Clinical history: A 38 year old female presents with a 10 month history of right hip and groin pain. Axial and sagittal fat-saturated proton density images are provided. What are the findings? What is your diagnosis?

1a

1b
Figure 1:
Axial and sagittal fat-saturated proton density images .
Findings

2a

2b
Figure 2:
Axial (2a) and sagittal (2b) fat-saturated proton density images demonstrate compression and moderate edema (arrows) of the right quadratus femoris muscle due to a narrowed ischiofemoral space. LT=lesser trochanter, I=ischium.
Diagnosis
Ischiofemoral impingement.
Introduction
Ischiofemoral impingement (IFI) was first reported by Johnson in 19771 in three patients with hip pain after hip surgery. Two patients had undergone total hip arthroplasty and one, a proximal femoral osteotomy. Each patient presented with pain that was increased with adduction of the extended hip. In two patients the lesser trochanter region was tender to palpation. Radiographs revealed narrowing between the ischium and lesser trochanter, with enlargement of the lesser trochanter. It was concluded that the pain was “due to a pinching of soft tissues between bone prominences”. Due to failure of conservative management, each patient underwent surgical excision of the lesser trochanter with complete relief of pain.
Beginning in 2008, IFI has been rediscovered as a source of hip, groin, and/or posterior thigh pain.2,3 Prior to that time, edema signal intensity on MR within the quadratus femoris muscle (QFM) was attributed to muscle strains. Using MR, it has been recognized that a narrowed ischiofemoral space may cause impingement or compression of the QFM, resulting in muscle edema and, over time, muscle atrophy. On physical exam, pain is elicited with various hip motions. It is important for the radiologist to be aware of IFI as it is added to the already long list of orthopaedic and non-orthopaedic conditions that may manifest as hip, groin and/or posterior thigh pain.4
Quadratus femoris anatomy and function
Quadratus femoris, Latin for “square muscle of the thigh,” is a quadrilateral-shaped muscle located between the lesser trochanter of the proximal femur and the ischial tuberosity. Its origin is often broad-based at the superior aspect of the lateral surface of the ischial tuberosity, just anterior to the origin of the semimembranosus tendon. It has a narrow insertion on the quadrate tubercle and adjacent base of the intertrochanteric crest, at the posteromedial aspect of the proximal femur. In normal adults the quadratus femoris muscle (QFM) occupies a 2 cm width between the ischium and proximal femur.1The muscle fibers are compact at the femoral end (adjacent to the narrow insertion) and are more loosely arranged, with interspersed fat, at the ischial aspect.5 A bursa may be found between this muscle and the lesser trochanter. The QFM is bordered anteriorly by the obturator externus muscle, posteriorly by the sciatic nerve, superiorly by the inferior gemellus muscle and inferiorly by the adductor magnus muscle (Figures 3-5).

3a
Figure 3:
Normal anatomy on an axial proton density image. At the intertrochanteric level, the quadratus femoris muscle (Q) extends from the lateral surface of the ischium to the posteromedial surface of the proximal femur. G=gluteus maximus m., H=common hamstring tendon, arrowhead=sciatic nerve, I=ischium, OE=obturator externus m., IP=iliopsoas muscle and tendon, P=pectineus m.

4a
Figure 4:
Normal anatomy on an axial proton density image. At the level of the lesser trochanter, the sciatic nerve (arrowhead) and the hamstrings (H) are posterior to the quadratus femoris muscle (Q). AM=adductor magnus m., AB=adductor brevis m., P=pectineus m., IP=iliopsoas muscle.

