Clinical History
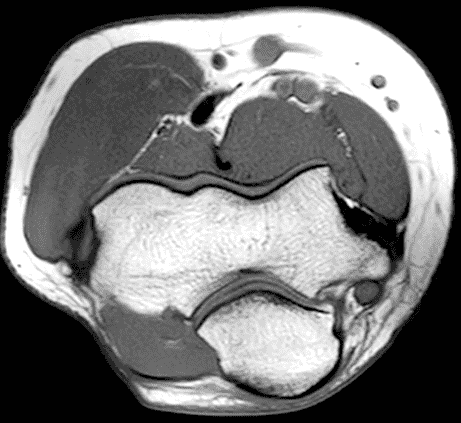
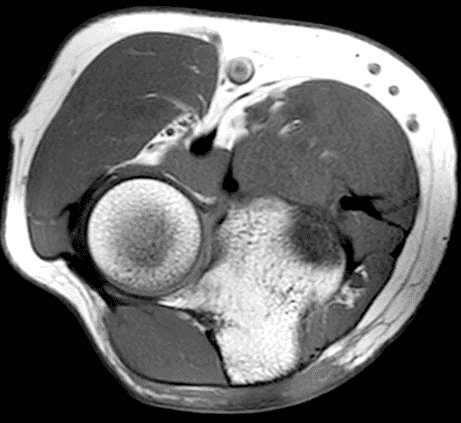
A 55-year-old man complains of pain, numbness, and tingling in the ulnar aspect of the hand and in the small and ring fingers. The symptoms are more severe with elbow flexion and during sleep. He has no muscle weakness or history of trauma. Axial T1-weighted (1A, 1B) and fat-suppressed, fluid-sensitive (1C, 1D) images are shown. What are the findings? What is your diagnosis?


Findings


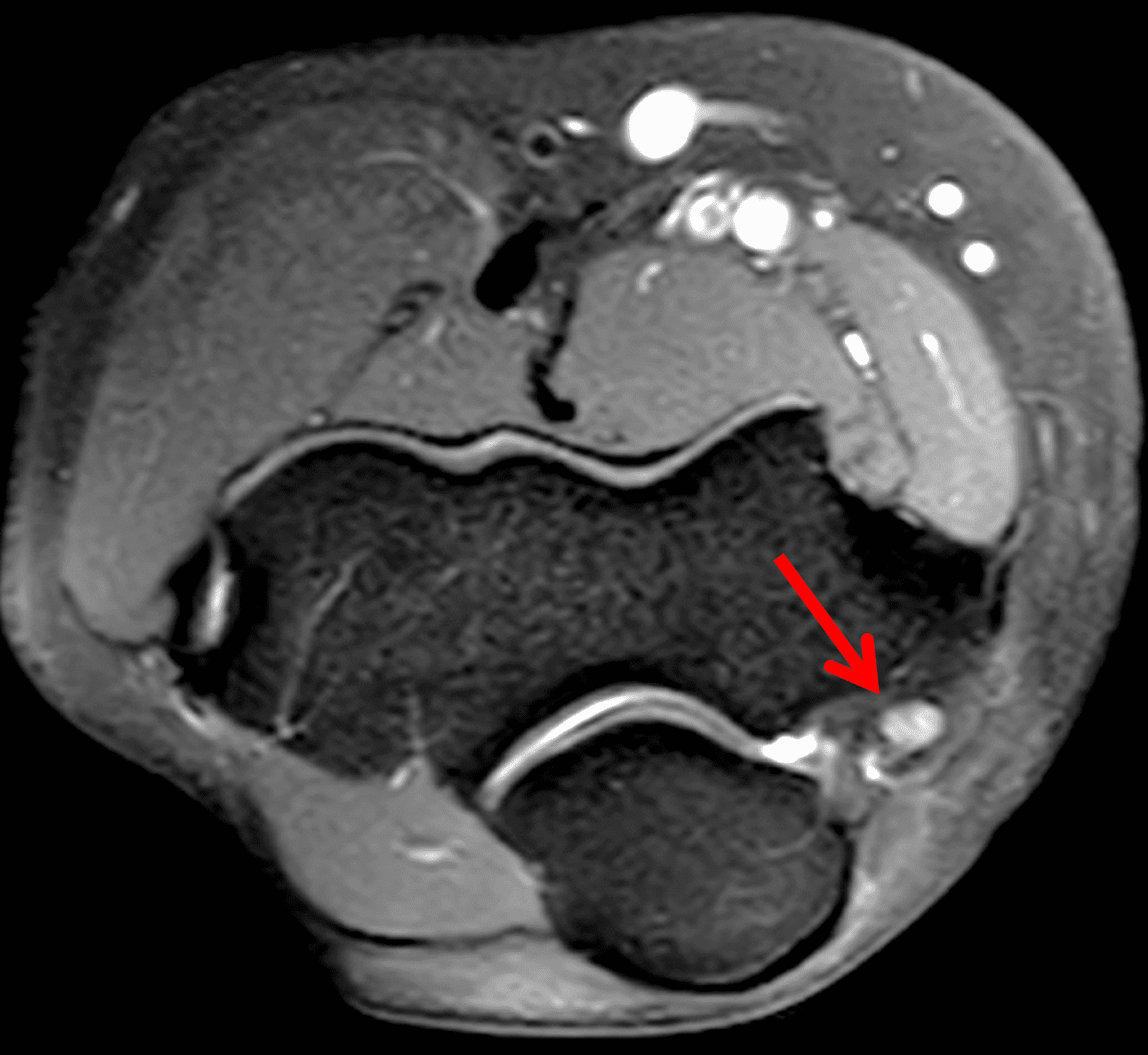
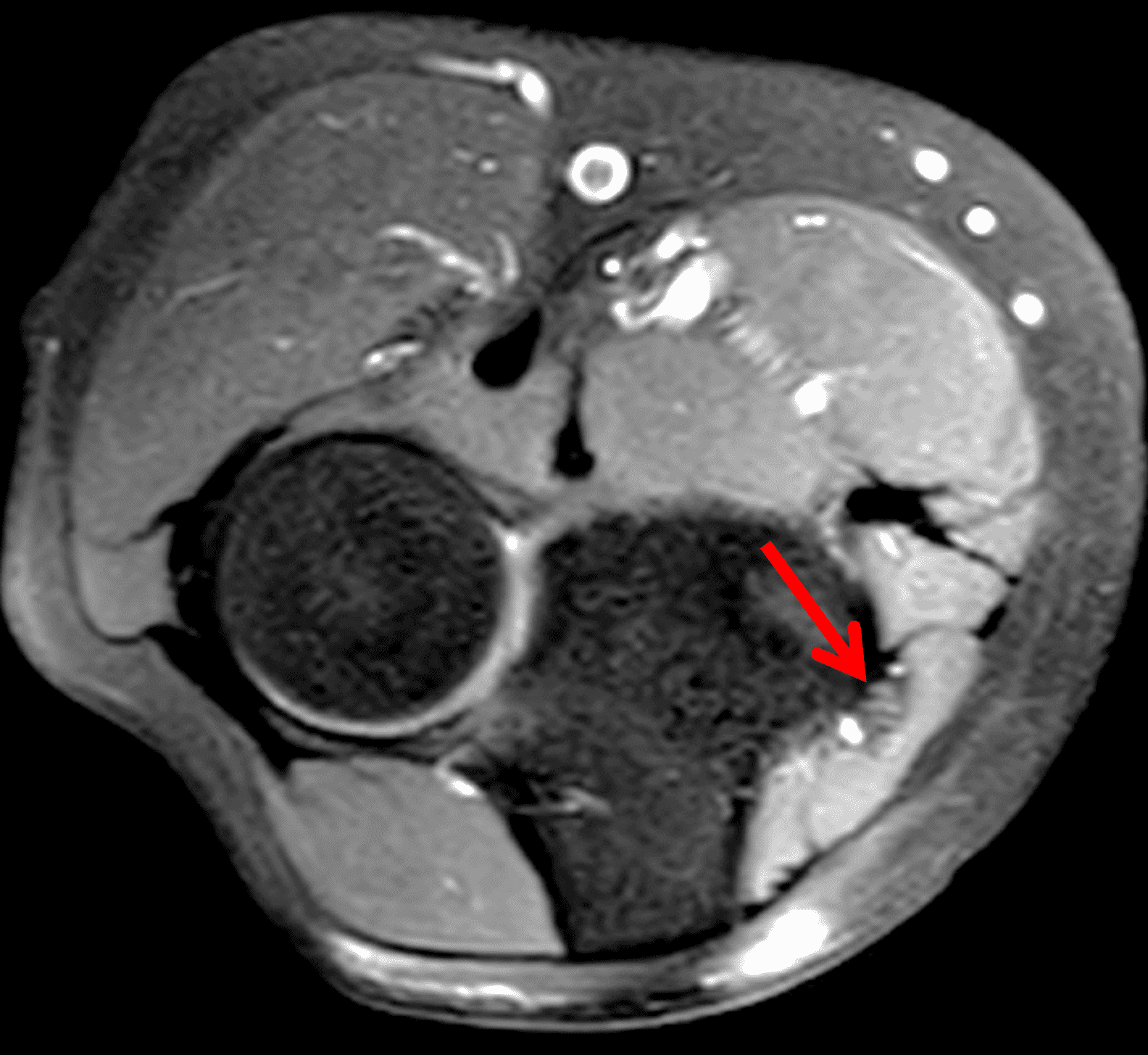
Figure 2: At the level of the cubital tunnel (2A and 2C), identifiable by the thin cubital tunnel retinaculum (yellow arrow), the ulnar nerve (red arrow) is focally enlarged and hyperintense compared to the nerve more distally (2B and 2D), where it lies between the two heads of the flexor carpi ulnaris muscle (asterisks). No soft tissue mass is present.
Diagnosis
Ulnar neuritis and cubital tunnel syndrome.
Introduction:
Median nerve compression in the carpal tunnel is the most common peripheral neuropathy in the upper extremity; ulnar neuropathy is the second most common.1 The ulnar nerve may be affected at multiple sites along it course, from above the elbow (typically at the arcade of Struthers) through the wrist at Guyon’s canal. But the most common location for ulnar nerve pathology is at the elbow, where the nerve traverses the cubital tunnel. In this location the ulnar nerve is susceptible to entrapment, compression, friction, and stretching due to a variety of causes. Imaging, particularly using MRI, plays a major role in evaluating the nerve and the surrounding tissues in patients presenting with ulnar nerve symptoms.
Relevant anatomy
The C8 and T1 nerve roots (and occasionally fibers from the C7 nerve root) contribute to the ulnar nerve, which originates from the medial cord of the brachial plexus. After traveling medial to the brachial artery in the arm, the nerve passes through the medial intermuscular septum into the posterior compartment near the insertion of the coracobrachialis muscle, passing under the aponeurotic arcade of Struthers. Next it courses along the posteromedial aspect of the humerus, through the cubital tunnel, and then between the two heads of the flexor carpi ulnaris muscle in the proximal forearm. More distally, the ulnar nerve lies between the flexor digitorum superficialis and profundus muscles, entering the wrist superficial to the flexor retinaculum. From there it travels through Guyon’s canal and into the hand.2
In the forearm, the ulnar nerve provides motor innervation to the flexor carpi ulnaris muscle as well as the medial half of the flexor digitorum profundus. Most of the muscles supplied by the nerve are in the hand, including the palmaris brevis, adductor pollicis, abductor digiti minimi, flexor digiti minimi, opponens digiti minimi, third and fourth lumbricals, and the palmar and dorsal interosseous muscles. Sensory branches supply the skin of the hypothenar eminence, small finger, ulnar half of the ring finger, and the ulnar aspect of the palm. Articular branches innervate the elbow and wrist joints.3
The cubital tunnel is a fibro-osseous space along the dorsoulnar aspect of the elbow joint, roughly triangular in cross-section (Figure 3). The medial humeral epicondyle and olecranon process of the proximal ulna form the anterior and lateral walls of the tunnel, respectively. A myofascial retinaculum joining these two bones (Osborne’s ligament) comprises the roof of the tunnel, and more distally the cubital tunnel retinaculum blends with a tendonous band that connects the two heads of the flexor carpi ulnaris muscle.4 Anatomic variations of the cubital tunnel retinaculum are common, and can contribute to the development of ulnar nerve pathology.5 The distal-most fibers of the medial head of the triceps muscle may extend into the proximal cranial portion of the cubital tunnel along the medial aspect of the olecranon. The posterior band of the ulnar collateral ligament (UCL) and the elbow joint capsule lie along the floor of the tunnel.6 The ulnar nerve and the posterior ulnar recurrent artery are located within the tunnel, surrounded by loose connective tissue and fat. The nerve can have one to several macroscopic fascicles, which may be visible on high-resolution ultrasound or fluid-weighted MRI studies (Figure 4).7,8
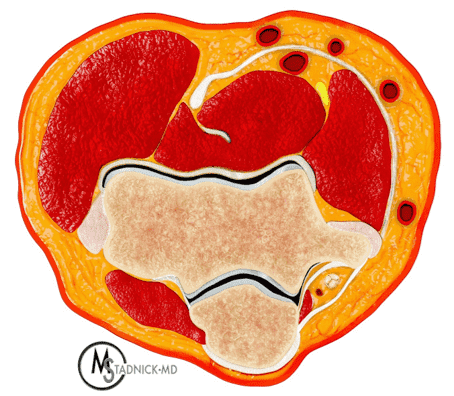
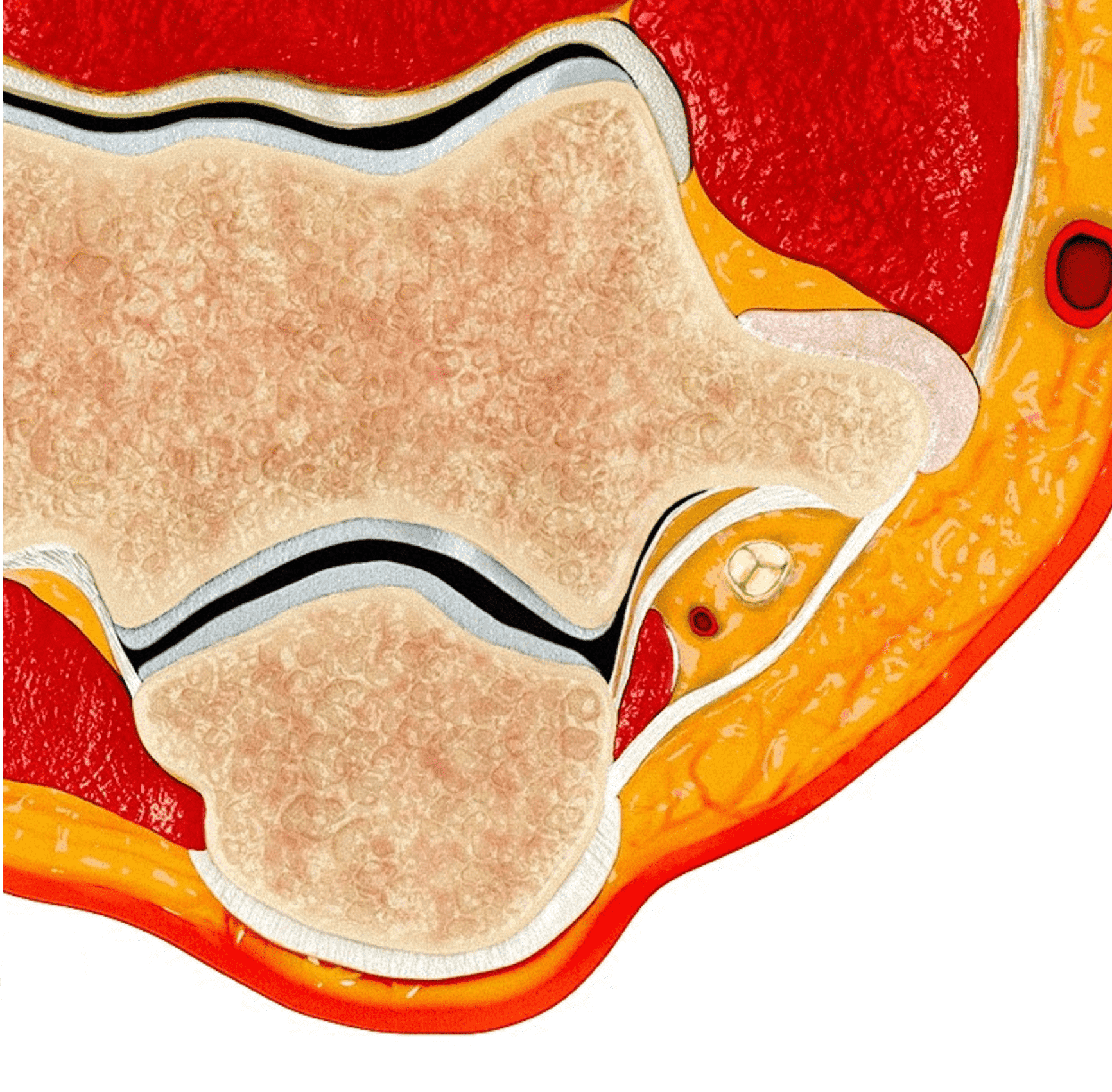

Figure 3: Normal cross-sectional anatomy of the cubital tunnel. (3A) Drawing showing a cross section of the elbow (3A) and an enlargement of the cubital tunnel (3B). The cubital tunnel retinaculum forms the roof of the tunnel. The posterior band of the ulnar collateral ligament and the posteromedial elbow joint capsule lie along the tunnel floor, and the distal muscle belly of the medial head of the triceps is present adjacent to the olecranon. The ulnar nerve and a branch of the ulnar artery are the main structures within the tunnel. Axial T1-weighted image (3C) demonstrates the corresponding anatomy: O = olecranon process of the proximal ulna, ME = medial humeral epicondyle, t = medial head triceps muscle, blue arrow = elbow joint capsule, red arrow = posterior band of the ulnar collateral ligament, arrowheads = cubital tunnel retinaculum, asterisk = ulnar nerve. The posterior ulnar recurrent artery is the round structure along the posterolateral aspect of the ulnar nerve.
