Clinical History
A 37-year-old man suffered a weight-lifting injury 6 weeks ago, with left hip and leg numbness, extending to the knee. No prior surgery. Sagittal (1A) T2-weighted, and fat-suppressed T1-weighted (1B) pre-contrast and (1C) post-contrast images are provided in addition to axial (1D) T2-weighted, and T1-weighted (1E) pre-contrast and (1F) post-contrast images. What are the findings? What is your diagnosis?






Findings
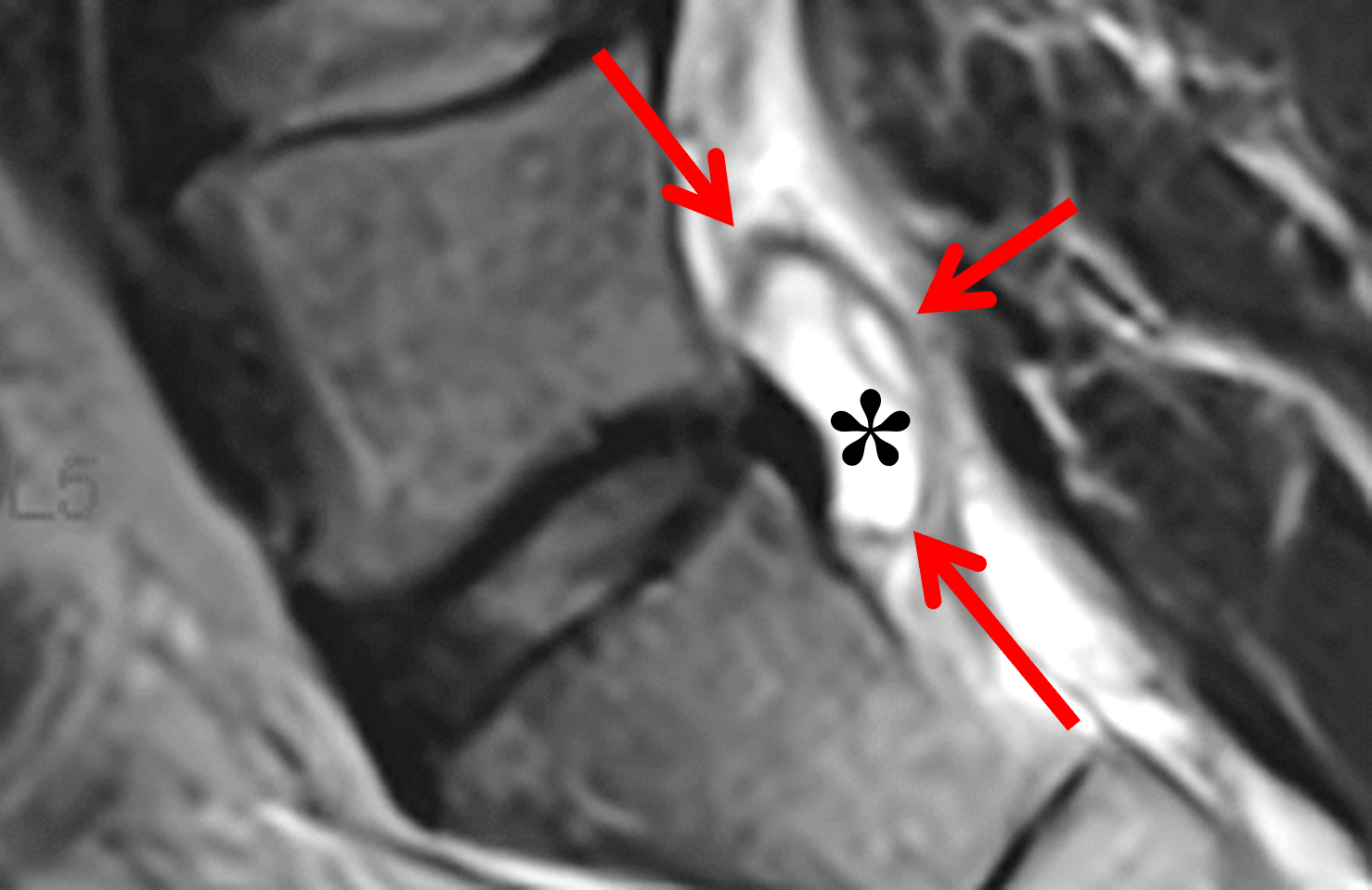
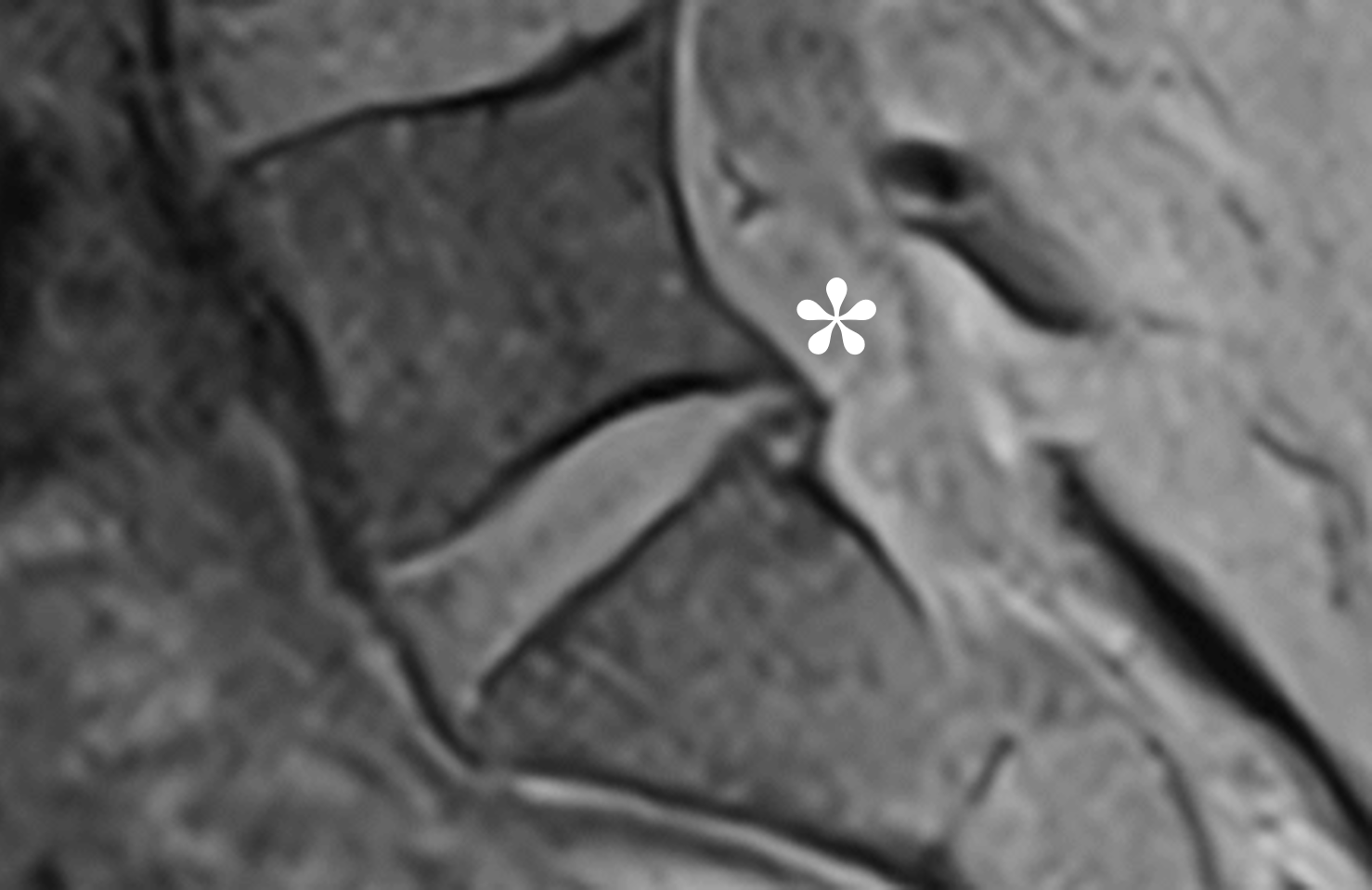
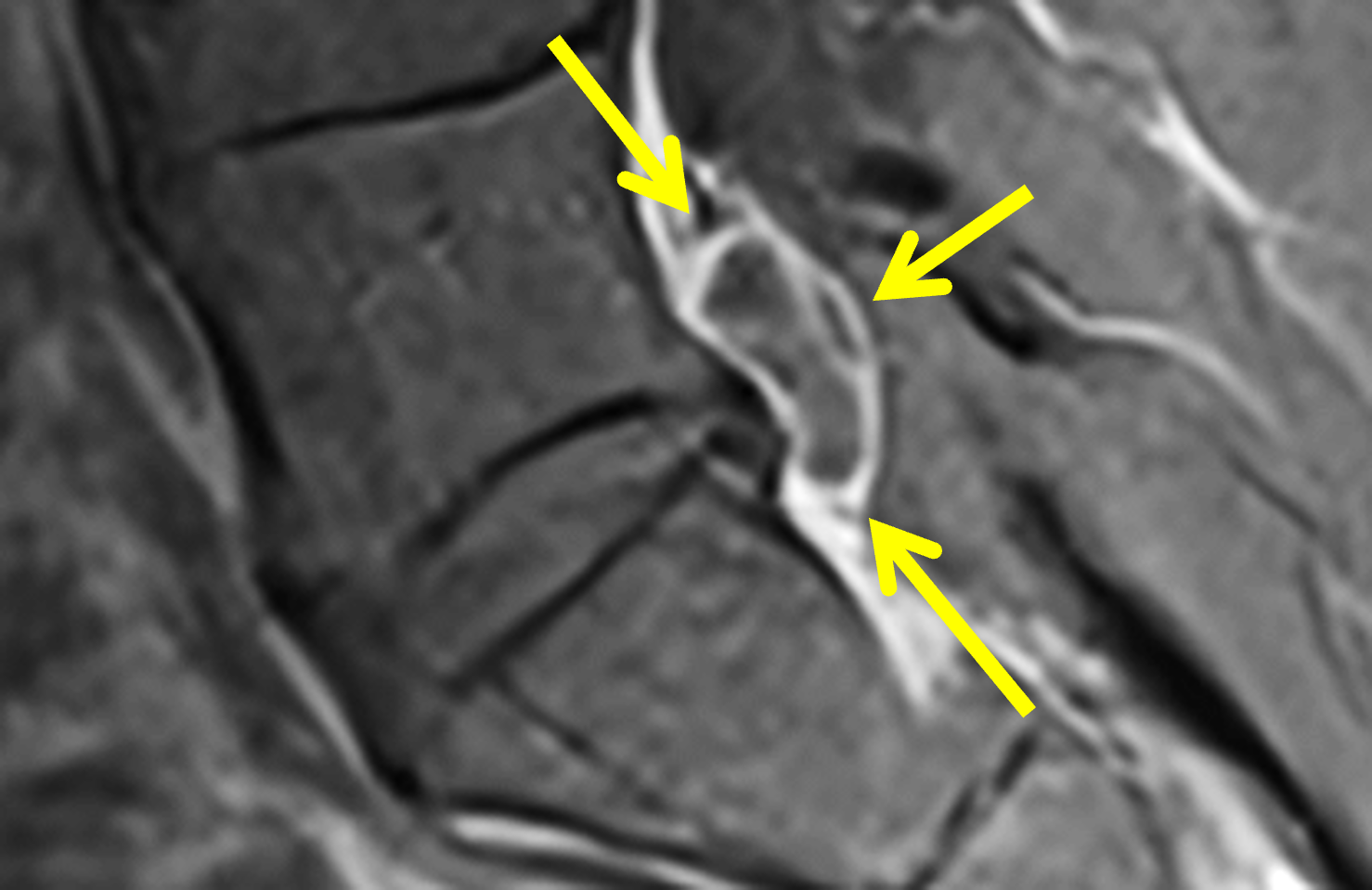


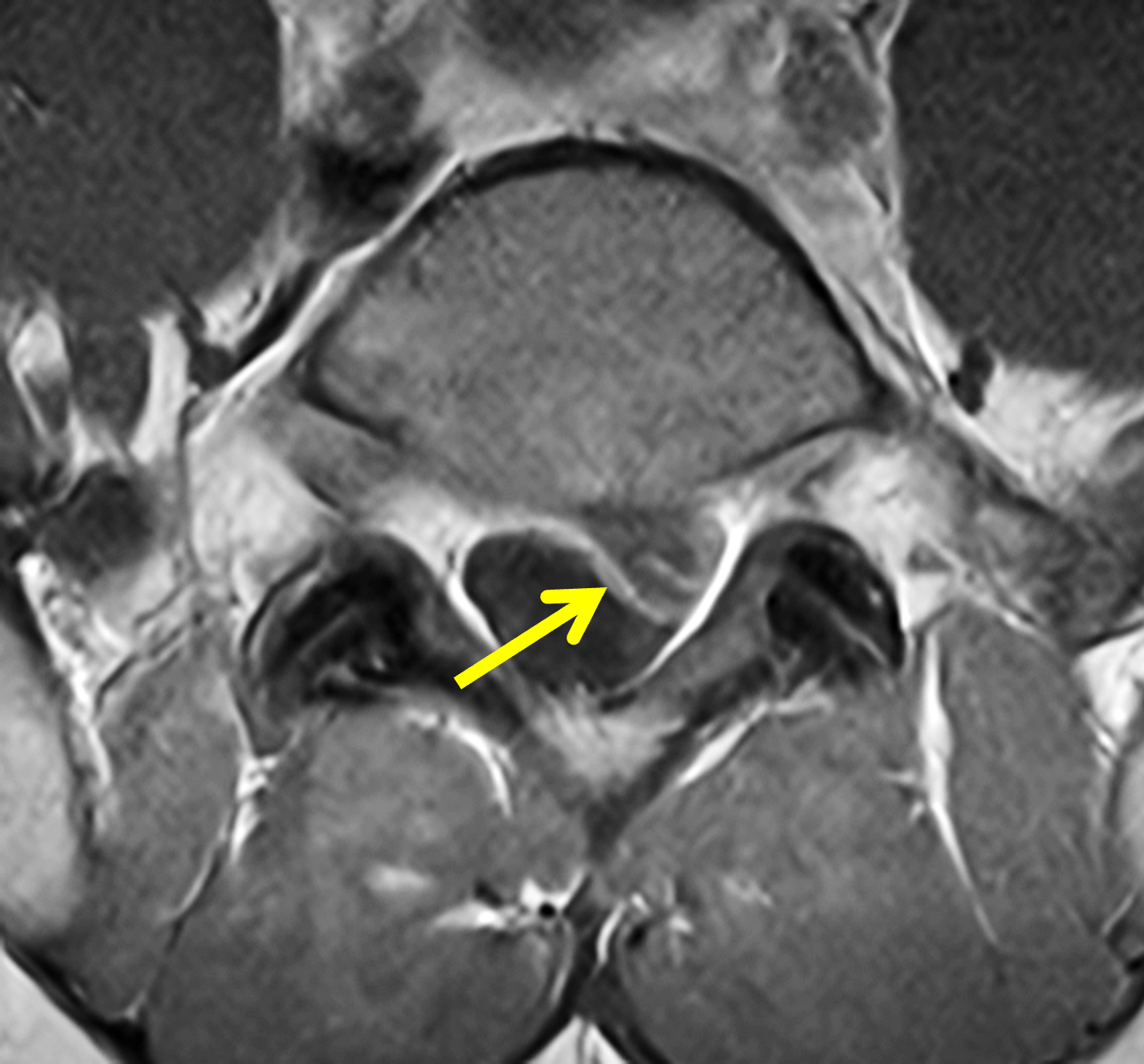
Figure 2: (2A) Sagittal T2-weighted image shows minimal disc degeneration at L5-S1, with an oval-shaped ventral epidural cyst (asterisk) with central signal intensity near CSF, a thin septation, and a hypointense