Clinical History: A 53-year-old male presents with chronic shoulder pain and clinically apparent deltoid atrophy. Coronal T1-weighted (1A) and fat-suppressed proton density-weighted (1B), coronal T1-weighted (1C), and sagittal T2- weighted (1D), and axial fat-suppressed proton density-weighted (1E) images are provided. What are the imaging findings? What is your diagnosis?

1a

1b

1c

1d

1e
Figure 1
Findings

2a

2b

2c

2d

2e
Figure 2:
The coronal T1-weighted (2A) image shows marked fatty atrophy of the deltoid muscle (red arrowheads), indicating chronic denervation. The fat-suppressed proton density-weighted (2B) coronal image shows a multiloculated cyst extending inferiorly from the inferior labrum (asterisk).
Note the chronic post-traumatic deformity of the inferior glenoid associated with thickening and scarring of the axillary pouch component of the inferior glenohumeral ligament (red arrow). The patient had concomitant rotator cuff disease with a deep bursal surface partial tear (white arrow) and a tear of the superior labrum (white arrowhead). A more posterior coronal T1-weighted (2C) image demonstrates marked posterior deltoid (red arrowheads) and teres minor (short black arrows) fatty atrophy indicating chronic denervation change of the axillary nerve (more than one atrophied muscle sharing the same innervation). A sagittal T2- weighted (2D) image shows the cyst (asterisk) inferior to the inferior glenoid and labrocapsular structures with a serpiginous connecting stalk (short red arrow). Note the marked fatty atrophy of the deltoid muscle (red arrowheads). The axial fat-suppressed proton density-weighted (2E) image reveals the cyst projecting into the quadrilateral space (asterisk), which is bounded superiorly by the teres minor, inferiorly by the teres major, medially by the long head of the triceps, and laterally by the humeral shaft. It contains the axillary nerve and posterior humeral circumflex artery.
Diagnosis
Labral cyst compressing the axillary nerve within the quadrilateral space with resultant chronic axillary neuropathy.
Pathogenesis
Cysts around and within the shoulder most commonly arise from a tear of the labrum or shoulder capsule.1,2,3,4,5,6,7,8,9,10,11 Cysts found adjacent to the glenoid labrum have been shown to arise from a tear of the labrum in most cases.1,4,8 The tear is most commonly the result of acute trauma or repetitive motion (chronic microtrauma) injury.12 Tendon or intramuscular cysts may develop after a delaminating rotator cuff tear, typically articular surface or full thickness associated with a tear of the adjacent adherent capsule.13,14
The histologic characterization of labral cysts is debated as cystic lesions near the glenohumeral joint have been described by various authors as “ganglion cysts”15,16. 1981;(63):492–4.],17 “ganglia”18,19,20, “synovial cysts”21 and pseudocysts.4,22 A synovial cyst is lined by synovial cells and forms from evagination of the joint capsule or para-articular bursa.10 A ganglion cyst may arise from a joint capsule, bursa, ligament, tendon, or subchondral bone. A pseudocyst may result from the extrusion of joint fluid through a labrocapsular tear into adjacent soft tissues, and the pseudocyst pathogenesis has been likened to that of a meniscal cyst.4,23,24 To add to the confusion, the definition of a synovial cyst is controversial with some authors using the term synonymously with “ganglion,” whereas others define synovial cysts as herniations of the synovial membrane through the capsule of a joint filled by synovial fluid, which may or may not keep a communication with the joint.25,26,27,28 Synovial cysts are thought to serve as drainage reservoirs for excessive joint effusion in the setting of any arthropathy, escaping from its regular location through a one-way-valve mechanism into the area of least resistance.29. 2016;7(2):179–86. Available from: https://doi.org/10.1007/s13244-016-0463-z] Ganglion cysts lack a synovial cell lining and are constituted by a dense collagenous capsule surrounding a mucopolysaccharide-rich gelatinous fluid25,26,27,28,29,30, like that of a synovial cyst but at a higher concentration.25,29 A developmental continuum between a true synovial cyst and ganglion cyst of a synovial herniation followed by myxoid degeneration has even been theorized, but is presently not confirmed.25,29,30 Finally, a pseudocyst is lined by fibrous tissue, not synovial membrane, and is filled with mucoid content.22
A cyst may form from a labral tear and remain small and localized. Small cysts are commonly located posteriorly and anteriorly, possibly due to the confining adjacent muscles. Small cysts may remain small, especially if the labral tear heals. The cyst may spontaneously resolve, also possibly due to healing of the labral tear.31 The cysts can enlarge, sometimes reaching a size of multiple centimeters. The most common locations for larger labral cysts can be explained by the specific regional anatomy of the shoulder joint (Figure 3). The most frequent location of larger cysts is the posterosuperior aspect of the joint which can be accounted for by the fact that the posterosuperior capsule above the posterior band of the inferior glenohumeral ligament is an area of relative weakness when compared with the thicker anterior capsule.32 This weakness may allow easier penetration by dissecting fluid. Once a cyst forms, it expands through the path of least resistance into the fibro-fatty tissue that lies between the supraspinatus and infraspinatus muscle bellies in the posterior superior quadrant. This channels cysts that originate from posterosuperior labral tears toward the spinoglenoid notch and the suprascapular notch. An alternative posterior pathway is along the gutter formed by the bony glenoid, the fibro-cartilaginous glenoid labrum, and the origin of the infraspinatus muscle, which may explain why pure posterior tears (reverse Bankart lesions) may channel superiorly and then medially between the 2 muscle bellies similar to those cysts seen with posterior superior tears or posterior extension of superior labral tears (SLAP lesions). The anterior superior path of least resistance is the recess between the labrum and anterior capsule projecting into the subscapularis recess often associated with the anterior aspect of a SLAP lesion (Figure 3). A common pathway for cyst extension often associated with a chronic Bankart lesion below the subscapularis tendon is anteriorly and inferiorly into the quadrilateral space as in the test case.