Clinical presentation and diagnosis
The incidence of cubital tunnel syndrome is between 2% and 6% of the population, depending on the exact definition applied.9 Patients typically present with numbness and paresthesia in the dorsoulnar aspect of the hand and the palmar and dorsal surfaces of the small finger and ulnar half of the ring finger. Elbow flexion may exacerbate the symptoms, including during sleep. In cases of mild ulnar nerve compression, muscle findings are typically minimal or absent. With chronic compression (or following transection), patients may experience weakness in flexion of the wrist, ring finger, and small finger, together with loss of fine motor skills and trouble gripping.10 In severe chronic cases, patients can develop muscle atrophy and a claw hand deformity characterized by flexion of the interphalangeal joints and extension of the metacarpophalangeal joints of the small and ring fingers.11
Physical exam findings may include a positive Tinel’s sign over the cubital tunnel. Froment’s sign refers to weakness of the adductor pollicis manifest by an impaired pinch grip between the thumb and index finger. Similarly, weakness of the hypothenar muscles can produce involuntary abduction of the small finger, due to the unopposed preserved muscles (Wartenberg’s sign). In severe cases with profound muscle weakness, clawing of the ring and small fingers may be observed, together with visible atrophy of the hypothenar muscles.11 Nerve conduction studies are typically used to assess the degree of ulnar nerve dysfunction and identify the site of abnormality; because the symptoms of ulnar nerve compression at the elbow are mainly confined to the hand, similar findings can occur due to nerve entrapment in the wrist at Guyon’s canal. Similarly, symptoms of C8 radiculopathy or brachial plexopathy may overlap with those of cubital tunnel syndrome.12 Electromyography testing is often normal early in the course of cubital tunnel syndrome but will reveal denervation of the affected hand muscles in more advanced cases.10
Pathophysiology and etiology
The ulnar nerve is susceptible to stretching, friction, and compression in the cubital tunnel. Normally with flexion, the cross-sectional area of the tunnel decreases as the overlying retinaculum becomes taut, increasing pressure within the tunnel. Additionally, the path that the nerve follows increases in length with elbow flexion, meaning that the nerve must be able to stretch and glide smoothly to prevent dysfunction.13 In some patients the nerve becomes flattened and compressed due to these physiologic changes during elbow flexion, resulting in ulnar neuritis and “idiopathic” cubital tunnel syndrome, which is similar to carpal tunnel syndrome where the median nerve in compressed without the presence of a space-occupying mass. Anatomic variations like a thick cubital tunnel retinaculum (Figure 5), a relatively distal insertion of the medial triceps muscle (Figure 6), or a shallow groove in the posterior medial humeral epicondyle may increase the likelihood of nerve compression. The cross-sectional area and volume of the cubital tunnel are smaller in patients with idiopathic cubital tunnel syndrome compared to controls, especially with elbow flexion.14

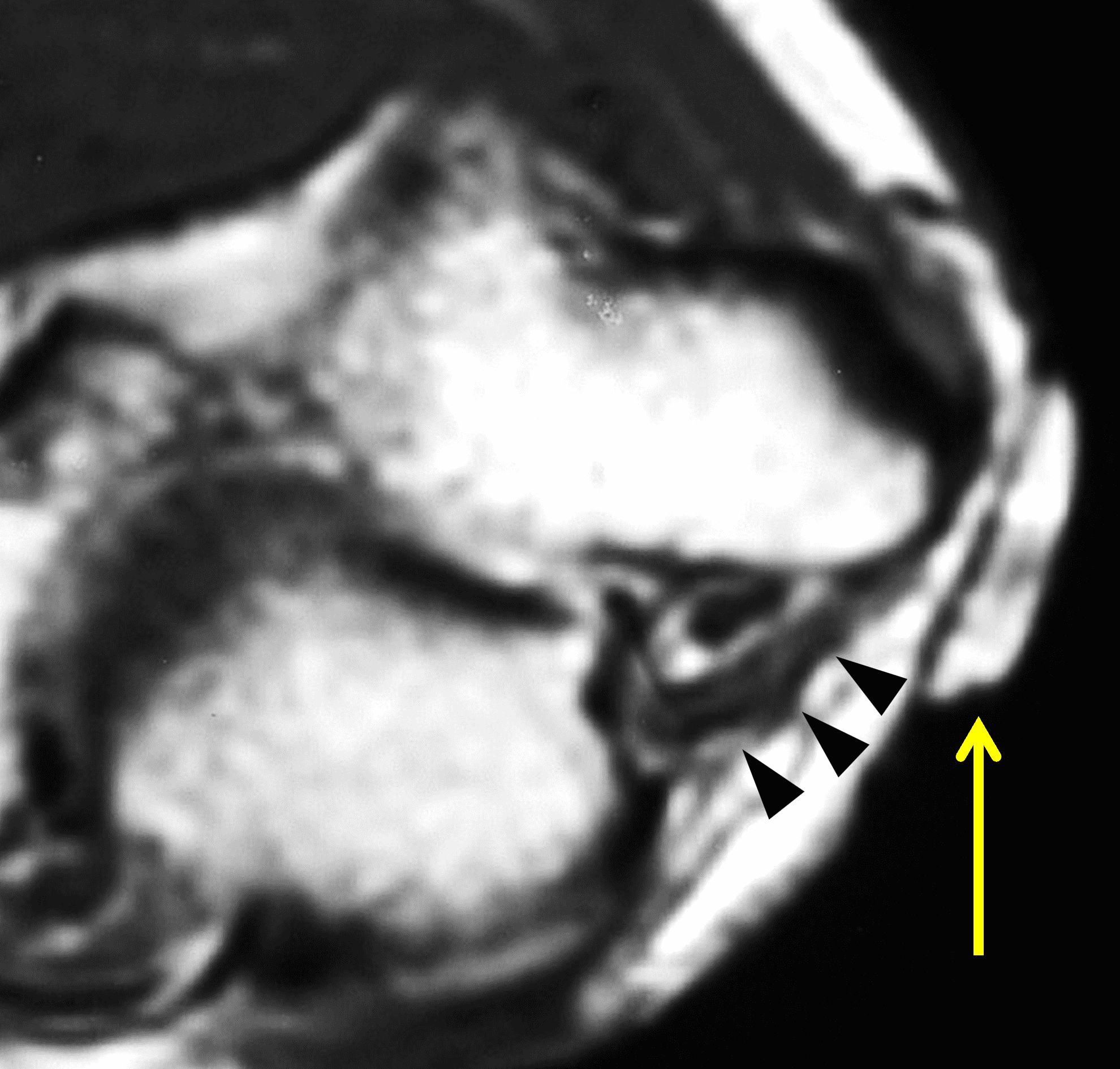
Figure 5: Thick cubital tunnel retinaculum. (5A) Drawing showing a thick retinaculum. Compare with Figure 3B. (5B) Axial T1-weighted image in a patient with clinical ulnar neuritis and a thick retinaculum (arrowheads) forming the roof of the cubital tunnel. This patient had a positive Tinel’s sign in the area localized by the placed marker (arrow).
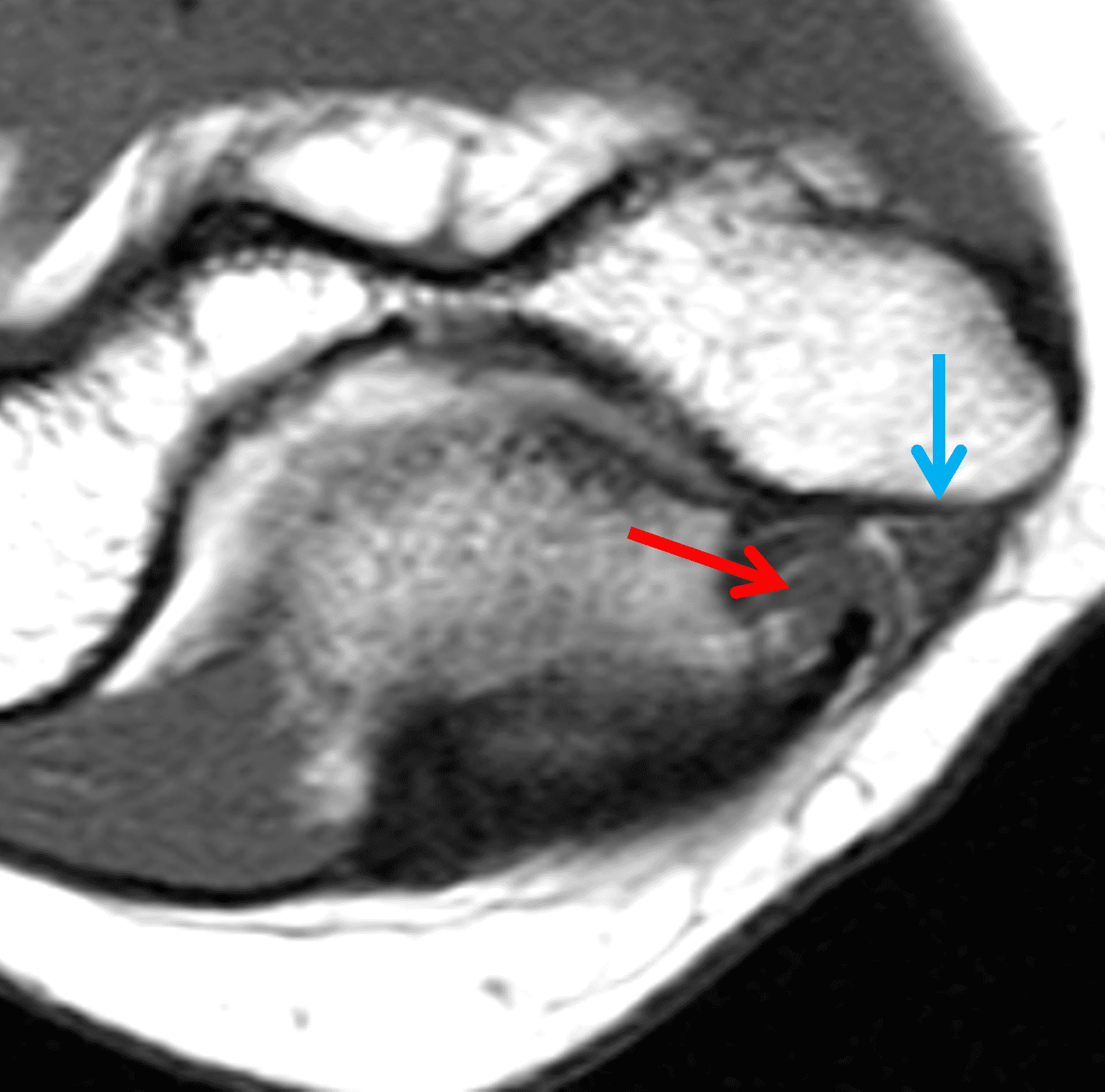
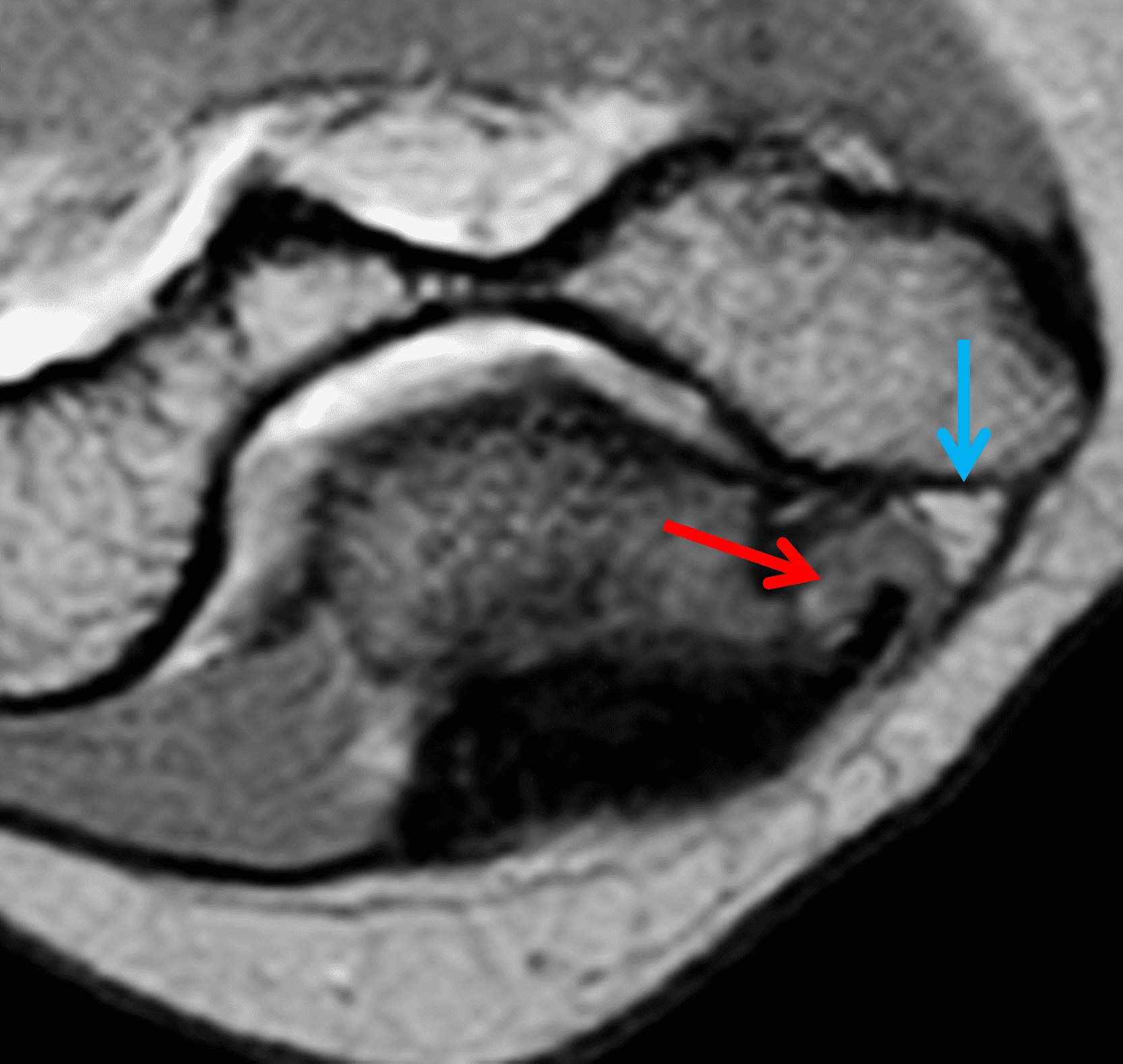
Figure 6: Cubital tunnel syndrome associated with an anomalous insertion of the medial head of the triceps. Axial (6A) T1-weighted and (6B) T2-weighted images at the level of the cubital tunnel retinaculum show the distal muscle belly and low signal-intensity tendon of the medial triceps (red arrows) filling more than half of the cubital tunnel cross-section. The ulnar nerve (blue arrows) is displaced by the muscle and appears compressed. This patient did not have any snapping or evidence of nerve subluxation with elbow flexion.