peripheral rim (arrows). (2B) Sagittal fat-suppressed T1-weighted image shows the cyst (asterisk) is slightly hyperintense compared to CSF. (2C) Sagittal fat-suppressed T1-weighted image obtained after intravenous contrast administration shows a thin rim of peripheral enhancement (arrows) and enhancement of the thin septation. (2D) Axial T2-weighted image demonstrates the cyst (asterisk) abutting the dorsal margin of the disk, with mass effect on the ventral thecal sac and displacement of the left S1 nerve root (arrow). No facet joint effusion or arthritis is present. (2E) Axial T1-weighted image shows mildly hyperintense cyst contents (asterisk) compared to CSF and normal facet joints. (2F) Axial T1-weighted image obtained after intravenous contrast administration demonstrates a thin layer of peripheral enhancement surrounding the cyst (arrow) but no internal enhancement other than the thin septation.
Diagnosis
L5-S1 discal cyst displacing the left S1 nerve root.
Introduction
Discal cysts are relatively rare ventral epidural cystic lesions that may closely mimic lumbar disc herniation clinically and radiologically. Many patients present with radicular symptoms from focal ventral or anterolateral epidural mass effect, often with relatively limited adjacent disc degeneration. Because their appearance overlaps with more common causes of radiculopathy, prospective diagnosis depends on careful analysis of the MRI location and morphology.1,2,3,4
Recognizing a reproducible MRI pattern – a sharply-marginated, ventrolateral epidural cyst closely related to the posterior annulus and traversing nerve root – is