Clinical History: A 30 year old male with shoulder pain and instability. Fat-suppressed (1a) axial proton density and (1b) T2-weighted oblique coronal images are provided. What are the findings? What is your diagnosis?

1a

1b
Figure 1:
Fat-suppressed (1a) axial proton density and (1b) T2-weighted oblique coronal images
Findings

2a

2b
Figure 2:
(2a) The fat-suppressed axial proton density-weighted image demonstrates a tear of the anterior inferior labrum (arrowhead). The inferior glenohumeral ligament (arrow), labrum, and periosteum (short arrows) are stripped and displaced medially along the glenoid neck, in a sleeve-like fashion. (2b) The fat-suppressed oblique coronal T2-weighted image demonstrates an impaction fracture of the posterolateral aspect of the humeral head (Hill Sachs deformity) (arrow), which occurred when the humeral head struck the anterior inferior glenoid during anterior dislocation. (An associated joint effusion is seen on both the axial and oblique coronal images.)
Diagnosis
ALPSA and Hill Sachs deformities, secondary to acute anterior glenohumeral dislocation.
An ALPSA lesion is an anterior labroligamentous periosteal sleeve avulsion. ALPSA is a variation of the Bankart lesion where the anterior inferior labrum is torn and the labrum, inferior glenohumeral ligament and intact scapular periosteum are stripped and displaced medially on the glenoid neck. 1, 2

3a
Figure 3:
The ALPSA lesion is characterized by a torn anteroinferior labrum (L) with an intact but stripped periosteum (P) and medial displacement of the labrum and inferior glenohumeral ligament (IGHL) relative to the glenoid (G). The humerus is indicated as H.
Introduction
The glenohumeral joint is a synovial-lined ball-in-socket joint that has the greatest range of motion of any joint in the human body. The glenohumeral joint is the most commonly dislocated joint, attributed to the much larger articular surface area of the humeral head and the smaller, shallow glenoid fossa.3,4,5 The glenoid labrum is a fibrocartilaginous cuff surrounding the glenoid fossa. The labrum deepens the fossa and increases the articular surface area of the glenoid. The osseous rim of the glenoid and the fibrocartilaginous labrum are sites of attachment for the glenohumeral ligaments and long head biceps tendon, which can be injured individually or in tandem.
Glenohumeral stability is provided by dynamic and static “restraints” (4a). Dynamic restraints include the rotator cuff and the long head biceps brachii tendon. Static restraints include the glenohumeral ligaments, glenohumeral joint capsule (including the rotator cuff interval capsule), the coracohumeral ligament, the glenoid labrum, and the bones.2,4,6,22 The attachments of the glenohumeral ligaments and the long head biceps anchor to the labrum are stronger than the attachment of the labrum to the glenoid rim.5 Therefore, the glenoid labrum is commonly torn or avulsed when excessive force is applied to a glenohumeral ligament or the long head biceps.3,7-11 These injuries have classic appearances, and are associated with multiple acronyms (such as ALPSA and SLAP) and eponyms (like the Hill Sachs deformity).
Relevant anatomy

4a
Figure 4:
Lateral view of the shoulder with the humerus removed demonstrates the restraints of the glenohumeral joint. Inferior glenohumeral ligament (IGHL), middle glenohumeral ligament (MGHL), superior glenohumeral ligament (SGHL), long head of the biceps (LHB), and coracohumeral ligament (CHL). The supraspinatus (Sup), infraspinatus (Is), subscapularis (Sub), and teres minor (Tm), and coracoacromial ligament (CAL) are indicated.
The glenohumeral ligaments (inferior, middle, and superior) are thickened bands of the joint capsule that extend from the inferior and anterior glenoid and glenoid labrum, to the anatomic neck region of the humerus, protecting against extreme range of motion.
The inferior glenohumeral ligament (IGHL) (5a,6a) is a hammock-like structure that attaches to the inferior glenoid, glenoid labrum, and the humeral neck. Thickened portions of the IGHL anteriorly and posteriorly are referred to as the anterior and posterior bands. Anterior inferior shoulder dislocation is the most common cause of shoulder instability, and the anterior band of the inferior glenohumeral ligament is believed to represent the major passive stabilizer of the glenohumeral joint.

5a
Figure 5:
A fat suppressed axial T1-weighted MR arthrogram image demonstrates the anterior band of the inferior glenohumeral ligament (arrow).