Various elbow conditions can also predispose to nerve compression at the cubital tunnel. Osteophytes originating from the posteromedial humeroulnar joint can decrease the area of the cubital tunnel and can also be a source of friction as the nerve glides. Prior malunited fractures of the distal humerus can alter the anatomy of the tunnel or result in increased cubital valgus,3 which stretches the nerve. Valgus extension overload – typically due to tears of the elbow UCL – can also lead to excessive stretching of the nerve with activities like baseball pitching.15 Less commonly, soft tissue masses like ganglia, proliferative conditions of the elbow synovium, posteromedial elbow loose bodies, and various tumors will directly compress the nerve.6
Intrinsic ulnar nerve abnormalities also occur in the cubital tunnel. The nerve is located relatively superficially and at risk for direct trauma, as may occur during sports.16 Nerve contusions result in an acute but transient shock-like pain and paresthesia in the forearm and hand, as anyone who has struck their “funny bone” can attest. Lacerations and transections of the nerve produce profound sensorimotor symptoms, which are permanent unless the nerve is repaired. A post-traumatic neuroma may follow a laceration.17 Mononeuritis or polyneuritis affecting the ulnar nerve can be caused by viral or other infections (including leprosy), collagen-vascular and autoimmune diseases, drug toxicity, diabetes, and other systemic conditions. Peripheral nerve sheath tumors can also involve the ulnar nerve.18
Lastly, the ulnar nerve is frequently mobile, and at risk of subluxation or dislocation. Absence or hypoplasia of the cubital tunnel retinaculum (Figure 7) predisposes the nerve to sublux or dislocate ulnarly with elbow flexion.6 Relative caudal extension of the medial head of the triceps can also increase the risk of nerve instability, which may be accompanied by a palpable or audible “snap” (or two) as the nerve and muscle belly dislocate over the medial humeral epicondyle with flexion, a condition called snapping triceps syndrome.19 It should be noted, however, that up to 30% of the population experience asymptomatic ulnar nerve dislocation.1


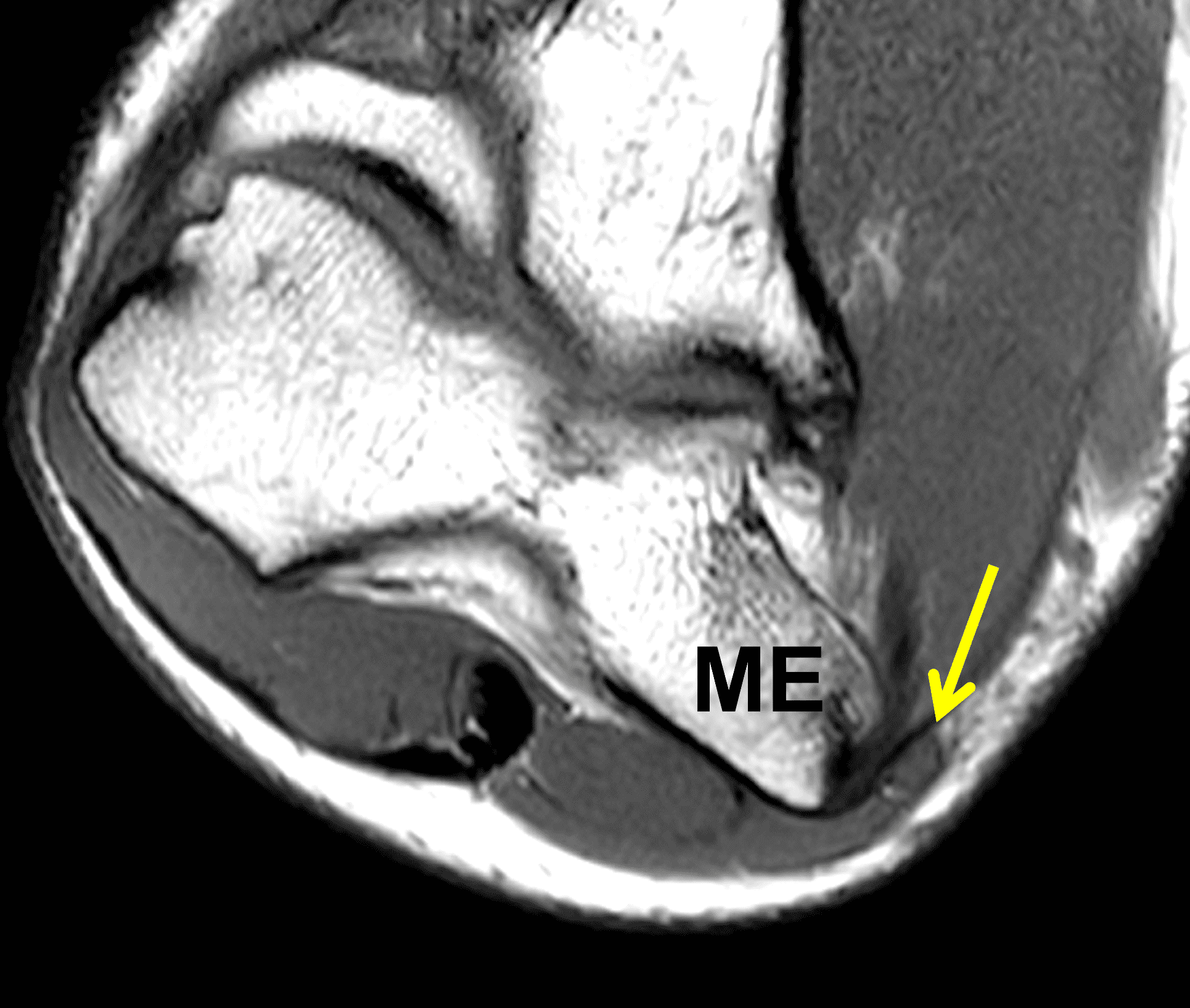

Figure 7: Absent cubital tunnel retinaculum. (7A) Drawing depicts absence of the retinaculum overlying the cubital tunnel contents. Compare with Figure 3B. (7B) Axial T1-weighted image with the elbow extended shows a normally-positioned ulnar nerve (arrow) with no defined retinaculum extending from the olecranon to the medial epicondyle. In the same patient with the elbow flexed, (7C) T1-weighted and (7D) fat-suppressed, fluid-sensitive images demonstrate dislocation of the ulnar nerve (arrows) relative to the medial epicondyle (ME).
Imaging Findings
Radiographs are often normal in cases of cubital tunnel syndrome, but may reveal evidence of prior humerus fracture, cubital valgus, heterotopic ossification, or elbow osteoarthritis with posterior osteophytes and/or loose bodies. CT is typically of limited use but occasionally may be helpful when a severe bone abnormality is present. Ultrasound can be used to trace the course of the ulnar nerve through the cubital tunnel to evaluate its size and echotexture, which can be altered with neuritis, and to assess surrounding mass lesions. Advantages of ultrasound include the ease of examining the contralateral side for comparison and the ability to dynamically assess the nerve and tunnel during elbow flexion and extension.2
MRI provides a comprehensive analysis of the cubital tunnel and ulnar nerve. Like all peripheral nerves, the normal ulnar nerve is approximately isointense to skeletal muscle on T1-weighted images (Figure 4A). However, on fluid-sensitive sequences (especially with fat suppression), increased signal intensity (greater than muscle and greater than the median and radial nerves) is frequently present in asymptomatic individuals.20 Thus a diagnosis of “ulnar neuritis” should be made with caution on the basis of signal intensity alone, without concomitant changes in nerve size or internal architecture. When the only finding is signal hyperintensity, correlation with clinical and/or neurodiagnostic studies is critical. One research publication found that the length of the high signal intensity nerve fibers correlated with the presence of clinical ulnar neuritis, with a minimum length of 10 mm resulting in a 78% specificity.21 It may be easiest to judge the length of the nerve signal changes on sagittal or coronal images (Figure 8). Diffusion-weighted imaging has been suggested as a way to increase accuracy of MRI for ulnar neuritis; however, this technique is not commonly applied to peripheral nerves in clinical practice.22
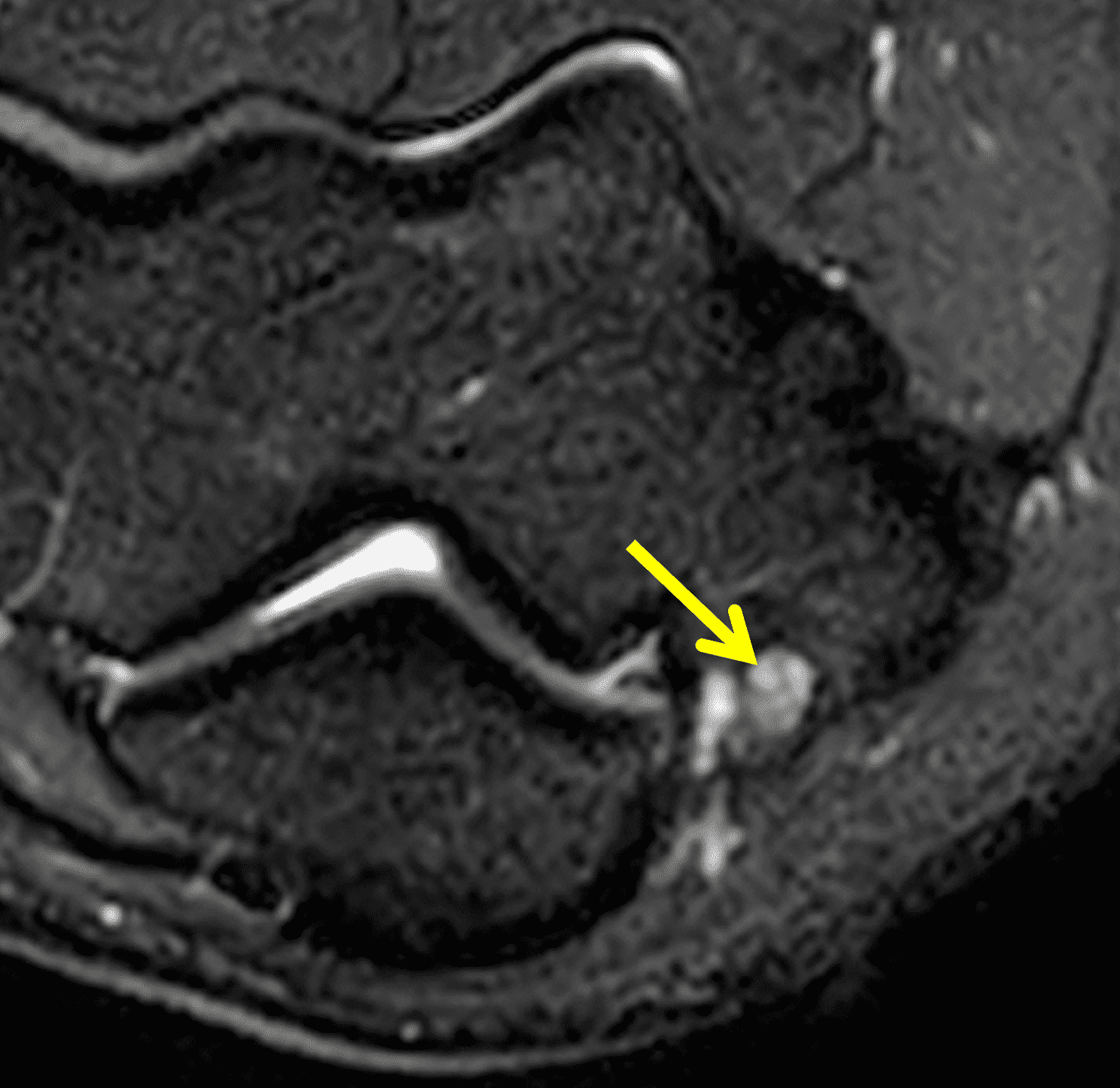
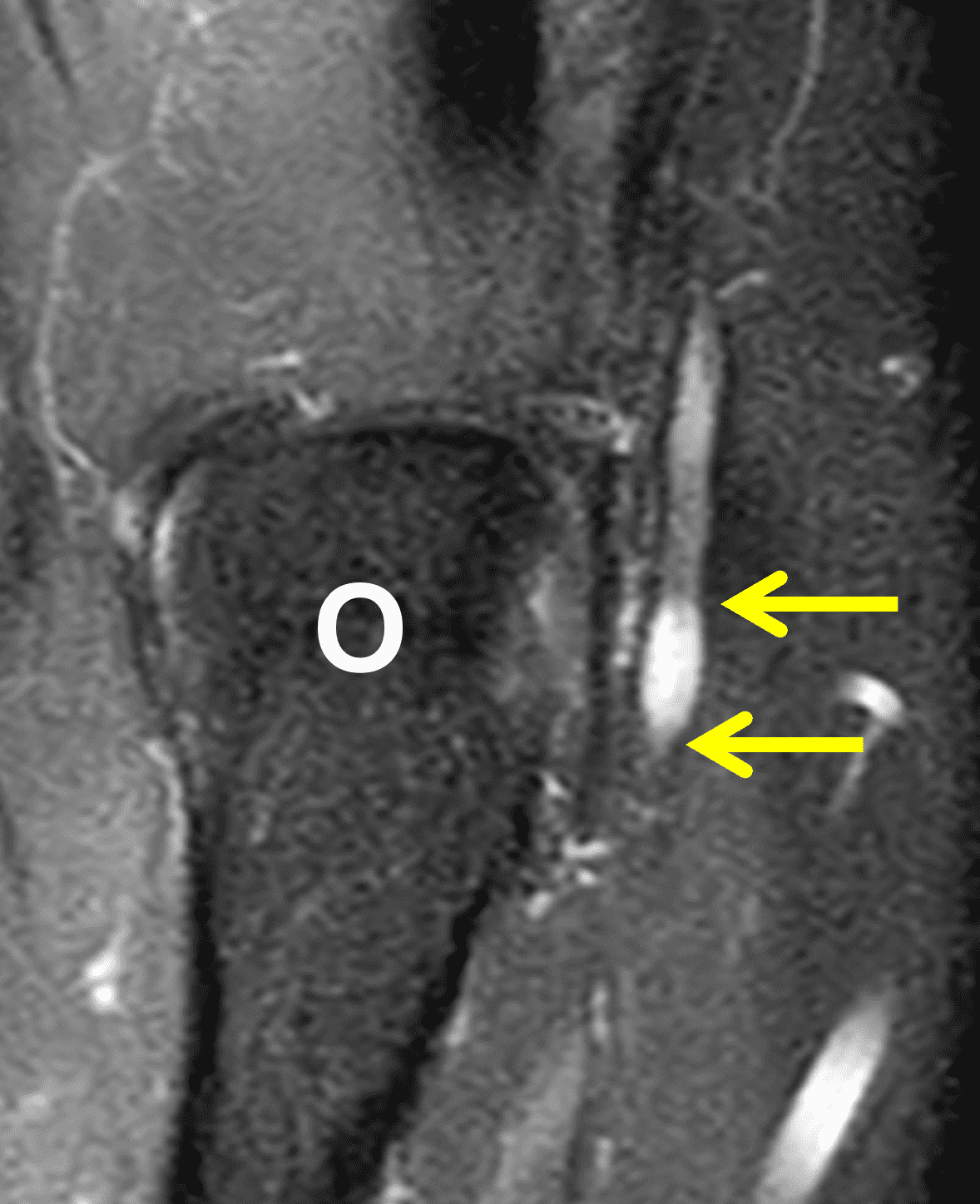

Figure 8: 17-year-old baseball pitcher with clinical ulnar neuritis, abnormal nerve conduction studies, and cubital tunnel syndrome. On the (8A) axial fat-suppressed, fluid-sensitive sequence the ulnar nerve is hyperintense compared to skeletal muscle and not enlarged, non-specific findings. Fat-suppressed (8B) coronal and (8C) sagittal fluid-sensitive images allow a more accurate measurement of the longitudinal extent of the signal changes in the nerve (arrows). O = olecranon, ME = medial humeral epicondyle.