5a

5b
Figure 5:
3-D renderings of the short hip rotator muscles: (5a) posterior perspective and (5b) anterior perspective. In (5a), the sciatic nerve (SN) is depicted exiting the sciatic foramen below the inferior margin of the piriformis muscle (P) and coursing posterior to the superior gemellus (SG), obturator internus (OI), inferior gemellus (IG) and quadratus femoris (Q) muscles. In (5b), the obturator externus (OE) muscle is anterior and superior to the quadratus femoris.
The QFM is one of the short rotator muscles of the hip along with the piriformis, superior and inferior gemellus, and obturator internus and externus muscles. It is a strong external rotator of the hip and thigh that assists with adduction. It is innervated by a small branch of the sacral plexus, the nerve to the quadratus femoris. This nerve emerges from the pelvis through the greater sciatic notch, travels inferiorly along the anterior border of the gemellus and obturator internus muscles and enters the QFM at its anterior surface. The medial circumflex femoral artery provides the arterial supply to the QFM.5
Clinical Presentation
IFI typically occurs in middle-aged to elderly women and is uncommon in males. The youngest patient reported was an 11 year old female. Bilateral hip involvement has been observed in 25-40% of patients.3,7 Most patients present with hip and/or groin pain. Distal radiation of pain to the posterior thigh and knee is not uncommon and is likely due to irritation of the adjacent sciatic nerve. Chronic low back pain is common and may prompt an MRI of the lumbar spine as the first advanced imaging test performed. Patients may report a snapping sensation, locking of the joint and crepitation.3,6,8 On physical examination, most patients have pain during hip range of motion. Symptoms may be reproduced by a combination of hip extension, adduction and external rotation or with flexion and internal rotation.6,7,9 This pain is usually localized to the posterior hip.7
Imaging Features
In patients with IFI, radiographs are usually normal but may show abnormal proximity of the ischium and lesser trochanter with subcortical cysts and sclerosis of the opposing surfaces.2 MRI is used to assess the size and signal intensity of the QFM and the space available for this muscle between the ischium and proximal femur. The axial plane is best for this and also demonstrates the QFM origin and insertion, adjacent muscles and tendons and the sciatic nerve. The space available for the QFM is subdivided into the ischiofemoral space and the quadratus femoris space (Figure 6). The quadratus femoris origin, muscle belly and insertion are also well shown on sagittal images. Coronal images demonstrate the QFM and its origin from the ischium. STIR, fat-suppressed proton density or fat-suppressed T2-weighted images are required to detect muscle edema. QFM atrophy with fatty replacement is best evaluated with axial T1-weighted images.

6a
Figure 6:
Normal anatomy on an axial proton density image. The ischiofemoral space (red line) is measured from the medial cortex of the lesser trochanter to the lateral cortex of the ischium. The quadratus femoris space (white line) is measured from the superolateral surface of the hamstring tendons to the posteromedial surface of the iliopsoas tendon or lesser trochanter.
On MRI, the QFM demonstrates edema, centered on the muscle belly, at the site of maximal impingement (Figure 7).10 On sagittal images, this edema is posterior to the lesser trochanter. With increased severity of impingement, edema becomes more severe and diffuse and may involve the surrounding soft tissue. Mild muscle enhancement is observed following intravenous administration of gadolinium.2,3,8 Fatty replacement of the QFM varies from absent to severe (Figure 8). A narrowed ischiofemoral space has been reported in all cases thus far.

7a
Figure 7:
Ischiofemoral impingement. In a 54 year old female with right hip pain x 6 months, an axial fat-saturated proton density image reveals right ischiofemoral narrowing, moderate quadratus femoris muscle compression and edema (arrows) and a partial tear of the common hamstring origin (arrowhead).

