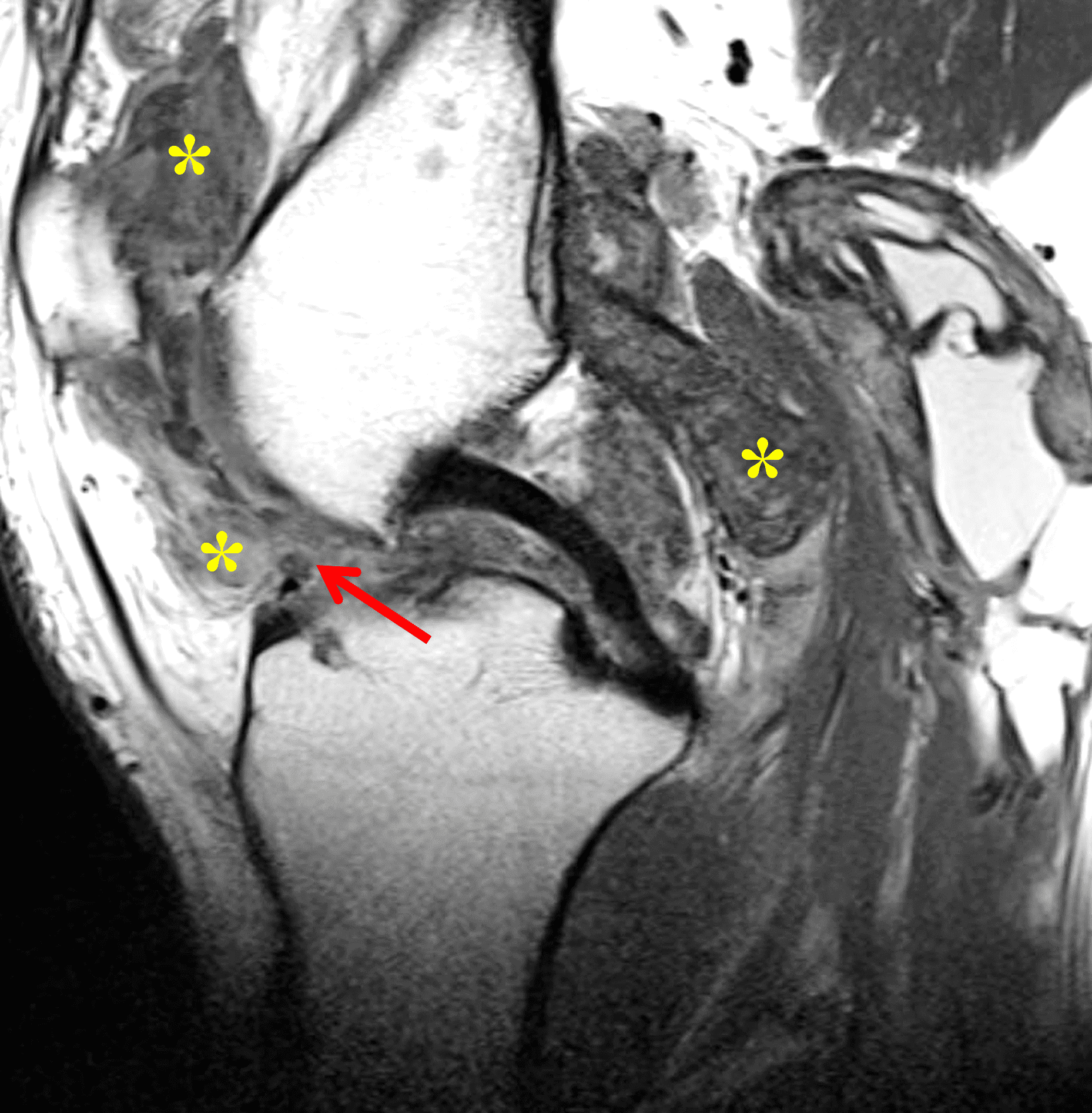

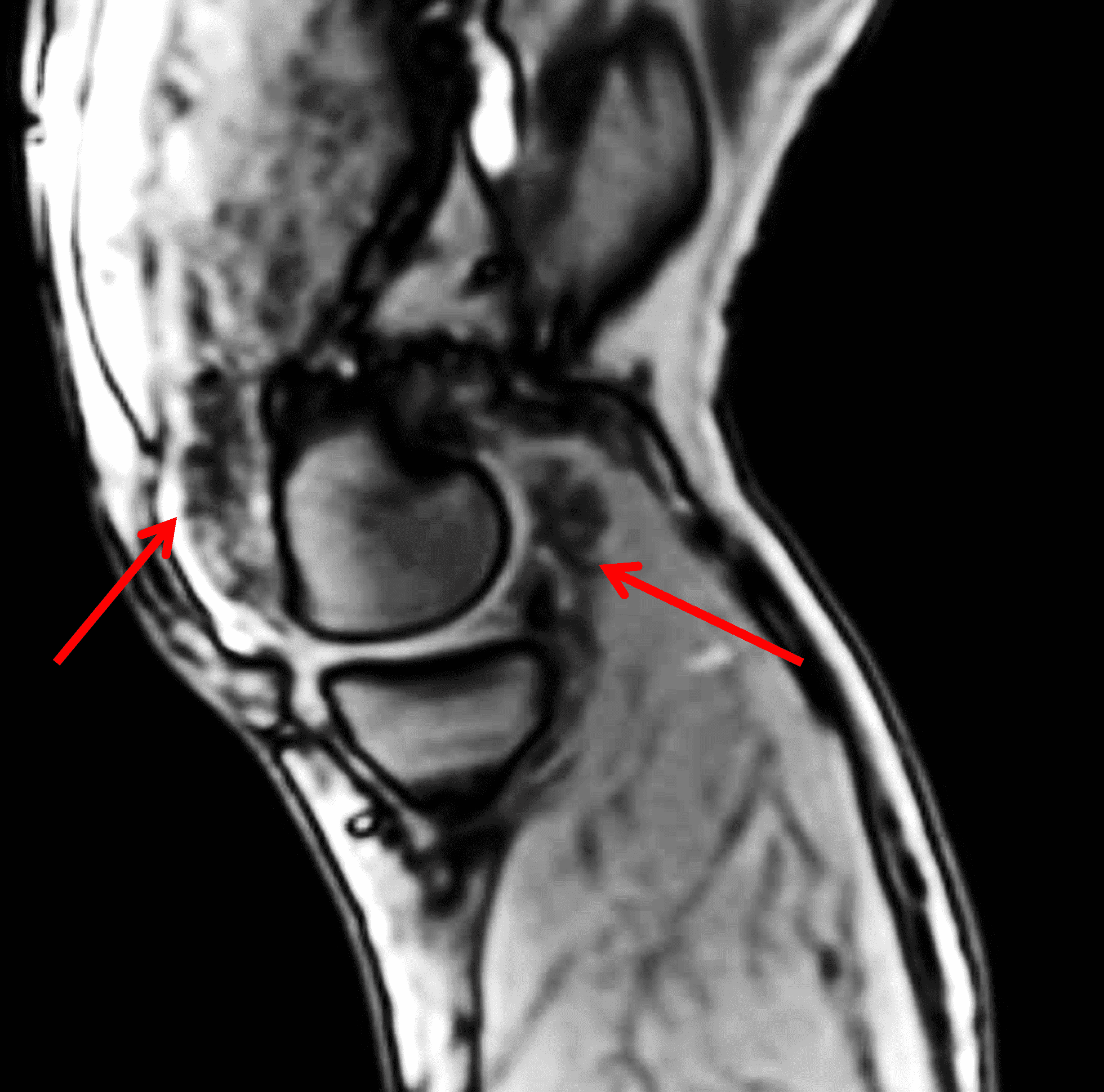
Figure 3: Diffuse type tenosynovial giant cell tumor in the knee. (3A) Sagittal fat-suppressed T2-weighted, (3B) sagittal proton density-weighted, and (3C) coronal T1-weighted images demonstrate diffuse mass-like synovial proliferation in the anterior and posterior joint space including the suprapatellar recess, with intermediate-to-hypointense signal on all pulse sequences (asterisks). Very low signal intensity foci represent hemosiderin deposition (arrows). (3D) A sagittal gradient echo localizer image shows “blooming” artifact from the hemosiderin (arrows).
Primary and Secondary Synovial (Osteo)chondromatosis
Primary synovial chondromatosis is a rare, benign, locally-aggressive neoplastic process characterized by proliferation of hyaline cartilage nodules within the synovial lining of a joint, bursa or tendon sheath.8 It occurs most commonly in the knee, followed by the hip and elbow.1,8 The cartilaginous nodules can enlarge, break from the synovium and become intra-articular bodies, which may calcify and ossify in later stages (primary synovial osteochondromatosis).1 Secondary synovial osteochondromatosis is a term sometimes used to describe multiple intra-articular bodies within a joint due to advanced osteoarthrosis or sequelae of other joint insult (Figure 4).1 It is more common in men, usually occurs in the third to fifth decades, and can present with pain, swelling and limited range of motion.2
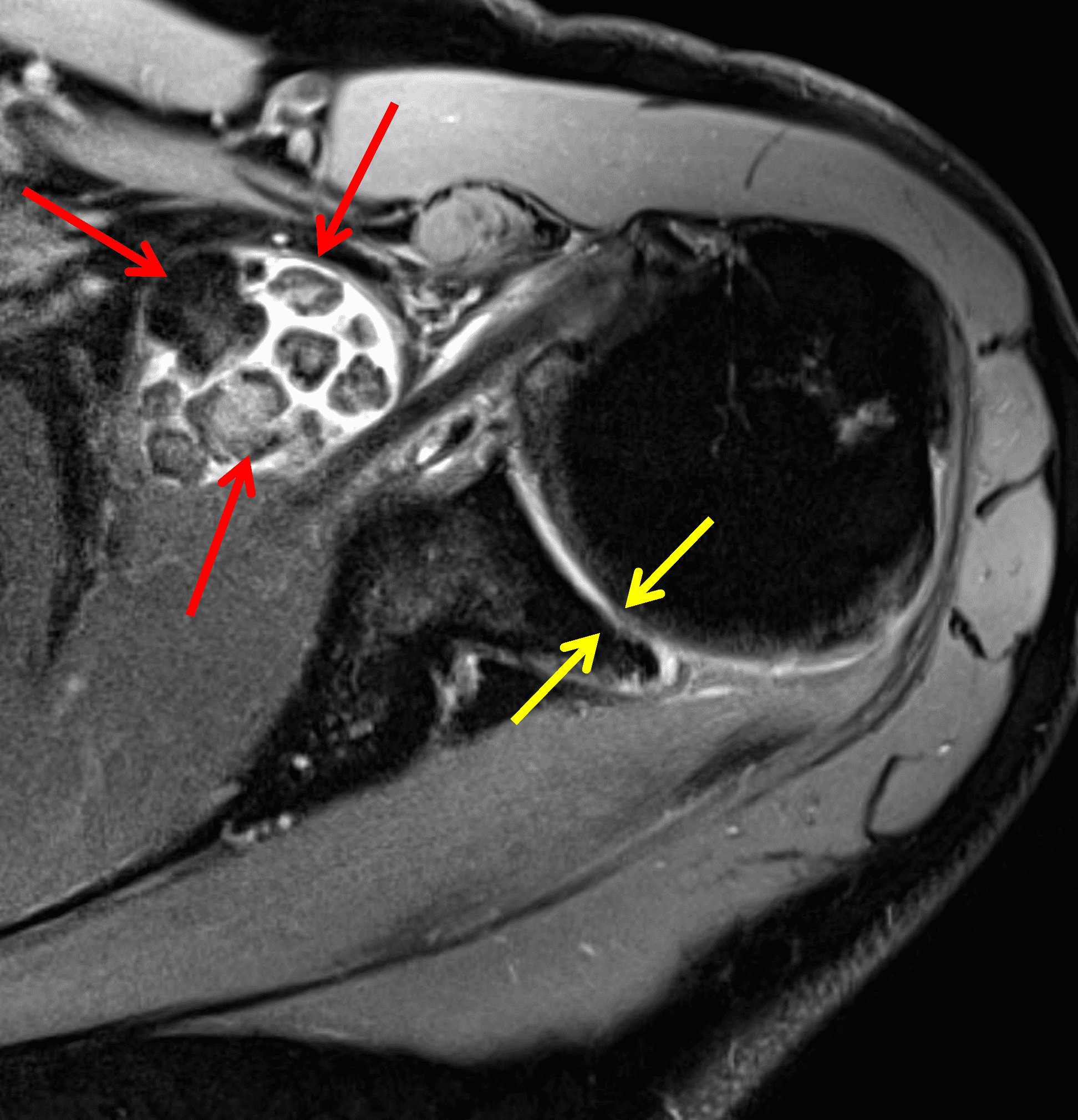
Figure 4: Secondary osteochondromatosis (loose bodies) in the shoulder joint. An axial fat-suppressed T2-weighted image shows multiple intra-articular bodies of variable size (red arrows) and severe glenohumeral cartilage (yellow arrows) due to osteoarthrosis.
In primary synovial chondromatosis, the MR imaging characteristics depend on the mineralization pattern of the lesions. In one study, the most common imaging pattern by far demonstrated isointense to hyperintense T1 signal and hyperintense T2 signal with internal areas of T2 hypointensity corresponding to calcification, followed by isointense to hyperintense T1 and hyperintense T2 signal without internal T2 hypointensities, and finally internally fat signal foci with a peripheral hypointense rim corresponding to endochondral ossification.1,9 Calcification is reported in up to 75-95% of cases, and erosions can also be seen.1 With intravenous contrast, thin peripheral and septal enhancement is seen in typical chondroid lesions.2 When mineralized, the radiographic and CT appearance is very characteristic, demonstrating ring and arc calcifications within the bodies (Figures 5 and 6). Primary synovial chondromatosis can be differentiated from secondary synovial osteochondromatosis by the presence of a greater number and more uniform size bodies in the former, and the presence of advanced osteoarthritis in the latter. Treatment of primary synovial chondromatosis includes removal of the intra-articular bodies with or without synovectomy.1

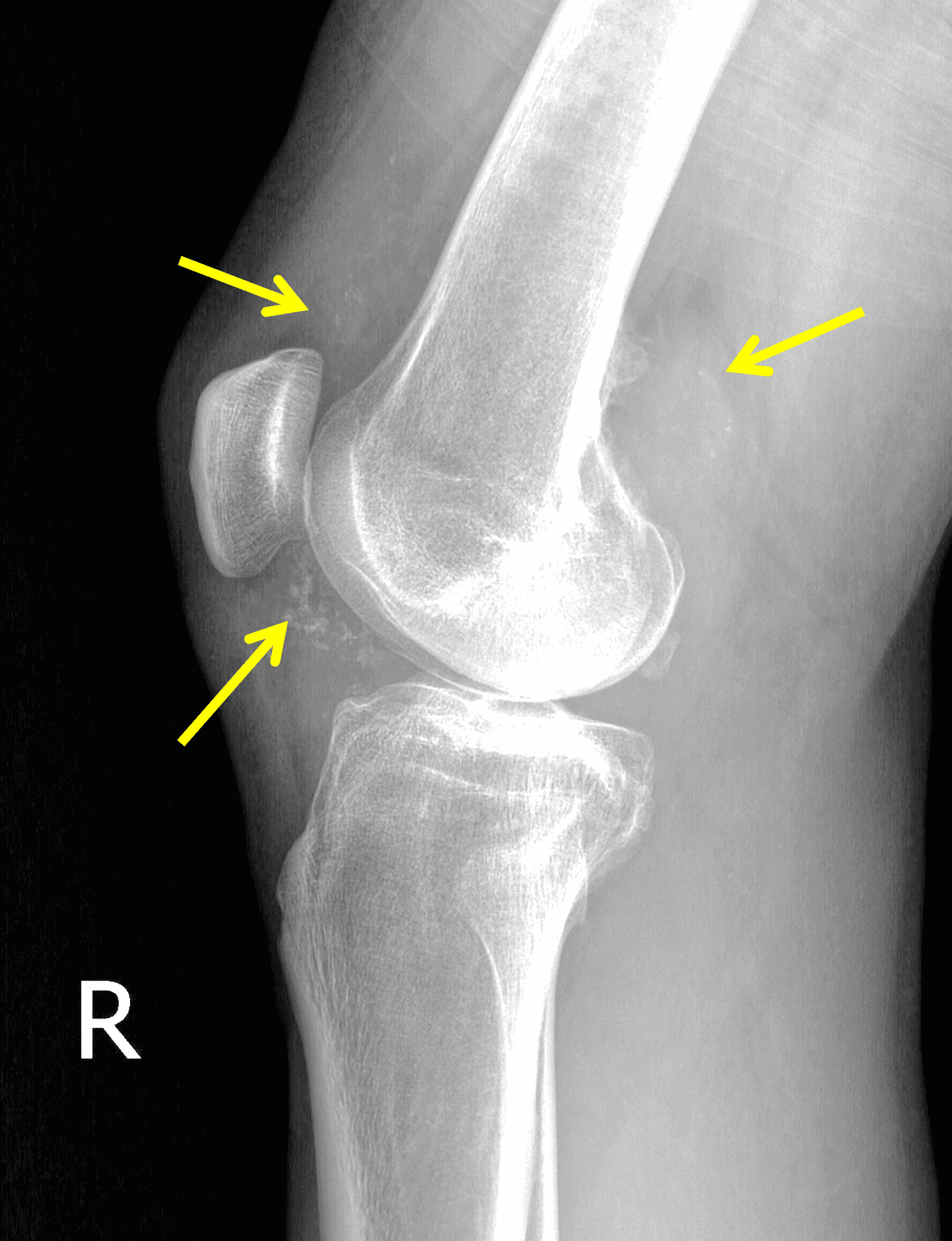
Figure 5: Primary synovial chondromatosis in the knee joint. (5A) Sagittal fat-suppressed, fluid-sensitive image demonstrates diffuse, heterogeneous intermediate and hyperintense signal synovially-based masses throughout the joint (asterisks). (5B) Lateral radiograph shows corresponding faint “ring and arc” calcifications (arrows).
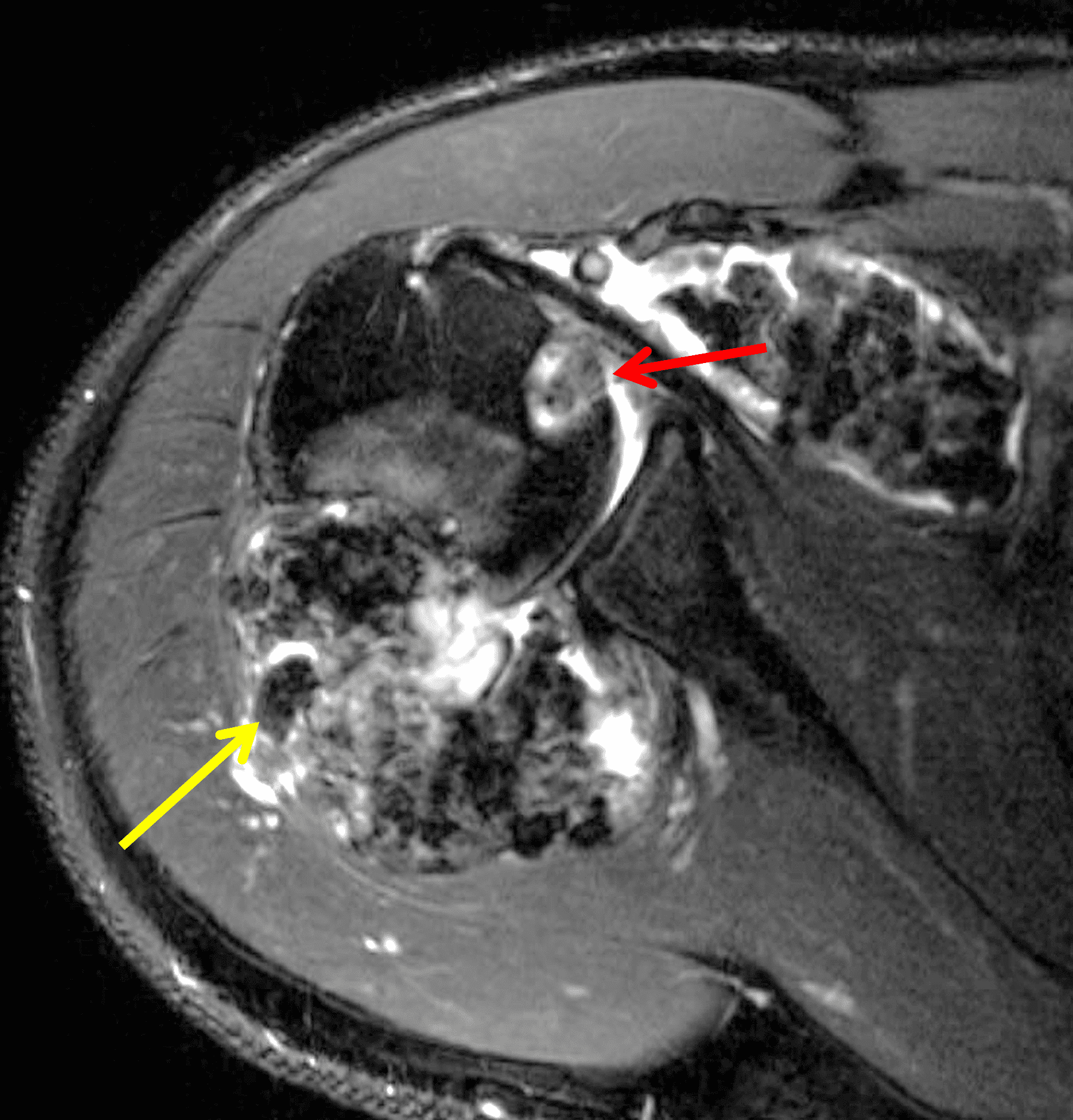


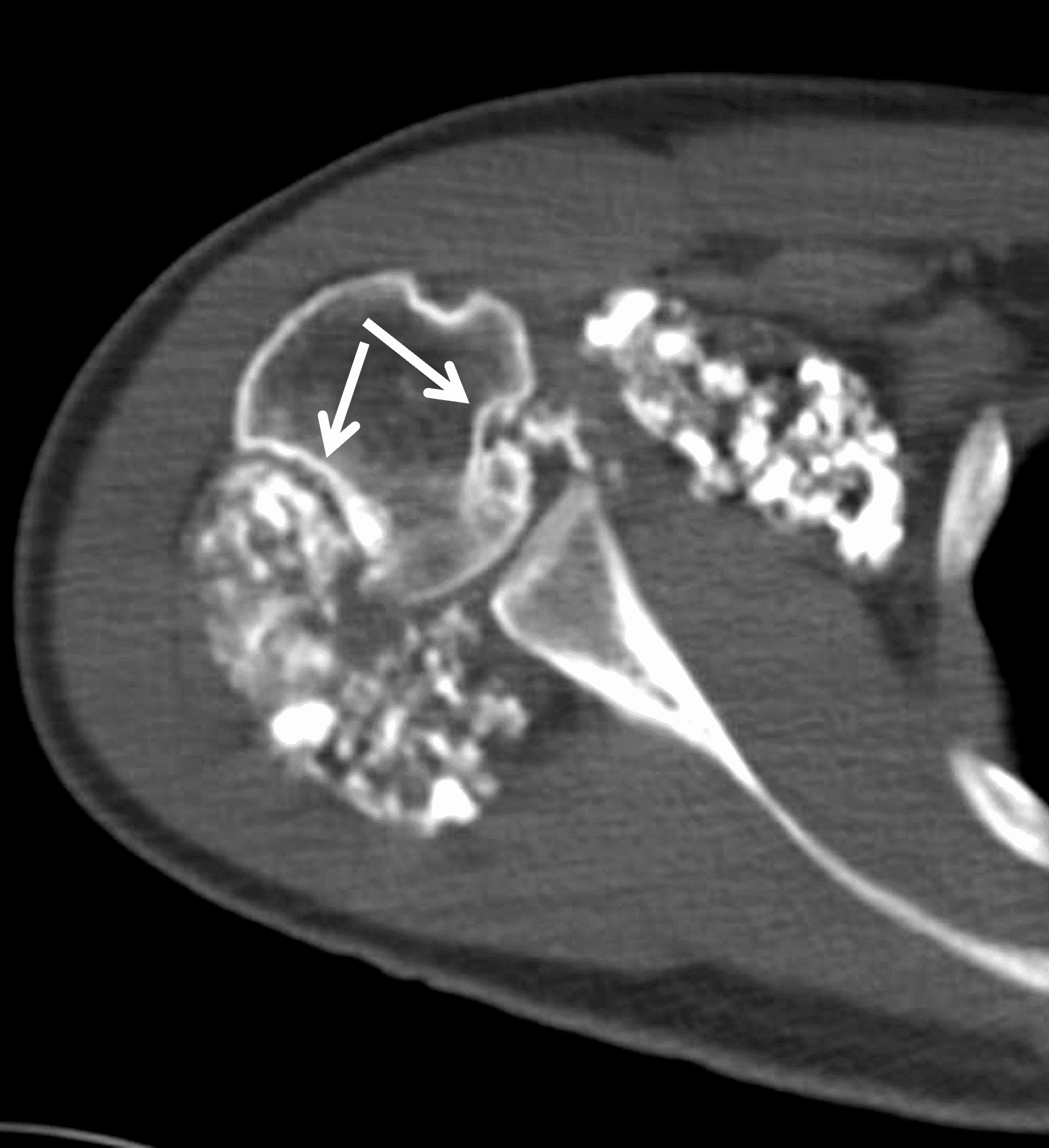
Figure 6: Primary synovial chondromatosis in the shoulder joint. Fat-suppressed fluid-sensitive (6A) axial and (6B) sagittal images, and (6C) sagittal T1-weighted image demonstrate diffuse, lobulated synovially-based heterogeneous masses. T2 hyperintense and intermediate T1 signal areas reflect chondroid matrix (red arrows). T1 and T2 hypointense foci reflect calcification (yellow arrows). T2 hypointense and T1 hyperintense foci reflect areas of endochondral ossification (blue arrows). (6D) Axial CT image shows calcification and ossification in the synovial masses, as well as osseous erosions (arrows).