6a
Figure 6:
A fat suppressed oblique sagittal T1-weighted MR arthrogram image, demonstrating the anterior and posterior bands of the inferior glenohumeral ligament (arrows).
The middle glenohumeral ligament (MGHL) (7a) is the most variable of the glenohumeral ligaments. It varies in thickness and is associated with labroligamentous anatomic variations such as in the Buford complex. The MGHL can share a common origin with the superior glenohumeral ligament, can be absent in approximately one tenth to one third of shoulders, and functions to help stabilize the shoulder anteriorly from 0-45 degrees of abduction and external rotation. 5,7,20

7a
Figure 7:
A fat suppressed oblique sagittal T1-weighted MR arthrogram image demonstrating the middle glenohumeral ligament (arrow).
The superior glenohumeral ligament (SGHL) (8a) is the smallest of the glenohumeral ligaments and acts with the coracohumeral ligament to stabilize the glenohumeral joint and prevent posterior and inferior translation of the humeral head. The SGHL can have a common attachment with the long head biceps anchor to the superior glenoid/superior labrum. The long head biceps tendon can also attach along the anterior, posterior, or along both the anterior and posterior superior glenoid/labrum.

8a
Figure 8:
A fat suppressed axial T1-weighted MR arthrogram image demonstrates the superior glenohumeral ligament (arrow), the glenoid labrum (arrowhead), the long head biceps tendon (short arrow), and the coracohumeral ligament (curved arrow).
For localization purposes, the labrum is divided into four zones, six zones, or according to the location on a clock face (9a). The four zones are superior, anterior, inferior, and posterior. Further subdivision of the labrum into six zones includes: superior, anterosuperior, anteroinferior, inferior, posteroinferior, and posterosuperior. By convention, when utilizing the clock face, the mid superior labrum is denoted as 12 o’clock and the mid inferior labrum as 6 o’clock. There is controversy regarding 3 o’clock and 9 o’clock, as radiologists tend to classify the anterior labrum as 3 o’clock regardless of side, whereas some of the orthopaedic literature assumes 3 o’clock as anterior at the right shoulder but posterior at the left shoulder. For this reason, we favor utilizing a descriptive method of localization, utilizing zones and the use of equator as a designation of the mid anterior or posterior labrum.

9a
Figure 9:
A fat suppressed oblique sagittal T1 weighted MR arthrogram image, demonstrating the six labral zones of the glenoid labrum.
Discussion
The normal labrum (10a,11a) demonstrates low signal intensity on all pulse sequences, due to the lack of mobile protons in this dense fibrocartilage. On cross sectional imaging, the normal labrum is most commonly triangular, but can also be round, cleaved, notched, flat, or absent.12,19

10a
Figure 10:
A fat suppressed axial proton density-weighted MR image demonstrates a normal labrum. Note the homogeneous low signal intensity throughout the labral tissue both anteriorly and posteriorly (arrows).

11a
Figure 11:
A fat suppressed oblique coronal T2-weighted MR image demonstrates homogeneously low signal intensity in the normal superior labrum (arrow).
MRI diagnosis of labral tears is based on abnormalities in the signal intensity, morphology, and location (displacement) of the labrum. The labrum may be frayed, crushed, avulsed, or torn. Tears are classified by morphology, displaced or nondisplaced, and by location. Labral tears can extend into the biceps anchor as well as the glenohumeral ligaments. MRI criteria for diagnosing labral tears include surface irregularity, increased signal within the substance of the labrum that extends to the labral surface (12a), fluid or contrast imbibed into the substance of the labrum (13a), and labral avulsions. Secondary signs of labral tears include paralabral cysts (14a), periosteal stripping and tearing, labral associated bone injuries such as Hill Sachs and Osseous Bankart lesions, and hyaline cartilage injuries such as the GLAD lesion.

12a
Figure 12:
A fat suppressed axial gradient echo image demonstrates increased signal intensity in the anterior labrum that extends through the labrum to the articular and non-articular surfaces (arrowheads), consistent with an anterior labral tear.

13a
Figure 13:
A fat suppressed oblique coronal T1-weighted MR arthrogram image demonstrates contrast extending into the superior labrum, consistent with a superior labral tear (arrow).