8a
Figure 8:
75 year old female with chronic bilateral ischiofemoral impingement. An axial T2-weighted image demonstrates bilateral ischiofemoral narrowing and quadratus femoris muscle atrophy with fatty replacement (arrows), greater on the left. Note small, bilateral bursa-like fluid collections (arrowheads). R=right, L=left.
Tosun et al. studied 70 hips in 50 patients with hip pain and QFM edema in order to evaluate the utility of several imaging parameters for diagnosis of IFI.7 QFM edema was scored as follows: grade 0 – normal muscle signal intensity; grade 1 – focal edema where IFS and QFS were narrowest; grade 2 – diffuse edema confined to muscle; grade 3 – edema extending to surrounding soft tissues. Fatty replacement was graded as follows: grade 0: no intramuscular fat signal intensity; grade 1 – tiny linear fat signal intensity between muscle fibers; grade 2 – linear and globular fat signal intensity occupying <50% of the QFM; grade 3 – globular fat signal intensity occupying> 50% of the muscle. Other parameters were defined and measured as follows (results listed in Table 1):
Ischiofemoral space (IFS): The smallest distance between the lateral cortex of the ischial tuberosity and medial cortex of the lesser trochanter on axial T1-weighted images.
Quadratus femoris space (QFS): The smallest space for the passage of the QFM bordered by the superolateral surface of the hamstring tendons and the posteromedial surface of the iliopsoas tendon or lesser trochanter on axial T1-weighted images.
Inclination angle (IA): Angle between the long axis of the femoral neck and the long axis of the femoral shaft on coronal T1-weighted images.
Hamstring tendon area (HTA): This tendon’s borders (including all of the semimembranosus, semitendinosus and the biceps femoris tendons) were traced on axial T1-weighted images at the level where the QFS was measured.
Total QFM volume (TQFMV): Borders of the QFM contours were traced on axial T1-weighted images and volume was calculated using the workstation.
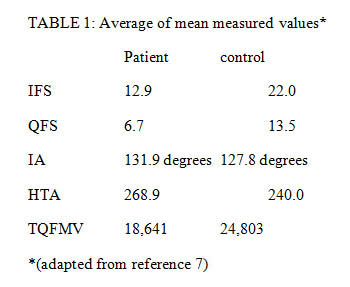
The reliability of QFM edema for diagnosis of IFI was not determined because a criterion for inclusion in the control group was a normal pelvic or hip MRI. Therefore, no control patients had QFM edema. In the patient group, 71% of hips had grade 1 edema, 21% grade 2 and 7% grade 3. It is not known what percentage of patients without IFI would demonstrate QFM edema on MRI. In one series of nine patients, three had bilateral QFM edema and two of these had only unilateral pain. QFM fatty replacement grades were significantly higher in the patient group, although, 50% of control hips revealed grade 1 or 2 fatty replacement. The cause of fatty replacement is uncertain, however, muscle atrophy, with replacement by intra-muscular fat, is the end-stage of many of the disease processes that produce muscle edema.11 An entrapment neuropathy is possible but would probably not account for this finding in controls. QF denervation may occur without prior tear, due to an injury or lesion of the QF nerve.5
The IFS and QFS of the patient group were significantly more narrow than that of the control group. These values are similar to those obtained in a smaller study which reported: IFS: patients=13mm, controls=23mm; QFS: patients=7mm, controls=12mm.3 Patients were studied with the hips either in neutral position7 or internally rotated.3 MRI with the hip in external rotation must be avoided as this may lead to overestimation of IFS and QFS narrowing.3 The mean IA in the patient group (131.9 degrees) was significantly elevated compared to that of the control group (127.8 degrees), consistent with coxa valga contributing to a narrowed IFS. The HTA was significantly higher than that of the control group and may contribute to narrowing of the QFS. The TQFMV value was significantly lower in the patient group and may be due to decreased space available for the muscle. Decreased muscle volume due to atrophy may also be contributory. Measurement of HTA and TQFMV may be impractical for the typical radiology practice as they require a workstation and are operator intensive.
In patients with IFI, IFS narrowing has been reported as bilateral in 25-40%, consistent with a congenital etiology.3,7 A strong female predominance (84 – 100% of patients) is observed.3,7 This is likely due to the female pelvis having greater width and smaller depth with the ischial tuberosities everted and further apart, resulting in a widened pelvic outlet. Not all females have a narrowed IFS so this anatomic difference may represent a relative predilection toward IFS narrowing. Several acquired conditions may narrow the IFS and QFS, including superior and medial migration of the proximal femur due to osteoarthrosis, osteochondroma, prominent lesser trochanter (Figure 9), enlarged ischium from prior fracture (Figure 10), QFM atrophy, displaced intertrochanteric fracture and valgus intertrochanteric osteotomy. The QFS may also be narrowed by enthesophytes extending laterally from the proximal hamstring origin. The prevalence of a narrowed IFS and QFS in asymptomatic patients is unknown. It is not uncommon that patients present with bilateral IFS narrowing and unilateral pain, sometimes with mild QFM edema on the asymptomatic side.

9a
Figure 9:
Ischiofemoral impingement. Axial fat-saturated proton density image in a 39 year old female with right hip and buttock pain shows ischiofemoral narrowing with a prominent lesser trochanter (arrowhead), compression and edema of the quadratus femoris muscle (long arrows) and a small partial tear of the right common hamstring origin (short arrow).