3a
Figure 3:
Labral cysts can occur anywhere a labral tear is present. Smaller cysts tend to occur posteriorly where the infraspinatus and teres minor muscle bellies restrict the size of the cyst and straight anteriorly where the subscapularis muscle belly tends to restrict their size. Larger cysts (long arrow) form posterosuperiorly and superiorly (typically due to a SLAP lesion) where the cyst is channeled between the infraspinatus and supraspinatus (path of least resistance) into the spinoglenoid and/or suprascapular notch. In this setting the suprascapular nerve (red asterisk) may be compressed resulting in denervation of the supraspinatus and/or infraspinatus muscles. A larger cyst may project anteriorly (short arrow) into the subscapularis recess in the anterosuperior quadrant. Larger cysts may also form anteroinferiorly or inferiorly (arrowhead) often from a Bankart lesion. If large enough, the cyst may dissect inferiorly adjacent to the triceps tendon into the quadrilateral space, where axillary denervation may occur from compression by the cyst (blue asterisk).

4a

4b
Figure 4:
Fat-suppressed proton density-weighted axial (4A) and coronal images (4B) show anteriorly (short arrow) and posteriorly (long arrow) projecting cysts associated with a chronic SLAP lesion leading to suprascapular denervation. Note the subacute denervation changes of the infraspinatus as a result of cyst compression of the suprascapular nerve (arrowheads).
Cysts around the shoulder joint have been termed labral cyst, paralabral cyst, ganglion cyst, synovial cyst, pseudocyst, and intramuscular and intratendinous cysts.4,13,14,27,29,33 Cysts in this discussion will be termed labral cysts when arising from the labrum and intratendinous or intramuscular cysts when arising from a rotator cuff tear if localized to the tendon (intratendinous) or into the muscle belly (intramuscular). Labral cyst is preferred when the cystic lesion is seen adjacent to the labrum, as this term emphasizes the important anatomic features of the lesion, rather than the variably defined terms ganglion and synovial cyst that describe the histologic appearance of the cyst wall.
Clinical Presentation