Synovial Chondrosarcoma
Synovial chondrosarcoma can arise de novo, or more commonly due to malignant transformation of primary synovial chondromatosis,10 which is estimated to occur in 2.5% of cases. Synovial chondrosarcoma is most common in the hip joint, and clinically behaves as a locally aggressive, recurring tumor.11,12 It may be difficult to differentiate between primary synovial chondromatosis and synovial chondrosarcoma but a few imaging features are suggestive of chondrosarcoma (Figure 7). While primary synovial chondromatosis can involve bone by pressure erosion, when synovial chondrosarcoma involves bone it appears more aggressive, invading the marrow and permeating the trabecular bone. Widespread extension beyond the joint capsule with invasion into the soft tissues also suggests malignancy, which is confirmed if distant metastases occur.12
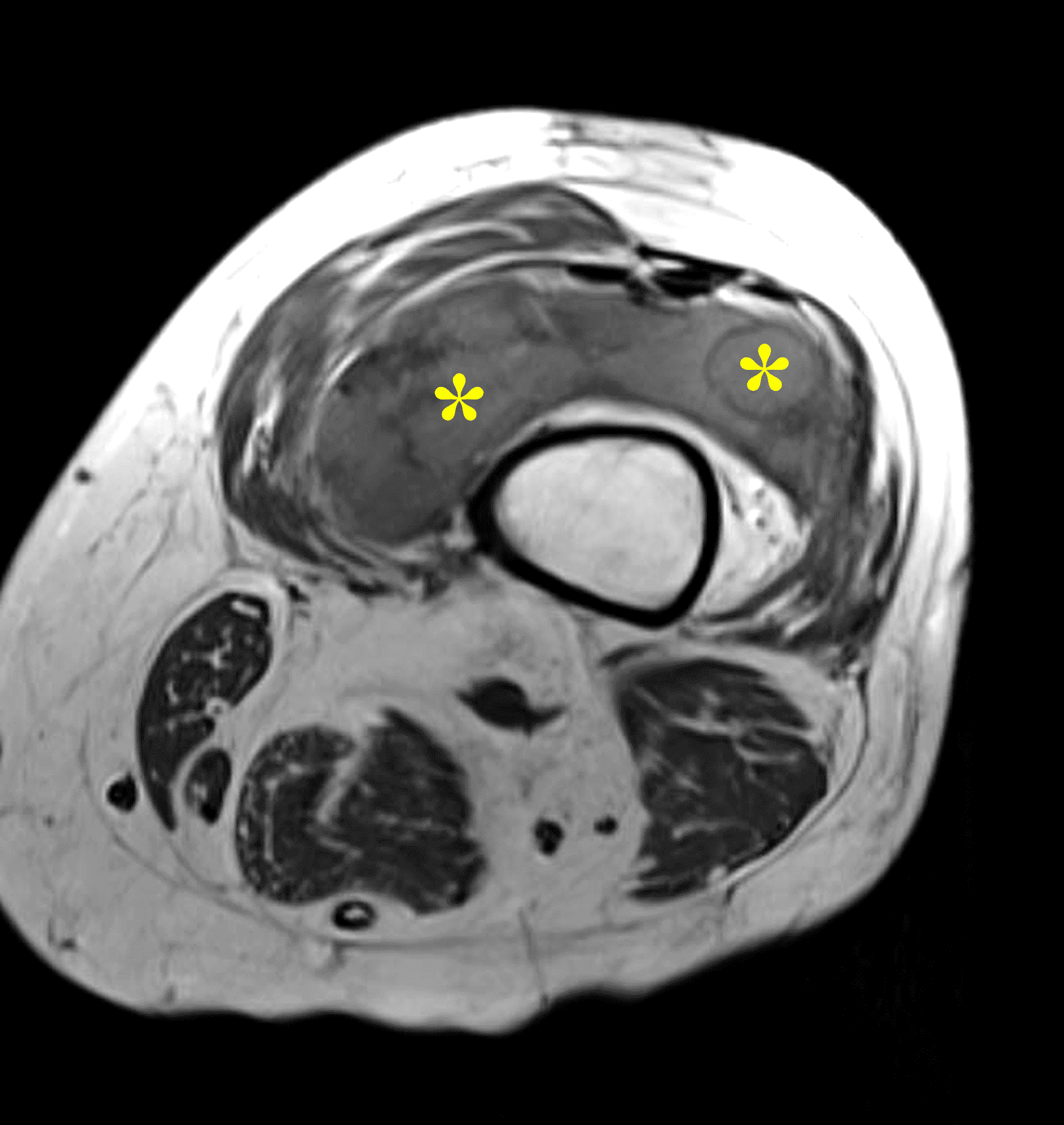
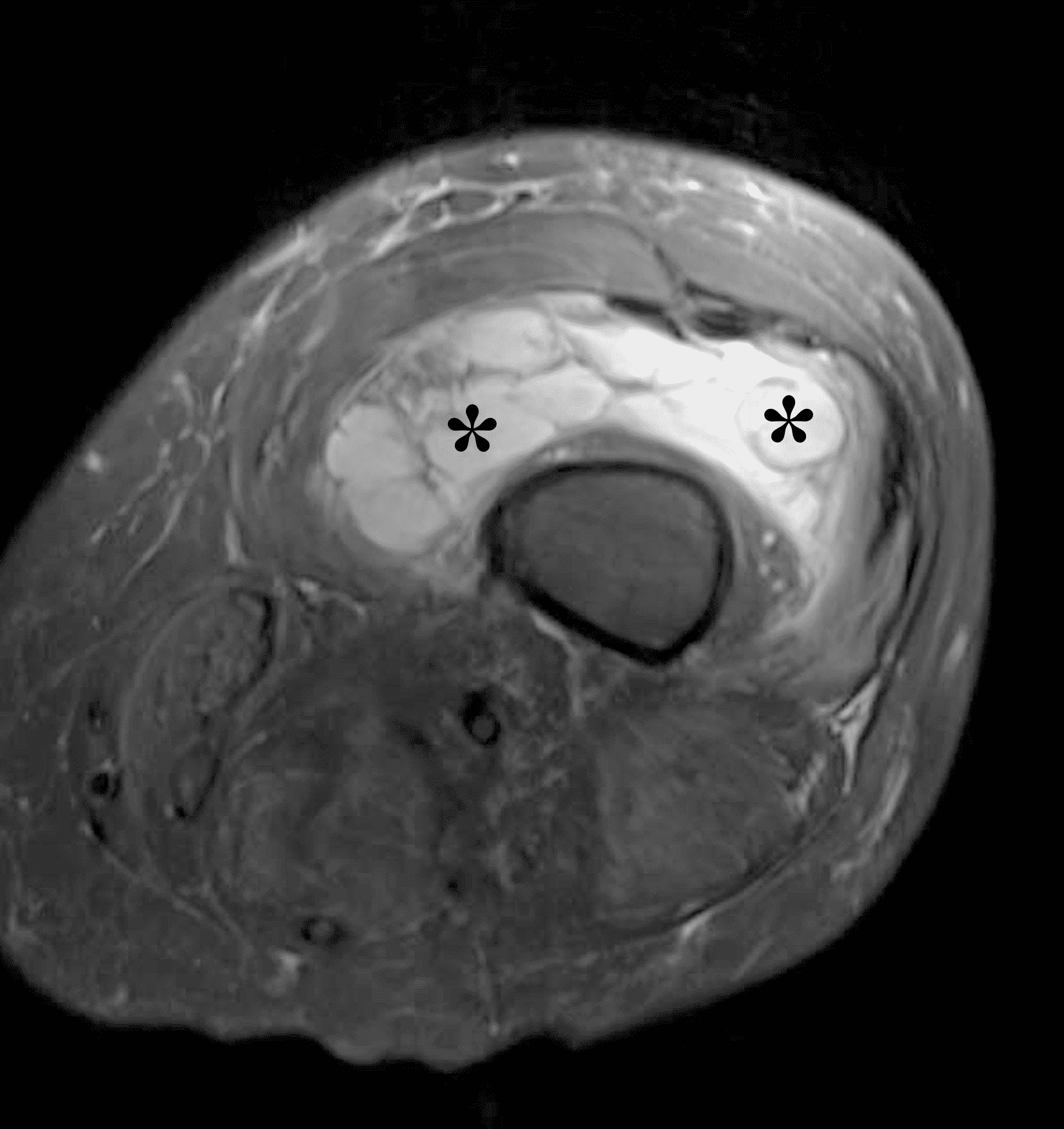
Figure 7: Synovial chondrosarcoma in the knee joint. Axial (7A) T1-weighted and (7B) fat-suppressed water-sensitive images show a multinodular, synovial mass (asterisks) in the suprapatellar recess, mildly hyperintense compared to skeletal muscle. This example shows no bone invasion or extra-articular spread, so diagnosis required histologic confirmation.
Lipoma Arborescens
Lipoma arborescens is a rare non-neoplastic process consisting of villous proliferation of the synovium and replacement of subsynovial tissue with mature adepocytes.1–4,13,14 It is most commonly a reactive process due to traumatic or inflammatory stimuli such as osteoarthrosis or inflammatory arthritis. Very rarely, primary forms have been described without underlying joint pathology. While lipoma arborescens can occur in any synovial lining, it is usually monoarticular and most commonly involves the suprapatellar recess of the knee. It usually presents in the fifth to seventh decades and has a male predilection.1-4,13-15 Patients may present with painless swelling and recurrent joint effusions. Management is usually conservative, but if necessary synovectomy can be performed without recurrence.
Radiographs are usually nonspecific but can demonstrate arthritic changes, swelling, effusion and occasionally fatty hypodensities. MRI findings demonstrate frondlike or villous synovial proliferation with fat signal on all sequences, and the presence of a joint effusion (Figure 8).1-4,13-15 Osseous erosions have also been reported.15
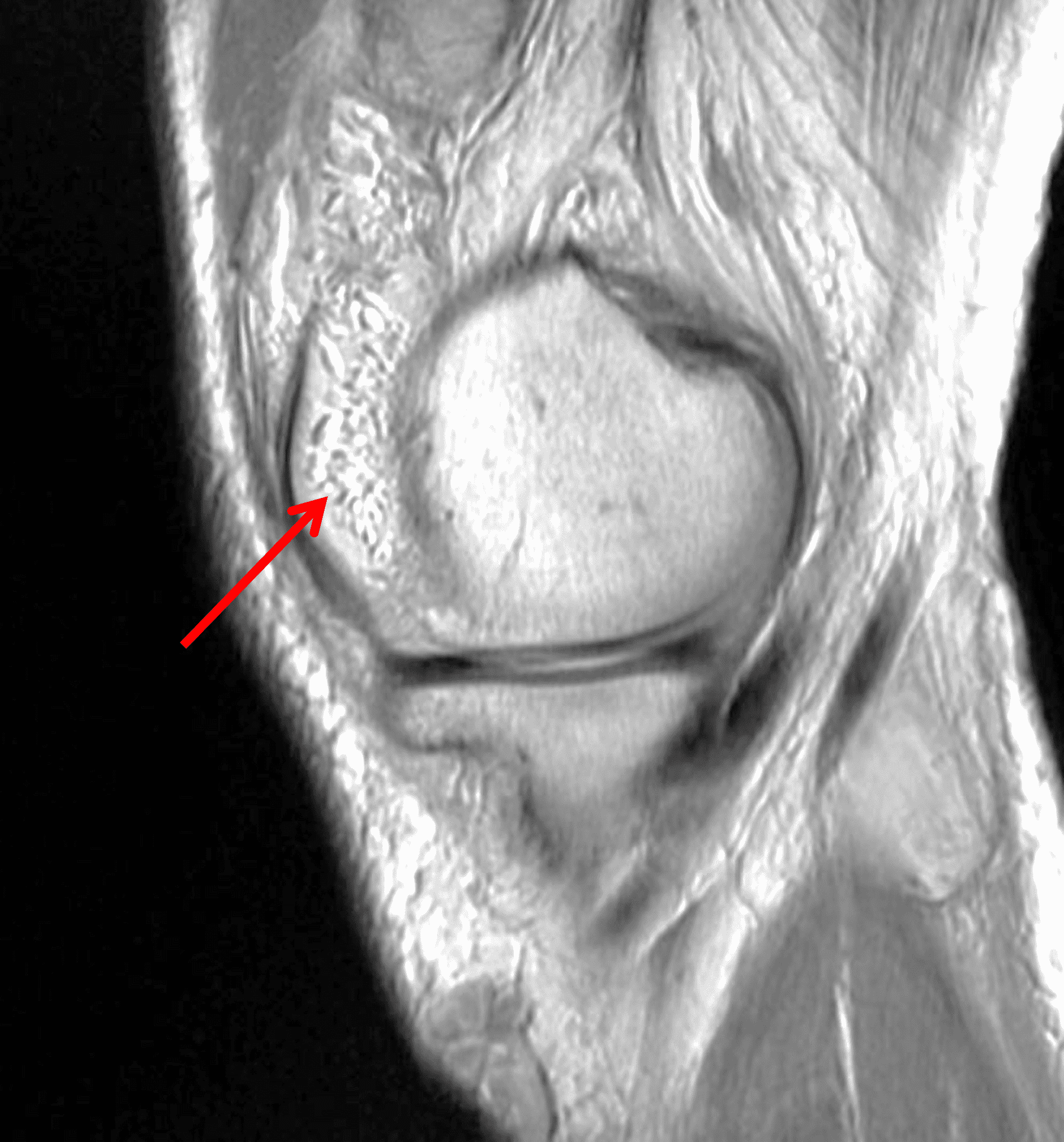
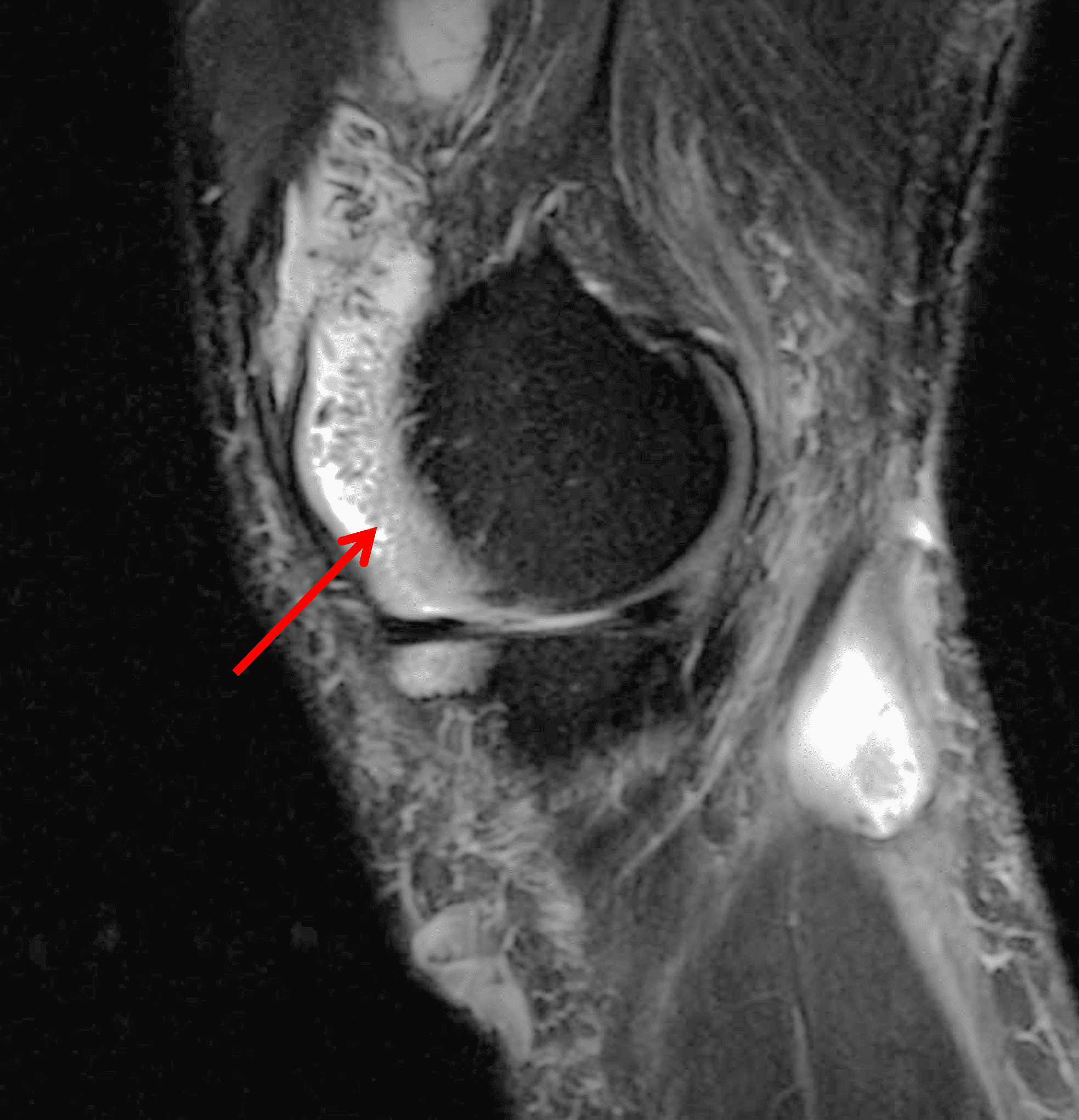
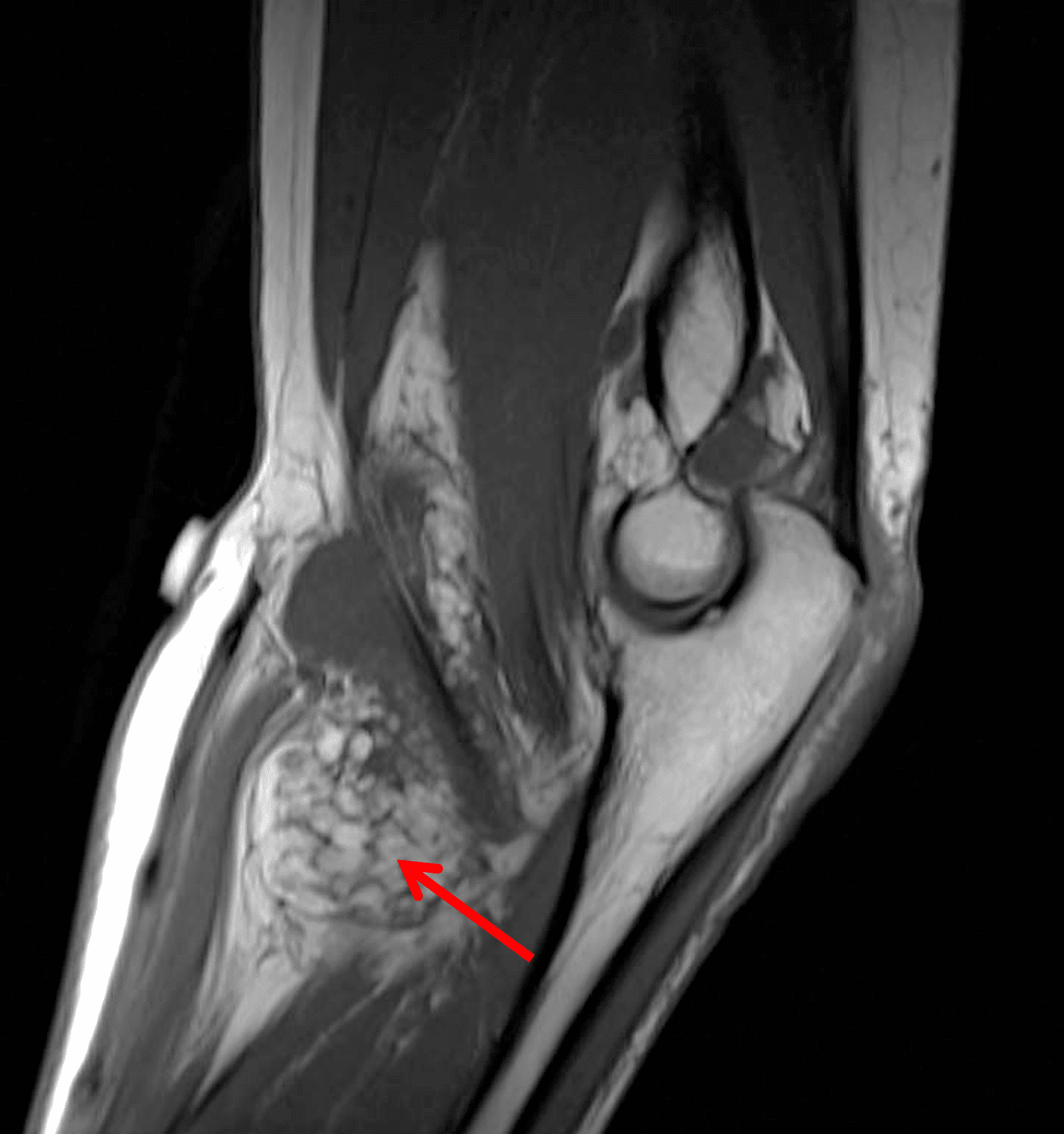

Figure 8: Lipoma arborescens in two patients. Sagittal (8A) proton density-weighted and (8b) fat-suppressed T2-weighted images of the knee show subsynovial proliferation in the suprapatellar recess, composed of fronds with fat signal intensity (arrows). In a second patient, sagittal (8C) T1-weighted and (8D) fat-suppressed fluid-sensitive images of the elbow demonstrate frond-like, fat signal synovial proliferation within the distended radiobicipital bursa (arrows).