10a

10b
Figure 10:
Ischiofemoral impingement. Axial proton density (10a) and fat-saturated proton density (10b) images in a 58 year old male with left hip pain reveal an expanded left ischium (asterisk) (most likely due to remote avulsion fracture) with a narrowed ischiofemoral space. In (10a), fatty atrophy of the lateral aspect of the quadratus femoris muscle is evident (short arrow). (10b) reveals moderate central edema of the quadratus femoris muscle (long arrow) and about the iliopsoas tendon at its insertion on the lesser trochanter (arrowhead).
Progressive narrowing of the IFS, over a 16 month period, has been documented in a 17 year old female who presented with post-traumatic hip pain and developed IFI, a snapping hip and an abnormal gait (with hip adduction).8 The authors postulate that the abnormal gait may have led to IFS narrowing. Snapping was alleviated by resection of the lesser trochanter. A snapping sensation with motion of the hip has been reported in one other patient with IFI and in two patients with partial tear of the QFM.3,12 Snapping may be due to interposition of the QFM, iliopsoas muscle or hamstring tendon between the ischium and lesser trochanter or be related to bursitis. One study of 12 hips with IFI revealed partial tear of the hamstring attachment in 3, hamstring tendon edema (from mild to severe) in 6 and mild iliopsoas peritendinous edema in 4.3 These hamstring and iliopsoas tendon changes tended to occur in patients with severe QFM edema and may be due to strain, overuse or enthesopathy. Partial tear of the QFM was observed in one-third of affected hips. Bursa-like formation may occur about the lesser trochanter and sciatic nerve. In patients with findings of ischiofemoral impingement and other adjacent muscle, tendon or bursal abnormalities, it may be difficult to determine the primary contributor to the patient’s symptoms (Figure 11).

11a
Figure 11:
Ischiofemoral impingement. In a 73 year old female with bilateral hip pain x 6 months, an axial STIR image reveals ischiofemoral narrowing, greater on the left, mild bilateral quadratus femoris muscle edema (long arrows), partial tear of each common hamstring origin (arrowheads) and a small amount of fluid within the right obturator externus bursa (short arrow).
The range of abnormality of the QFM in patients who are asymptomatic or with other causes of hip pain is uncertain. QFM edema or atrophy and ischiofemoral narrowing have been observed in asymptomatic patients (Figure 12). Symptomatic patients with QF edema have been observed with normal space parameters, however, at least some of these may have had QFM tear, rather than impingement.10,12

12a
Figure 12:
Bilateral ischiofemoral impingement and unilateral symptoms. In a 58 year old female with only left hip pain, an axial fat-saturated proton density image reveals bilateral ischiofemoral narrowing and moderate left (long arrow) and mild right (short arrow) quadratus femoris muscle edema. Moderate left (arrowhead) and mild right (asterisk) hamstring tendinosis is present.
Differential Diagnosis
Based on the clinical presentation and findings on physical examination, the differential diagnosis of IFI may be quite long but principally includes QFM or adductor muscle tear and tendinitis, hamstring injury, snapping hip syndrome, piriformis syndrome and lumbar radiculopathy.5,13 Tear of the QFM is infrequently reported in the medical literature.12-15 Patients may present with acute or chronic hip, groin and/or posterior gluteal pain. In a summary of 7 reported cases, none was correctly diagnosed clinically. Diagnoses that were offered were hamstring injury, adductor tendinitis, snapping hip syndrome, stress fracture or sciatica. In each case diagnosis was achieved utilizing MR.12 In one reported case with persistent sciatica 6 months after injury, an up to 5 cm diameter hematoma was compressing the sciatic nerve.16
On MR, QFM tears appear as an area of intramuscular fluid signal intensity with surrounding muscle edema. Published cases of QFM tears usually involve the distal myotendinous junction, at the posteromedial aspect of the proximal femur, although tear at the femoral tendon insertion has also been reported (Figure 13).16 A grade I strain appears as muscle edema and may occur at the ischial origin of the QFM or as central or diffuse muscle edema, indistinguishable from that seen with IFI (Figure 14). In these cases, the clinical history of acute onset of pain associated with activity or the absence of IFS narrowing lead away from a diagnosis of ischiofemoral impingement. Isolated QFM strains or tears are uncommon. Rather, QFM injury is often accompanied by hamstring or adductor muscle strain or tear. In a study of acute, slow speed stretching injuries of the hamstrings in dancers, both the semimembranosus tendon and QFM were involved in 87% of cases. This injury occurs during hip flexion and knee extension and usually has a prolonged recovery time.17

13a
Figure 13:
QFM tear. In a 48 year old female with right hip pain, an axial STIR image shows central and distal quadratus femoris muscle edema (arrowheads) and a mild tear (grade 2 strain) of the distal quadratus femoris myotendinous junction (arrow).