A labral cyst of the shoulder joint is present in 2-4% of the general population, particularly in males during the 3rd and 4th decade.8 The cyst may be asymptomatic, be associated with nonspecific shoulder pain often in association with glenohumeral arthrosis, may be associated with clinical glenohumeral instability and/or in association with compression neuropathy.4 Instability of the shoulder should be clinically suspected and evaluated for when a cyst is found with an anterior inferior (Bankart), posterior (reverse Bankart), posterior superior (often posterior extension of a SLAP lesion), or superior labral tear (SLAP lesion). If the cyst is large enough, it may dissect into the suprascapular or spinoglenoid notch (or both) to impinge upon the suprascapular nerve or the quadrilateral space to impinge upon the axillary nerve. In the case of nerve impingement, the patient may present with pain, muscle weakness, and resulting loss of proprioception. In the case of suprascapular denervation there will be weakness of the muscles innervated (supraspinatus and infraspinatus). In the case of compression neuropathy of the axillary nerve within the quadrilateral space, there will be weakness of the deltoid and teres minor muscles (Table 1). 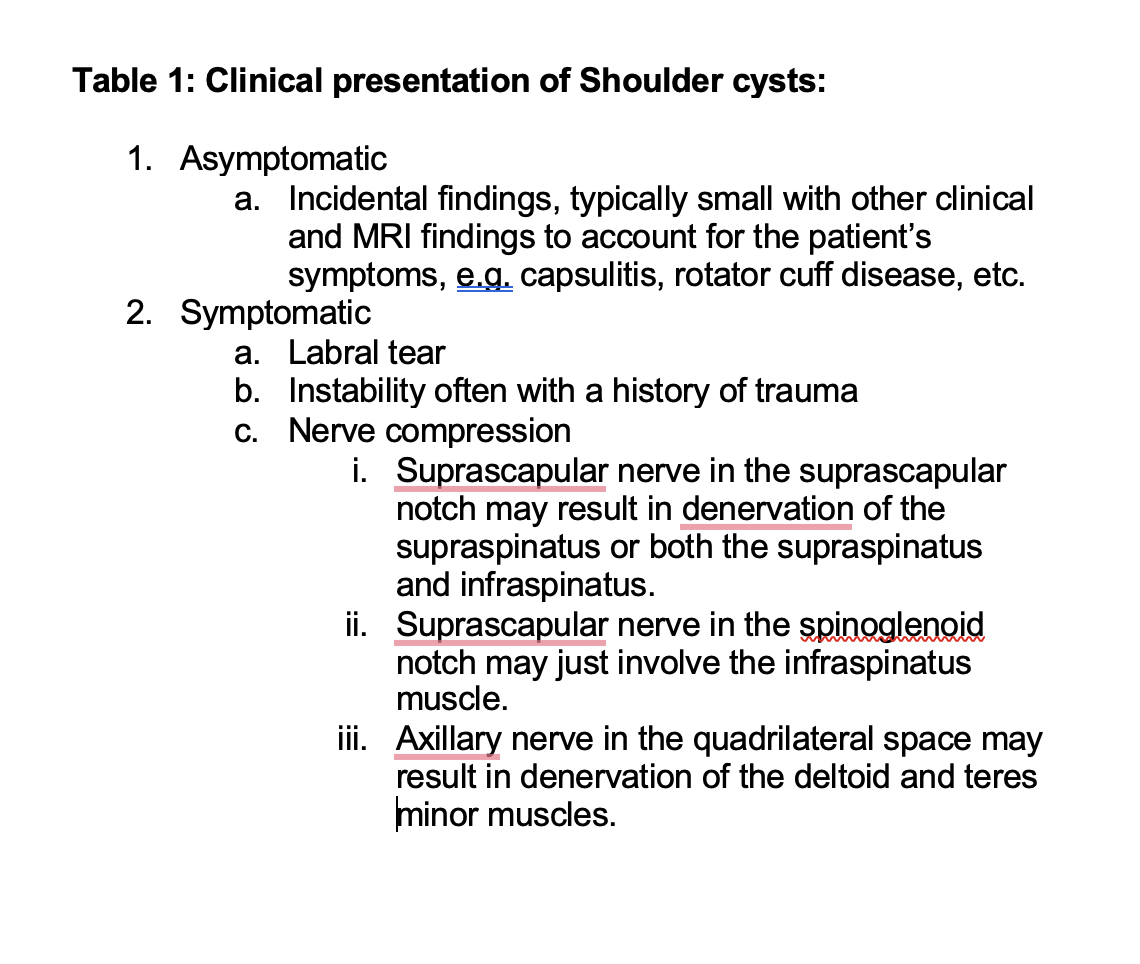
MRI Findings
Shoulder cysts are decreased in signal intensity on TI-weighted images and of increased signal intensity on T2- or T2*-weighted images.1,2,4,34 The cysts can be unilocular (Figure 5), multilocular (Figure 6), rounded or oval-shaped, variably lobulated, and frequently located adjacent to a tear of the fibrocartilaginous glenoid labrum (Figure 7).1,4,29,34 Associated glenoid labral tears are characterized by areas of linear or complex increased signal intensity extending through the labrum on TI- weighted and GRE images, less intense high signal or fluid signal on T2-weighted images (Figure 7), or may be filled with contrast at MRI arthrography.

5a
Figure 5:
A fat-suppressed proton density-weighted axial image demonstrates a small focal unilocular labral cyst (arrowhead) adjacent to a subtle labral tear(arrow). The cyst may enlarge over time if the tear progresses or may stay stable in size or regress if the tear heals.