Deposition Processes
Gout
Gout (https://radsource.us/gout/) is the most common metabolic crystalline deposition disease, characterized by monosodium urate crystal deposition in joints and soft tissues in patients with long standing hyperuricemia.2–4,16,17 It most commonly occurs in the first metatarsophalangeal joint and is more common in men, presenting most frequently in the fifth decade. Early disease is usually monoarticular, but location, duration and frequency of attacks increase with disease progression. Gout occurs in idiopathic, secondary, and drug-induced forms, and can also be divided into acute, intermediate and chronic forms by imaging.2-4,16,17 With acute flares, patients present with pain, swelling and erythema about a joint, bursa or tendon sheath, typically lasting 24-48 hours and resolving by 5-7 days. Crystals remain in the joint, predisposing to subsequent attacks due to chronic low-grade inflammation. Tophus formation is almost always a manifestation of chronic gout, although some cases of tophi have been described in the acute setting. Tophi are composed of urate crystals, protein matrix, inflammatory cells and foreign body giant cells. Tophus deposition can be intra-articular or extra-articular, and can involve cartilage, bone, ligaments, tendons and subcutaneous tissues.2-4,16,17
Imaging characteristics are variable in different stages. On radiographs, in early stages, soft tissue swelling may be the only finding. With chronic gout, intra-articular or juxta-articular erosions with overhanging edges, and soft tissue mass with or without calcification can be seen, with relative preservation of joint spaces until late stage of disease.2-4,16,17 On MRI (Figures 2 and 9), tophi usually appear as intermediate T1 signal masses with variable T2 signal depending on the amount of calcification present, and somewhat variable contrast enhancement. On CT, tophi are usually hyperattenuating with or without calcifications. Gout may also present on imaging as focal or multifocal disease within a joint.2-4,16,17
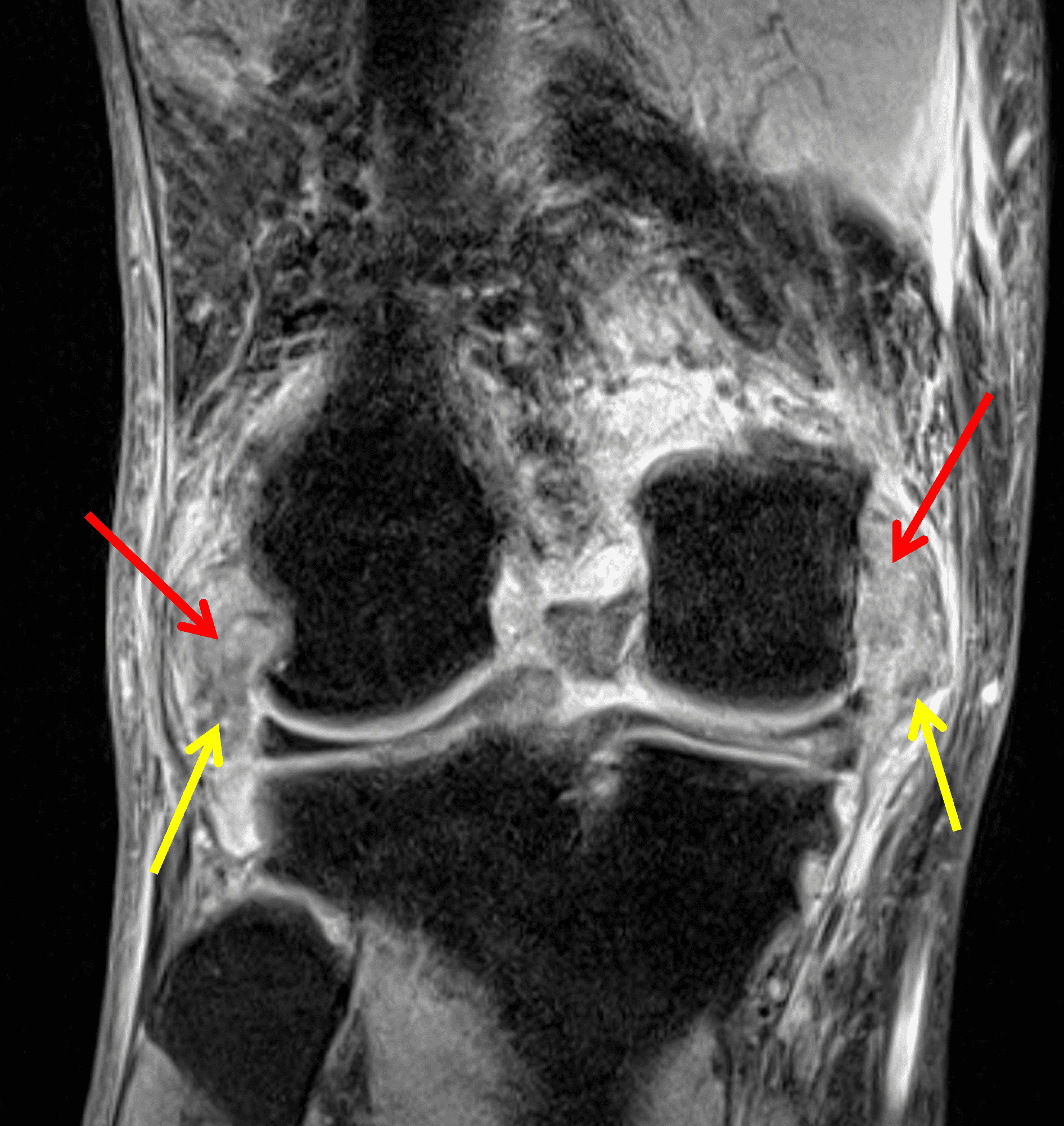
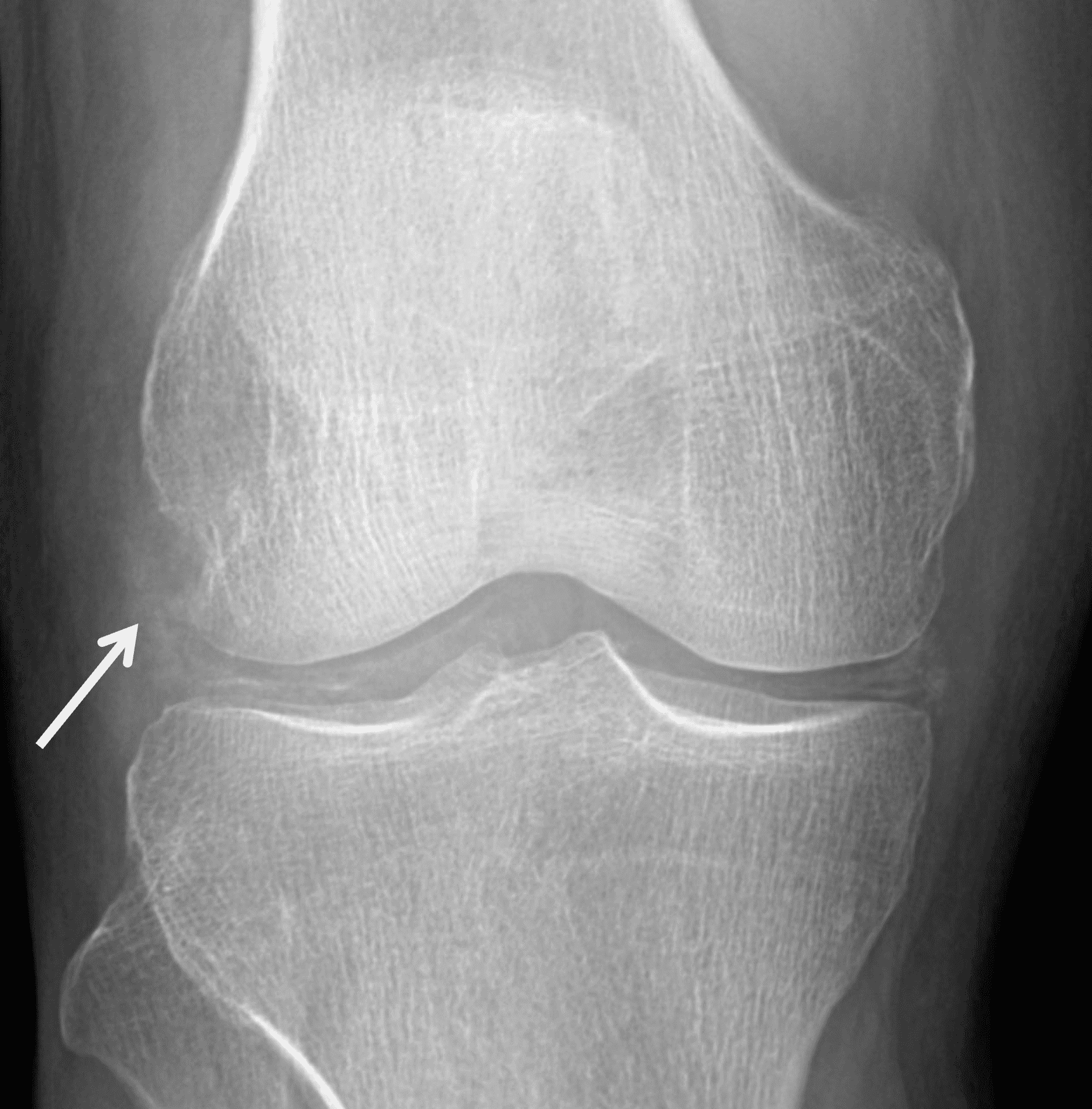
Figure 9: Tophaceous gout in the knee. (9A) Coronal fat-suppressed, fluid-sensitive image demonstrates heterogeneous intermediate signal intra-articular masses (red arrows). Hypointense foci (yellow arrows) correspond to calcifications. (9B) AP radiograph confirms calcification within the tophi (arrow) as well as meniscal chondrocalcinosis.
Amyloidosis
Amyloid arthropathy is a destructive, erosive arthropathy characterized by intra-articular and peri-articular amyloid deposition, most commonly in the hips, wrists, shoulders, knees and spine and often bilateral.2-4,18 It is most commonly seen in patients on chronic dialysis, plasma cell dyscrasias, and less often in chronic inflammatory conditions such as rheumatoid arthritis, chronic osteomyelitis and familial Mediterranean fever.2-4,18
On CT and radiography, juxta-articular soft tissue masses are seen with subchondral cysts, erosions and localized osteopenia as well as joint effusions with preserved joint spaces. On MRI, the masses demonstrate intermediate to hypointense T1 signal, and intermediate T2 signal which can occasionally be variable (Figure 10). Unlike TCGCT, there is usually no hemosiderin or blooming artifact.2-4,18
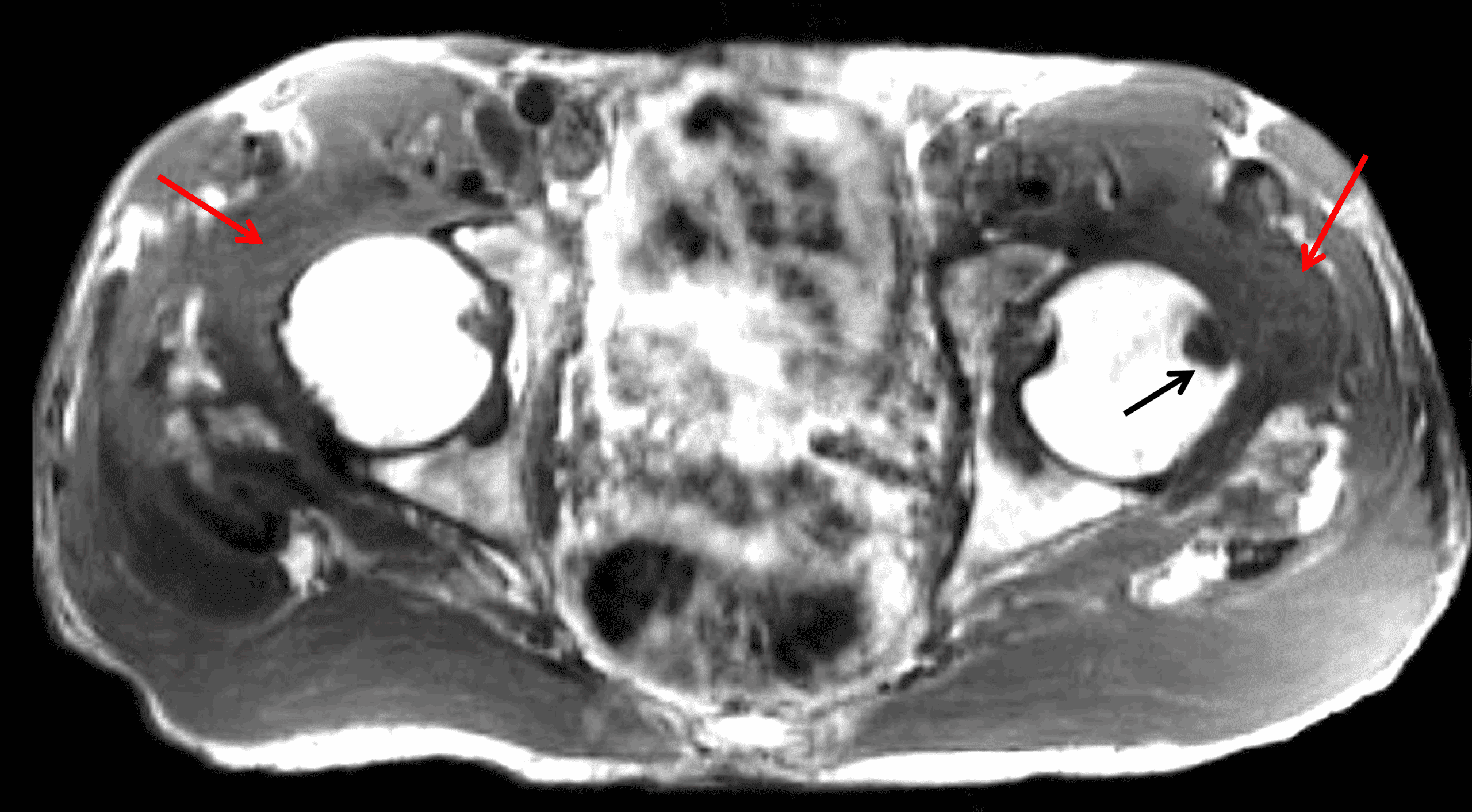
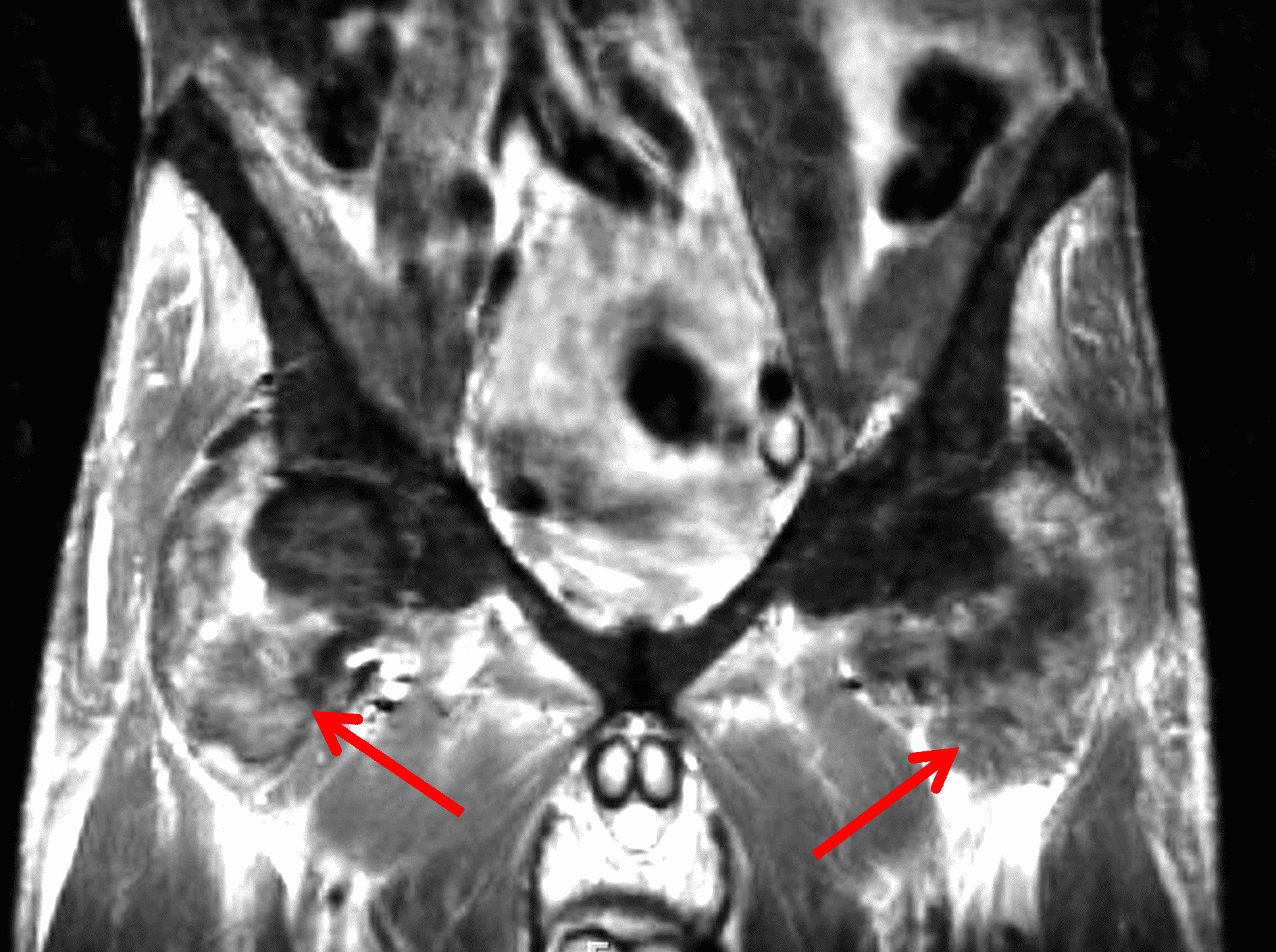
Figure 10: Amyloidosis in a patient with chronic renal failure. (10A) Axial T1-weighted and (10B) coronal STIR images demonstrate diffuse intermediate to hypointense T1 and heterogeneously intermediate STIR signal masses in both hip joints (red arrows) with an erosion in the left femoral head (black arrow).
Calcium pyrophosphate deposition
While acute pseudogout can clinically present similarly to gout, tophi are not present, so imaging studies show no synovial-based masses.19 Radiographic chondrocalcinosis may be present in chronic calcium pyrophosphate deposition disease but is a nonspecific finding that also occurs with other conditions and aging.
Granulomatous Infection
Tuberculosis
Approximately 3% of patients with tuberculosis develop a musculoskeletal manifestation, either spondylodiscitis and Pott disease, or infectious arthritis, bursitis or tenosynovitis. Tuberculous arthritis most commonly occurs in the hip, knee and ankle, typically from hematogenous spread to the synovium rather than direct extension from osteomyelitis.2-4
Radiographic findings include monoarticular involvement, soft tissue swelling, periarticular osteopenia, joint effusion, marginal erosions and preservation of joint space, because cartilage destruction does not occur until late in the disease course. On MRI, there is relatively uniform intermediate to hypointense T2 signal synovial proliferation with avid contrast enhancement and possible rice bodies, which are detached synovial villi that form fibrinoid bodies within the joint. There may be associated marrow edema, osteomyelitis, myositis, abscess formation, skin ulceration and sinus tracts (Figure 11).2-4,20,21,22
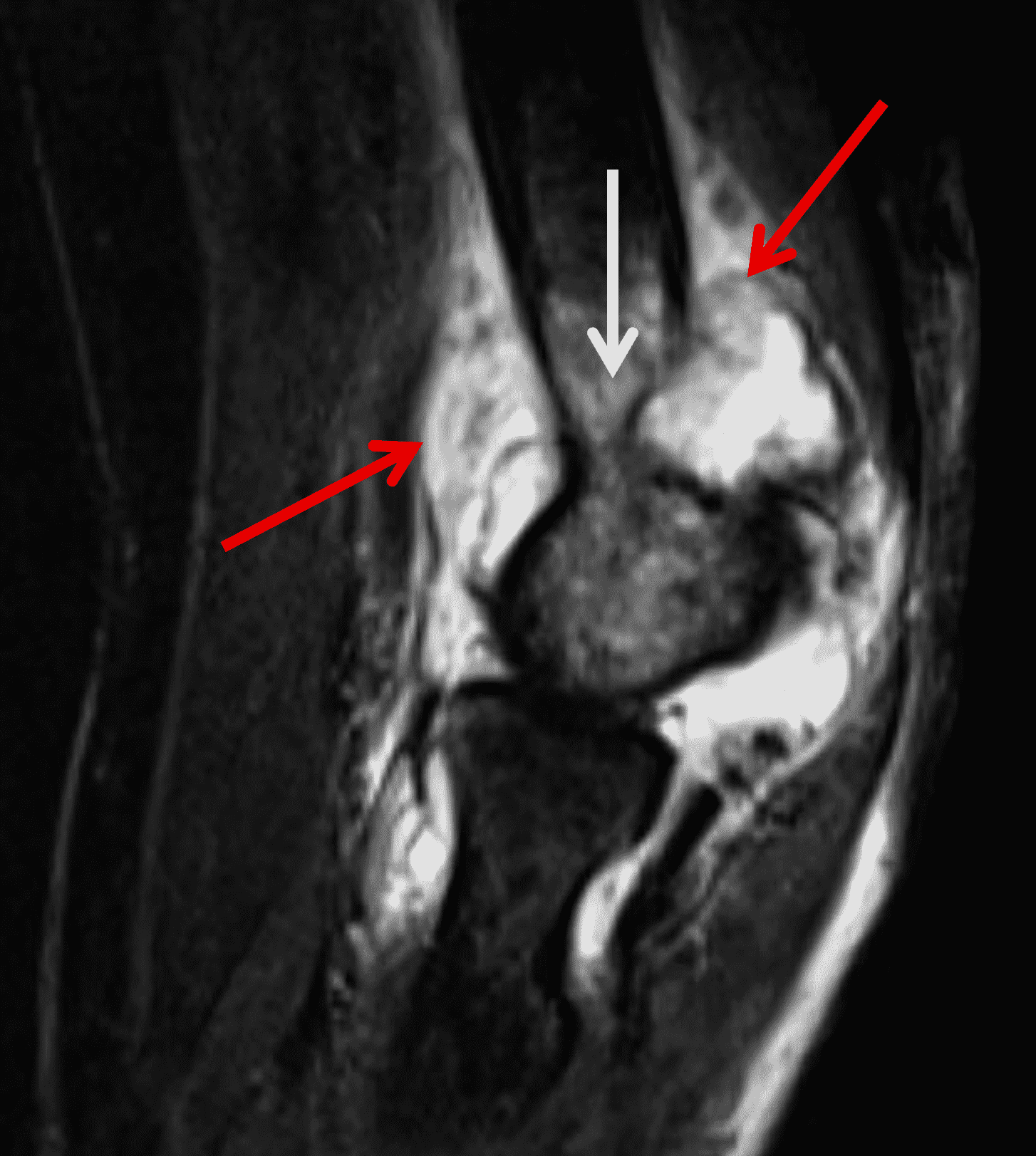
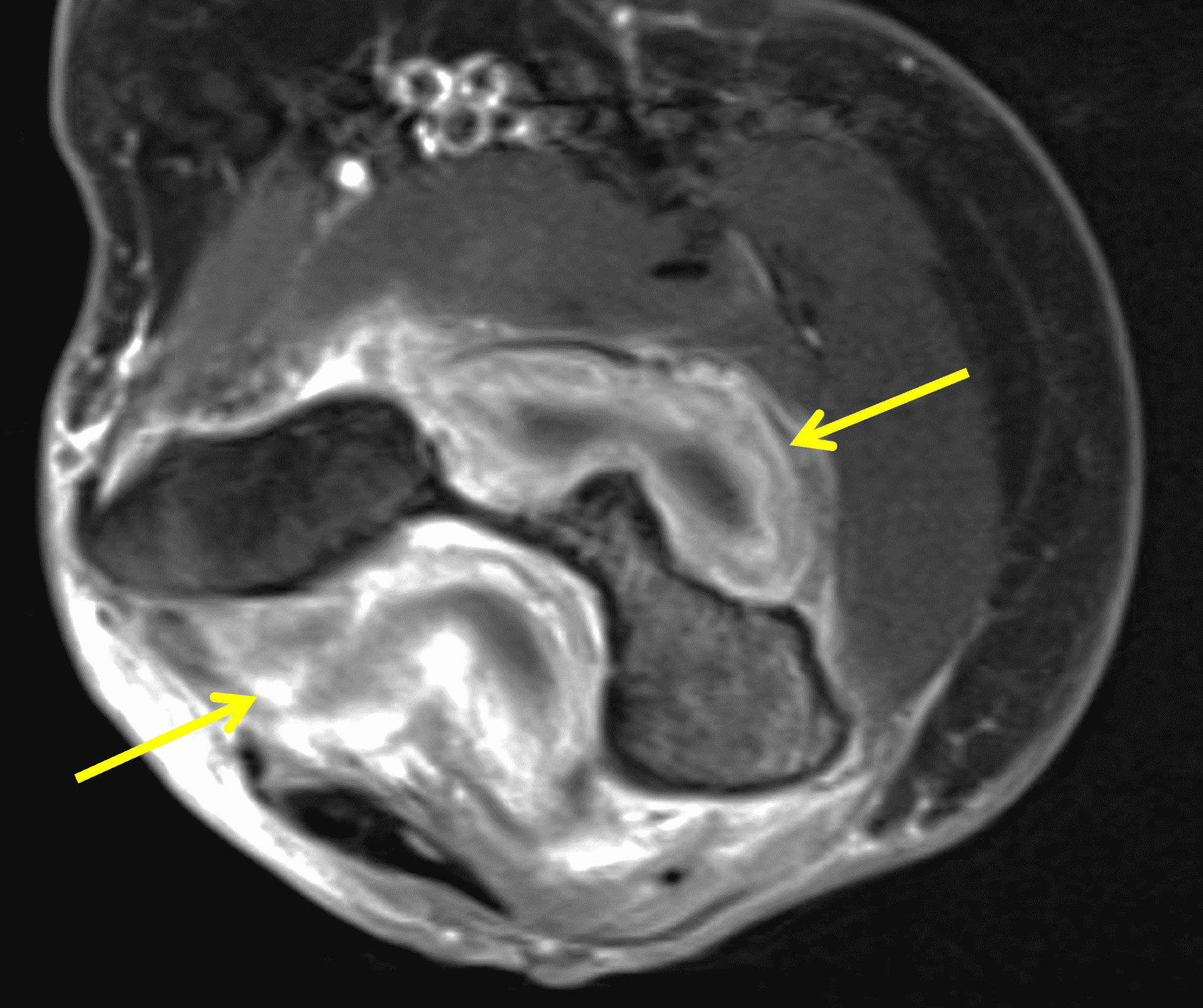
Figure 11: Tuberculous arthritis in the elbow. (11A) Sagittal fat-suppressed fluid-sensitive and (11B) axial post-contrast fat-suppressed T1-weighted images demonstrate intermediate signal diffuse synovial thickening (red arrows) with avid contrast enhancement (yellow arrows). Note the marrow edema in the distal humerus (white arrow).