14a
Figure 14:
A fat suppressed oblique coronal T2-weighted image demonstrates a superior labral tear (arrow) and associated paralabral cyst (arrowhead). (Rotator cuff tendinosis is also noted).
Multiple acronyms and eponyms are used to describe labral, glenohumeral ligament, and associated shoulder injuries. A Bankart lesion (15a) is a tear of the anterioinferior glenoid labrum with an associated tear of the anterior scapular periosteum, with or without associated fracture of the anterior inferior glenoid rim. (Some radiologists and surgeons use the term Bankart lesion to describe all tears of the anterioinferior labrum.)

15a
Figure 15:
A fat suppressed axial proton density-weighted image of a classic Bankart lesion, with tears of the anterioinferior labrum (arrow) and the adjacent scapular periosteum (arrowhead).

16a
Figure 16:
Illustration depicting the components of the classic Bankart lesion consisiting of a tear of the anteroinferior labrum (L) and periosteum (P). Inferior glenohumeral ligament (IGHL), humerus (H), and glenoid (G).
A Perthes lesion (17a) is a variant of the Bankart, where the anterioinferior labrum is avulsed from the glenoid and the scapular periosteum remains intact but is stripped medially.

17a
Figure 17:
A fat suppressed axial T1-weighted MR arthrographic image of a Perthes lesion demonstrates an avulsed anteroinferior labrum (arrow). The scapular periosteum remains intact but is stripped medially (arrow head).

18a
Figure 18:
The Perthes is a Bankart variant in which the labrum (L) is torn and the periosteum is stripped (P) but remains intact. Inferior glenohumeral ligament (IGHL), humerus (H), and glenoid (G).
A HAGL lesion (19a) is humeral avulsion of the glenohumeral ligament that occurs from shoulder dislocation, with avulsion of the inferior glenohumeral ligament from the anatomic neck of the humerus. A BHAGL is a bony HAGL, or a HAGL lesion that involves a bone fragment.


19a
Figure 19:
Fat suppressed oblique coronal T1-weighted MR arthrogram images of a HAGL lesion. The axillary pouch in a normal patient is typically "U" shaped. This patient's axillary pouch has an abnormal inverted "J" shape (arrowheads). There is fraying of the inferior glenohumeral ligament (arrow), and cortical irregularity along the humeral neck (short arrows) consistent with a humeral avulsion of the glenohumeral ligament.
The GLAD lesion (20a) refers to glenolabral articular disruption, which involves a tear of the anterior inferior labrum with an associated glenoid chondral defect.

20a
Figure 20:
A gradient-echo axial MR image of a GLAD lesion. The anterior labrum is torn (arrowhead) and there is an adjacent glenoid chondral defect (arrow).
The POLPSA lesion is a posterior labrum periosteal sleeve avulsion lesion. The POLPSA lesion is associated with posterior glenohumeral instability and most commonly occurs with posterior dislocation. In the POLPSA lesion, the posterior labrum is torn and the posterior scapular periosteum is intact but stripped from the posterior glenoid. The POLPSA lesion is similar to the ALPSA lesion, however it occurs posteriorly
SLAP (21a,22a,23a,24a) is an acronym for superior labral tears, that propagate anterior and posterior in reference to the biceps anchor. Originally, SLAP lesions were classified by Snyder et al, based on arthroscopic evaluation.13 Additional categories of SLAP tears were described by Maffet et al , Morgan et al , Resnick and Beltran.14,15,16 Although the classification of SLAP tears is useful in terms of prognosis and treatment, a careful description of the type and location of labral tear can provide equivalent information.
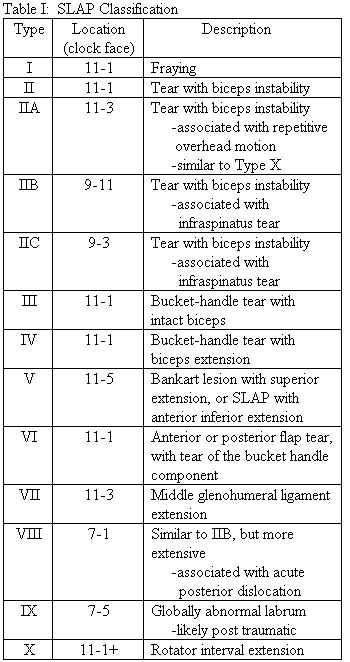
Snyder et al, Maffet et al, Morgan et al, Resnick and Beltran.13,14,15,16 Adapted from Mohana-Borges, Chung, and Resnick16

21a
Figure 21:
A fat suppressed oblique coronal T2-weighted MR image demonstrates a Type II SLAP lesion. Note fluid signal extending through the superior labrum (arrow) consistent with a superior labral tear. (Rotator cuff tendinosis with a tiny interstitial tear is also noted.)