6a

6b
Figure 6:
(6A) A fat-suppressed proton density-weighted axial image shows a multiloculated labral cyst (arrowhead) and a fluid-filled posterior superior labral tear (arrow).
In a different patient (6B), a fat-suppressed proton density-weighted sagittal image reveals a multiloculated anterior inferior labral cyst (arrowheads) in a patient with a remote history of anterior shoulder subluxation. Clinically the patient had a history of chronic instability.

7a
Figure 7:
A fat-suppressed proton density-weighted coronal image demonstrates a suprascapular notch cyst (arrowhead) originating from a fluid containing SLAP lesion (arrow) without suprascapular nerve denervation change. Note the normal signal intensity of the supraspinatus muscle belly isointense to the subscapularis, trapezius, and deltoid muscle bellies.
Healed labral tears may not demonstrate contrast filling but still exhibit the findings of a non-fluid filled labral tear. The area of abnormal signal intensity in the labrum may be in contact with or connected to a portion of the cyst.1,4,29 An MRI arthrogram may (Figure 8) or may not (Figure 9) show contrast material extending from the shoulder joint into a cyst via a labral tear. As some patent labral tears may not be fluid filled, MRI (or CT) arthrography may be necessary to help prove patency (Figure 8).

8a

8b

8c

8d

8e
Figure 8:
(8A,B) Communicating cyst at MRI arthrography. A fat-suppressed proton density-weighted coronal image (8A) shows a fluid signal intensity small labral cyst (arrow) along the superior border of the supraglenoid tubercle. The SLAP lesion (arrowhead) is of increased signal consistent with degeneration or a tear but is not fluid filled on the T2 weighted image. It is uncertain whether the tear is patent on this image. A fat-suppressed T1-weighted coronal image after intraarticular injection of dilute gadolinium (8B), shows extension of the intraarticular contrast into the labral cyst (arrow) proving patency of the tear communicating with the joint through a SLAP lesion (arrowhead). In a different patient (8C,D,E) a multiloculated communicating cyst is associated with a SLAP lesion. Fat-suppressed proton density-weighted axial (8C) and coronal images (8D) demonstrate the fluid signal intensity cyst projecting anteriorly at the superior joint (arrow). A fat-suppressed T1-weighted coronal image after injection of dilute gadolinium as an arthrogram (8E) shows contrast enhancement of the cyst (arrowhead) proving patency of the SLAP lesion and communication of the cyst with the joint through the labral tear.

9a

9b
Figure 9:
Non-communicating cyst at MR arthrography. A fat-suppressed proton density-weighted coronal image (9A) shows a cyst (arrow) medial to the posterior glenoid extending into the spinoglenoid notch. Note fluid signal intensity within a posterior inferior labrum tear (arrowhead). A corresponding fat-suppressed T1-weighted coronal image (9B) after injection of dilute gadolinium as an arthrogram shows contrast within the posterior inferior labral tear (arrowhead) but no contrast within the cyst medial to the posterior glenoid (arrow). The cyst is difficult to see because of the lack of enhancement and the isointensity of the fluid-filled cyst on a T1-weighted image to that of adjacent muscle. In this example, communication of the cyst with the joint through the labral tear is not proven. It is possible that patency and communication exists in this case but not proven because the image was acquired shortly after the injection. Delayed imaging may have eventually shown filling of the cyst.
Similarly intratendinous and/or intramuscular cysts will exhibit the same MRI findings of a labral cyst except that the cyst is often away from the joint within the tendon or muscle (or both) and is not associated with the labrum. Intratendinous or muscular cysts tend to be associated with delaminating rotator cuff tears13,14 and often appear elongated (Figure 10). The connection to the articular surface or full thickness rotator cuff tendon tear may be patent (Figure 11) or closed (Figure 12). Cysts with patent communication may fill with contrast in the case of CT or MRI arthrography, thus proving patency whether the communication with the joint is directly visualized or not visualized (Figure 11).

10a
Figure 10:
Intratendinous and/or intramuscular cysts can form from a break in the glenohumeral capsule (short arrow) in association with a rotator cuff tear, often a delamination tear. The cyst tends to be elongated and can extend medially into the muscle belly (long arrow). The presence of the cyst indicates communication with the articular surface although the opening that led to the cyst may close by healing. Arthrography may demonstrate the patency of the communication if present.

11a

11b

11c
Figure 11:
Communicating intramuscular cyst. A fat-suppressed proton density-weighted coronal image (11A) demonstrates a fluid-intensity cyst within the posterior supraspinatus muscle belly (arrow). Fat-suppressed T1-weighted coronal (11B) and sagittal (10C) images after injection of dilute gadolinium as an arthrogram demonstrate faint contrast filling the cyst (arrows) within the posterior aspect of the supraspinatus muscle belly, proving communication of the cyst with the joint through a patent tendon tear. The tendon tear is not shown on these images.