Coccidioidomycosis
Coccidioidomycosis is endemic to portions of the southwestern United States, Mexico and South America, resulting from inhalation of Coccidioides immitis, a fungus. In disseminated disease, it can spread to the liver, spleen, lymph nodes and bones. Osteoarticular infection usually occurs in the knee and ankle joints, due to direct spread from osteomyelitis and rarely due to hematogenous spread.4
Imaging findings are similar to other granulomatous infections and include periarticular osteopenia, joint effusion, erosions and relatively preserved joint spaces until late in the disease process, as well as the possible presence of rice bodies.4 Abscess formation can also be seen. On MRI, the bone lesions have a variable appearance but are usually well circumscribed intermediate T1 signal and intermediate to hyperintense T2 signal with enhancement following intravenous contrast administration (Figure 12).4,23
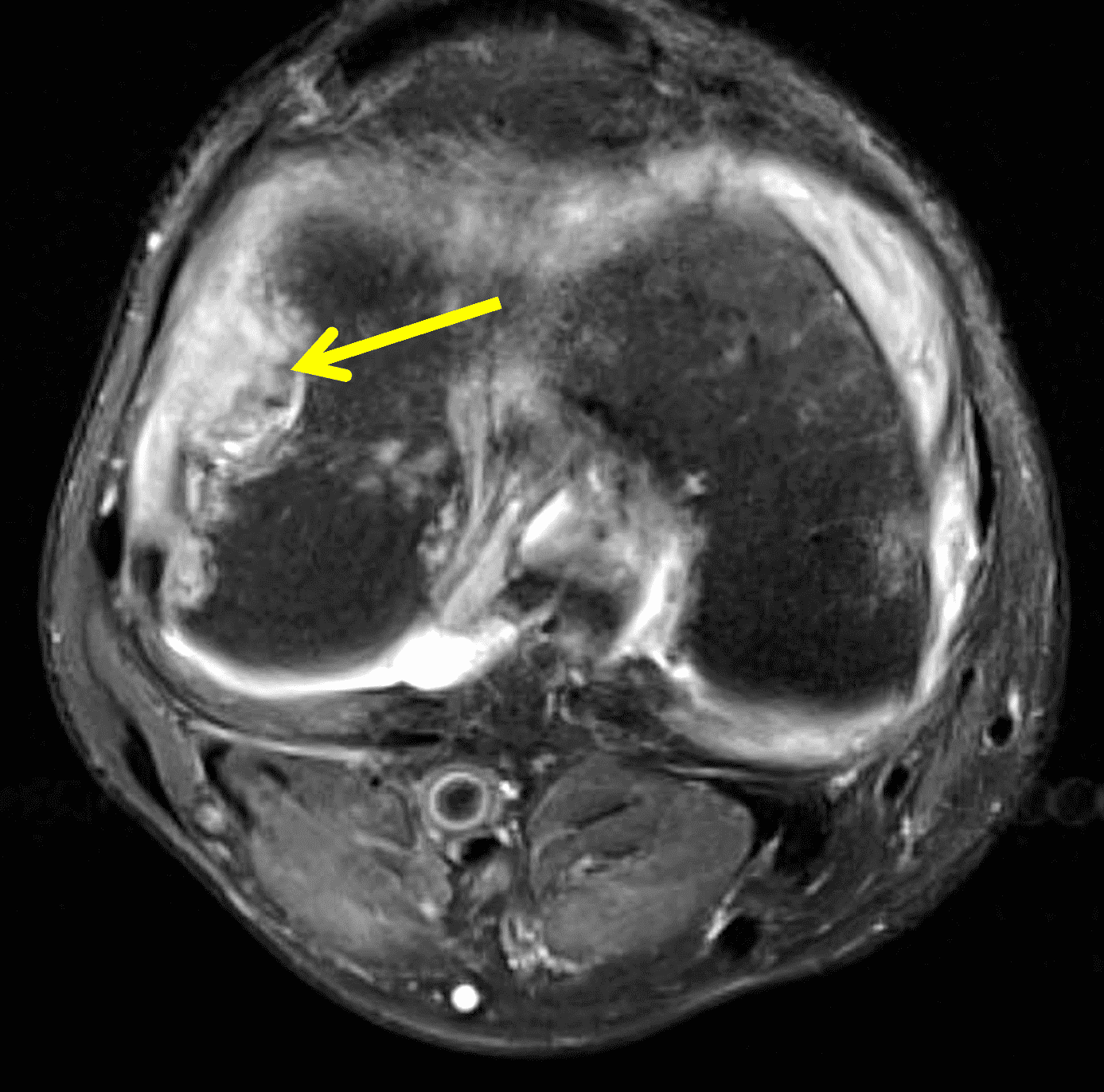
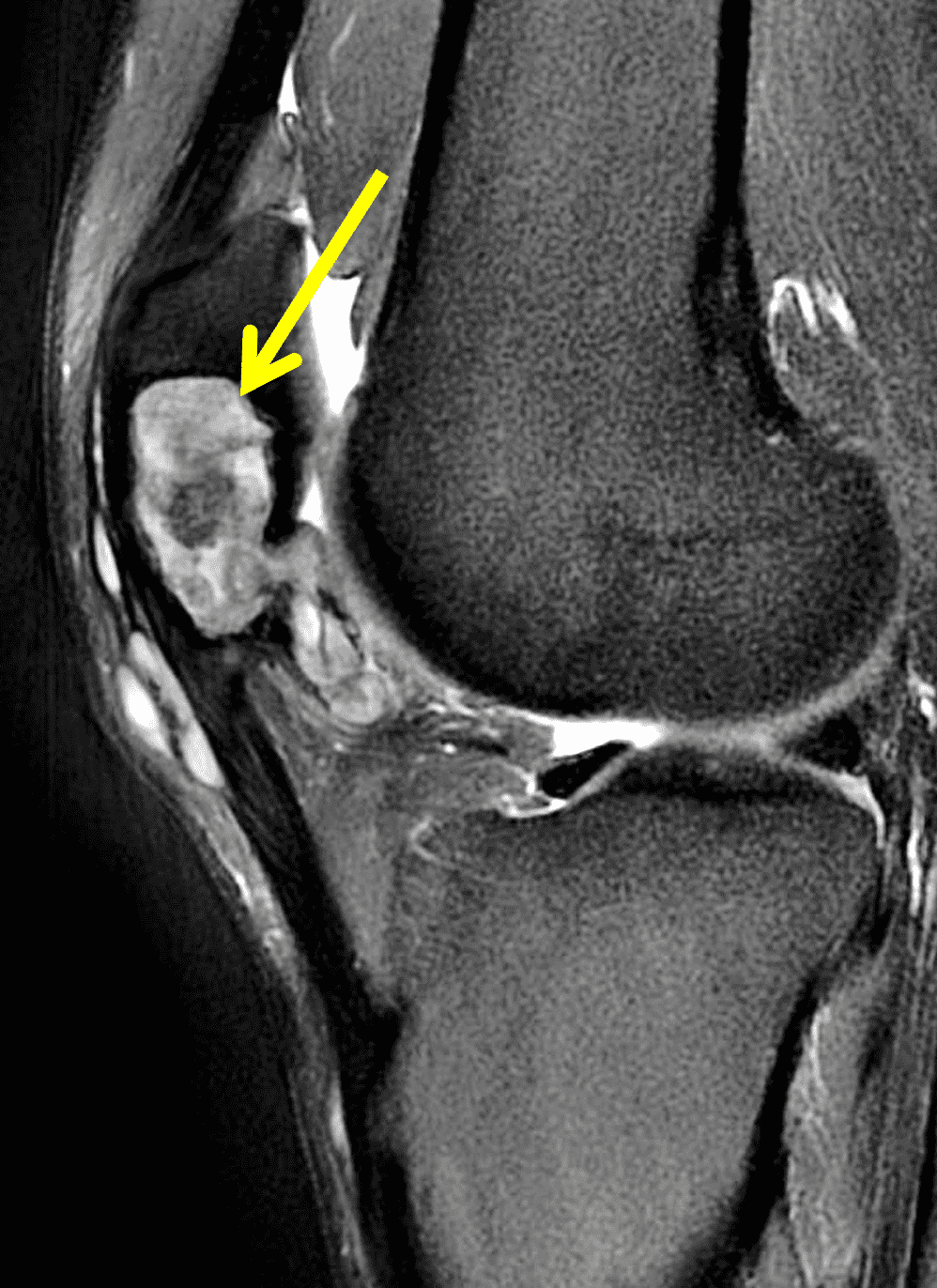
Figure 12: Histologically-proved coccidiomycosis in the knee. Fat-suppressed, water-sensitive (12A) axial and (12B) sagittal images demonstrate intermediate signal synovial proliferation eroding into the femur and patella producing large erosions (arrows).
Hemophilic Arthropathy
Hemophilia A and B are rare X-linked bleeding disorders due to partial or complete deficiency in coagulation factor VIII or IX; affected patients have a propensity for spontaneous hemarthroses.24 Repeated bouts of hemarthrosis result in chronic inflammatory changes, synovial hyperplasia, siderosis, fibrosis, osteochondral destruction, soft tissue and intra-articular pseudotumor, and joint contracture.2,3,24 Patients usually present in the first and second decades of life, with acute episodes involving a single joint but eventually develop polyarticular disease.3
On radiographs, there may be epiphyseal overgrowth if the hemarthroses began before skeletal maturity. Bony demineralization, erosions, joint effusion, intra-osseous pseudotumors and joint space narrowing with secondary osteoarthrosis are typical findings. MRI usually demonstrates diffuse intermediate hypointense T1 and T2 signal thickened synovium with blooming artifacts due to the presence of hemosiderin with secondary osteoarthrosis changes (Figure 13).2,3,24
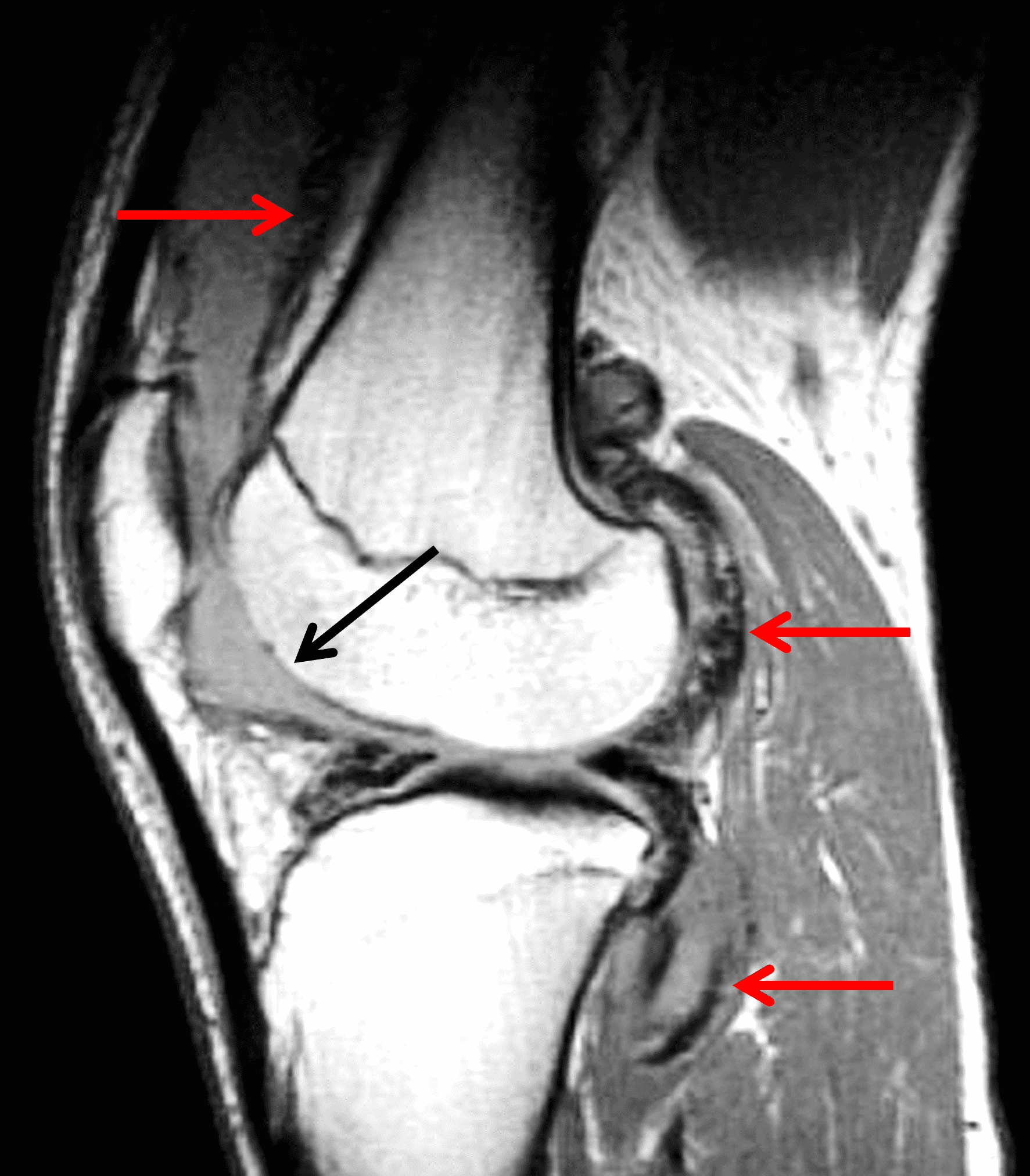
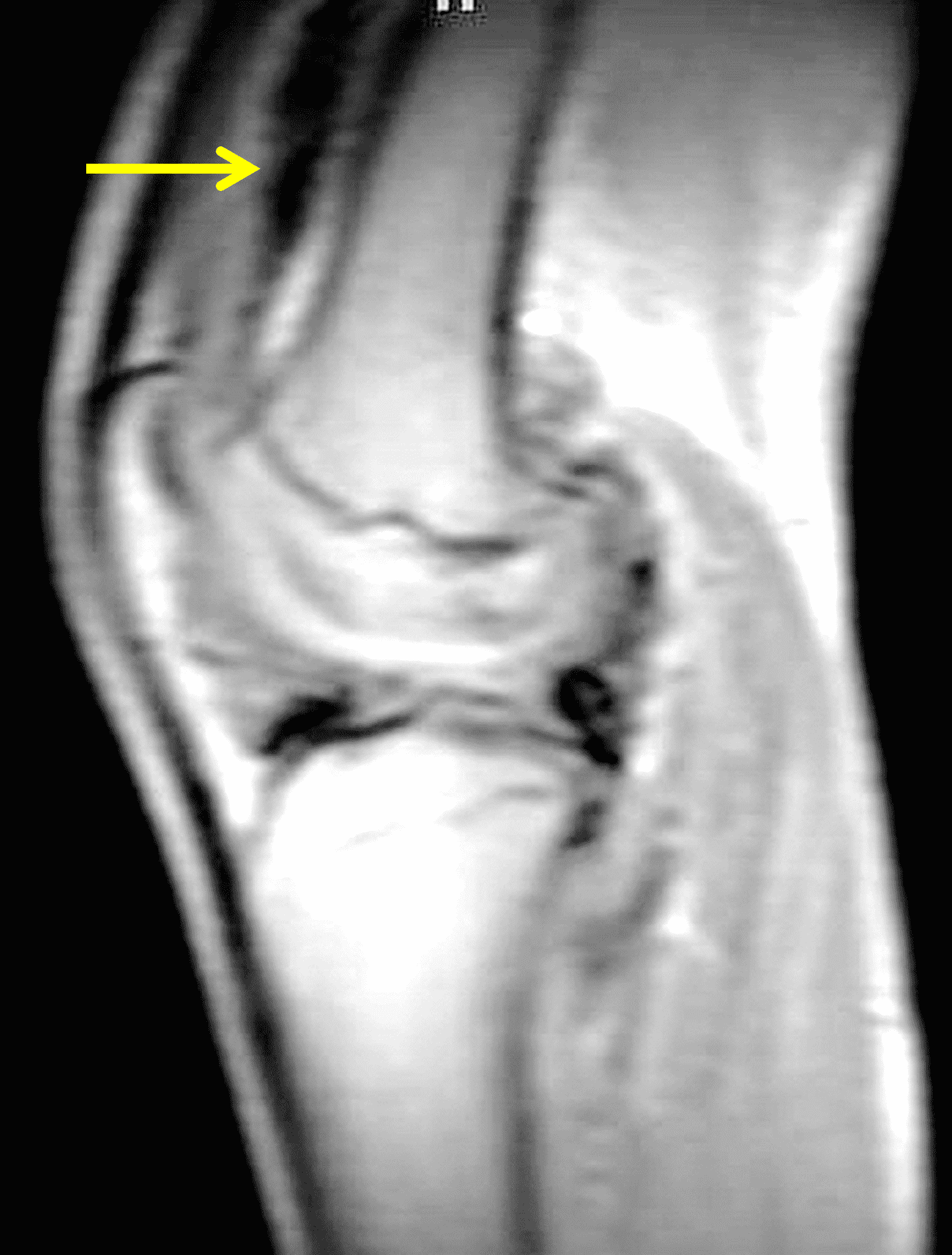
Figure 13: Chronic hemophilic arthropathy in the knee. (13A) Sagittal PD-weighted image shows severe arthritis with extensive full-thickness cartilage loss in the femoral trochlea (black arrow). Very low signal intensity foci in the synovium represent hemosiderin. (13B) Sagittal scout image acquired with gradient echo technique shows “blooming” artifact due to hemosiderin, most prominent in the suprapatellar recess (yellow arrow).
Rheumatoid Arthritis
Rheumatoid arthritis (RA) is one of the most common chronic systemic autoimmune diseases, affecting 1% of the world population. It usually presents in the fourth through sixth decades, typically involving the wrists, hands and feet, and is more common in women. RA is characterized by inflammation of the synovial membrane, resulting in bone erosions and cartilage destruction.3,4,25,26,27
Radiographic findings include diffuse multicompartmental uniform joint space loss, marginal or central erosions, periarticular osteopenia and soft tissue swelling, usually without osteophytes or subchondral sclerosis.2-4,25-27 Inflammation results in pannus formation, which is characterized by a proliferative, hyperplastic vascular synovium that can cause erosions (Figure 14). On MRI, pannus is hypointense to intermediate signal on T1 and T2 sequences, demonstrating postcontrast enhancement of the active pannus. Rice bodies may also be present.2-4,25-27 While very rare, intra-articular rheumatoid nodules have been reported in the knee, wrist, elbow, ankle and sacrococcygeal joints.25,28

Figure 14: Rheumatoid arthritis in the shoulder joint. Axial fat-suppressed proton density-weighted image demonstrates diffuse intermediate to hyperintense signal synovial proliferation with rice bodies posteriorly (red arrow) and pannus anteriorly (yellow arrow). There is also generalized full-thickness glenohumeral cartilage loss without osteophyte formation.
Miscellaneous
Additional intra-articular processes include but are not limited to: neuropathic osteoarthropathy, osteoarthrosis-related synovitis, septic arthritis (Figure 15), plica related pathology, articular xanthoma, reactive processes related to hardware, and trauma-related findings including lipohemarthrosis.2,3,29


Figure 15: Septic arthritis involving a metacarpophalangeal joint. Long axis (15A) T1-weighted and (15B) fat-suppressed fluid sensitive (15B) images of the finger demonstrate extensive soft tissue edema, joint effusion with osteochondral destruction, diffuse marrow infiltration and an intra-osseous abscess (arrows). Note the high-signal-intensity peripheral rim (“penumbra sign”) around the abscess on the T1-weighted sequence.