22a
Figure 22:
A fat suppressed oblique coronal T1-weighted MR indirect arthrogram image demonstrates a Type IV SLAP lesion, with increased signal undercutting the superior labrum (arrow) and extending into the biceps tendon (arrowhead).

23a
Figure 23:
A fat suppressed axial T1-weighted MR arthrogram image demonstrates a Type VII SLAP lesion. The superior labral tear (arrowheads), extends into the conjoined attachment of the superior and middle glenohumeral ligaments (arrow). A small paralabral cyst (short arrow)arises posterosuperiorly from the superior labral tear.

24a
Figure 24:
A fat suppressed oblique sagittal MR arthrogram image demonstrates a global labral abnormality (arrowheads) consistent with Type IX SLAP lesion. Also note tearing and fraying of the labral/glenoid attachment of the middle glenohumeral ligament (arrow).
Labroligamentous anatomic variants can mimic pathology, but their appearance and typical location can aid in making the correct diagnosis. Labral variations most commonly ocurr anterosuperiorly, at the 11 o’clock to 3 o’clock position. The sublabral recess (25a) or sulcus is seen at the 11 o’clock to 1 o’clock position, at the junction of the biceps labral complex, but it does not extend posterior to the biceps anchor. The sublabral recess is differentiated from a labral tear by the specific location, the smooth margin, and the fact that it follows the contour of the glenoid. Sublabral recess occurrence increases with increasing patient age, suggesting that sublabral recesses are an age dependant degenerative phenomenon.17

25a
Figure 25:
A fat suppressed oblique coronal T1 MR arthrogram of a sublabral recess. Contrast undercuts the normal labrum and follows the contour of the glenoid cartilage (arrow heads), but does not extend posterior to the biceps anchor.
A sublabral hole, or foramen (26a), occurs between the anterosuperior labrum and the adjacent glenoid cartilage at the 12 o’clock to 3 o’clock position. It occurs most commonly at the 2 o’clock position, and in patients with a “pear shaped” glenoid.

26a
Figure 26:
A fat suppressed T1-weighted MR arthrogram of a sublabral hole (arrow). Sublabral holes/foramina occur anterosuperiorly (1 o'clock to 3 o'clock position). Note the smoothly contoured, otherwise normal appearing anterior superior labrum (arrow head), and middle glenohumeral ligament (short arrow).
The Buford complex (27a) is an anatomic variant that is seen anterosuperiorly, when the anterosuperior portion of the labrum is absent and the middle glenohumeral ligament is thick and cordlike.18