In cross-section, the nerve appears ovoid and is composed of one-to-several fascicles. Most of the data concerning nerve measurements come from ultrasound studies, which report a normal ulnar nerve diameter 6 – 10 mm.1 On MRI, the reported median diameter of the nerve in asymptomatic individuals is 2.4 x 4.0 mm, but can be as large as 4.0 x 7.0 mm.20 With ulnar neuritis the nerve may appear diffusely enlarged, or focally enlarged either within the cubital tunnel or proximal or distal to the tunnel (Figure 9) . A cut-off of 13 mm2 for the nerve cross-sectional area with the cubital tunnel has been suggested, with higher values statistically associated with clinical neuritis.21 For comparison, a published meta-analysis established a 10 mm2 cut-off on ultrasound.23 Combined nerve enlargement and increased signal intensity was the most common abnormality (seen in 63% of cases of cubital tunnel syndrome) in one large study.24 Results of another study suggest that larger nerve diameters are associated with more severe neuritis.12
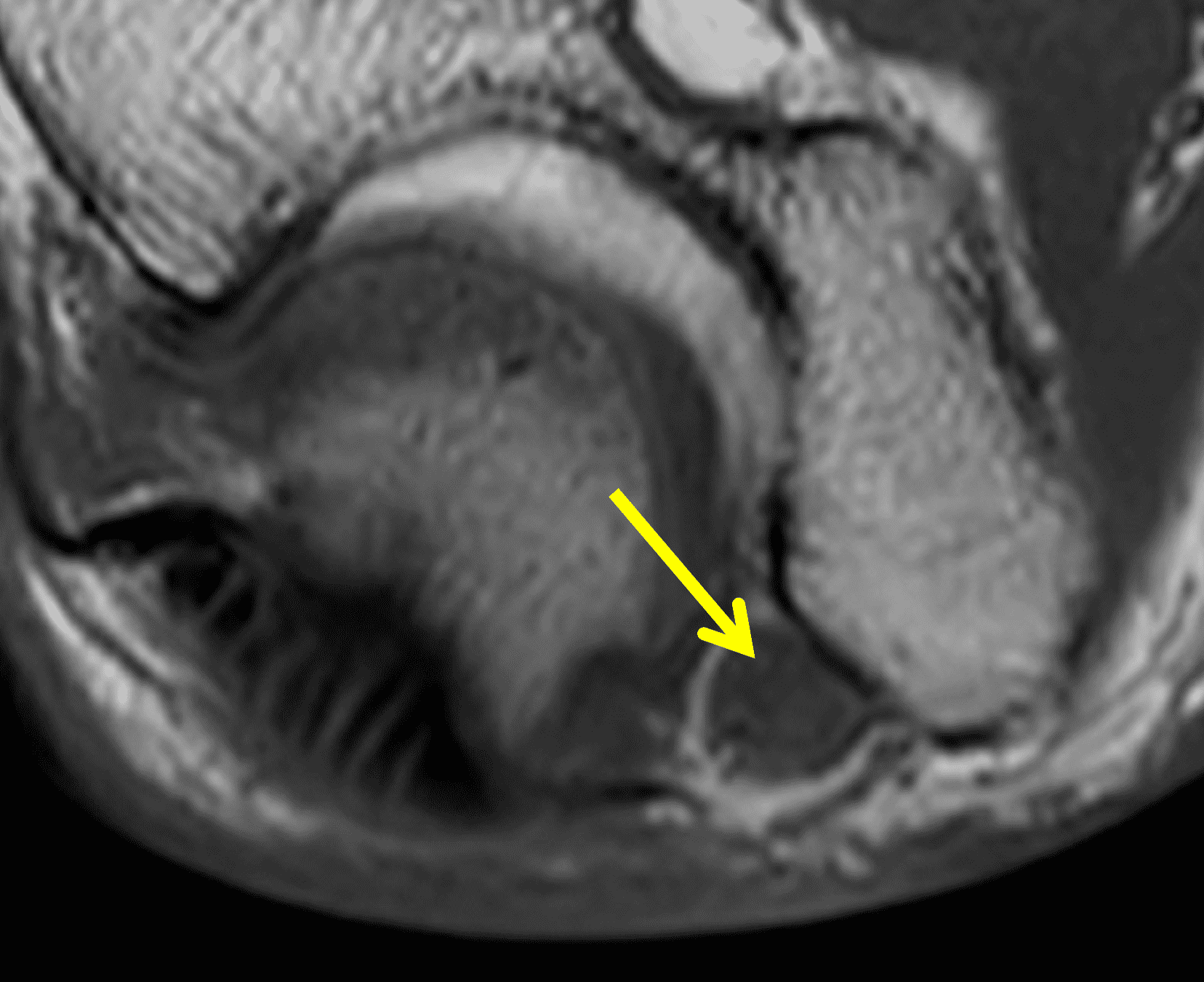
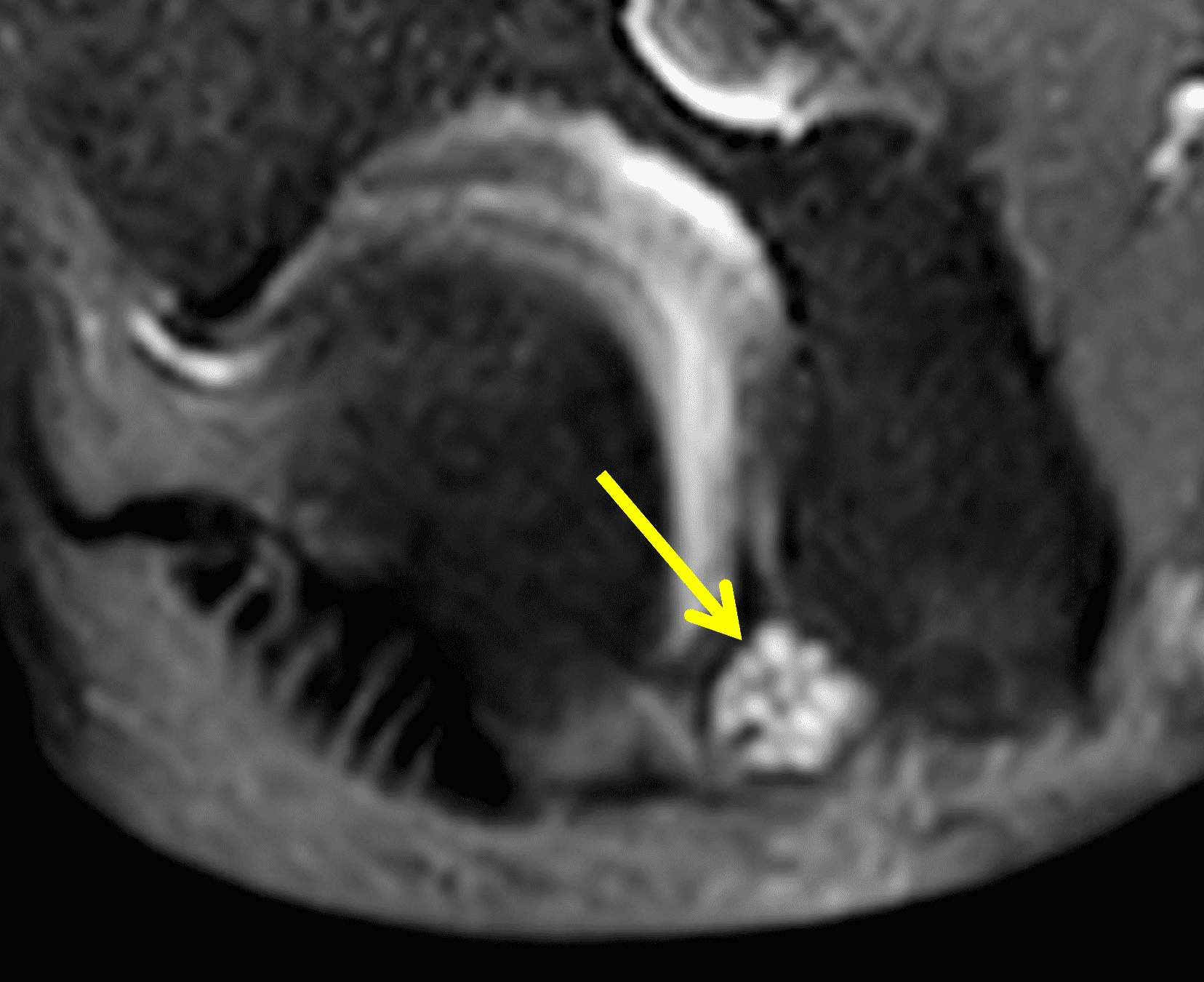
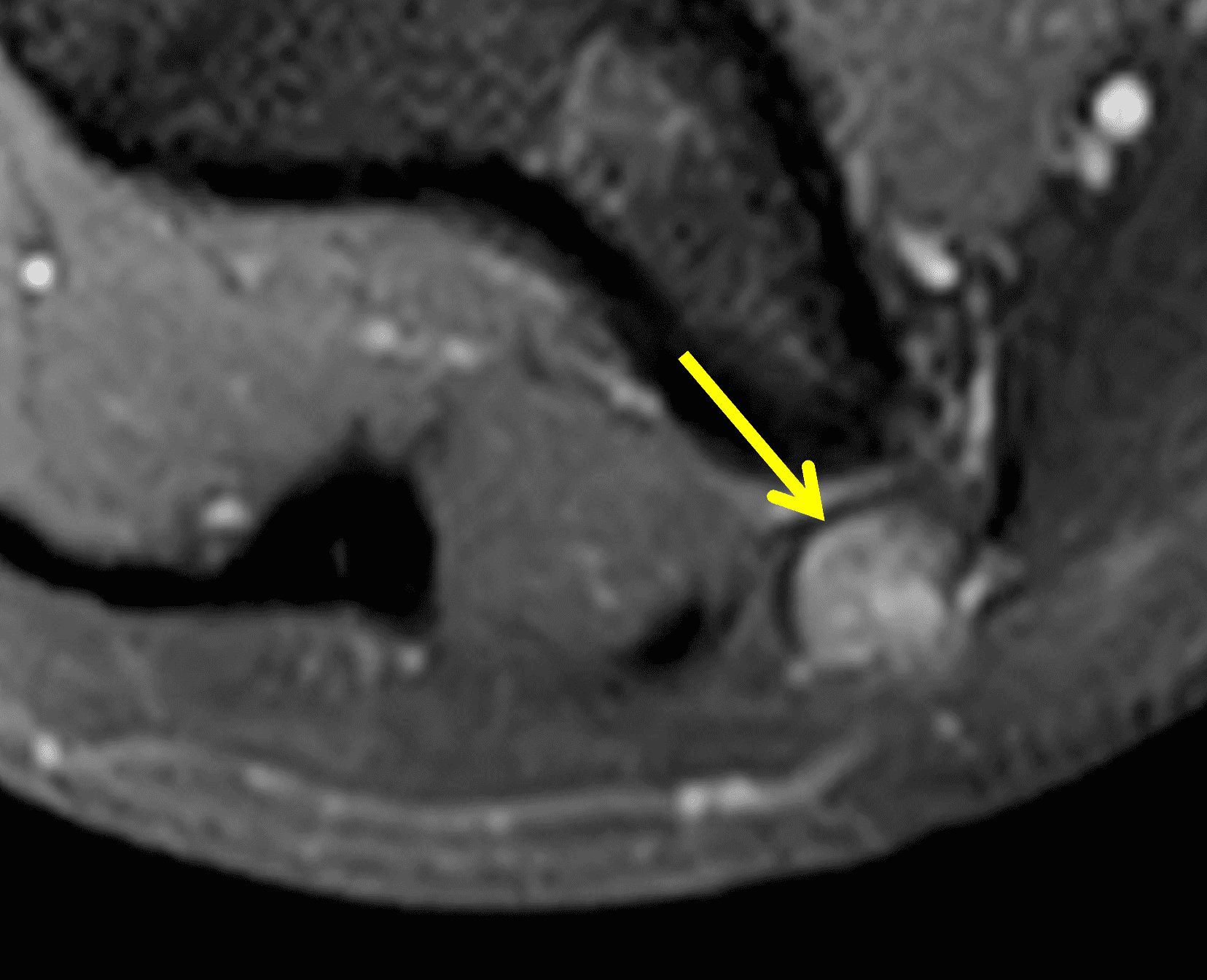
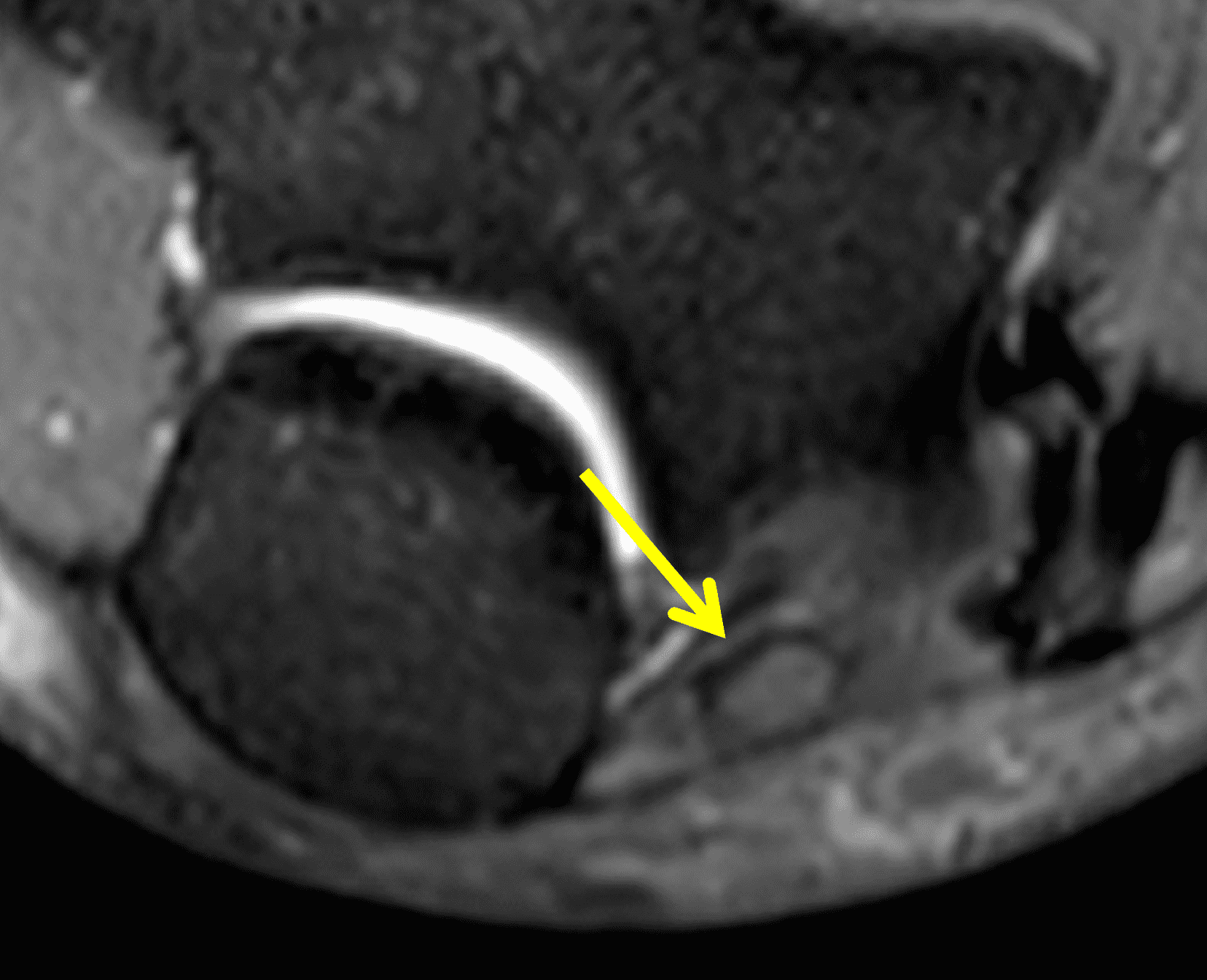
Figure 9: 56-year-old woman with ulnar neuritis due to cubital tunnel syndrome. Axial (9A) T1-weighted and (9B) fat-suppressed, fluid-sensitive images through the cubital tunnel show that the ulnar nerve (arrows) is both enlarged and high in signal intensity, though with preserved fascicular architecture. (9C) Proximal to the cubital tunnel the ulnar nerve (arrow) is mildly hyperintense but enlarged with loss of the normal fascicular appearance. (9D) Distal to the cubital tunnel the ulnar nerve (arrow) has returned to its normal size and is isointense compared with skeletal muscle.