Focal Processes
Tenosynovial Giant Cell Tumor, Localized Type (Localized Nodular Synovitis)
Localized type TSGCT (also known as focal nodular synovitis) presents as a single nodular mass and most commonly involves small joints, primarily the hand/wrist followed by the knee. Joint effusion and hemarthrosis are less likely to be present compared to the diffuse type. Treatment consists of marginal excision with a low recurrence rate.5 Histologically, localized type TSGCT is similar to the diffuse type except it involves a focal portion of the synovium and contains less hemosiderin.1,5
MRI demonstrates a well circumscribed, usually ovoid (sometimes multilobulated) intra-articular mass with nonspecific signal, usually intermediate to hyperintense T1 and variable T2 signal, with internal contrast enhancement due to capillary proliferation. Internal hypointense areas may be present, representing hemosiderin deposition and may demonstrate blooming artifact on gradient echo sequences. Internal linear T2 hyperintensity has also been described, possibly representing focal necrosis or fluid entrapment (Figure 16).1 Joint effusion is less common compared to the diffuse type.5
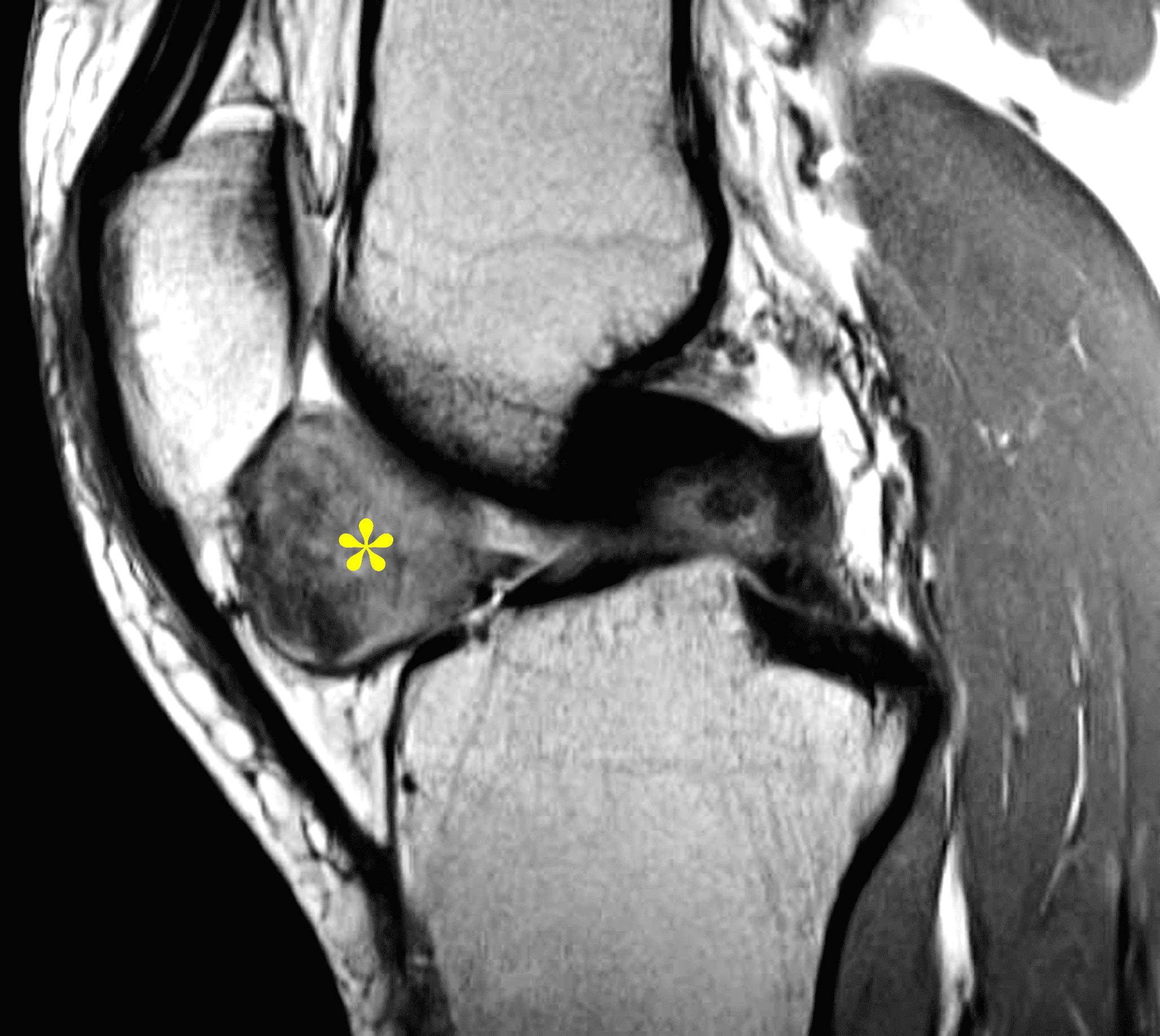
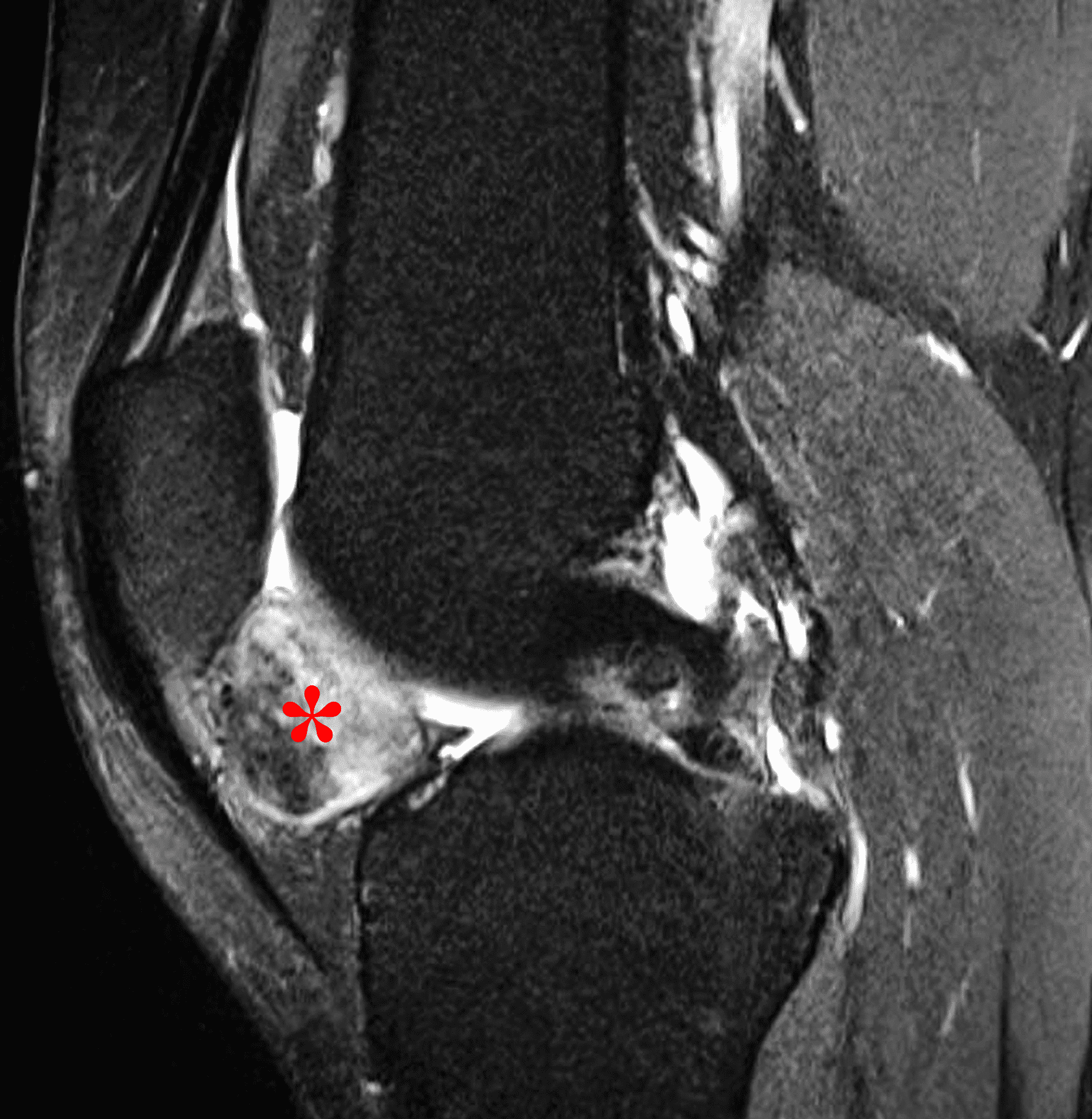
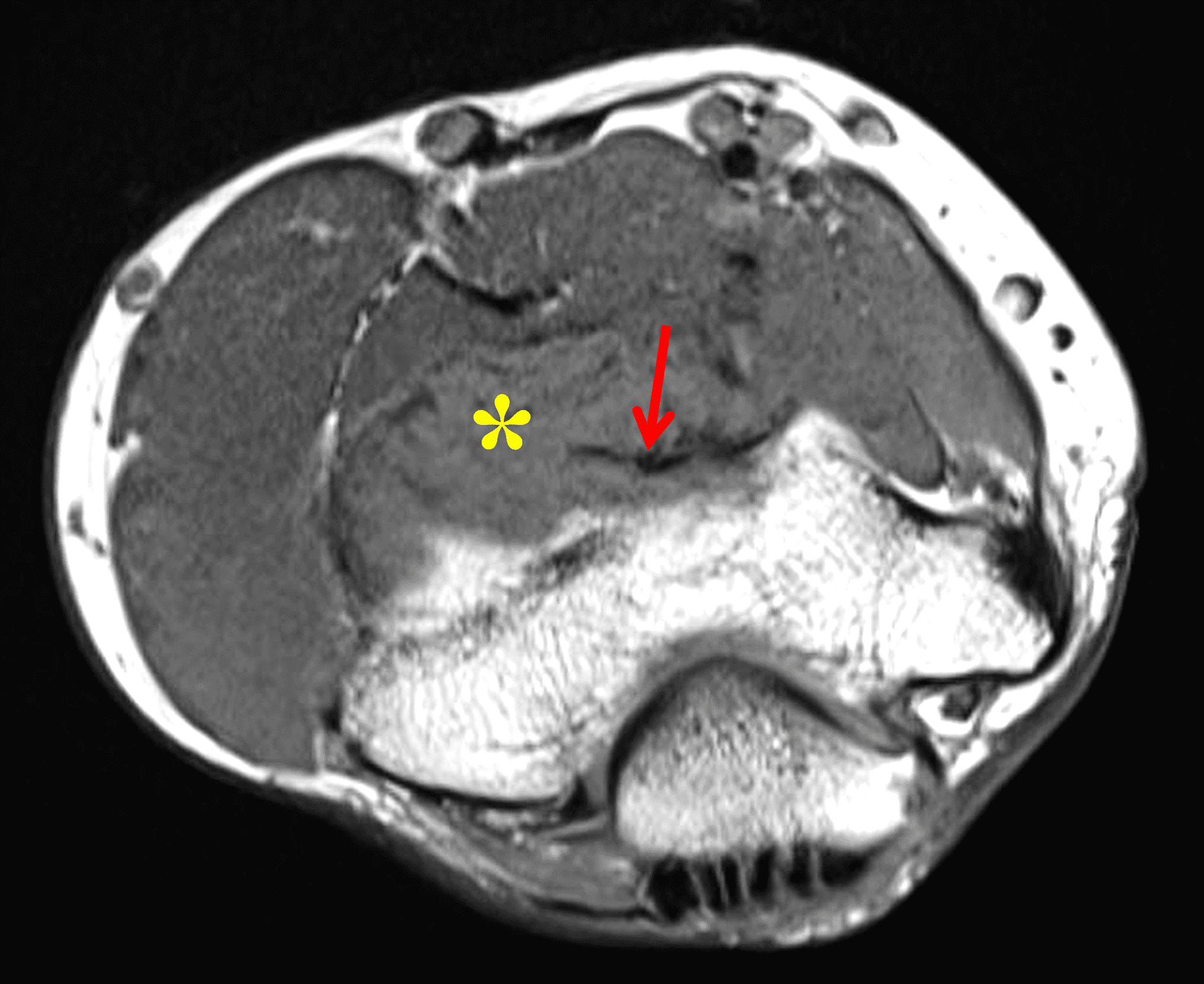
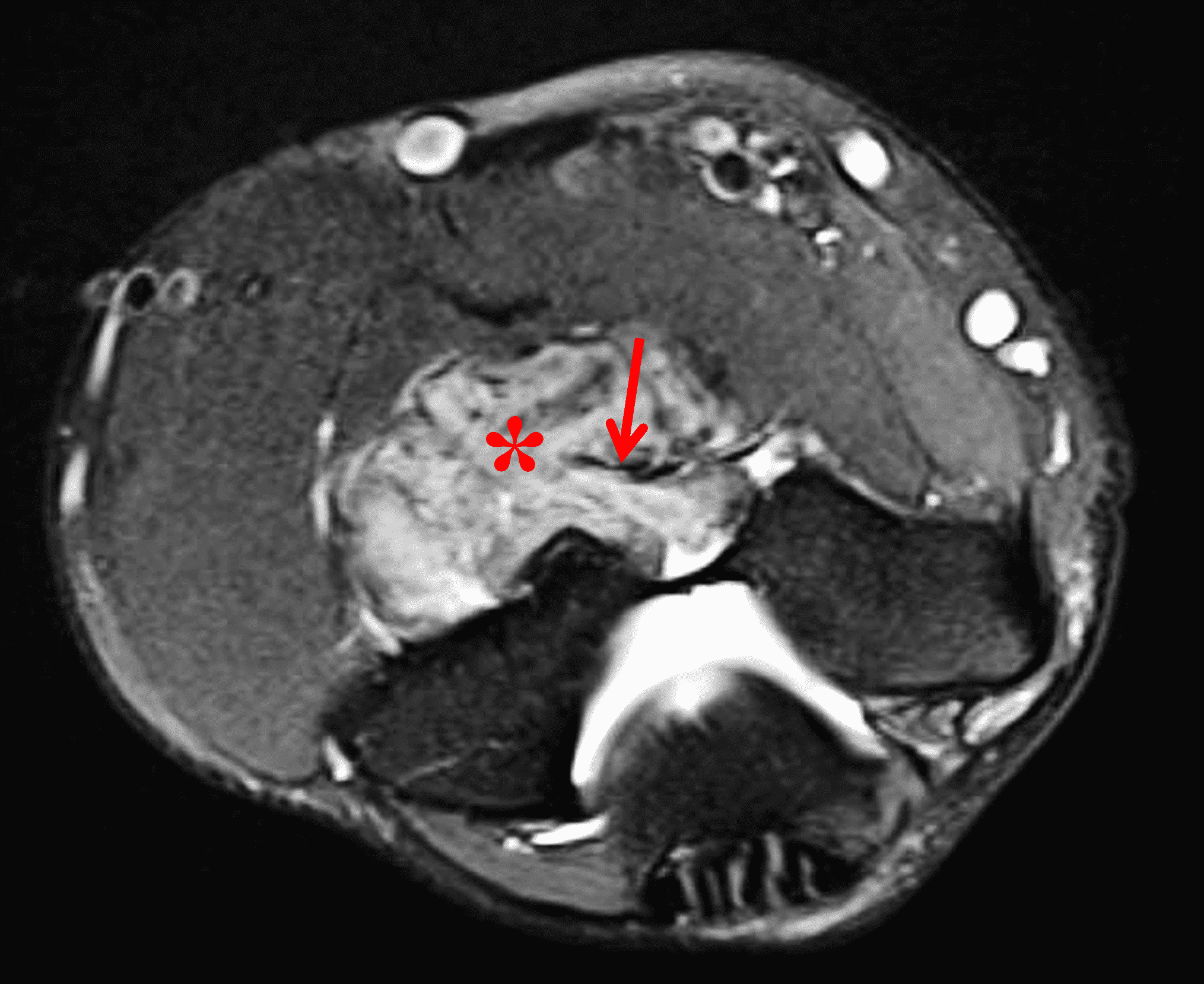
Figure 16: Localized type of tenosynovial giant cell tumor in two patients. Sagittal (16A) proton density-weighted and (16B) fat-suppressed fluid sensitive images of the knee demonstrate a circumscribed, intermediate T1 and T2 signal mass in Hoffa’s fat pad (asterisks), with areas of internal hypointensity representing hemosiderin deposition. In a second patient, axial (16C) T1-weighted and (16D) fat-suppressed fluid-sensitive images of the elbow demonstrate an anterior mass (asterisks) with the same signal intensity as well as characteristic curved hypointense foci within the lesion (arrows).
Occasionally, an intra-articular hematoma or blood clot unrelated to an underlying TSGCT may mimic a localized TSGCT; hematoma can usually be differentiated by clinical history such as recent known injury, signal characteristics of blood without additional mass, and a freely mobile appearance (Figure 17). Sometimes, a short-term follow-up MRI may be needed, which may demonstrate interval resolution or improvement in imaging findings, or migration of the structure to another location in the joint.
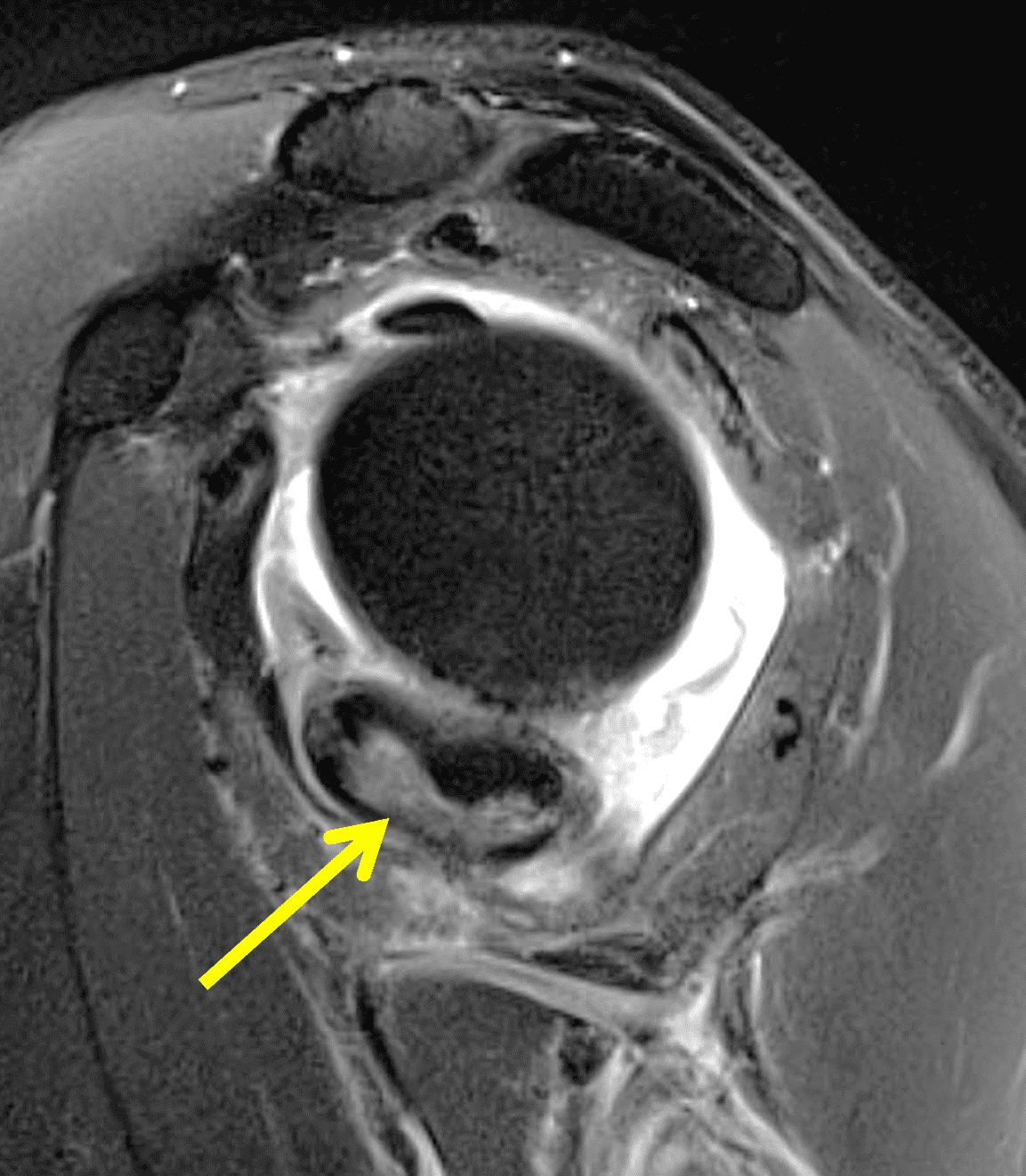
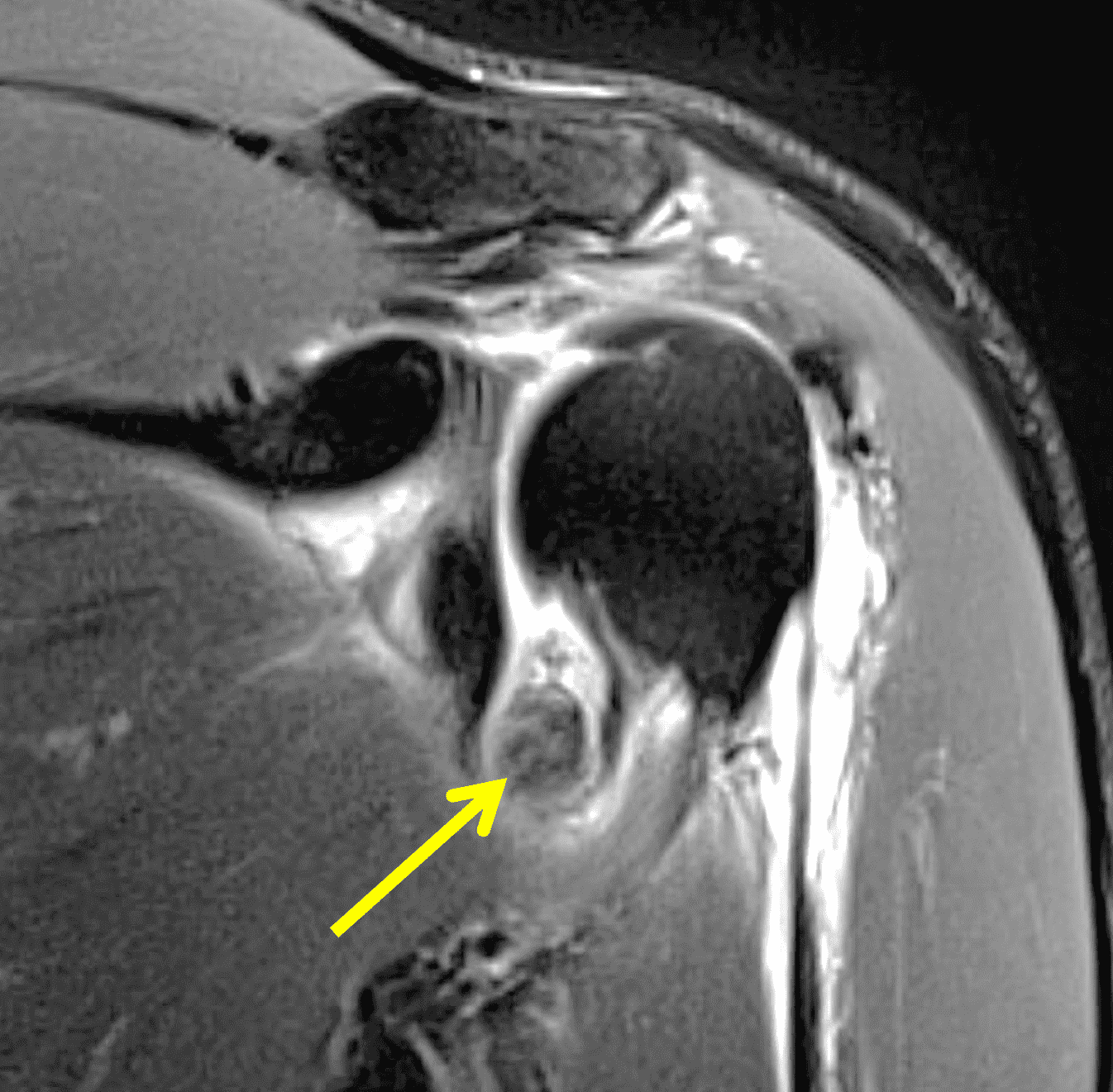
Figure 17: Intra-articular hematoma in the shoulder mimicking focal nodular synovitis. Fat-suppressed T2-weighted images in the (17A) oblique sagittal and (17B) oblique coronal planes demonstrate an intermediate signal and hypointense mass in the axillary recess (arrows). Note the extensive periarticular edema as well as joint effusion related to recent injury.
Vascular Anomalies
There is significant confusion and variability of nomenclature in the literature when referring to vascular anomalies. The International Society for the Study of Vascular Anomalies categorizes lesions into vascular tumors (proliferative lesions of endothelial cells) and vascular malformations (structural vascular abnormalities).30
Synovial hemangiomas are rare benign lesions that occur around joints, accounting for 1% of hemangiomas. They are subdivided into juxta-articular, intra-articular or intermediate (mixed). Synovial hemangiomas are composed of variable amounts of fibrous, adipose, endothelial and muscular tissue and histologically classified like other soft tissue hemangiomas, including cavernous, capillary, venous and arteriovenous types.1-3,31 They occur most commonly in the knee, typically in children and young adults. Patients may present with nonspecific findings such as pain, swelling, limited range of motion and hemarthrosis. Recurrent hemarthroses may cause early joint degeneration like hemophilic arthropathy. Masses can be localized or more diffuse. Localized lesions are usually resected. Diffuse lesions have a higher chance of recurrence due to the infiltrative nature and are treated with sclerotherapy.