12a

12b

12c
Figure 12:
Non-communicating intramuscular cyst. Fat-suppressed proton density-weighted coronal (12A) and sagittal (12B) images show a fluid intensity cyst within the supraspinatus myotendinous junction (arrows). A fat-suppressed T1-weighted coronal arthrogram (12C) image reveals no contrast entering the cyst (arrow), thus not proving communication of the cyst with the joint through a patent tendon tear. The cyst is difficult to see on the T1-weighted image due to the cyst being relatively isointense to adjacent muscle.
Cysts and associated labral tears are frequently found with posttraumatic changes of the glenoid because of a traumatic etiology of the labral tear. Posttraumatic changes can include subchondral cyst formation from posttraumatic arthrosis, intraosseous extension of the labral cyst, or both (Figure 13).

13a
Figure 13:
Labral cyst associated with chronic posttraumatic deformity of the posterior glenoid including intraosseous cyst formation in a patient with a chronic posterior instability history. Intraosseous cyst (arrow) formation was contiguous with a labral cyst (arrowhead).
Administration of intravenous gadolinium may show smooth rim enhancement of a cyst without internal enhancement. Pericystic enhancement may occur including within a labral tear as a result of hyperemia, possibly inflammatory mediated. (Figure 14).

14a

14b
Figure 14:
Rim enhancement of a labral cyst after intravenous gadolinium administration given to evaluate a chondroid mass in the humeral head. A fat-suppressed proton density-weighted axial (14A) image demonstrates a fluid signal intensity cyst (arrowhead) within the spinoglenoid notch and a fluid filled tear (short arrow) of the posterior labrum with an elongated neck (long arrow) leading to the cyst. A fat-suppressed T1-weighted axial (14B) image after injection of intravenous gadolinium contrast reveals rim enhancement of the cyst (arrowhead) without internal enhancement, typical of the benign enhancement pattern of labral cysts. Note faint enhancement of the neck and enhancement of the tear felt to be due to granulation, hyperemia or both. Communication of the tear and cyst is not inferred on a T1-weighted image after intravenous gadolinium administration as it can be during an arthrogram. The humeral head “mass” was an enchondroma.
Radsource Teleradiology Partnerships for Busy Radiology Teams
Boost your diagnostic confidence with RadSource’s Teleradiology services & partnership. Reliable MRI interpretation is just a click away.