Peripheral nerve sheath tumors (schwannomas and neurofibromas) are typically ovoid with signal intensity approaching fluid on T2-weighted images, sometimes demonstrating target-like morphology with higher signal intensity in the periphery, and intense enhancement following contrast administration.18 Post-traumatic neuromas appear as ill-defined focal enlargements of the nerve with increased signal intensity on fluid-sensitive sequences, disorganized fibers, and contrast enhancement (Figure 10). Unlike most cases of ulnar nerve compression, neuromas and nerve sheath tumors often show muscle findings of denervation in the forearm.


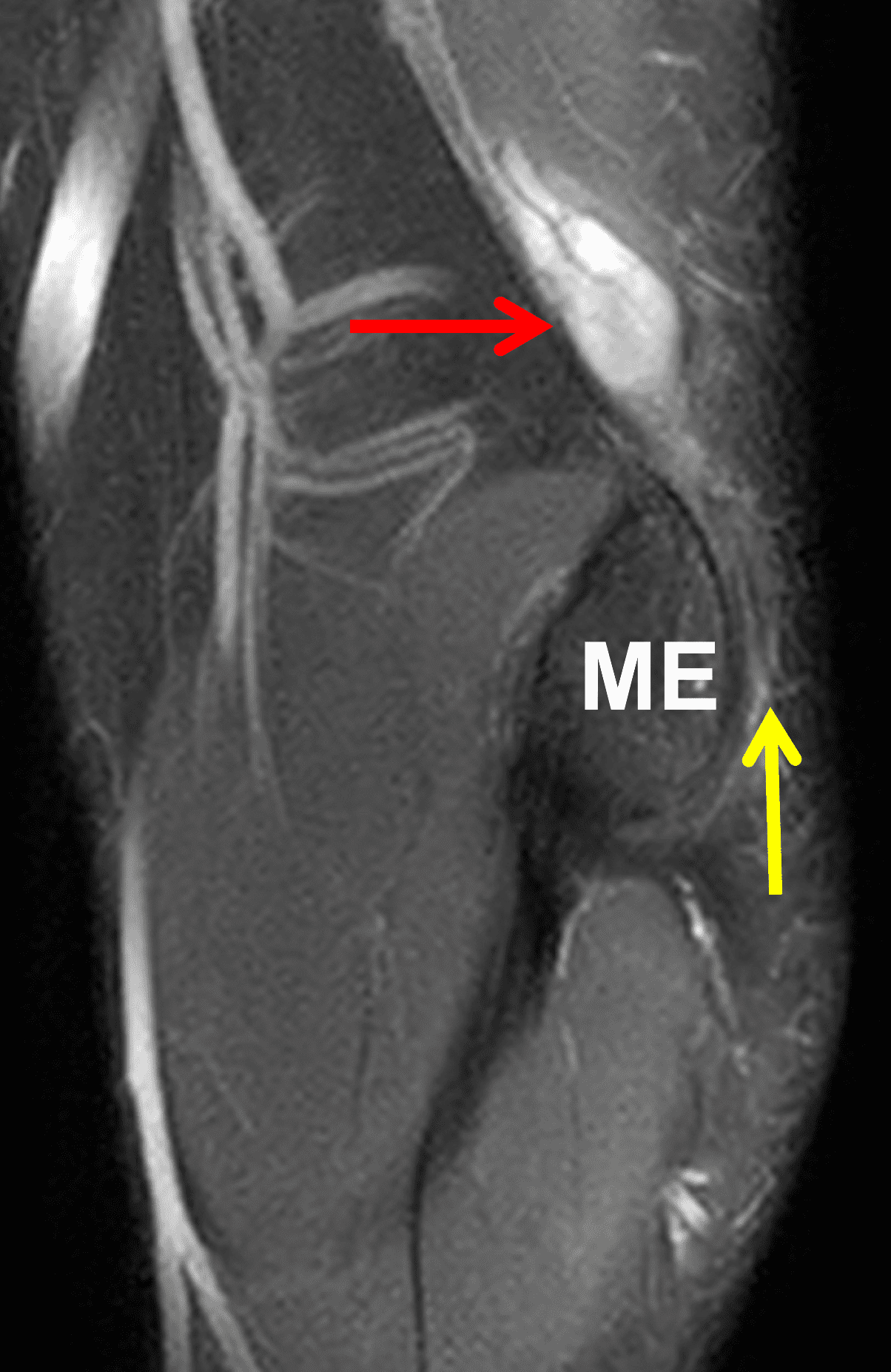
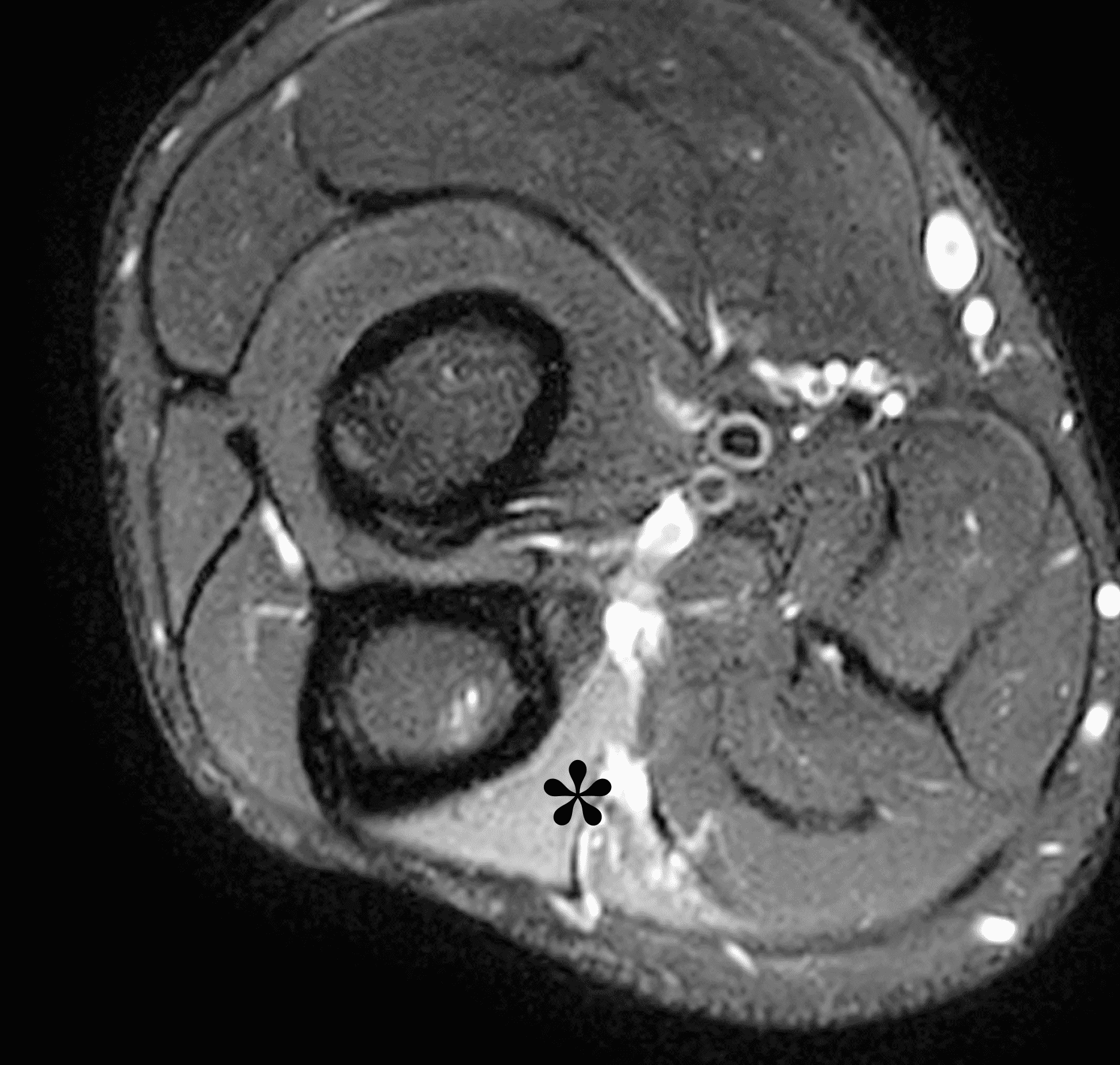
Figure 10: 32-year-old man with a post-traumatic neuroma that developed following an ulnar nerve laceration. Axial (10A) T1-weighted and (10B) fat-suppressed, fluid-sensitive sequences demonstrate enlargement and disorganized architecture of the ulnar nerve (arrows) proximal to the cubital tunnel. (10C) On a sagittal fat-suppressed, fluid-sensitive image, no nerve fibers are visible posterior to the medial epicondyle (ME) in the cubital tunnel (yellow arrow), the site of the nerve transection. The post-traumatic neuroma (red arrow) involves the proximal nerve stump. (10D) An axial fat-suppressed, fluid-sensitive image in the proximal forearm shows subacute denervation with the flexor digitorum profundus muscle (asterisk).
On MRI, the radiologist should assess the appearance of the cubital tunnel retinaculum. A thick retinaculum (Figure 5B) can be associated with increased pressure in the tunnel and predisposed to ulnar neuritis. Conversely, when the retinaculum is absent (Figure 7B) the nerve is more likely to sublux or dislocate. Rarely, an unstable ulnar nerve may lie outside of the cubital tunnel (medial or even anterior to the medial epicondyle) with the elbow extended (Figure 11). More commonly, however, the nerve is normally located with the elbow straight and only moves outside of the tunnel with elbow flexion. While some practitioners advocate adding an additional set of short axis images with the elbow flexed as a useful adjunct maneuver on MRI (Figure 12),6 subluxation or dislocation of the ulnar nerve has been observed in 49% of patients with elbow flexion, whether or not clinical ulnar neuritis is present.25
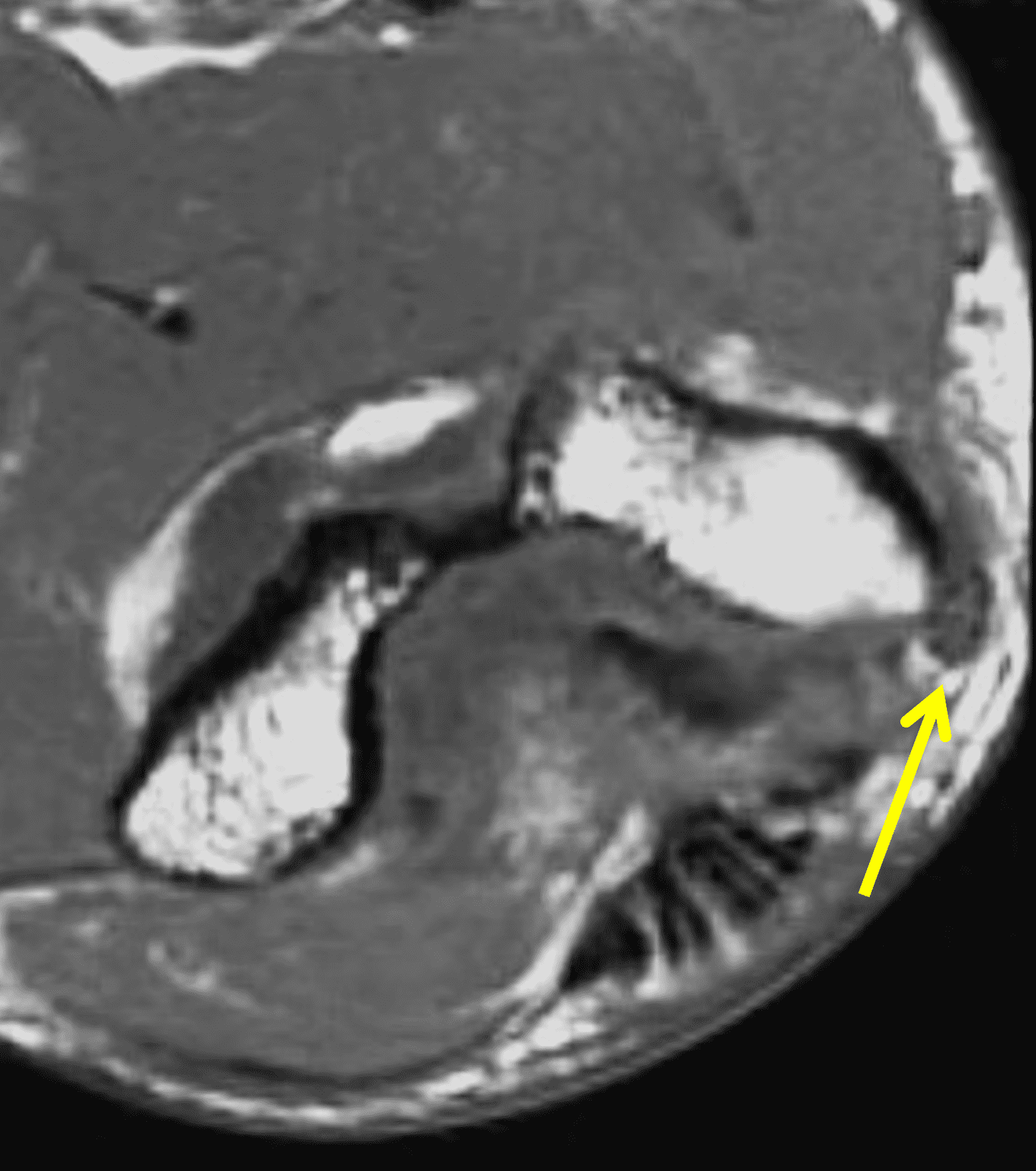

Figure 11: 33-year-old professional football player with ulnar nerve subluxation after an injury. Axial (11A) T1-weighted and (11B) fat-suppressed, fluid-sensitive images show the ulnar nerve (arrows) subluxed medially from the cubital tunnel. A joint effusion is also present. The injury also tore the ulnar collateral ligament (not shown).