Radiographs are often normal but may demonstrate a nonspecific mass, phleboliths and adjacent osseous remodeling. MRI usually demonstrates a mass with intermediate or hyperintense T1 signal, hyperintense T2 signal as well as possible rounded hypointense foci representing phleboliths, curvilinear thin hypointense septations and possible flow voids. Intervening T1 hyperintense fat is characteristic for intramuscular lesions (Figure 18). Synovial hemangiomas may also demonstrate fluid-fluid levels and thrombus, as well as MRI findings of hemosiderin deposition, which should not be confused for TSGCT.1-3,31
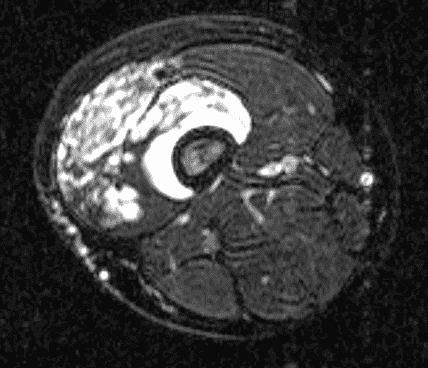
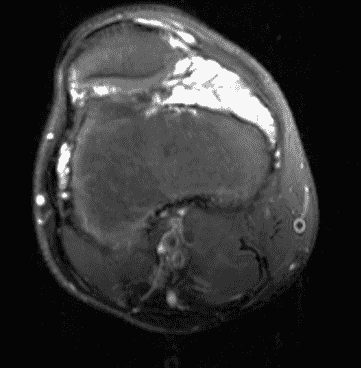
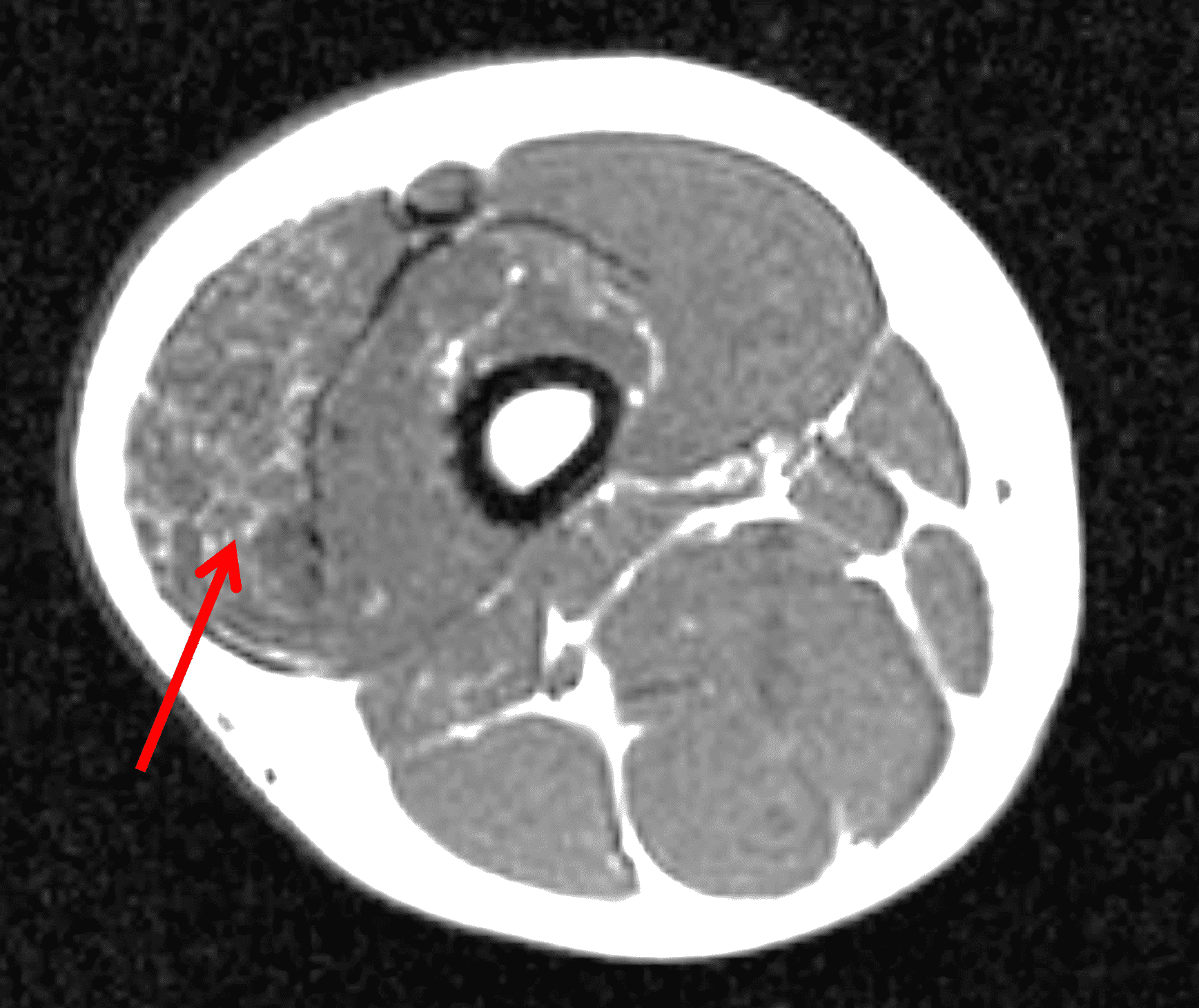
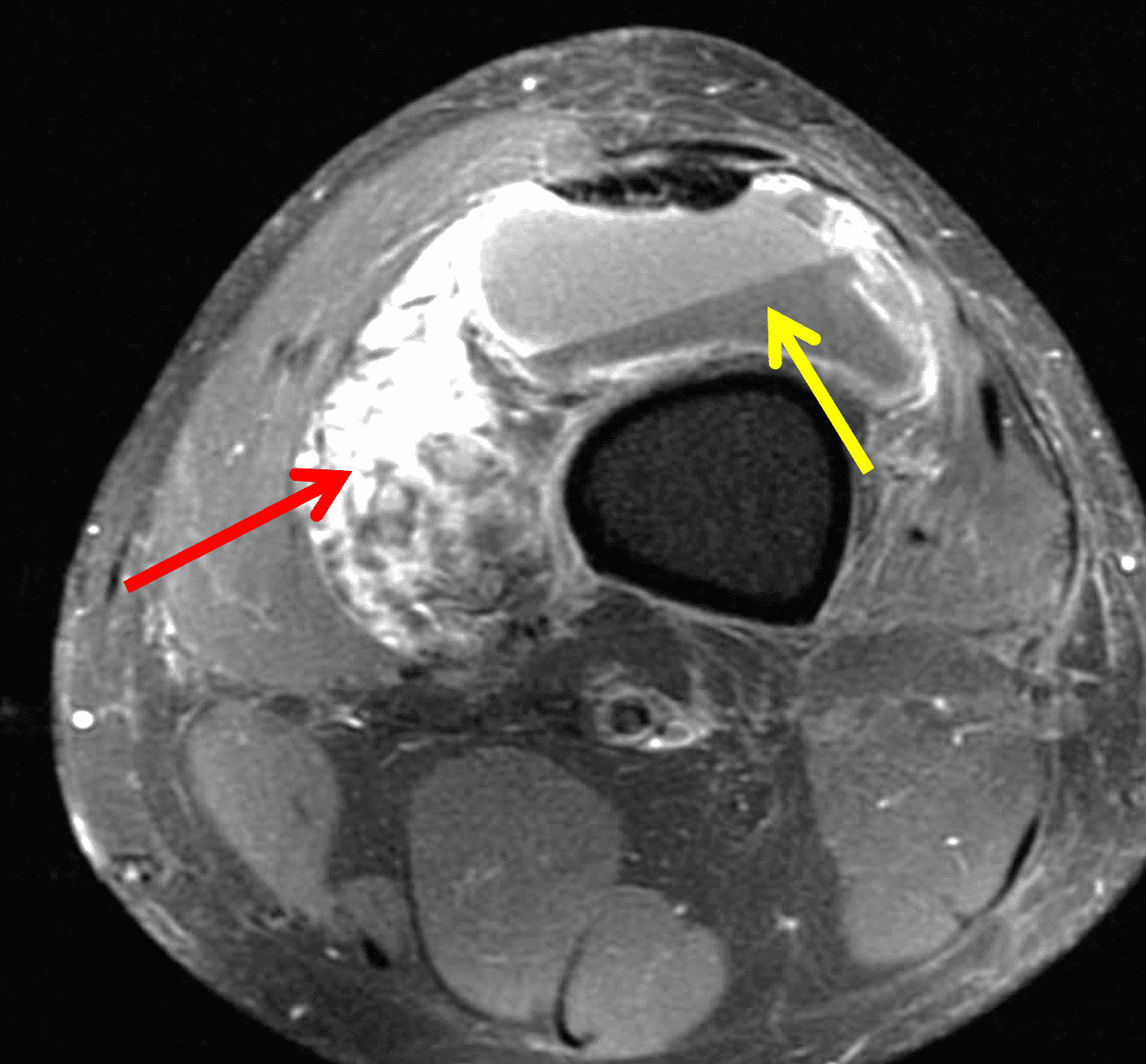
Figure 18: Synovial hemangiomas in two patients. Axial (18A and 18B) fat-suppressed fluid-sensitive and (18C) T1-weighted images of the knee and distal thigh show a synovial hemangioma extending into the surrounding soft tissues. The mass demonstrates intermediate T1 signal and T2 hyperintense signal, with tubular and ovoid foci and areas of intervening T1 hyperintense signal in the musculature (red arrow). In a second patient, (18D) axial fat-suppressed T1-weighted image obtained following intravenous contrast administration shows enhancement of the hemangioma (red arrow), as well as a fluid-fluid level in the suprapatellar recess consistent with hemarthrosis (yellow arrow).
Vascular malformations are subdivided by their dominant contributing vessels into venous, arterial, capillary and lymphatic, as well combinations of different vessel types. They are well evaluated by ultrasound and MRI, which can show a variable number of feeding vessels. The amount and timing of enhancement following intravenous contrast administration depends on the composition of the lesion.1–3
Lipomatous Tumors
Synovial lipomas are very rare, with few reported cases, most of which occur in the knee. They usually occur de novo, presenting as a well circumscribed mass with a thin fibrous capsule, and demonstrate homogenous fat signal on all MR sequences (Figure 19). There may be associated intra-lesional calcification or ossification due to osseous metaplasia. They can be found incidentally, present with a palpable mass or may cause impingement/locking. Acute pain due to torsion of the vascular pedicle has been reported. Symptomatic synovial lipomas are usually surgically resected.1, 32,33,34,35,36
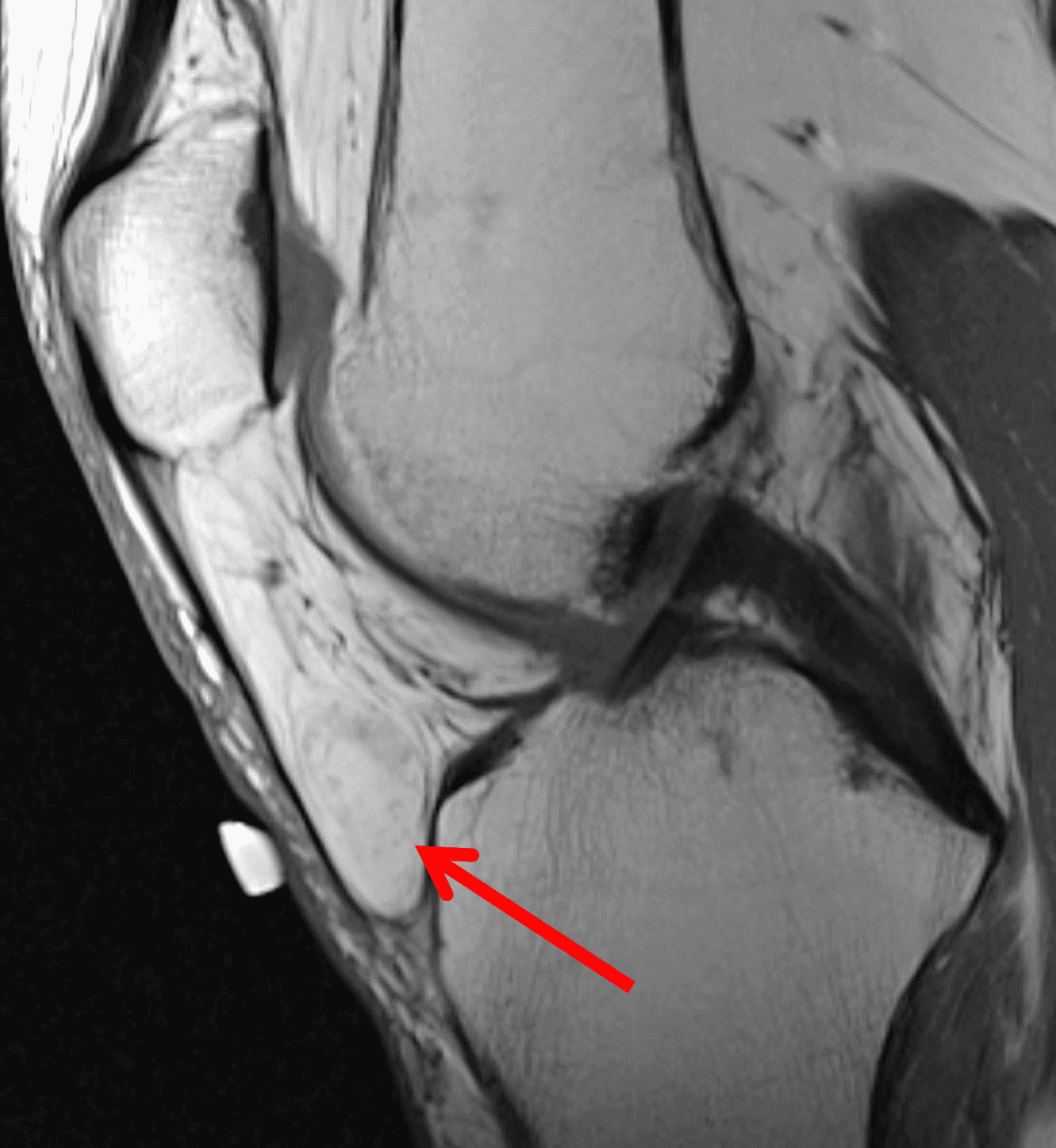
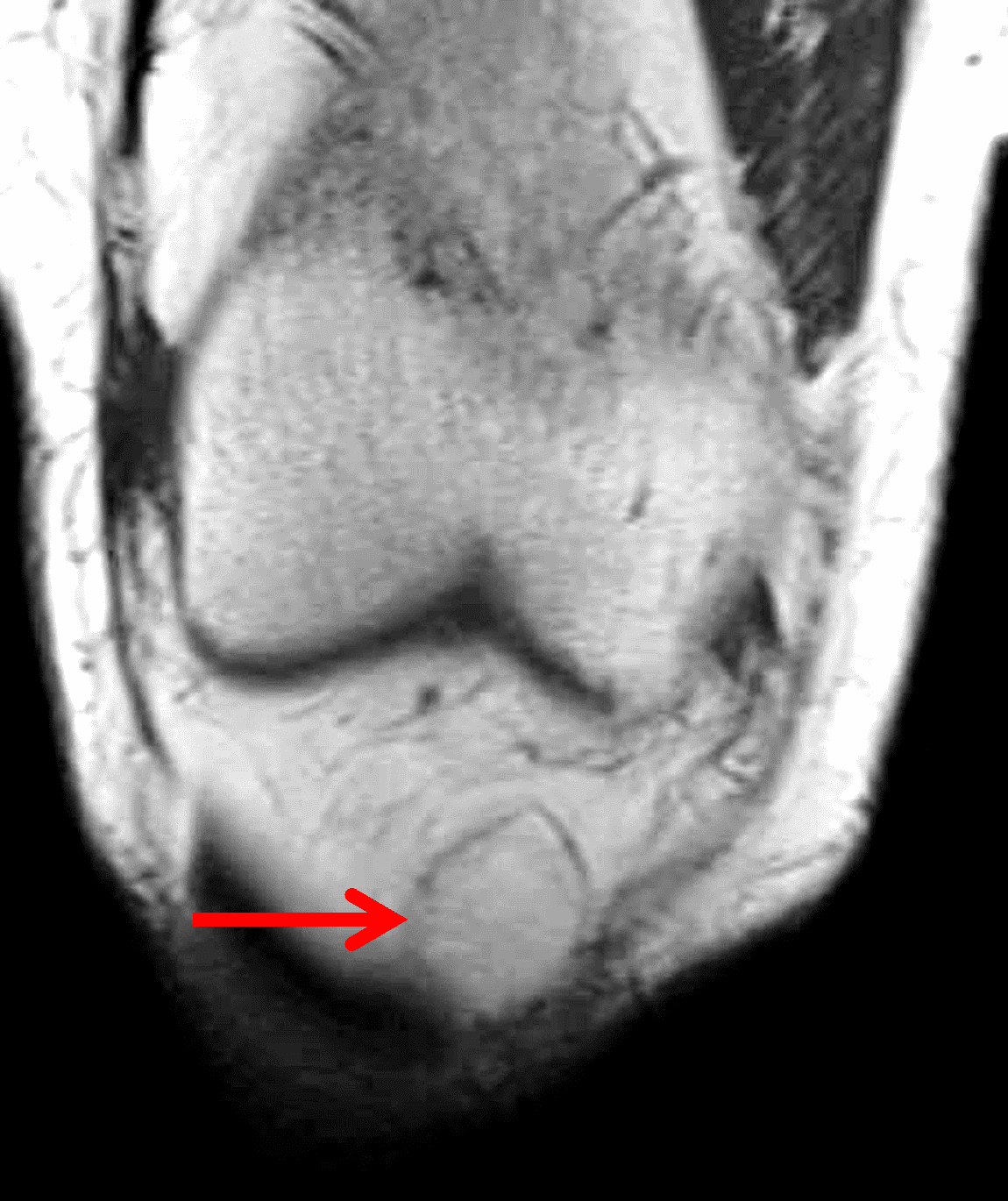
Figure 19: Synovial lipoma in the knee. (19A) Sagittal proton-density weighted and (19B) coronal T1-weighted images demonstrate an encapsulated, ovoid intra-articular mass with signal isointense to fat (arrows).
Intra-articular liposarcomas are even rarer, with very few reported cases. These may present as a synovially based mass with T2 hyperintensity and lack of macroscopic fat signal.37
Juxta-articular Myxoma
Juxta-articular myxomas are mesenchymal tumors of uncertain etiology, and occur most commonly about the large joints, especially the knee. They have a male predilection and a large age range that peaks in the fourth to sixth decade. Patients may present with a palpable mass, swelling and pain. In general, juxta-articular myxomas demonstrate the same imaging and histologic characteristics of intra-muscular myxomas with a sharply marginated mass demonstrating myxoid type T2 hyperintensity, T1 hypointensity and thin variable amount of enhancement mostly in the periphery and septations (Figure 20). They may cause remodeling or erosion of adjacent bone and have a propensity to recur after resection.38,39
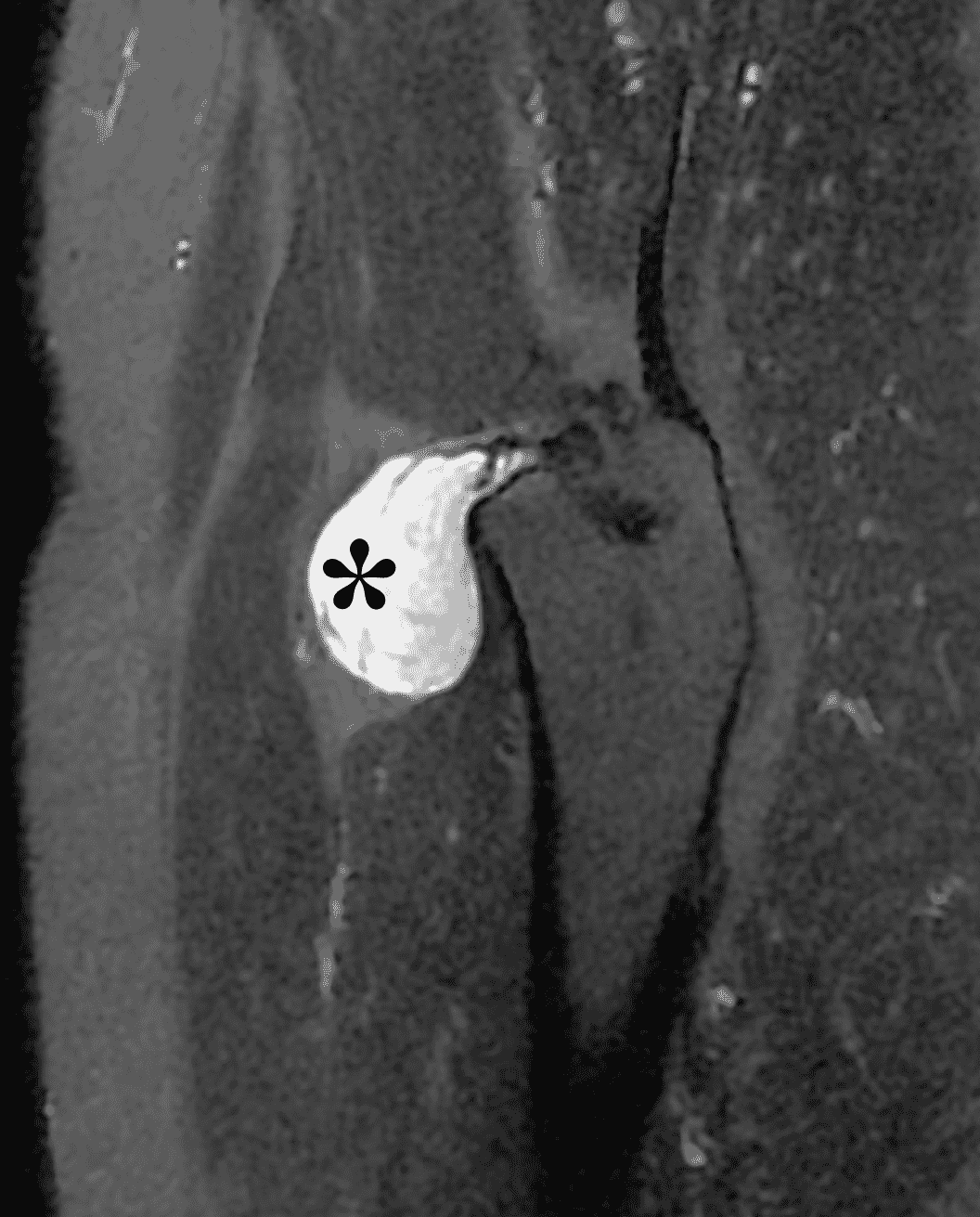
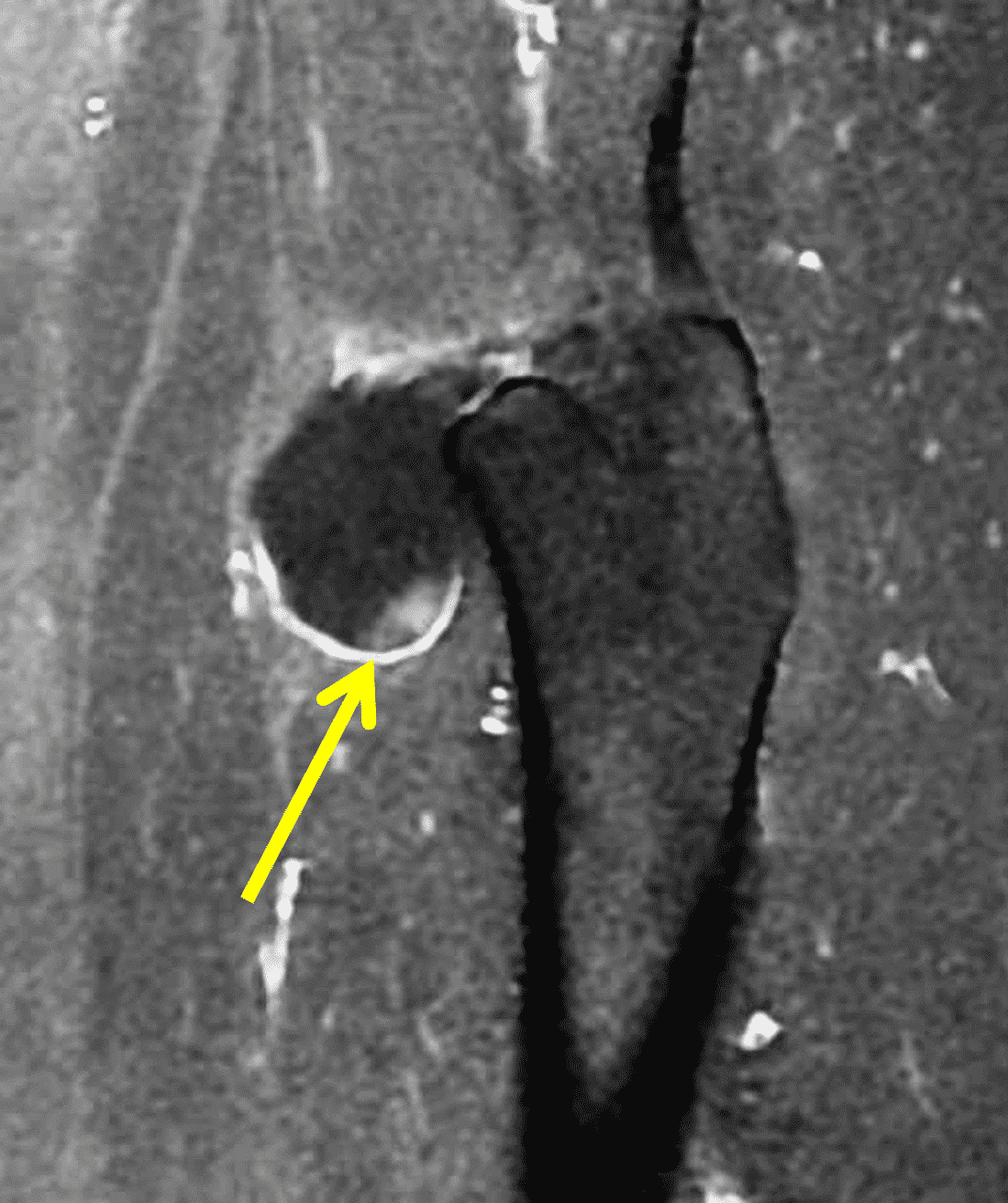
Figure 20: Juxta-articular myxoma of the hip. Sagittal (20A) fat-suppressed fluid-sensitive and (20B) post-contrast fat-suppressed T1-weighted images demonstrate a juxta-articular T2 hyperintense mass (asterisk) with thin, wispy septations and mild peripheral enhancement (arrow).