14a

14b
Figure 14:
QFM strain. In a 26 year old female with left hip pain, axial; fat-saturated proton density (14a) and coronal fat-saturated T2-weighted (14b) images demonstrate a small focus of edema within the ischial origin of the left quadratus femoris muscle (arrow), consistent with a grade 1 strain. Minimal bilateral tendinosis of the common hamstring origins is present (arrowheads).
A snapping hip has been reported in five patients with IFI.2,3,8,12 It is probably due to interposition of soft tissue, such as the QFM, iliopsoas muscle, hamstring tendons or bursal thickening and fluid, between the narrowed ischiofemoral space. This may lead to confusion with snapping hip syndrome, which refers to pain and/or an audible or perceived snapping of the hip during hip motion.18-20 In contrast to the older age group typically affected with IFI, snapping hip usually occurs in teenagers and young adults. Clinical diagnosis of the underlying pathoanatomy is sometimes difficult.
Depending upon the cause, a snapping hip may be characterized as intra-articular or extra-articular. Intra-articular causes include acetabular labral tear, loose body, cartilage flaps, fracture fragments, synovial osteochondromatosis and synovial folds.19 Diagnosis is accomplished with MR or MR-arthrography and surgery is often required. Extra-articular causes are categorized as internal or external. The external, extra-articular form is the most common overall and is due to abnormal motion of the ilotibial band or gluteus maximus muscle over the greater trochanter with hip flexion and extension. This is usually diagnosed clinically. An internal snapping hip is usually due to abnormal motion of the iliopsoas tendon over the iliopectineal eminence, the lesser trochanter or the anterior-inferior iliac spine.21 Because of its dynamic capability and decreased cost, ultrasound is preferred over MR for this diagnosis. The offending iliopsoas tendon is often normal on MR but tendinosis, peritendinous fluid or iliopsoas bursitis may be observed. Most patients with a snapping iliopsoas tendon respond to conservative treatment. Tendon release or lengthening or fasciotomy may be performed in those with persistent symptoms.20
Piriformis syndrome is a rare, controversial clinical entity in which buttock and hip pain are attributed to entrapment of the sciatic nerve by the piriformis muscle at the greater sciatic notch. Potential etiologies include an enlarged piriformis muscle (Figure 15), a constricting fibrous band, anomalous course of the sciatic nerve through the muscle and anomalous sacral attachment of the piriformis muscle medial to the S2 foramen, crossing over the right S2 nerve. MRI of the pelvis has shown potential in evaluating this syndrome but a large series of patients has not been studied due to the rarity of this disorder.22,23