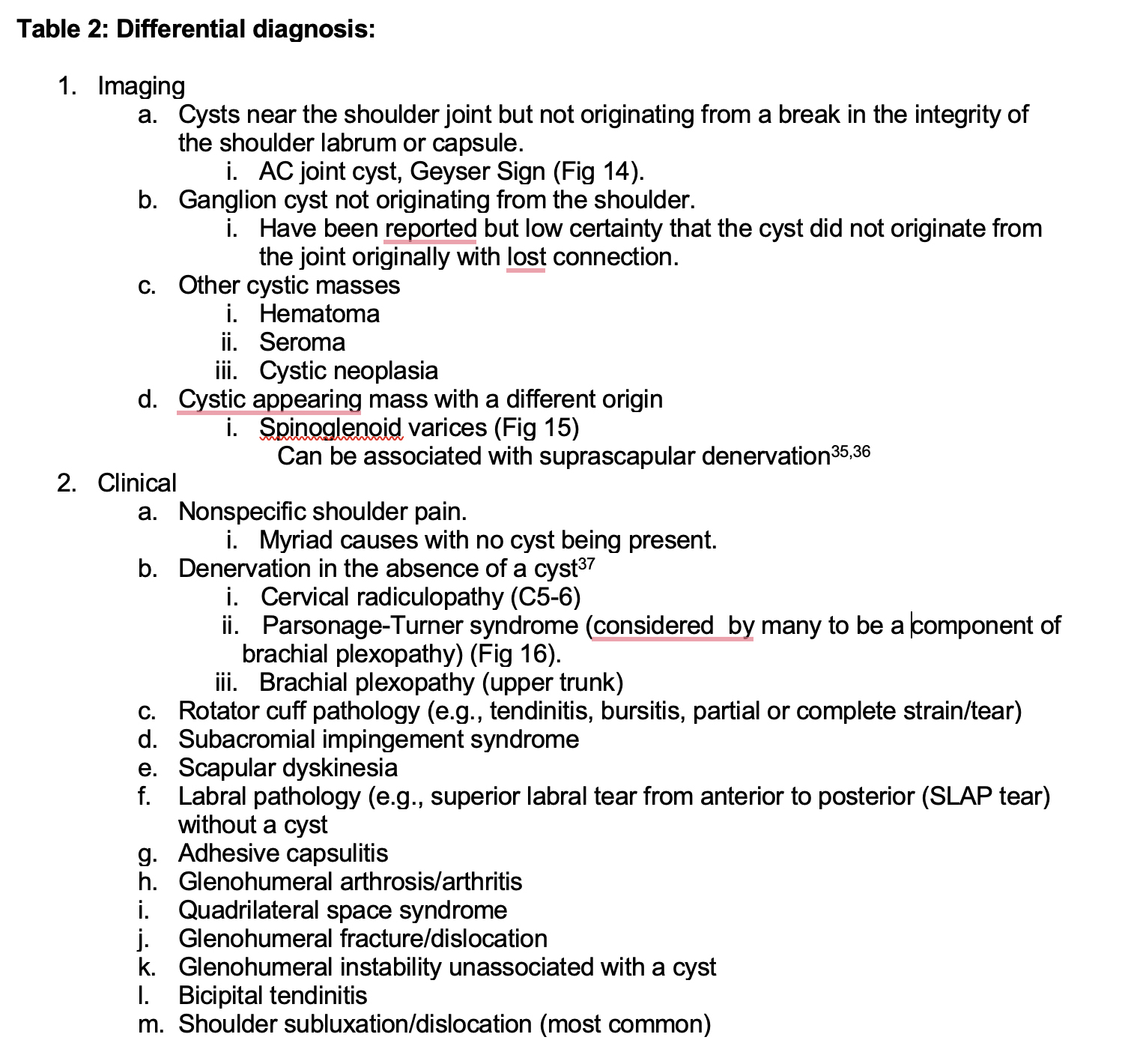
Differential Diagnosis
Differential diagnostic possibilities can be split into imaging and clinical differentials. Imaging differential diagnostic possibilities include any cystic mass originating outside of the joint and include cysts originating from the AC joint typically associated with AC joint arthrosis as a result from previous trauma or a cyst that forms superior to the AC joint as a result of a defect in the acromioclavicular joint ligaments in association with long standing subacromial subdeltoid bursitis, also referred to as the geyser sign.27,34 Other diagnostic possibilities include cystic masses arising from trauma such as a hematoma acutely or sub-acutely or serous collections, including a degloving lesion from trauma or seroma from prior trauma or surgery. Varices arising in the venous plexus normally found in the spinoglenoid notch can enlarge, appear as a cystic mass and can be associated with suprascapular nerve denervation.35,36 Finally, cystic neoplasm may mimic a labral cyst. Clinically the differential diagnostic possibilities are varied and extensive as the cyst can be asymptomatic or symptomatic and associated with glenohumeral instability in the case of an associated labral tear or denervation in the case of nerve compression associated with a larger cyst or both. Any suprascapular or axillary denervation presentation that occurs without a cyst present can have a similar clinical presentation and therefore is in the differential diagnosis. Shoulder pain from a wide variety of causes are typically not associated with a cyst (Table 2) but can be associated and are therefore in the list of differential diagnostic possibilities.37

15a
Figure 15:
Differential Diagnostic consideration for a shoulder labral or intramuscular cyst. A fat-suppressed proton density-weighted coronal image shows a cyst (arrow) extending superiorly from the AC joint and not originating from the shoulder joint.

16a

16b
Figure 16:
Prominent varices in the spinoglenoid and suprascapular notches associated with suprascapular nerve denervation. T1-weighted coronal image (16A) and fat-suppressed proton density-weighted coronal image (16B) demonstrate fatty atrophy of the supraspinatus muscle belly (arrow) in a patient with clinical suprascapular denervation. Prominent varices (arrowheads) appear as elongated cystic masses within the spinoglenoid notch (16B).