Synovial Sarcoma
Synovial sarcoma is a mesenchymal tumor (intermediate to high-grade) that usually occurs in the extremities, often periarticular, and most commonly in the popliteal fossa. Approximately 5% of synovial sarcomas are intra-articular, most commonly in the infra-patellar fat pad. They are most common among adolescents and young adults, although they can be seen in a wide spectrum of ages.
Intra-lesional calcifications occur in approximately 30% of cases, which can be seen radiographically.1-3,40 On MRI, findings are generally non-specific. They are usually heterogenous and multilobulated, demonstrating intermediate to hypointense signal on T1-weighted and hyperintense signal on T2-weighted sequences, with variable heterogeneous contrast enhancement. A few imaging clues have been described, including the “triple sign,” referring to T2 hyperintense (necrosis/hemorrhage), intermediate (cellular) and hypointense (calcification/fibrous) foci (Figure 21), as well as a “bowl of grapes” appearance with cysts, foci of hemorrhage and fluid levels. These findings are non-specific as they can be seen with other entities. Osseous invasion and neurovascular encasement occur in approximately 20% of lesions. In general, synovial sarcomas can have imaging characteristics that mimic benign lesions, including small size, homogenous signal, lack of invasion and a split fat sign due to intermuscular location. Intra-articular synovial sarcomas are even more challenging to diagnose in our experience due to their non-specific appearance and occasional small size.1-3,40
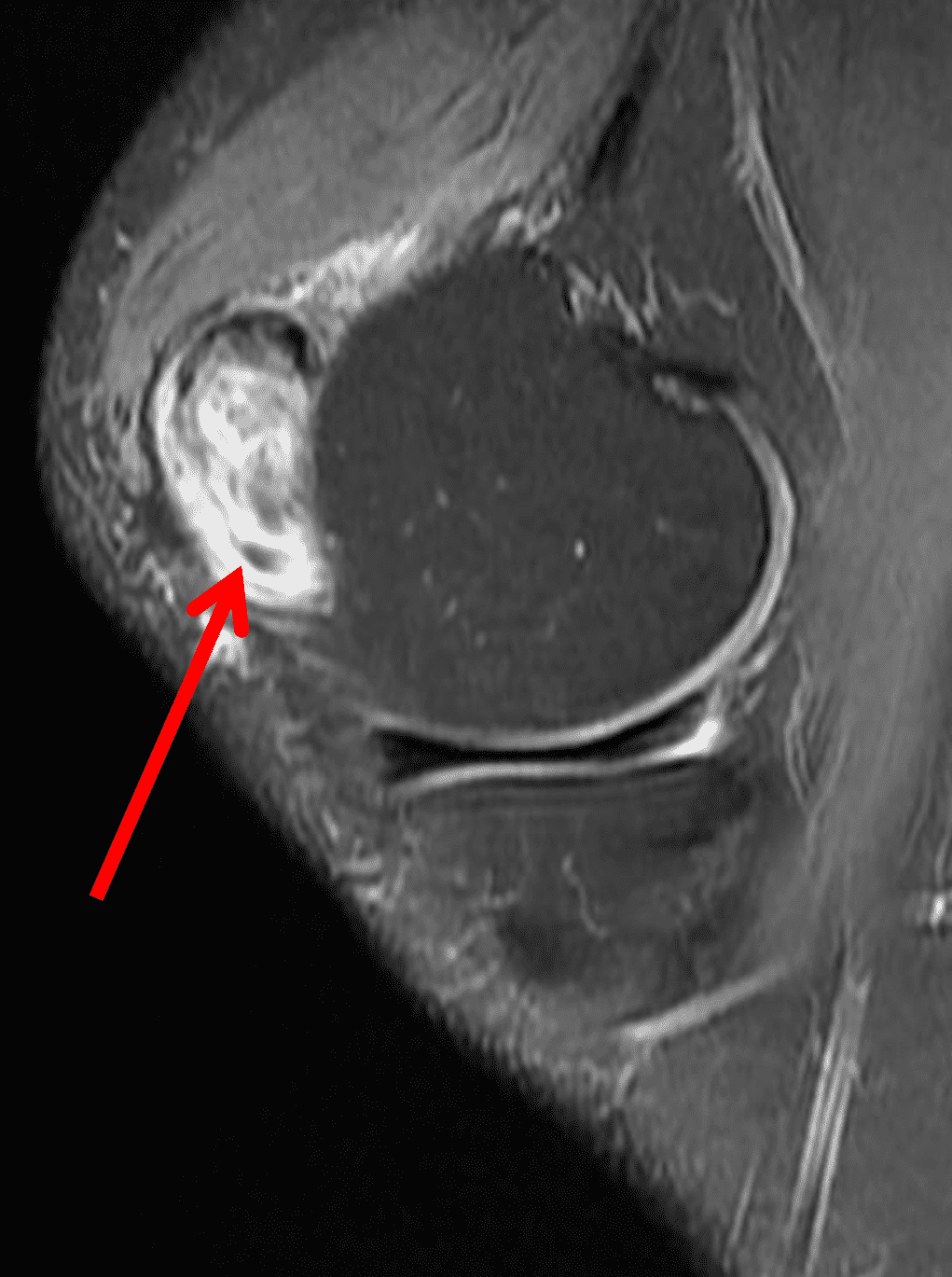
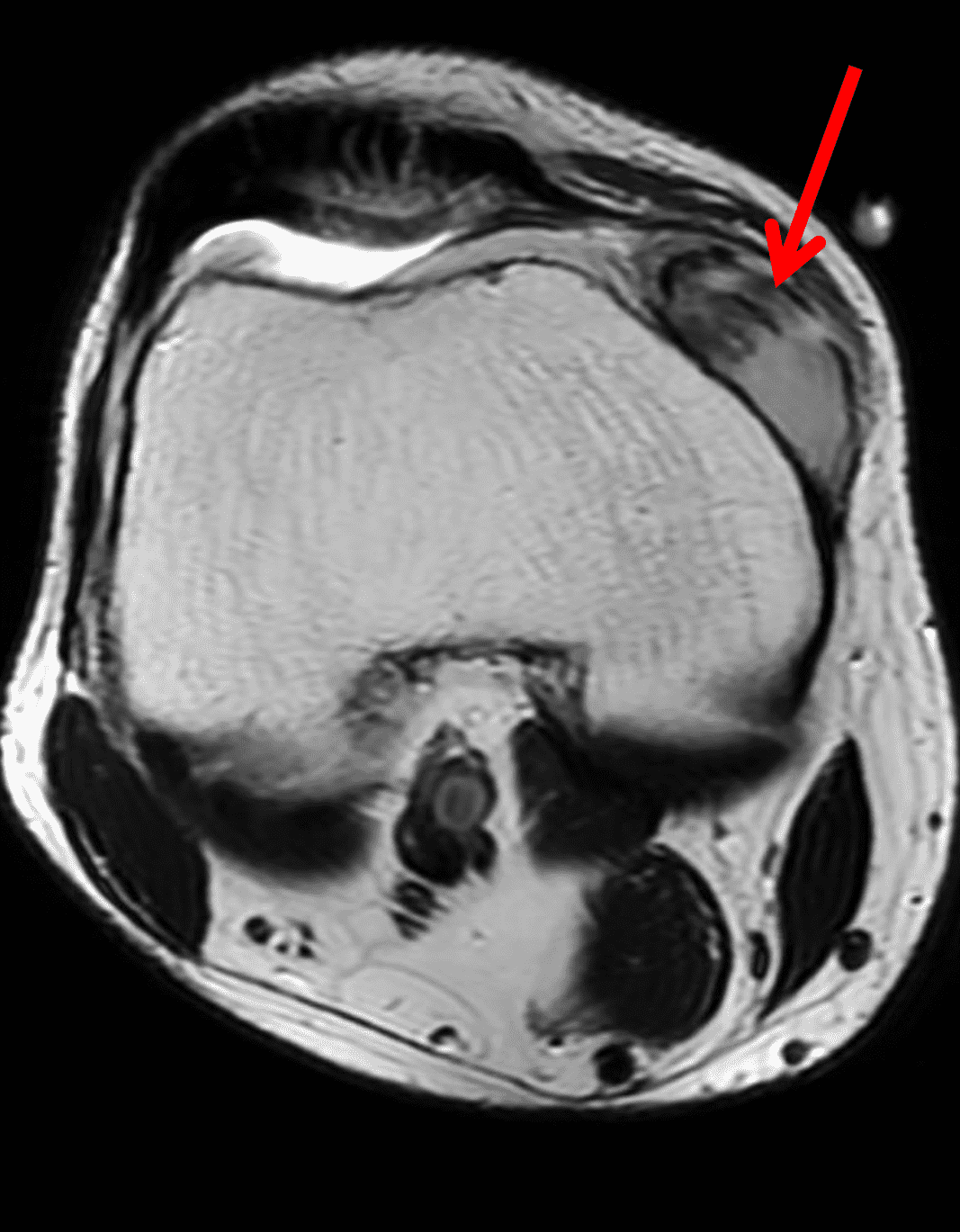
Figure 21: Histologically-proved intra-articular synovial sarcoma in the knee joint. (21A) Sagittal fat-suppressed proton-density weighted and (21B) axial T2-weighted images demonstrate an intra-articular ovoid mass (arrows) demonstrating areas of T2 hyperintensity, intermediate signal and hypointensity (triple sign).
Intra-articular Nodular Fasciitis
Nodular fasciitis is a benign mesenchymal neoplasm of myofibroblastic proliferation that is typically self-limiting. It is associated with recurrent gene fusions, MYH9:USP6 being the most common fusion product, although other USP6 partners have been identified. Nodular fasciitis can occur in multiple sites of the body, most commonly in the subcutaneous, fascial and muscular tissues. It is rarely found within the joints, with apparent predilection for the knee joint. Nodular fasciitis can occur at any age, most commonly in young adults between 20-40 years old. Rapid growth, high cellularity and mitotic rate histologically can mimic malignancy. Intra-articular nodular fasciitis usually presents in a more indolent fashion compared to the more common extra-articular type. Patients usually complain of pain, swelling and restriction of joint motion, with a possible palpable mass around the joint. In some cases, prior injury may be reported. Overall, MRI features are non-specific in the intra-articular form, usually presenting as an ovoid mass with intermediate to hypointense T1 and hyperintense T2 signal, and heterogenous contrast enhancement (Figure 22). Most reported cases have been surgically resected.41,42,43,44,45,46
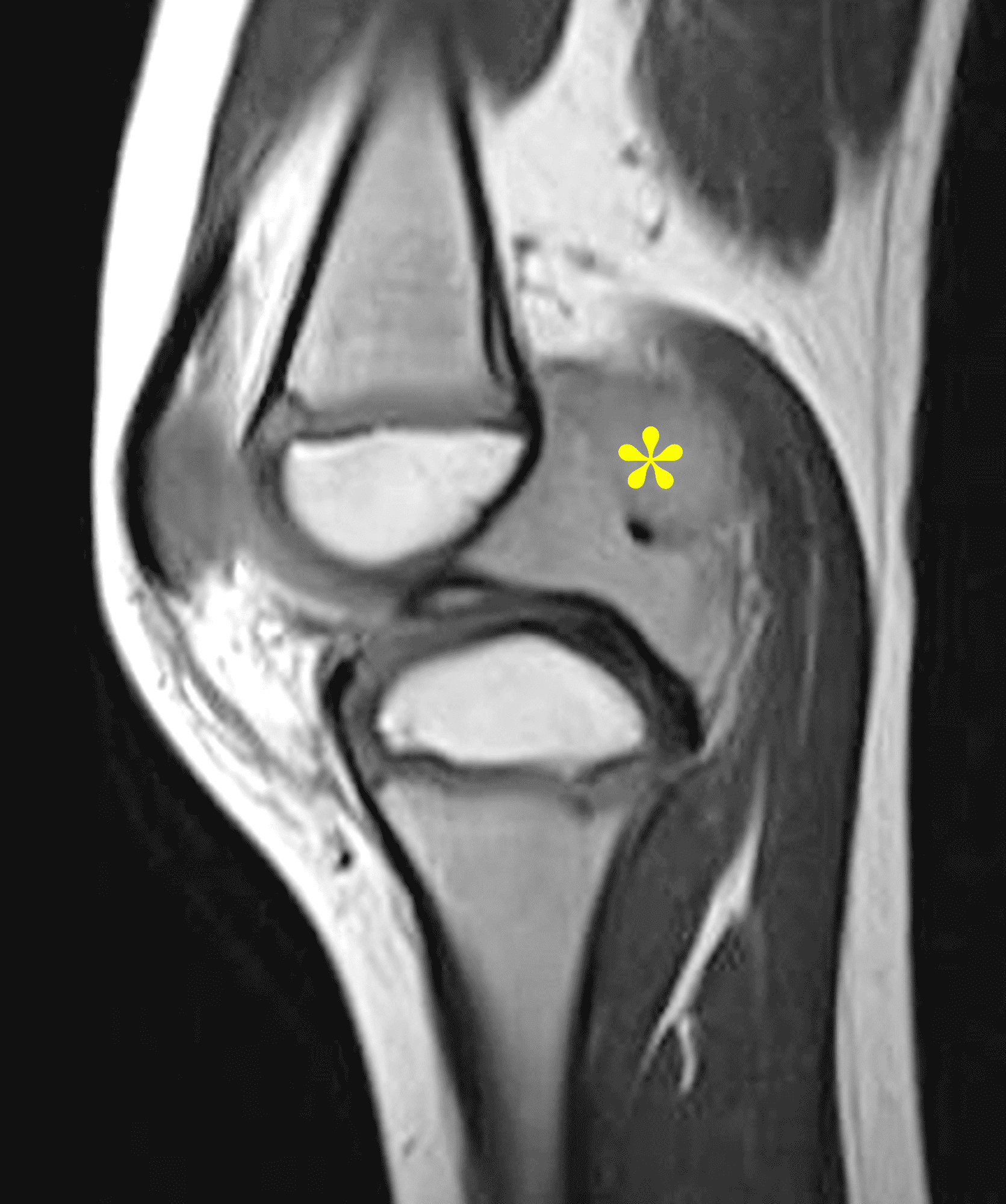
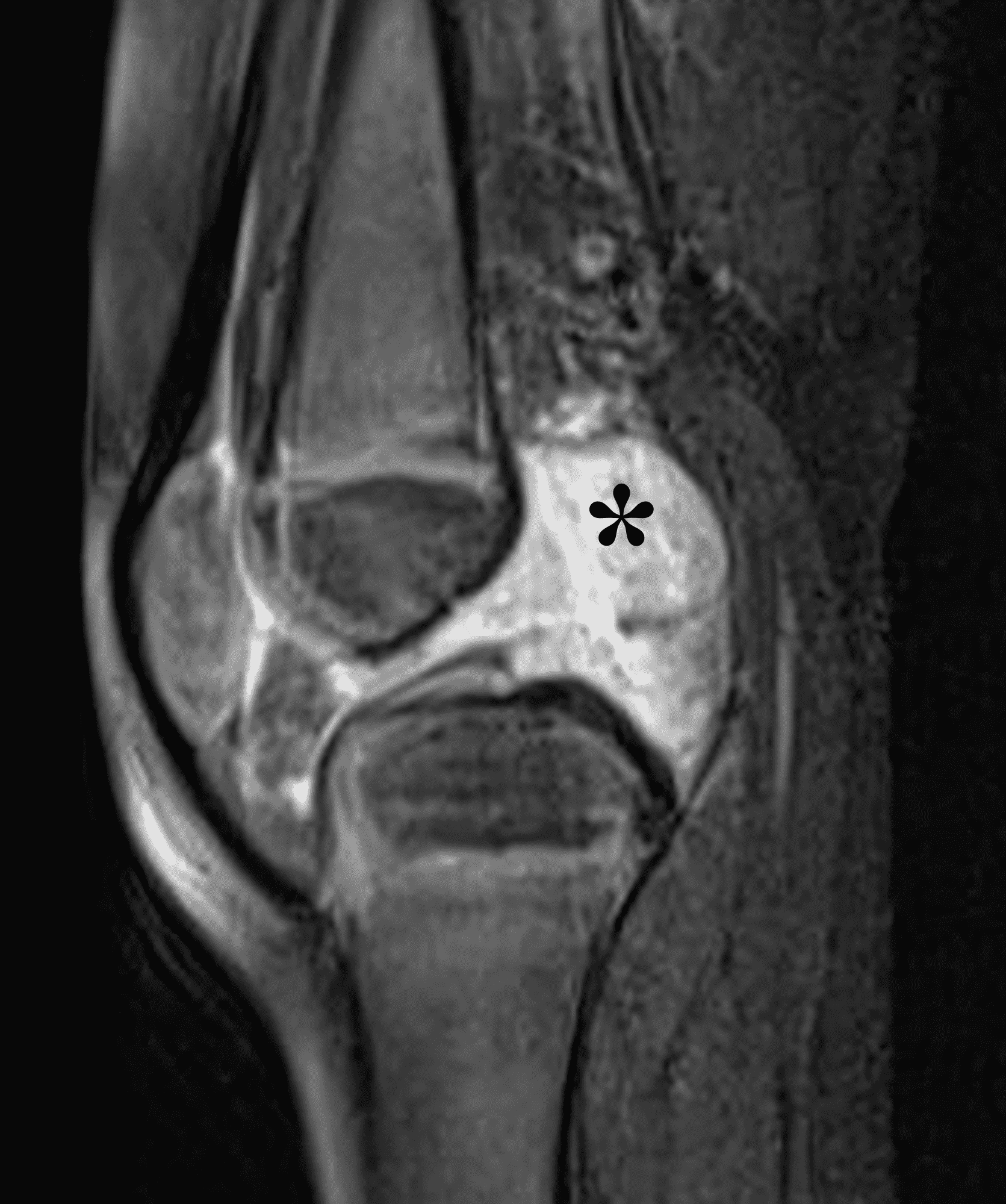
Figure 22: Intra-articular nodular fasciitis in the knee. Sagittal (22A) proton density-weighted and (22B) fat-suppressed fluid-sensitive images demonstrate a non-specific large intra-articular T2 hyperintense mass (asterisks).
Ganglion Cyst
Intra-articular and periarticular ganglion cysts are seen relatively commonly on MRI. They are well marginated masses containing gelatinous contents and surrounded by a dense connective tissue capsule. Ganglion cysts commonly occur around the anterior cruciate ligament (ACL), especially near its tibial insertion. Ganglion cysts have characteristic imaging features on MRI, with a well circumscribed mass demonstrating fluid signal on all sequences, sometimes with thin septations, and thin hypointense walls (Figure 23). However, depending on the complexity of the fluid, there may be more heterogeneous signal foci within the mass. If intravenous contrast is administered, there is typically a thin peripheral enhancing rim but no internal enhancement.1
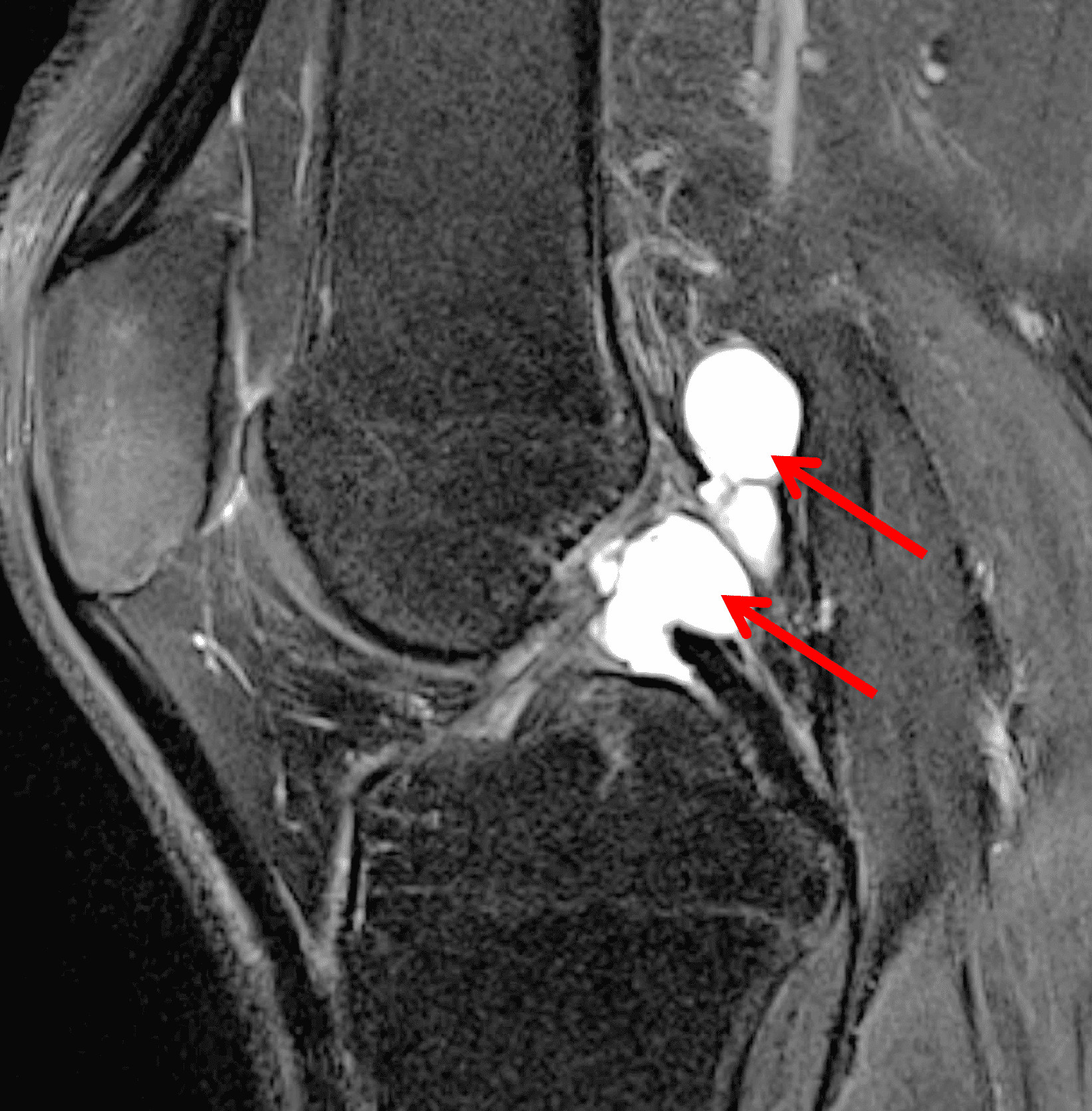
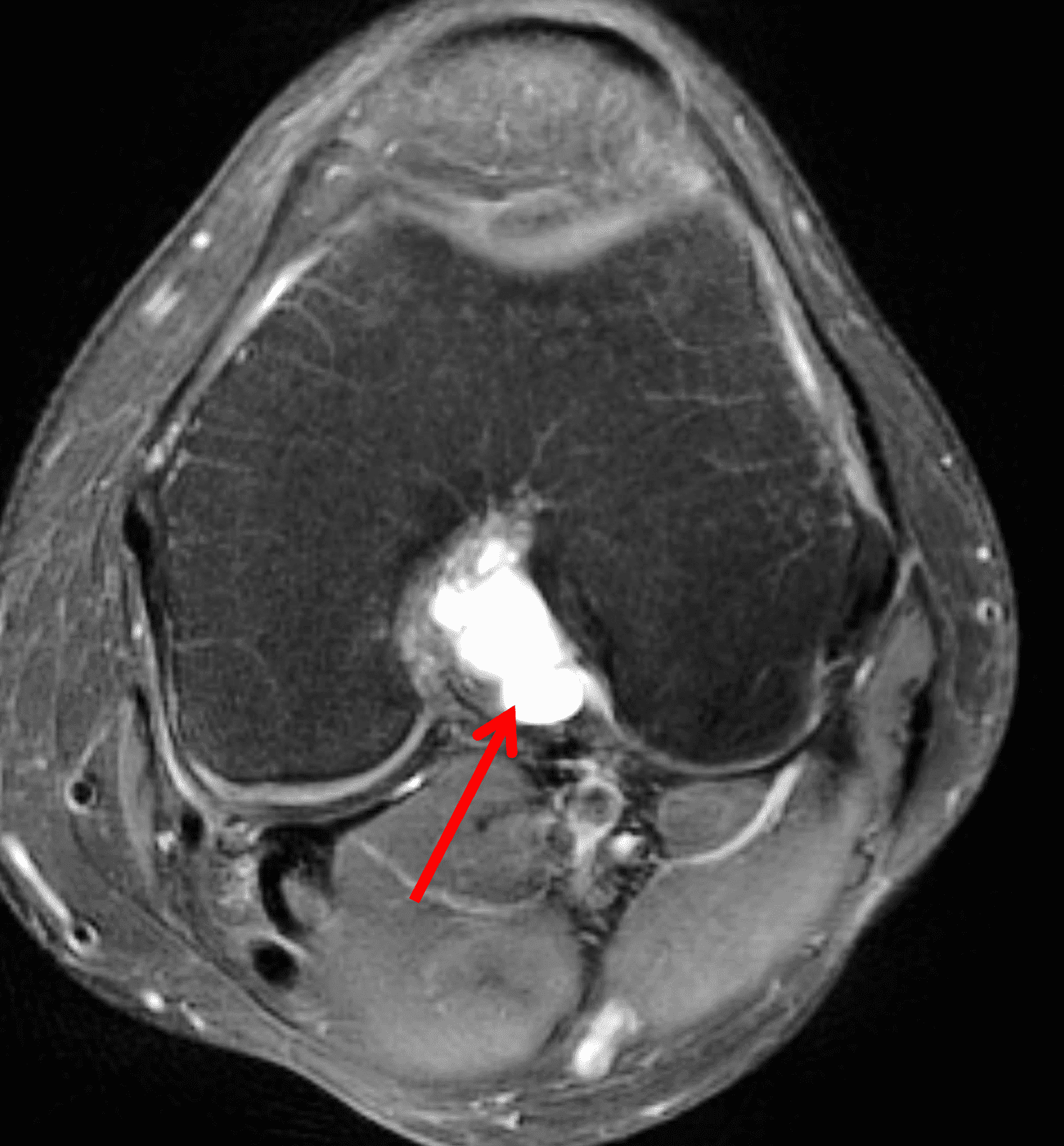
Figure 23: Cruciate ganglion cyst in the knee. (23A) Sagittal and (23B) axial fat-suppressed fluid-sensitive images demonstrate a lobulated, homogeneously T2 hyperintense mass (arrows) in the intercondylar notch, adjacent to the anterior and posterior cruciate ligaments.