15a

15b
Figure 15:
T1-weighted (15a) coronal and (15b) axial images in a patient with left lower extremity weakness and numbness reveal asymmetrical enlargement of the left piriformis muscle (P). The resultant decreased space within the sciatic notch (arrowheads) is readily apparent on 15b.
Potentially in the differential diagnosis of IFI are the myriad causes of groin pain. Perhaps the most frequent is chronic adductor longus tendinitis. The list includes a wide range of entities including acetabular labral tear, femoroacetabular impingement, athletic pubalgia, osteitis pubis, avascular necrosis, pelvic inflammatory disease and classic hernias. In middle-aged and elderly women (the typical patient with IFI), stress fracture is an important cause of hip or groin pain and MR is usually relied upon for diagnosis.
Treatment
No definitive treatment strategy for IFI has been established. Initial treatment is conservative and includes rest, activity restriction and non-steroidal anti-inflammatory drugs. Computed tomography-guided infiltration of the QFM with local anesthetic and steroid has been reported to provide long-lasting pain relief.3 For patients who do not respond to conservative management, surgical excision of the lesser trochanter and removal of reactive or bursal-type tissue has been performed without reports of complication.1,8 It has been suggested that periarticular endoscopic decompression of the ischiofemoral space may be a feasible approach.9 This technique has been used to treat snapping iliopsoas tendon, gluteus medius and minimus tears and sciatic nerve compression.24,25
Conclusion
Ischiofemoral impingement is an uncommon source of hip, groin and/or posterior thigh pain that is usually seen in middle-aged to elderly women. Congenital or acquired narrowing of the ischiofemoral space results in compression or impingement of the quadratus femoris muscle, leading to edema, best demonstrated by MR. Fatty atrophy of the muscle may ensue. It is postulated that, with severe edema, irritation of the adjacent sciatic nerve may cause sciatica. MRI is required for diagnosis but not all patients with ischiofemoral narrowing or quadratus femoris muscle edema are symptomatic. Affected patients often have adjacent muscle or tendon abnormalities and these, as well as the hip joint, are generally well evaluated with MR.
References
1 Johnson KA. Impingement of the lesser trochanter on the ischial ramus after total hip arthroplasty. Report of three cases. J Bone Joint Surg Am 1977; 59:268-269.
2 Patti JW, Ouellette H, Bredella MA, Torriani M. Impingement of lesser trochanter on ischium as a potential cause for hip pain. Skeletal Radiol 2008; 37:939-941.
3 Torriani M, Souto SC, Thomas BJ, Ouellette H, Bredella MA: Ischiofemoral impingement syndrome: an entity with hip pain and abnormalities of the quadratus femoris muscle. AJR 2009; 193:186-190.
4 Shah A, Busconi B. In DeLee JC, Drez D Jr., Miller MD: Orthopaedic Sports Medicine. Principles and Practice, 3rd Edition, Saunders Elsevier, 2010: 1451-1477.
5 Kassarjian A, Tomas X, Cerezal L, Canga A, Llopis E. MRI of the quadratus femoris muscle: anatomic considerations and pathologic lesions. AJR 2011; 197: 170-174.
6 Tosun O, Nurdan C, Bozkurt M, Arslan H. Ischiofemoral impingement in an 11-year-old girl. Diagn Interv Radiol DOI 10.4261/1305-3825.DIR.5728-12.1, 2012, published online.
7 Tosun O, Algin O, Yalcin N, et al. Ischiofemoral impingement: evaluation with new MRI parameters and assessment of their reliability. Skeletal Radiol 2012; 41:575-587.
8 Ali AM, Whitwell D, Ostlere SJ. Case report: imaging and surgical treatment of a snapping hip due to ischiofemoral impingement. Skeletal Radiol 2011; 40:653-656.
9 Stafford GH, Villar RN. Ischiofemoral impingement. J Bone Joint Surg Br 2011; 93:1300-1302.
10 Kassarjian A. Signal abnormalities in the quadratus femoris muscle: tear or impingement? AJR 2008; 190:W379; author reply W380-381.
11 McMahon CJ, Wu JS, Eisenberg RL. Muscle edema. AJR 2010; 194:865-866.
12 O’Brien SD, Bui-Mansfield LT. MRI of Quadratus femoris muscle tear: another cause of hip pain. AJR 2007; 189:185-1189.
13 Klinkert P Jr, Porte RJ, de Rooij TP, de Vries AC. Quadratus femoris tendinitis as a cause of groin pain. BR J Sports Med 1997; 31:348-349.
14 Peltola K, Heinonen OJ, Orava S, Mattila K. Quadratus femoris muscle tear: an uncommon cause for radiating gluteal pain. Clin J Sport Med 1999; 9:228-230.
15 Willick SE, Lazarus M, Press JM. Quadratus femoris muscle strain. Clin J Sport Med 2002; 12:130-131.
16 Bano A, Karantanas A, Pasku D, et al. Persistent sciatica induced by quadratus femoris muscle tear and treated by surgical decompression: a case report. Journal of Medical Case Reports 2010; 4:236-239.
17 Askling CM, Tengvar M, Saartok T, Thorstensson A. Proximal hamstring strains of stretching type in different sports. Injury situations, clinical and magnetic resonance imaging characteristics, and return to sport. Am J Sports Med 2008; 36:1799-1804.
18 Pelsser V, Cardinal E, Hobden R, et al. Extraarticular snapping hip: sonographic findings. AJR 2001; 176:67-73.
19 Blakenbaker DG, Tuite MJ. The painful hip: new concepts. Skeletal Radiol 2006; 35: 352-370.
20 Deslandes M, Guillin R, Cardinal E, et al. The snapping iliopsoas tendon: new mechanisms using dynamic sonography. AJR 2008; 190:576-581.
21 Miller TT. Abnormalities in and around the hip: MR imaging versus sonography. Magn Reson Imaging Clin N Am 2005; 13:799-809.
22 Russell JM, Kransdorf MJ, Bancroft LW et al. Magnetic resonance imaging of the sacral plexus and piriformis muscles. Skeletal Radiol 2008; 37:709-713.
23 Pecina HI, Boric I, Smoljanovic T, Duvancic D, Pecina M. Surgical evaluation of magnetic resonance imaging findings in piriformis muscle syndrome. Skeletal Radiol 2008; 37:1019-1023.
24 Ilizaliturri VM Jr, Chaidez C, Villegas P, Briseno A, Camacho-Galindo J. Prospective randomized study of 2 different techniques for endoscopic iliopsoas tendon release in the treatment of internal snapping hip syndrome. Arthroscopy 2009; 25:159-163
25 Martin HD, Shears SA, Johnson JC, Smathers AM, Palmer IJ. The endoscopic treatment of sciatic nerve entrapment/deep gluteal syndrome. Arthroscopy 2011; 27:172-181.