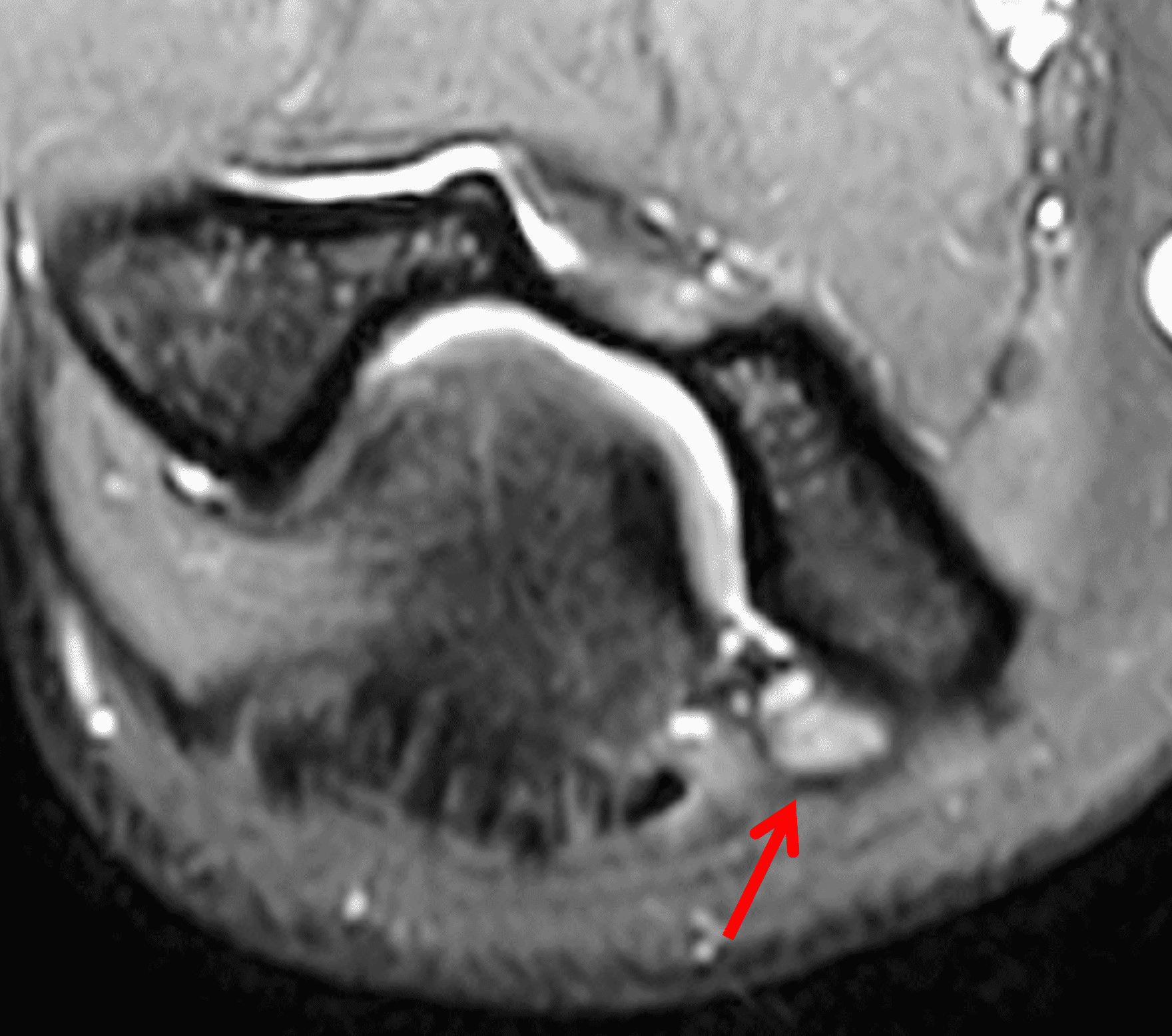
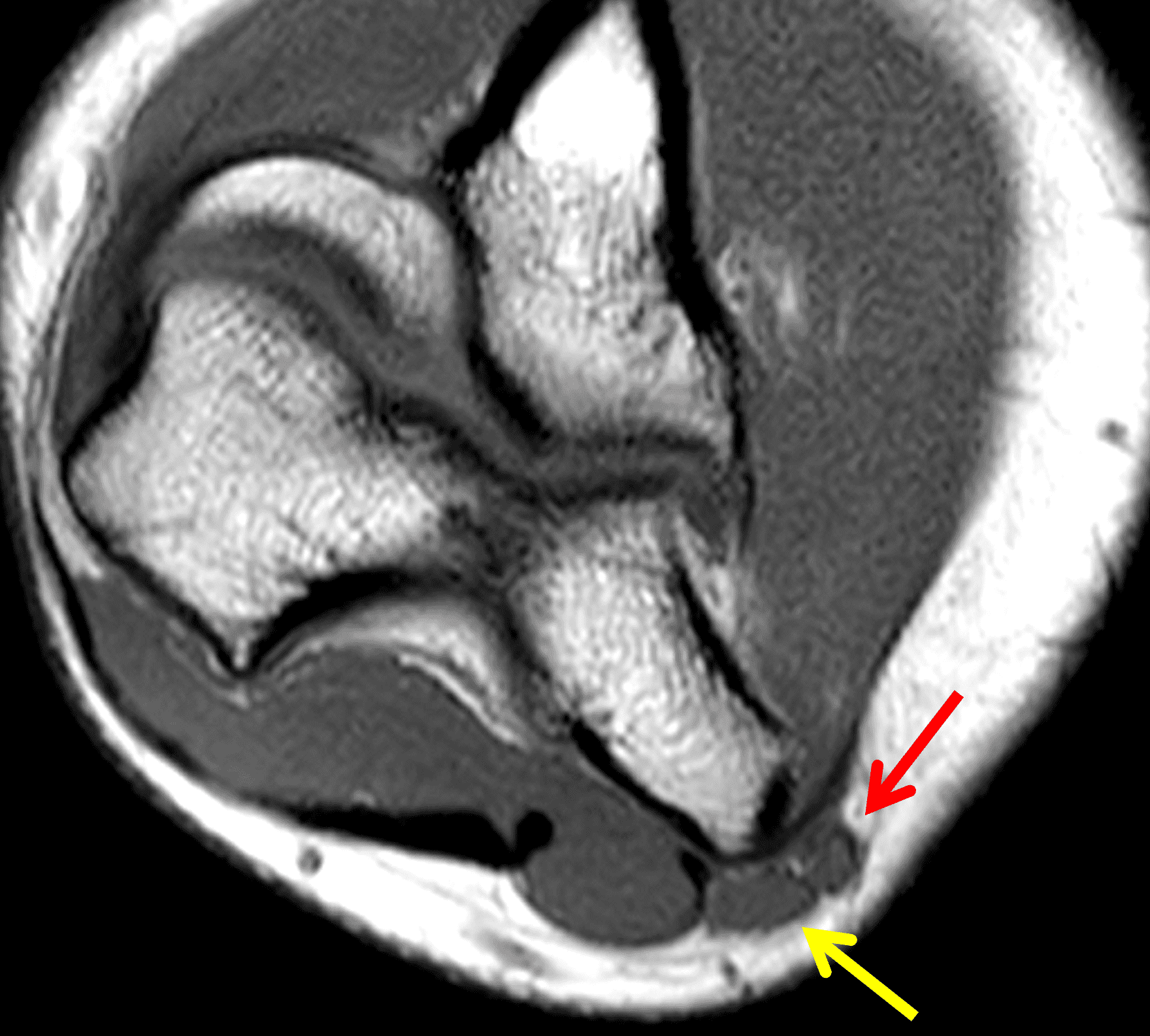
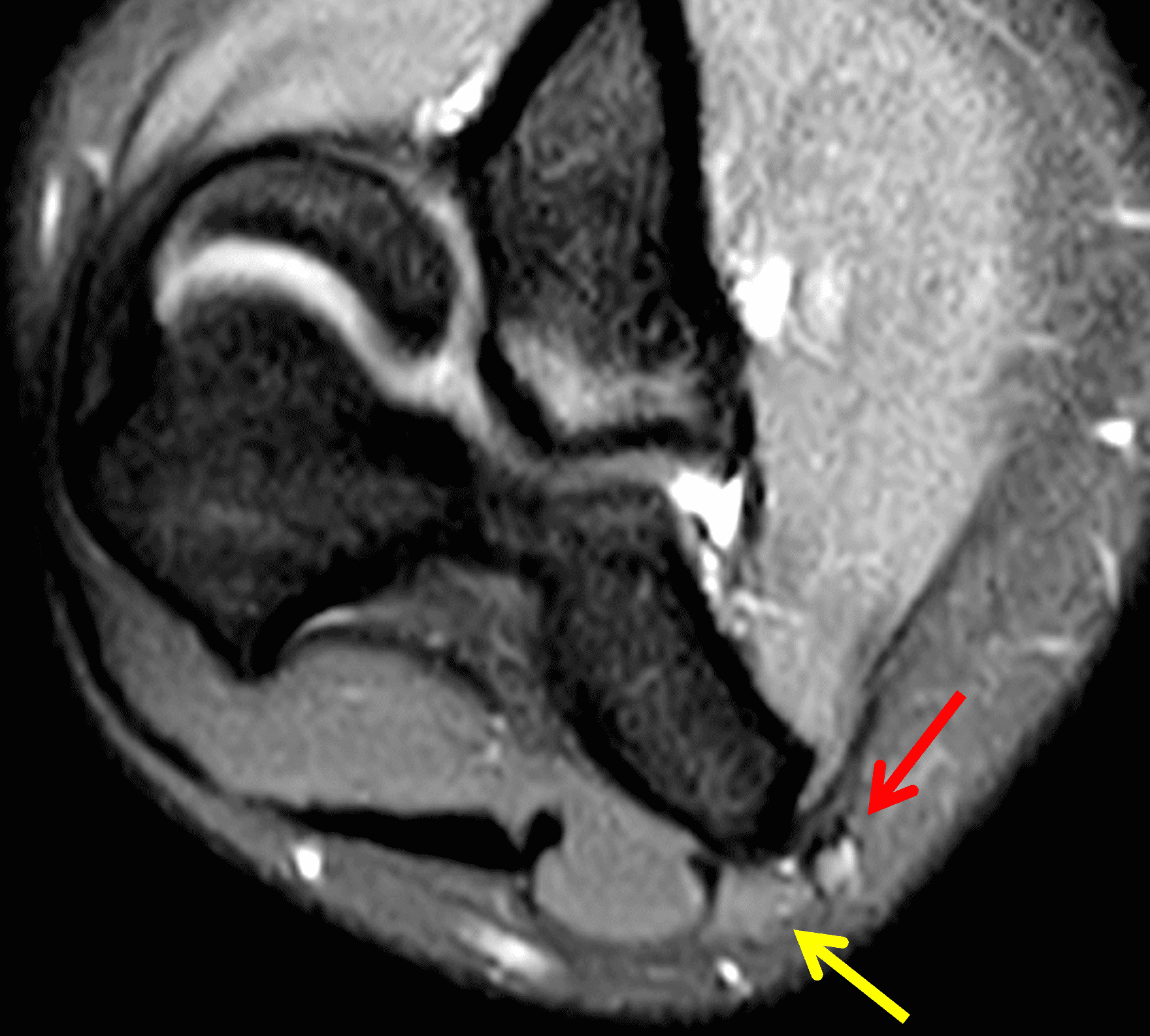
Figure 12: 16-year-old girl who reports a “snapping” sensation with elbow flexion. She has no neurologic symptoms. Axial (12A) T1-weighted and (12B) fat-suppressed, fluid-sensitive images with the elbow extended show the ulnar nerve (arrows) normally located within the cubital tunnel. The retinaculum is either hypoplastic or absent. With elbow flexion, (12C) T1-weighted and (12D) fat-suppressed, fluid-sensitive images show the ulnar nerve (red arrows) dislocated medial to the medial humeral epicondyle. Note that a portion of the medial triceps muscle (yellow arrows) is also subluxed.
In cadaveric and imaging studies, the cubital tunnel retinaculum is replaced by an anomalous muscle – the anconeus epitrochlearis – in 3-34% of the population.26 The prevalence does not appear to be related to age or gender.27 This structure has signal intensity and internal structure identical to other skeletal muscles. It may be present unilaterally or bilaterally. An anconeus epitrochlearis muscle can vary in size from a few millimeters thick to being as large as the normal forearm extensor muscles, and many are simply incidental findings on elbow MRI studies performed for other reasons (Figure 13).20 Some authors believe that an anconeus epitrochlearis (especially a large one) can cause dynamic compression of the ulnar nerve and lead to cubital tunnel syndrome (Figure 14),28 while others argue that the muscle is less stiff than the typical retinaculum and is protective; at least one surgical series found a lower MRI prevalence of an anconeus epitrochlearis in patients undergoing surgery for cubital tunnel syndrome compared to patients undergoing MRI for other reasons.26 The presence of an anconeus epitrochlearis does limit the amount of potential ulnar nerve subluxation with elbow flexion.25

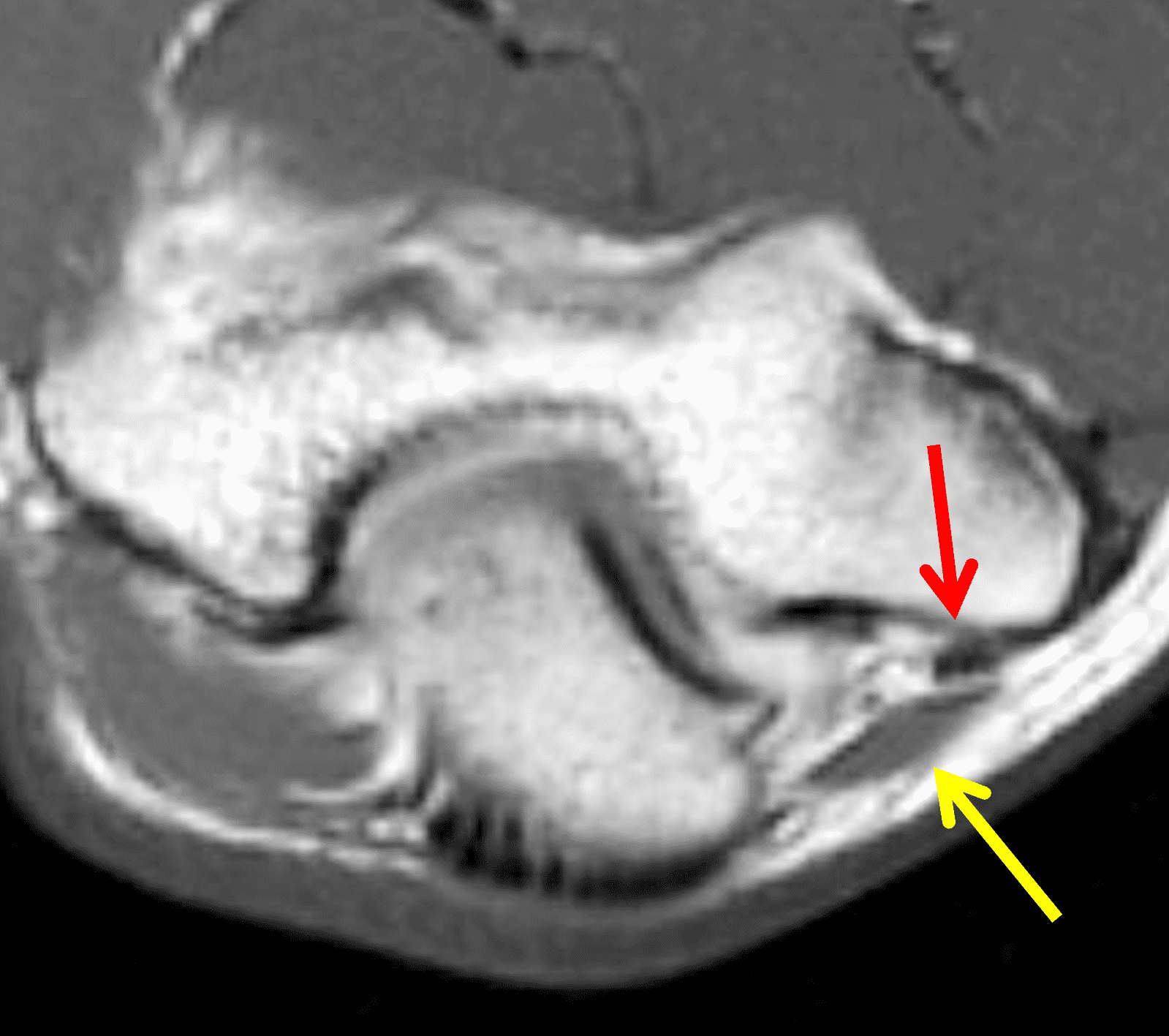
Figure 13: Anconeus epitrochlearis muscle. (13A) Drawing shows the normal cubital tunnel retinaculum replaced by an anomalous muscle. Compare with Figure 3B. (13B) An axial T1-weighted image in a subject with no ulnar nerve symptoms shows a small anconeus epitrochlearis muscle (yellow arrow), an incidental finding in this patient. The ulnar nerve (red arrow) appears normal.