17a

17b
Figure 17:
Fat-suppressed proton density-weighted coronal images show supraspinatus (long arrow) (17A) and infraspinatus (short arrow) (17B) denervation changes in a patient without a cyst and with the clinical diagnosis of Parsonage Turner Syndrome.
Treatment
Treatment of labral cysts includes repair of the associated labral tear with or without drainage of the cyst.3,6,8,38,39 Cyst aspiration alone has been performed with recurrences reported4 and the general consensus is to treat the causative labral tear in order to prevent recurrence.3,6,8,38,39 In the case of compression neuropathy, current recommendations are to decompress the cyst and repair the labrum (often a SLAP lesion or posterior superior labral tear).3,9,39 There is a relative paucity of reports of treatment of intratendinous and/or intramuscular cysts and in general cyst decompression may be accomplished at the time of rotator cuff repair. Many cysts are incidental and may be treated conservatively if found in a patient that is not a good candidate for rotator cuff surgery.
Conclusion
Cysts around and within the shoulder most commonly arise from a tear of the labrum or shoulder capsule and can occur in up to 4% of patients, (possibly higher) presenting for MRI with shoulder pain. The clinical presentation varies and the cysts can be asymptomatic or be painful in the setting of instability with a labral tear. The cyst may also be associated with pain in the case of an intratendinous and/or intramuscular cyst associated with a rotator cuff tear. Larger labral cysts in the posterior superior quadrant can compress the suprascapular nerve and cysts in the anterior inferior quadrant can compress the axillary nerve and cause neuropathy. MRI is an excellent modality to demonstrate cysts, labral tears, and compression neuropathy, as well as associated findings related to chronic instability. MRI arthrography can demonstrate patency of an associated labral or rotator cuff tendon tear by filling of the cyst with contrast. The results of MRI or MRI arthrography aid in the clinical management of a patient with a cyst about the shoulder.
References
- Tirman PFJ, Feller JF, Janzen DL, Peterfy CG, Bergman AG. Association of glenoid labral cysts with labral tears and glenohumeral instability: Radiologic findings and clinical significance. Radiology. 1994;190(3). ↩
- Sanders TG, Tirman PFJ. Paralabral cyst: An unusual cause of quadrilateral space syndrome. Arthroscopy – Journal of Arthroscopic and Related Surgery. 1999;15(6). ↩
- Promsang T, Kongrukgreatiyos K, Kuptniratsaikul S. Arthroscopic Decompression of Spinoglenoid Notch Cyst and SLAP Repair Through a Single Working Portal. Arthrosc Tech. 2018;7(9). ↩
- Tung GA, Entzian D, Stern JB, Green A. MR imaging and MR arthrography of paraglenoid labral cysts. American Journal of Roentgenology. 2000;174(6). ↩
- Mencias T, Kotsonis T. Poster 279 Delayed Diagnosis of a Posterior Superior Labral Tear with Associated Suprascapular Neuropathy: A Case Report. PM&R. 2014;6(9S). ↩
- Schrøder CP, Lundgreen K, Kvakestad R. Paralabral cysts of the shoulder treated with isolated labral repair: effect on pain and radiologic findings. J Shoulder Elbow Surg. 2018;27(7). ↩
- Ramaswamy AG, Patil NP, Srinivasan N. An unusual case of anteroinferior paralabral cyst with axillary nerve compression: A case report. Journal of Arthroscopic Surgery and Sports Medicine. 2021;3. ↩
- Moon CY, Ji JH, Kim SJ. Multidirectional instability accompanying an inferior labral cyst. Clin Orthop Surg. 2010;2(2). ↩
- Shon MS, Jung SW, Kim JW, Yoo JC. Arthroscopic all-intra-articular decompression and labral repair of paralabral cyst in the shoulder. J Shoulder Elbow Surg. 2015;24(1). ↩
- Ji JH, Shafi M, Lee YS, Kim DJ. Inferior paralabral ganglion cyst of the shoulder with labral tear – A rare cause of shoulder pain. Orthopaedics and Traumatology: Surgery and Research. 2012;98(2). ↩
- Moore TP, Fritts HM, Quick DC, Buss DD. Suprascapular nerve entrapment caused by supraglenoid cyst compression. Journal of shoulder and elbow surgery / American Shoulder and Elbow Surgeons. (et al). 1997;6(5). ↩
- Athwal GM. Shoulder Joint Labral Tear. https://orthoinfo.aaos.org/en/diseases–conditions/shoulder-joint-tear-glenoid-labrum-tear/. 2022. ↩