Cyclops Lesion (Arthrofibrosis)
A cyclops lesion is a reactive mass almost always seen in the intercondylar notch anterior to an ACL graft, thought to arise as a reaction to debris from tibial tunnel drilling or possibly to repetitive microtrauma of the ACL graft. Rare cases have been reported in native knee joints, which are thought to be related to prior ligamentous injury. These masses can be divided histologically into true cyclops and cyclopoid lesions. True cyclops lesions demonstrate fibrocartilaginous proliferation with central ossification, while cyclopoid lesions demonstrate fibrocartilaginous proliferation with surrounding granulation tissue. True cyclops lesions are more likely to cause graft impingement and are usually resected for symptomatic relief. Cyclops lesions are seen in up to 25% ACL reconstructions. Most are managed conservatively unless symptomatic, and have been shown to not affect clinical outcomes at 2 years. On MRI, there is usually a well circumscribed ovoid mass anterior to the ACL graft, demonstrating intermediate T1 signal, variable T2 signal, and sometimes central ossification (Figure 24).1


Figure 24: Cyclops lesion. Sagittal (24A) proton density-weighted and (24B) fat-suppressed fluid-sensitive images of the knee demonstrate an ovoid circumscribed T2 hypointense mass (arrows) anterior to an anterior cruciate ligament reconstruction graft.
Other intra-articular degenerative masses include intra-articular loose bodies which demonstrate variable signal depending on the cartilaginous or ossification pattern, meniscal ossicles and post-surgical scarring.2
Additional Rare Benign and Malignant Tumors
Extra-skeletal chondroma is a rare benign intra- or para-articular tumor, usually occurring about the knee, arising from the joint capsule or surrounding connective tissues. The lesion is commonly found in the infra-patellar fat pad, with variable amount of internal ossification.1 The tumors are usually large at time of diagnosis and may cause erosion of the adjacent tibia. Imaging characteristics follow typical chondroid characteristics. Treatment consists of surgical excision with low risk of recurrence.1
Myopericytoma, a rare tumor usually located in the dermal and subcutaneous tissues, consisting of a concentric proliferation of myoid cells has been described in the knee, appearing as a nonspecific T2 hyperintense mass.3
Solitary fibrous tumor is a rare spindle cell neoplasm of mesenchymal origin most commonly involving the pleura but also occurring elsewhere and rarely within a joint. MRI characteristics are non-specific, including isointense T1, and mildly hyperintense T2 signal and sometimes demonstrating T2 hypointense internal foci, and avid contrast enhancement.47,48
Glomus tumor is a mesenchymal tumor of modified smooth muscle cells arising from the glomus body. They are usually very painful, with cold sensitivity and tenderness to palpation. Glomus tumors most commonly arise in the subungual region and usually demonstrate hyperintense T2 and isointense to hypointense T1 signal with avid contrast enhancement. They have been described in the knee and glenohumeral joints with nonspecific imaging characteristics on MRI, with avid contrast enhancement.49,50
Metastatic disease to the synovium can rarely occur, most commonly due to lung adenocarcinoma although others have been described, such as metastatic chordoma and melanoma.2-4
Other intra-articular benign and malignant masses reported in the literature include but are not limited to: neurofibroma, fibroma, aggressive fibromatosis, benign fibrous histiocytoma, spindle cell sarcoma, undifferentiated pleomorphic sarcoma, myxofibrosarcoma, leiomyosarcoma, fibrosarcoma, epithelioid sarcoma and lymphoma.2,3,51,52,53
Any bone neoplasm near a joint can potentially invade the joint space, including benign and malignant processes (Figure 25).2
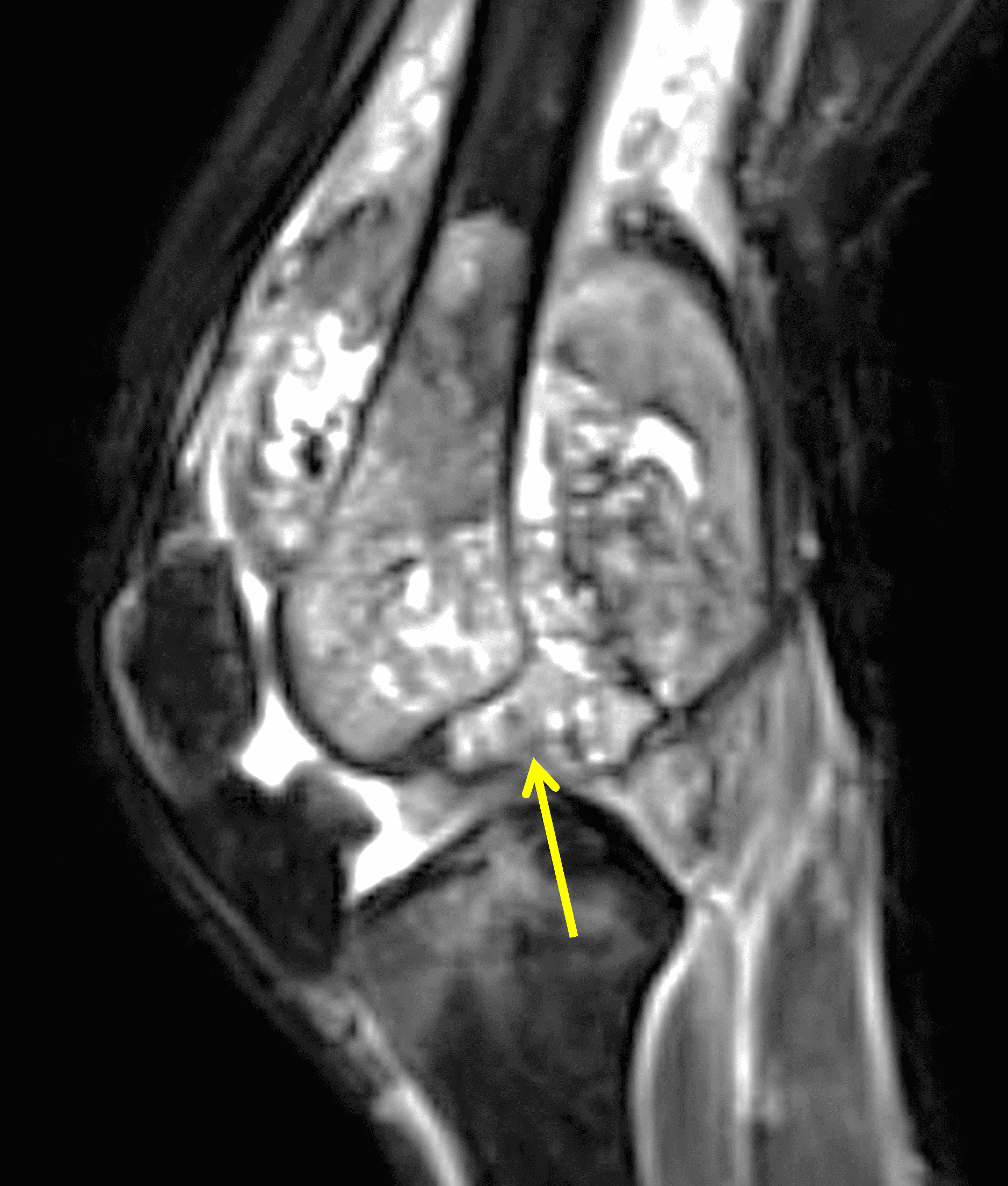
Figure 25: Telangiectatic osteosarcoma of the distal femur invading the knee joint. Sagittal fat-suppressed fluid-sensitive image of the knee demonstrates a large, heterogeneous destructive mass in the medullary space of the distal femur, with an associated large surrounding soft tissue mass, and invasion into the joint (arrow).
Conclusion
The differential diagnosis of intra-articular masses and mass-like processes is relatively small for the lesions commonly encountered in daily practice. However, it is important to recognize that many less common benign and malignant process can also occur in or around a joint. Familiarity with the MRI appearances and clinical presentations can help decrease the risk of an incorrect diagnosis.
References
- Rudd A, Pathria MN. Intra-articular Neoplasms and Masslike Lesions of the Knee: Emphasis on MR Imaging. Magn Reson Imaging Clin N Am. 2022;30(2):339-350. doi:10.1016/J.MRIC.2021.11.011 ↩
- Dhanda S, Quek ST, Bathla G, Jagmohan P. Intra-articular and Peri-articular Tumours and Tumour Mimics- What a Clinician and Onco-imaging Radiologist Should Know. Malays J Med Sci. 2014;21(2):4-19. ↩
- Ghosn Y, Alam R, El Annan T, et al. Para-articular and intra-articular soft tissue lesions: Radiologic-pathologic correlation. Eur J Radiol. 2024;181:111718. doi:10.1016/j.ejrad.2024.111718 ↩
- Sheldon PJ, Forrester DM, Learch TJ. Imaging of Intraarticular Masses. RadioGraphics. 2005;25(1):105-119. doi:10.1148/rg.251045050 ↩
- Stacchiotti S, Dürr HR, Schaefer IM, et al. Best clinical management of tenosynovial giant cell tumour (TGCT): A consensus paper from the community of experts. Cancer Treat Rev. 2023;112:102491. doi:10.1016/j.ctrv.2022.102491 ↩
- Bansal A, Goyal S, Goyal A, Jana M. WHO classification of soft tissue tumours 2020: An update and simplified approach for radiologists. Eur J Radiol. 2021;143:109937. doi:10.1016/j.ejrad.2021.109937 ↩
- Spierenburg G, Suevos Ballesteros C, Stoel BC, et al. MRI of diffuse-type tenosynovial giant cell tumour in the knee: a guide for diagnosis and treatment response assessment. Insights Imaging. 2023;14(1):22. doi:10.1186/s13244-023-01367-z ↩
- Amary F, Perez-Casanova L, Ye H, et al. Synovial chondromatosis and soft tissue chondroma: extraosseous cartilaginous tumor defined by FN1 gene rearrangement. Modern Pathology. 2019;32(12):1762-1771. doi:10.1038/s41379-019-0315-8 ↩
- Kramer J, Recht M, Deely DM, et al. MR Appearance of Idiopathic Synovial Osteochondromatosis. J Comput Assist Tomogr. 1993;17(5):772-776. doi:10.1097/00004728-199309000-00020 ↩
- Bertoni F, Krishnan Unni K, Beabout JW, Sim FH. Chondrosarcomas of the synovium. Cancer. 1991;67(1):155-162. doi:10.1002/1097-0142(19910101)67:1<155::AID-CNCR2820670127>3.0.CO;2-W ↩
- McCarthy C, Anderson WJ, Vlychou M, et al. Primary synovial chondromatosis: a reassessment of malignant potential in 155 cases. Skeletal Radiol. 2016;45(6):755-762. doi:10.1007/s00256-016-2353-3 ↩
- Schlachter TR, Wu Q, Matlyuk-Urman Z. AIRP Best Cases in Radiologic-Pathologic Correlation: Synovial Chondrosarcoma. RadioGraphics. 2011;31(7):1883-1888. doi:10.1148/rg.317105210 ↩
- Ryu KN, Jaovisidha S, Schweitzer M, Motta AO, Resnick D. MR imaging of lipoma arborescens of the knee joint. American Journal of Roentgenology. 1996;167(5):1229-1232. doi:10.2214/ajr.167.5.8911186 ↩
- Dawson JS, Dowling F, Preston BJ, Neumann L. Lipoma arborescens of the sub-deltoid bursa. Br J Radiol. 1995;68(806):197-199. doi:10.1259/0007-1285-68-806-197 ↩
- Chae EY, Chung HW, Shin MJ, Lee SH. Lipoma arborescens of the glenohumeral joint causing bone erosion: MRI features with gadolinium enhancement. Skeletal Radiol. 2009;38(8):815-818. doi:10.1007/s00256-009-0686-x ↩
- Girish G, Glazebrook KN, Jacobson JA. Advanced Imaging in Gout. American Journal of Roentgenology. 2013;201(3):515-525. doi:10.2214/AJR.13.10776 ↩
- Chowalloor PV, Siew TK, Keen HI. Imaging in gout: A review of the recent developments. Ther Adv Musculoskelet Dis. 2014;6(4):131-143. doi:10.1177/1759720X14542960 ↩
- Kiss E, Keusch G, Zanetti M, et al. Dialysis-Related Amyloidosis Revisited. American Journal of Roentgenology. 2005;185(6):1460-1467. doi:10.2214/AJR.04.1309 ↩
- Żyluk A. Calcium pyrophosphate dihydrate deposition disease (chondrocalcinosis): a review. Wiadomości Lekarskie. 2025;(2):402-409. doi:10.36740/WLek/200864 ↩
- Choi JA, Koh SH, Hong SH, Koh YH, Choi JY, Kang HS. Rheumatoid Arthritis and Tuberculous Arthritis: Differentiating MRI Features. American Journal of Roentgenology. 2009;193(5):1347-1353. doi:10.2214/AJR.08.2164 ↩
- Hong SH, Kim SM, Ahn JM, Chung HW, Shin MJ, Kang HS. Tuberculous versus Pyogenic Arthritis: MR Imaging Evaluation. Radiology. 2001;218(3):848-853. doi:10.1148/radiology.218.3.r01fe27848 ↩
- Sanghvi DA, Iyer VR, Deshmukh T, Hoskote SS. MRI features of tuberculosis of the knee. Skeletal Radiol. 2009;38(3):267-273. doi:10.1007/s00256-008-0617-2 ↩
- McConnell MF, Shi A, Lasco TM, Yoon L. Disseminated coccidioidomycosis with multifocal musculoskeletal disease involvement. Radiol Case Rep. 2017;12(1):141-145. doi:10.1016/j.radcr.2016.11.017 ↩
- Gualtierotti R, Solimeno LP, Peyvandi F. Hemophilic arthropathy: Current knowledge and future perspectives. Journal of Thrombosis and Haemostasis. 2021;19(9):2112-2121. doi:10.1111/jth.15444 ↩
- Park EJ, Kim YU, Kim J, Hyun CL, Lee KR, Kim J. A Case of Rheumatoid Arthritis Presenting as an Intra-articular Mass of the Wrist Joint in a Patient with Chronic Monoarthritis. Journal of Rheumatic Diseases. 2015;22(5):298. doi:10.4078/jrd.2015.22.5.298 ↩
- Sommer OJ, Kladosek A, Weiler V, Czembirek H, Boeck M, Stiskal M. Rheumatoid Arthritis: A Practical Guide to State-of-the-Art Imaging, Image Interpretation, and Clinical Implications. RadioGraphics. 2005;25(2):381-398. doi:10.1148/rg.252045111 ↩
- Kgoebane K, Ally MMTM, Duim-Beytell MC, Suleman FE. The role of imaging in rheumatoid arthritis. South African Journal of Radiology. 2018;22(1). doi:10.4102/sajr.v22i1.1316 ↩
- Porko S, Chowdhuri C, Barsagade AK, Priya S, Mustafa M. An Unusual and Rare Location of Intra-articular Rheumatoid Nodule in the Elbow Joint – A Case Report. Cureus. Published online March 27, 2023. doi:10.7759/cureus.36747 ↩
- Su H, Gong Y, Chen L, et al. Xanthoma combining osteonecrosis in knee joint: a case report. BMC Musculoskelet Disord. 2024;25(1):666. doi:10.1186/s12891-024-07776-5 ↩
- Kunimoto K, Yamamoto Y, Jinnin M. ISSVA Classification of Vascular Anomalies and Molecular Biology. Int J Mol Sci. 2022;23(4):2358. doi:10.3390/ijms23042358 ↩
- Abdulwahab AD, Tawfeeq DN, Sultan OM. Intra-articular Synovial Hemangioma: A Rare Cause of Knee Pain and Swelling. J Clin Imaging Sci. 2021;11:26. doi:10.25259/JCIS_129_2020 ↩
- Shafqat A, Shafqat S, Ahmed TM, et al. A Rare Presentation of a True Intra-articular Lipoma: A Case Report and Review of Imaging Findings. Cureus. Published online May 18, 2022. doi:10.7759/cureus.25094 ↩
- Poorteman L, Declercq H, Natens P, Wetzels K, Vanhoenacker F. Intra-articular synovial lipoma of the knee joint. BJR|case reports. 2015;1(2):20150061. doi:10.1259/bjrcr.20150061 ↩
- Mettu S, Gavvala SN, Iyengar KP, Papineni VRK, Botchu R. Intra-articular lipoma of the hip joint – A report of two cases and literature review. Journal of Arthroscopic Surgery and Sports Medicine. 2024;6:74. doi:10.25259/JASSM_24_2024 ↩
- Mells AJ, Gosey GM, Muldoon MP. Intra-articular lipoma of the hip. BMJ Case Rep. 2017;2017:bcr-2017-220349. doi:10.1136/bcr-2017-220349 ↩
- Ishida N. Intra-articular Lipoma of the Knee Joint Located in the Lateral Recess: A Case Report. J Orthop Case Rep. 2021;11(8). doi:10.13107/jocr.2021.v11.i08.2364 ↩
- Shaerf DA, Mann B, Alorjani M, Aston W, Saifuddin A. High-grade intra-articular liposarcoma of the knee. Skeletal Radiol. 2011;40(3):363-365. doi:10.1007/s00256-010-1070-6 ↩
- Claudi C, Andreisek G, Vrugt B, Ganser J. A Juxta-Articular Myxoma of the Thumb. J Hand Surg Glob Online. 2020;2(3):171-174. doi:10.1016/j.jhsg.2020.04.002 ↩
- Meis JM, Enzinger FM. Juxta-articular myxoma: A clinical and pathologic study of 65 cases. Hum Pathol. 1992;23(6):639-646. doi:10.1016/0046-8177(92)90319-X ↩
- Justin E H, Ryan P F, Austin H, et al. Primary Intra-Articular Synovial Sarcoma of the Knee: A Report of Two Cases and Review of the Literature. International Journal of Radiology and Imaging Technology. 2018;4(1). doi:10.23937/2572-3235.1510031 ↩
- Patel NR, Chrisinger JSA, Demicco EG, et al. USP6 activation in nodular fasciitis by promoter-swapping gene fusions. Modern Pathology. 2017;30(11):1577-1588. doi:10.1038/MODPATHOL.2017.78 ↩
- Miyama A, Kuratsu S, Takenaka S, et al. Two case reports of intra-articular nodular fasciitis of the knee confirmed by MYH9-USP6 gene fusion expression. Journal of Orthopaedic Science. 2021;26(6):1138-1142. doi:10.1016/J.JOS.2018.12.008 ↩
- Coyle J, White LM, Dickson B, Ferguson P, Wunder J, Naraghi A. MRI characteristics of nodular fasciitis of the musculoskeletal system. Skeletal Radiol. 2013;42(7):975-982. doi:10.1007/s00256-013-1620-9 ↩
- Hornick JL, Fletcher CDM. Intraarticular Nodular Fasciitis-A Rare Lesion. American Journal of Surgical Pathology. 2006;30(2):237-241. doi:10.1097/01.pas.0000180441.48904.50 ↩
- Wang W, Huang Y, Wang C, et al. Intra-articular nodular fasciitis: a rare lesion case report and an updated review of the literature. BMC Musculoskelet Disord. 2019;20(1):5. doi:10.1186/s12891-018-2375-1 ↩
- Kwon OH, Cho KH, Suh JH, Choi JH. Intra-Articular Nodular Fasciitis of the Knee: A Case Report of MRI Findings. Journal of the Korean Society of Radiology. 2014;71(5):254. doi:10.3348/jksr.2014.71.5.254 ↩
- Hyodo R, Komada T, Takada A, et al. Solitary fibrous tumors in the extremities: imaging findings for six patients. Nagoya J Med Sci. 2015;77(1-2):167-178. ↩
- Roth M, Alowami S, Popovic S, Harish S. Intra-articular solitary fibrous tumor of the knee. Skeletal Radiol. 2018;47(9):1305-1310. doi:10.1007/s00256-018-2906-8 ↩
- Sachdev R, Mohapatra I, Goel S, Gajendra S. Intra-articular glomus tumor– a rare presentation. Turkish Journal of Pathology. Published online 2017. doi:10.5146/tjpath.2016.01384 ↩
- Clark ML, O’Hara C, Dobson PJ, Smith AL. Glomus tumor and knee pain: A report of four cases. Knee. 2009;16(3):231-234. doi:10.1016/j.knee.2008.11.013 ↩
- Falconiero T, LaGreca M, Badragheh A, Jones N, Kester C. Intra-articular Knee Neurofibroma in a Patient with Neurofibromatosis: A Case Report and Review of Literature. J Orthop Case Rep. 2024;14(10):140-145. doi:10.13107/jocr.2024.v14.i10.4840 ↩
- Nottrott M, Streitbürger A, Gosheger G, Guder W, Hauschild G, Hardes J. Intra-articular soft-tissue sarcoma of the knee: Is extra-articular resection and tumor endoprosthetic reconstruction the solution? A retrospective report on eight cases. Orthop Rev (Pavia). 2019;11(1). doi:10.4081/or.2019.7764 ↩
- Zhang R, Liu J, Liu L, Lin Y, Zhang Q. Delayed diagnosis of pediatric intra-articular epithelioid sarcoma: a case report and literature review. BMC Pediatr. 2023;23(1):488. doi:10.1186/s12887-023-04305-6 ↩