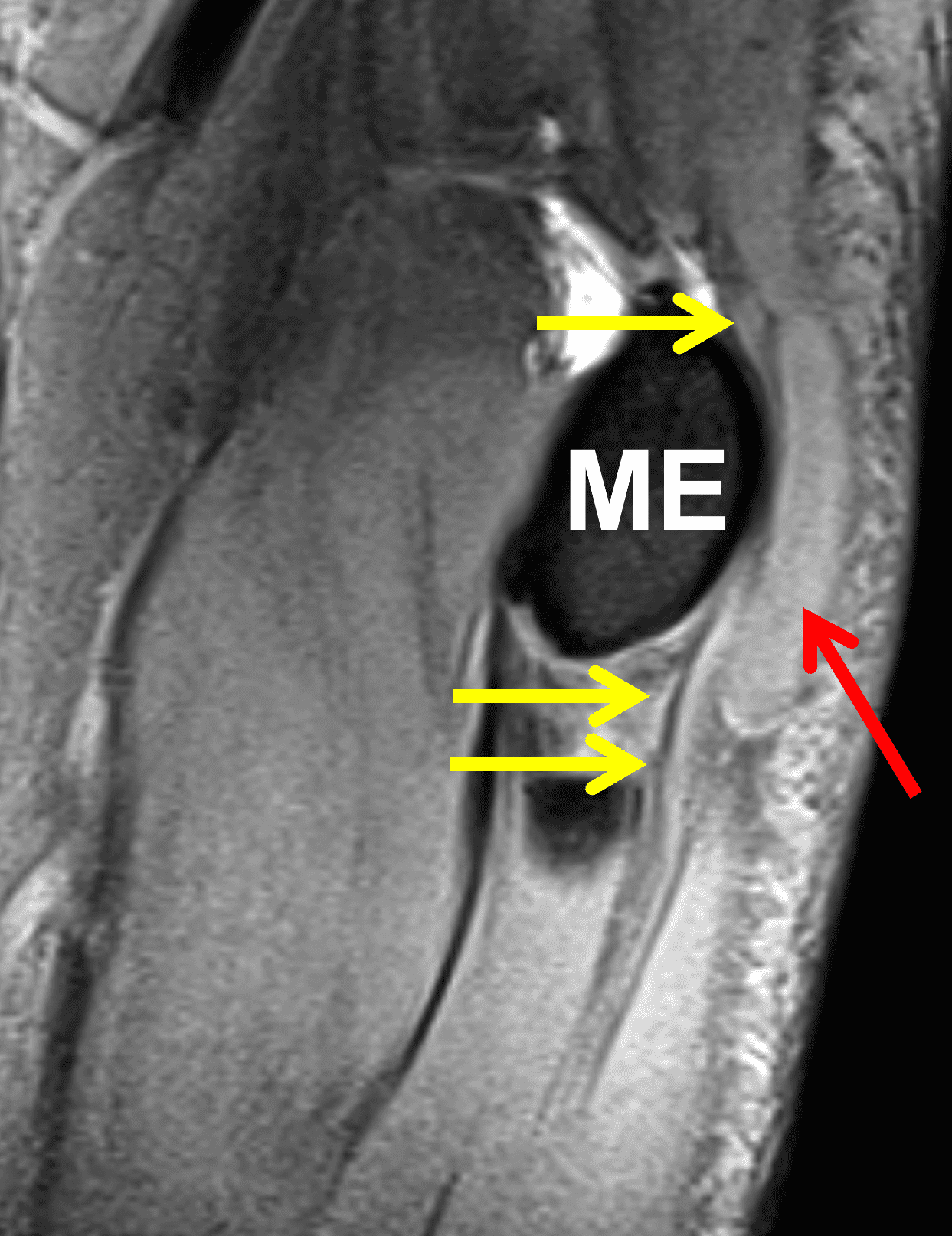
Figure 14: Anconeus epitrochlearis muscle associated with cubital tunnel syndrome. (14A) An axial T1-weighted image from an MR arthrogram shows a large anconeus epitrochlearis muscle (arrow) forming the roof of the cubital tunnel. (14B) A sagittal fat-suppressed, fluid sensitive image shows the large accessory muscle (red arrow) compressing the ulnar nerve against the medial epicondyle (ME). Portions of the non-compressed ulnar nerve are visible proximal and distal to this site (yellow arrows). The patient had clinical symptoms of ulnar neuritis that were relieved following resection of the anomalous muscle.
The radiologist should also assess the other posteromedial structures on MRI studies. Any soft tissue mass in the tunnel should be noted together with its relationship to the ulnar nerve, and the presence of any nerve compression.24 Osteophytes and loose bodies in the posteromedial elbow are important to identify (Figure 15). Similarly, the radiologist should note any excess extension of the elbow synovium or triceps muscle into the tunnel. Lastly, other medial elbow abnormalities (e.g., involving the UCL, flexor-pronator tendons and muscles, articular cartilage, and medial humeral epicondyle/growth plate) should be reported because these additional findings can influence patient management.
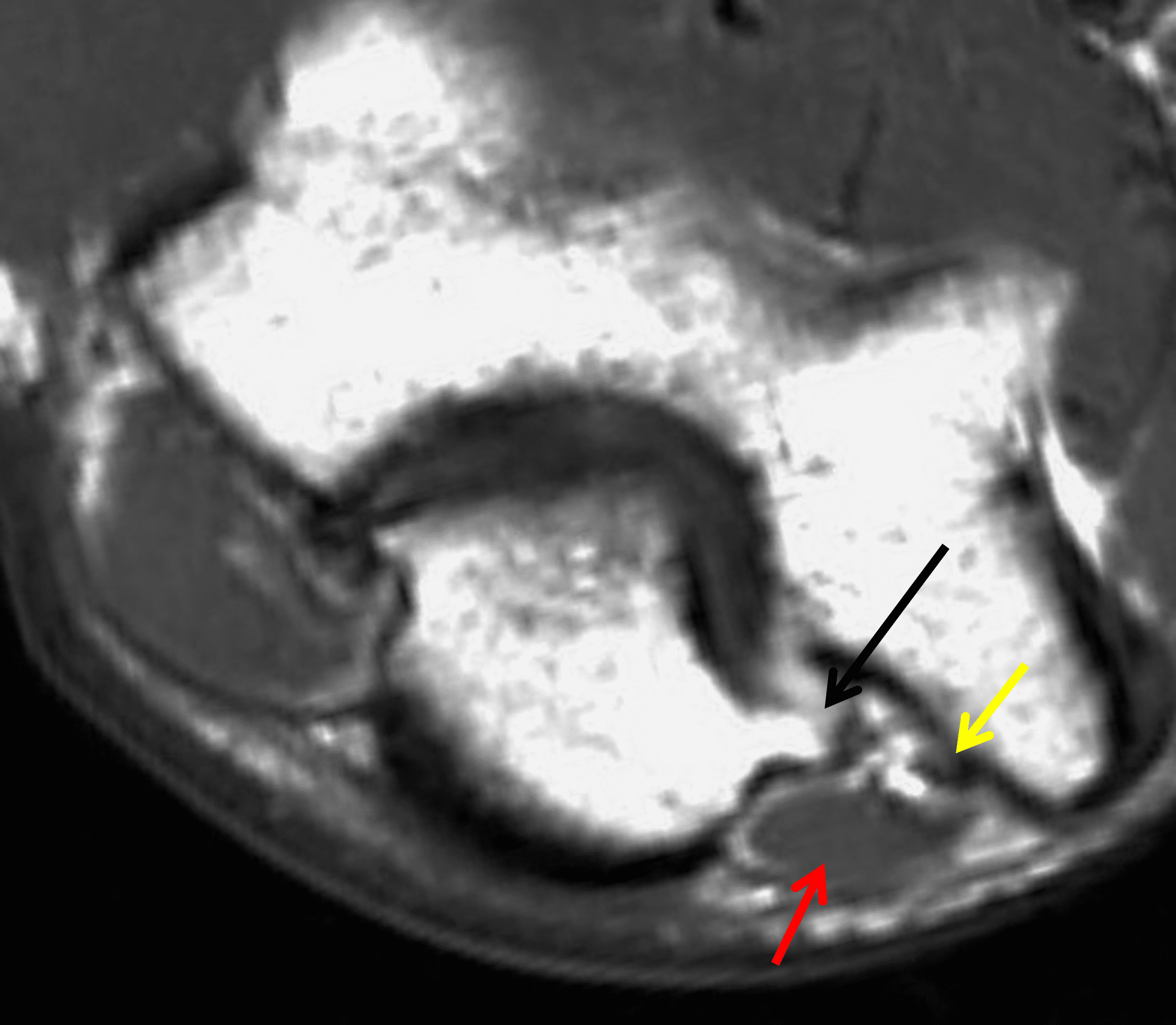
Figure 15: Cubital tunnel syndrome associated with osteoarthritis. An axial T1-weighted image shows an olecranon osteophyte (black arrow) extending into the lateral aspect of the cubital tunnel. Also note an anconeus epitrochlearis muscle (red arrow) overlying the ulnar nerve (yellow arrow). Symptoms of ulnar neuritis were relieved following cubital tunnel release that included excision of both the osteophyte and anomalous muscle.
Unlike other peripheral neuropathies, where denervation changes in the muscle are often the earliest clue to a nerve lesion, in cubital tunnel syndrome muscle changes develop late, and they occur primarily in the hand, which is not included in MRI studies of the elbow. Nevertheless, if a hand MRI shows evidence of unexplained subacute (edematous) or chronic (fatty atrophy) denervation in muscles supplied by the ulnar nerve (Figure 16), elbow imaging to assess the cubital tunnel should be considered.

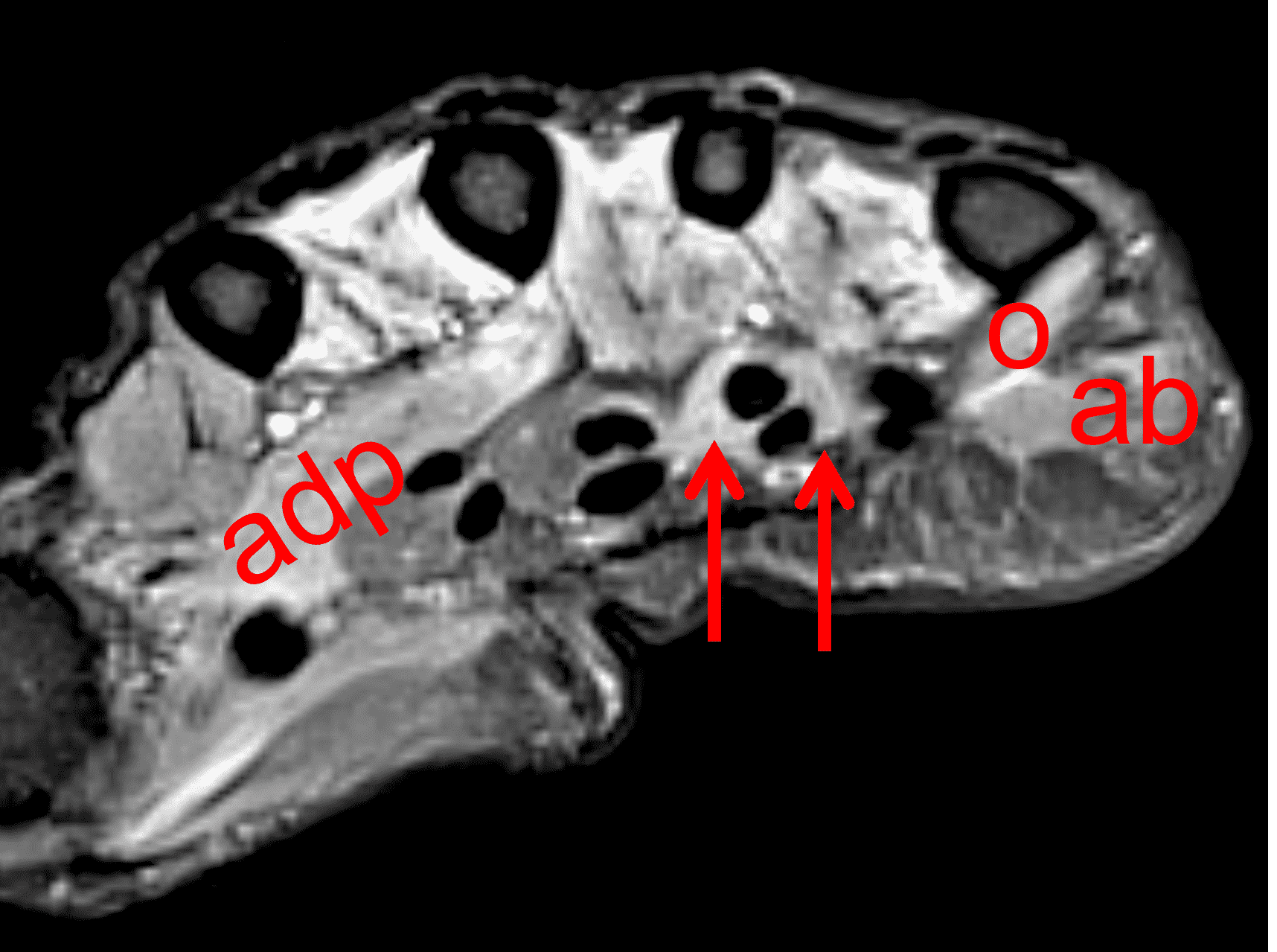
Figure 16: Ulnar neuritis with muscle denervation. In addition to sensory symptoms, this woman also presented with decreased grip strength. (16A) Axial STIR image through the proximal palm shows high signal intensity within the dorsal (d) and palmar (p) interosseous muscles, representing subacute denervation in the ulnar nerve distribution. (16B) A STIR image slightly more distally also shows subacute denervation involving the adductor pollicis (adp), opponens digiti minimi (o), abductor digiti minimi (ab), and third and fourth lumbrical (arrows) muscles. Despite having no symptoms at the elbow, nerve conduction studies and EMG confirmed ulnar nerve dysfunction at the cubital tunnel.