- Sanders TG, Tirman PFJ, Feller JF, Genant HK. Association of intramuscular cysts of the rotator cuff with tears of the rotator cuff: Magnetic resonance imaging findings and clinical significance. Arthroscopy. 2000;16(3). ↩
- Choo HJ, Lee SJ, Kim JH, Kim DW, Park YM, Kim OH, et al. Delaminated tears of the rotator cuff: Prevalence, characteristics, and diagnostic accuracy using indirect MR arthrography. American Journal of Roentgenology. 2015;204(2). ↩
- Neviaser TJ, Ain BR, Neviaser RJ. Suprascapular nerve denervation secondary to attenuation by a ganglionic cyst. JBJS. 1986;68(4):627–8. ↩
- Garizhom R HJHMSHE. Suprascapular nerve entrapment: a case report. . Bone Joint Surg [Am ↩
- Fritz RC, Helms CA, Steinbach LS, Genant HK. Suprascapular nerve entrapment: Evaluation with MR imaging. Radiology. 1992;182(2). ↩
- Thompson Jr RC, Schneider W, Kennedy T. Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia. Clin Orthop Relat Res. 1982;(166):185–7. ↩
- Ogino T, Minami A, Kato H, Hara R, Suzuki K. Entrapment neuropathy of the suprascapular nerve by a ganglion. A report of three cases. JBJS. 1991;73(1):141–7. ↩
- Takagishi K, Maeda K, Ikeda T, Itoman M, Yamamoto M. Ganglion causing paralysis of the suprascapular nerve: Diagnosis by MRI and ultrasonography. Acta Orthop Scand. 1991;62(4):391–3. ↩
- Moran MC, Warren RF. Development of a synovial cyst after arthroscopy of the shoulder. A brief note. JBJS. 1989;71(1):127–9. ↩
- Proscan Imaging. THEY IN’CYST’ED THAT WE HAVE A HISTOLOGICAL REVIEW. Retrieved from https://proscan.com/proscan-case-review/msk/they-incysted-that-we-have-a-histological-review/. 2018. ↩
- Lantz B, Singer KM. Meniscal cysts. Clin Sports Med. 1990;9(3):707–25. ↩
- Burk DL, Dalinka MK, Kanal E, Schiebler ML, Cohen EK, Prorok RJ, et al. Meniscal and ganglion cysts of the knee: MR evaluation. American Journal of Roentgenology. 1987;150(2). ↩
- Giard MC, Pineda C. Ganglion cyst versus synovial cyst? Ultrasound characteristics through a review of the literature. Rheumatol Int. 2015;35(4):597–605. ↩
- Beaman FD, Peterson JJ. MR imaging of cysts, ganglia, and bursae about the knee. Magn Reson Imaging Clin N Am. 2007;15(1):39–52. ↩
- Bermejo A, de Bustamante TD, Martinez A, Carrera R, Zabía E, Manjón P. MR imaging in the evaluation of cystic-appearing soft-tissue masses of the extremities. Radiographics. 2013;33(3):833–55. ↩
- Perdikakis E, Skiadas V. MRI characteristics of cysts and “cyst-like” lesions in and around the knee: what the radiologist needs to know. Insights Imaging. 2013;4(3):257–72. ↩
- Neto N, Nunnes P. Spectrum of MRI features of ganglion and synovial cysts. Insights Imaging [Internet ↩
- Apostolaki E, Davies AM, Evans N, Cassar-Pullicino VN. MR imaging of lumbar facet joint synovial cysts. Eur Radiol. 2000;10(4):615–23. ↩
- Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg. 2002;11(6):600–4. ↩
- O’Brien SJ, Neves MC, Arnoczky SP, Rozbruck SR, Dicarlo EF, Warren RF, et al. The anatomy and histology of the inferior glenohumeral ligament complex of the shoulder. Am J Sports Med. 1990;18(5):449–56. ↩
- Giard MC, Pineda C. Ganglion cyst versus synovial cyst? Ultrasound characteristics through a review of the literature. Rheumatol Int. 2015;35(4):597–605. ↩
- O’Connor EE, Dixon LB, Peabody T, Stacy GS. MRI of cystic and soft-tissue masses of the shoulder joint. American Journal of Roentgenology. 2004;183(1). ↩
- van Meir N, Fourneau I, Debeer P. Varicose veins at the spinoglenoidal notch: an unusual cause of suprascapular nerve compression. J Shoulder Elbow Surg. 2011;20(7):e21–4. ↩
- Carroll KW, Helms CA, Otte MT, Moellken S, Fritz R. Enlarged spinoglenoid notch veins causing suprascapular nerve compression. Skeletal Radiol. 2003;32(2):72–7. ↩
- Reece CVMSAdam. Suprascapular Nerve Injury. NIH National Library of Medicine. ↩
- Prasad NK, Spinner RJ, Smith J, Howe BM, Amrami KK, Iannotti JP, et al. The successful arthroscopic treatment of suprascapular intraneural ganglion cysts. Neurosurg Focus. 2015;39(3). ↩
- Ji JH, Park SE, Suh DW, Han YH, Oh S. Comparisons between treatment of isolated posterosuperior paralabral cysts and simultaneous treatment of cysts combined with associated shoulder pathologies: arthroscopic treatment of posterosuperior paralabral cysts. Arch Orthop Trauma Surg. 2021; ↩