27a
Figure 27:
An axial fat suppressed T1-weighted MR arthrogram of a Buford complex. Note absence of the anterior superior labrum (arrowhead) and a thick, cord-like middle glenohumeral ligament (arrow).
Conclusion
Shoulder pain and instability are common orthopaedic problems. Although there are many causes of shoulder pain and instability (including fractures and rotator cuff tears), injuries to the glenohumeral ligaments, labrum, and biceps labral complex are often the cause. Its high spatial resolution, excellent image contrast, and multiplanar capabilities make MRI an excellent tool in the evaluation of the labrum. MR allows accurate depiction of the size and location of labral tears and their associated capsular and glenohumeral ligament injuries. Normal variants that can mimic pathology are also well depicted on MR imaging.
References
1 Neviaser TJ. The anterior labroligamentous periosteal sleeve avulsion lesion: a cause of anterior instability of the shoulder. Arthroscopy 1993; 9:17-21.
2 Waldt S. Burkart A, Imhoff AB, Bruegel M, Rummeny EJ, Woertler K. Anterior shoulder instability: accuracy of MR arthrography in the Classification of Anteroinferior labroligamentous injuries. Radiology 2005; 237:578-583.
3 Beltran J, Rosenberg ZS, Chandnani VP, Cuomo F, Beltran S, Rokito A. Glenohumeral instability: evaluation with MR arthrography. Radiographics 1997;17(3):657-673.
4 McCauley TR. MR imaging of the glenoid labrum. Magnetic resonance Imaging Clinics of North America 2004;12:97-109.
5 Bencardino JT, Beltran J. MR imaging of the glenohumeral ligaments. Magnetic resonance Imaging Clinics of North America 2004; 12:11-24.
6 Saupe N, White LM, Bleakney R, Schweitzer ME, Recht MP, Jost B, Zanetti M. Acute Traumatic Posterior Shoulder Dislocation: MR Findings. Radiology 2008; 248:185-193.
7 Palmer WE, Brown JH, Rosenthal DI. Labral-ligamentous complex of the shoulder: evaluation with MR arthrography. Radiology 1994; 190:645-651.
8 Bowen MK, Warren RF. Ligamentous control of shoulder stability based on selective cutting and static translation experiments. Clin Sports Med 1991; 10:757-782.
9 O’Connell PW, Nuber GW, Mileski RA, Lautenschlager E. The contribution of the glenohumeral ligaments to anterior stability of the shoulder joint. Am J Sports Med 1990; 18:579-584.
10 Turkel SJ, Panio NW, Marshall JL, et al. Stabilization mechanisms preventing anterior dislocation of the glenohumeral joint. J Bone Joint Surg 1981; 63:1208-1217.
11 Terry GC, Hammon D, France P, Norwood LA. The stabilizing function of passive shoulder restraints. Am J Sports Med 1991; 19-26-34.
12 Park YH, Lee JY, Moon SH, Mo JH, Yang BK, Hahn SH, Resnick, D. MR Arthrography of the Labral Capsular Ligamentous Complex in the Shoulder: Imaging Variations and Pitfalls. AJR 2000; 175:667-672.
13 Snyder SJ, Karzel RP, Del Pizzo W, et al. SLAP lesions of the shoulder. Arthroscopy 1990; 6:274-279.
14 Maffet MW, Gartsman GM, Moseley B. Superior labrum-biceps tendon complex lesions of the shoulder. Am J Sports Med 1995; 23:93-98.
15 Morgan CD, Burkhart SS, Palmeri M, Gillespie M. Type II SLAP lesions: three subtypes and their relationships to superior instability and rotator cuff tears. Arthroscopy 1998; 14:553-565.
16 Mohana-Borges AV, Chung CB, Resnick D. Superior labral anteroposterior tear: Classification and diagnosis on MRI and MR Arthrography. AJR 2003; 181:1449-1462.
17 DePalma AF, Gallery G, Bennett GA. Variational anatomy and degenerative lesions of the shoulder joint. In: American Academy of orthopaedic Surgery: Instructional course lectures, vol6. St. Louis: Mosby; 1949:225-281.
18 Williams MM, Snyder SJ, Buford D Jr. The Buford complex: the “cord-like” middle glenohumeral ligament and absent anterosuperior labrum complex – a normal anatomic capsulolabral variant. Arthroscopy 1994; 10:241-247.
19 Chung CB, Corrente L, Resnick D. MR arthrography of the shoulder. Magnetic resonance Imaging Clinics of North America 2004; 12:25-38.
20 De Maeseneer M, Van Roy P, Shahabpour M. Normal MR imaging anatomy of the rotator cuff tendons, glenoid fossa, labrum, and ligaments of the shoulder. Magnetic resonance Imaging Clinics of North America 2004; 12:1-10
21 Beltran J, Bencardino J, Mellado J, Rosenberg ZS, Irish RD. MR Arthrography of the shoulder: variants and pitfalls. Radiographics 1997; 17:1403-1412.
22 Morag Y, Jacobson JA, Shields G, Rajani R, Jamadar DA, Miller B, Hayes CW. Radiology 2005; 235:21-30.
23 Wischer TK, Bredella MA, Genant HK, Stoller DW, Bost FW, Tirman PF. Perthes Lesion (A Variant of the Bankart Lesion). AJR 2002; 178:233-237.
24 Cleeman E, Flatow EL. Shoulder dislocations in the young patient. Orthop Clin North Am 2000; 31(2):217-29.
Special thanks to Stadnick ME, Awh MH, Flemming DJ, Overdeck KH, and Caswell KL