Treatment
Nonoperative treatments is the first line of therapy for patients with mild sensory symptoms and normal or only slightly slowed nerve conduction (motor velocity above 40 m/s). Recommendations include activity modification to avoid prolonged elbow flexion, nighttime splinting or bracing, elbow padding, and anti-inflammatory medications. 50–60% of patients with mild symptoms will respond to conservative therapy.10
Operative treatment is typically reserved for more severe or long-lasting cases where nerve function continues to decline, or in patients who fail nonoperative treatment. Surgical techniques include simple decompression and nerve transposition. Evidence suggests that decompression is often just as effective as more invasive methods and may have fewer complications.29 While endoscopic decompression might offer slightly less pain and scarring compared to an open procedure, overall outcomes are similar.10 Patients with an anconeus epitrochlearis muscle tend to improve faster after cubital tunnel release compared to those without an accessory muscle.26
Anterior subcutaneous nerve transposition is usually performed in elbows with ulnar nerve subluxation or dislocation associated with painful snapping.29 Additionally, many surgeons combine ulnar nerve transposition with UCL reconstruction, especially if there are preoperative nerve symptoms (Figure 17).30 Other techniques like submuscular transposition or medial epicondylectomy are used less commonly and lack strong evidence of increased effectiveness.10
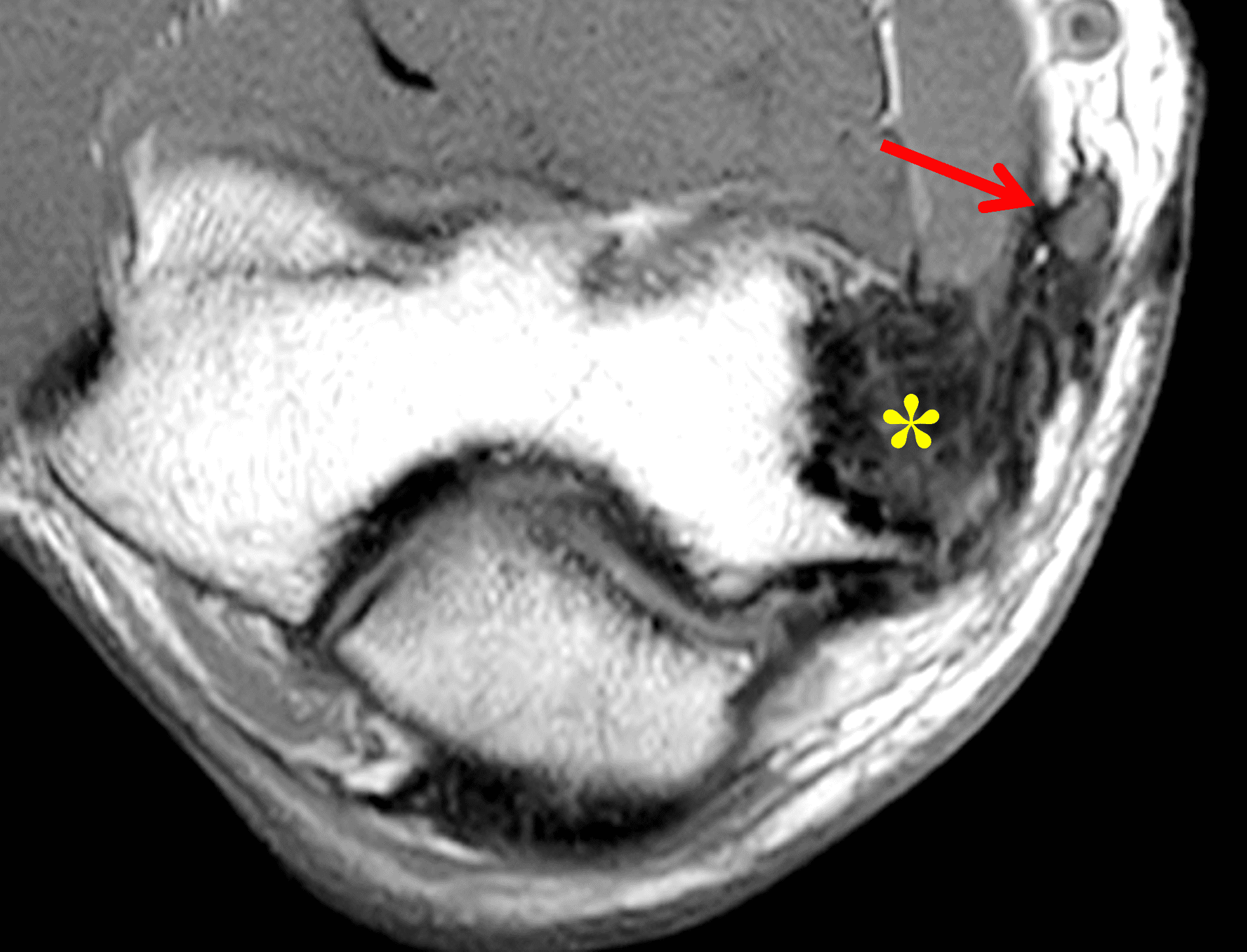
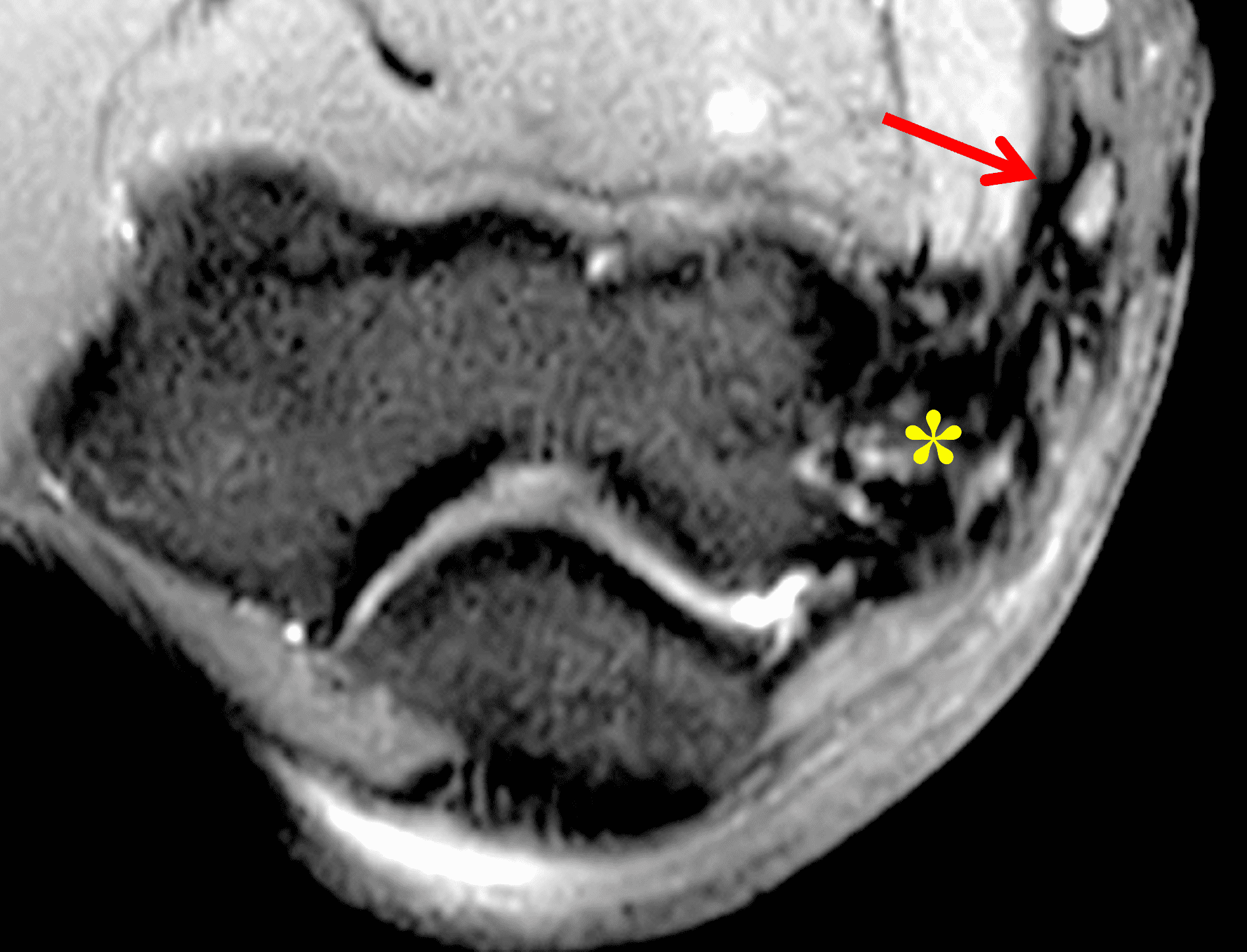
Figure 17: Anterior subcutaneous ulnar nerve transposition in a 30-year-old baseball pitcher, performed as part of an ulnar collateral ligament reconstruction procedure. Axial (17A) T1-weighted and (17B) fat-suppressed, fluid-sensitive images show the ulnar nerve (arrows) transferred from the cubital tunnel to the anteromedial subcutaneous fat, separate from the artifact and scar tissue related to the ligament reconstruction (asterisks).
Conclusions
Ulnar nerve dysfunction commonly has its origin in the cubital tunnel at the elbow, where the nerve is susceptible to stretching, compression, and instability. Elbow imaging plays a complementary role to clinical evaluation and neurodiagnostic testing. MRI is useful in assessing both the nerve itself and anatomic abnormalities in the surrounding tissues.
References
- Hussein M, Hanumanthu MM, Shirodkar K, Papineni VRK, Rahij H, Velicheti S, et al. Cubital tunnel syndrome: anatomy, pathology, and imaging. Skeletal Radiol. 2025;54(1):1–15. doi:10.1007/s00256-024-04705-4 ↩
- Kalia V, Jacobson JA. Imaging of Peripheral Nerves of the Upper Extremity. Radiol Clin North Am. 2019;57(5):1063–1071. doi:10.1016/j.rcl.2019.04.001 ↩
- Shen L, Masih S, Patel DB, Matcuk GR, Jr. MR anatomy and pathology of the ulnar nerve involving the cubital tunnel and Guyon’s canal. Clin Imaging. 2016;40(2):263–274. doi:10.1016/j.clinimag.2015.11.008 ↩
- Macchi V, Tiengo C, Porzionato A, Stecco C, Sarasin G, Tubbs S, et al. The cubital tunnel: a radiologic and histotopographic study. J Anat. 2014;225(2):262–269. doi:10.1111/joa.12206 ↩
- O’Driscoll SW, Horii E, Carmichael SW, Morrey BF. The cubital tunnel and ulnar neuropathy. J Bone Joint Surg Br. 1991;73(4):613–617. doi:10.1302/0301-620X.73B4.2071645 ↩
- Bencardino JT, Rosenberg ZS. Entrapment neuropathies of the shoulder and elbow in the athlete. Clin Sports Med. 2006;25(3):465–487, vi–vii. doi:10.1016/j.csm.2006.03.005 ↩
- Ozturk E, Sonmez G, Colak A, Sildiroglu HO, Mutlu H, Senol MG, et al. Sonographic appearances of the normal ulnar nerve in the cubital tunnel. J Clin Ultrasound. 2008;36(6):325–329. doi:10.1002/jcu.20486 ↩
- Chaudhary RK, Karkala N, Nepal P, Gupta E, Kaur N, Batchala P, et al. Multimodality imaging review of ulnar nerve pathologies. Neuroradiol J. 2024;37(2):137–151. doi:10.1177/19714009231166087 ↩
- An TW, Evanoff BA, Boyer MI, Osei DA. The Prevalence of Cubital Tunnel Syndrome: A Cross-Sectional Study in a U.S. Metropolitan Cohort. J Bone Joint Surg Am. 2017;99(5):408–416. doi:10.2106/JBJS.15.01162 ↩
- Nakashian MN, Ireland D, Kane PM. Cubital Tunnel Syndrome: Current Concepts. Curr Rev Musculoskelet Med. 2020;13(4):520–524. doi:10.1007/s12178-020-09650-y ↩
- Wojewnik B, Bindra R. Cubital tunnel syndrome – Review of current literature on causes, diagnosis and treatment. J Hand Microsurg. 2009;1(2):76–81. doi:10.1007/s12593-009-0020-9 ↩
- Bäumer P, Dombert T, Staub F, Kaestel T, Bartsch AJ, Heiland S, et al. Ulnar neuropathy at the elbow: MR neurography–nerve T2 signal increase and caliber. Radiology. 2011;260(1):199–206. doi:10.1148/radiol.11102357 ↩
- James J, Sutton LG, Werner FW, Basu N, Allison MA, Palmer AK. Morphology of the cubital tunnel: an anatomical and biomechanical study with implications for treatment of ulnar nerve compression. J Hand Surg Am. 2011;36(12):1988–1995. doi:10.1016/j.jhsa.2011.09.014 ↩
- Lee SK, Hwang SY, Kim SG, Choy WS. Analysis of the Anatomical Factors Associated with Cubital Tunnel Syndrome. Orthop Traumatol Surg Res. 2020;106(4):743–749. doi:10.1016/j.otsr.2020.01.016 ↩
- Cummins CA, Schneider DS. Peripheral nerve injuries in baseball players. Neurol Clin. 2008;26(1):195–215; x. doi:10.1016/j.ncl.2007.11.014 ↩
- Izzi J, Dennison D, Noerdlinger M, Dasilva M, Akelman E. Nerve injuries of the elbow, wrist, and hand in athletes. Clin Sports Med. 2001;20(1):203–217. doi:10.1016/s0278-5919(05)70256-8 ↩
- Kim DH, Han K, Tiel RL, Murovic JA, Kline DG. Surgical outcomes of 654 ulnar nerve lesions. J Neurosurg. 2003;98(5):993–1004. doi:10.3171/jns.2003.98.5.0993 ↩
- Woertler K. Tumors and tumor-like lesions of peripheral nerves. Semin Musculoskelet Radiol. 2010;14(5):547–558. doi:10.1055/s-0030-1268073 ↩
- Spinner RJ, Goldner RD. Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve. Anatomical and dynamic factors. J Bone Joint Surg Am. 1998;80(2):239–247. doi:10.2106/00004623-199802000-00011 ↩
- Husarik DB, Saupe N, Pfirrmann CW, Jost B, Hodler J, Zanetti M. Elbow nerves: MR findings in 60 asymptomatic subjects–normal anatomy, variants, and pitfalls. Radiology. 2009;252(1):148–156. doi:10.1148/radiol.2521081614 ↩
- Kim S, Chung BM, Kim WT, Lee GY, Hur J, Kim JH, et al. Diagnosing ulnar neuropathy at the elbow on MRI: importance of the longitudinal extent of the hyperintense ulnar nerve. Skeletal Radiol. 2022;51(7):1473–1481. doi:10.1007/s00256-022-03990-1 ↩
- Altun Y, Aygun MS, Cevik MU, Acar A, Varol S, Arikanoglu A, et al. Relation between electrophysiological findings and diffusion weighted magnetic resonance imaging in ulnar neuropathy at the elbow. J Neuroradiol. 2013;40(4):260–266. doi:10.1016/j.neurad.2012.08.004 ↩
- Chang KV, Wu WT, Han DS, Ozcakar L. Ulnar Nerve Cross-Sectional Area for the Diagnosis of Cubital Tunnel Syndrome: A Meta-Analysis of Ultrasonographic Measurements. Arch Phys Med Rehabil. 2018;99(4):743–757. doi:10.1016/j.apmr.2017.08.467 ↩
- Vucic S, Cordato DJ, Yiannikas C, Schwartz RS, Shnier RC. Utility of magnetic resonance imaging in diagnosing ulnar neuropathy at the elbow. Clin Neurophysiol. 2006;117(3):590–595. doi:10.1016/j.clinph.2005.09.022 ↩
- Kawahara Y, Yamaguchi T, Honda Y, Tomita Y, Uetani M. The Ulnar Nerve at Elbow Extension and Flexion: Assessment of Position and Signal Intensity on MR Images. Radiology. 2016;280(2):483–492. doi:10.1148/radiol.2016150173 ↩
- Maslow JI, Johnson DJ, Block JJ, Lee DH, Desai MJ. Prevalence and Clinical Manifestations of the Anconeus Epitrochlearis and Cubital Tunnel Syndrome. Hand (N Y). 2020;15(1):69–74. doi:10.1177/1558944718789412 ↩
- Nascimento SRR, Ruiz CR. A study on the prevalence of the anconeus epitrochlearis muscle by magnetic resonance imaging. Rev Bras Ortop. 2018;53(3):373–377. doi:10.1016/j.rboe.2018.03.015 ↩
- Morgenstein A, Lourie G, Miller B. Anconeus epitrochlearis muscle causing dynamic cubital tunnel syndrome: a case series. J Hand Surg Eur Vol. 2016;41(2):227–229. doi:10.1177/1753193414559491 ↩
- Assmus H, Antoniadis G, Bischoff C, Hoffmann R, Martini AK, Preissler P, et al. Cubital tunnel syndrome – a review and management guidelines. Cent Eur Neurosurg. 2011;72(2):90–98. doi:10.1055/s-0031-1271800 ↩
- Conti MS, Camp CL, Elattrache NS, Altchek DW, Dines JS. Treatment of the ulnar nerve for overhead throwing athletes undergoing ulnar collateral ligament reconstruction. World J Orthop. 2016;7(10):650–656. doi:10.5312/wjo.v7.i10.650 ↩