key to the correct diagnosis. Careful attention to lesion origin, epidural compartment anatomy, and axial image morphology often narrows the differential diagnosis.1,3,5
A discal cyst is an extradural spinal canal cyst with demonstrable or presumed continuity with the adjacent intervertebral disc. Histologically, reported lesions typically have a fibrous connective tissue wall, without an epithelial or synovial lining, supporting a pseudocyst.1,2,4,6 The pathogenesis remains uncertain. The favored model is annular disruption resulting in an annular fissure, with fluid leakage from the disc and reactive pseudomembrane formation; impaired resorption of an epidural hematoma has also been proposed, particularly for hemorrhagic lesions.1,2,4,7
On MRI, the defining characteristics are ventral or ventrolateral epidural location, close association with the posterior disc margin, and signal characteristics indicating a cystic rather than solid lesion; communication with the adjacent disc may be demonstrated on discography or CT discography.1,2,8
Clinical Presentation
Symptomatic lesions most often present with unilateral radicular pain from compression of the traversing nerve root, usually within the lateral recess. Low back pain is common and can accompany or precede radicular symptoms. Neurologic findings are variable, and may include sensory disturbance, motor weakness, reflex asymmetry, and a positive straight-leg-raise test.2-5
Most lesions occur in the lower lumbar spine, particularly at L4-L5 and L5-S1. Early literature emphasized a predominance in young Asian men, whereas contemporary series demonstrate a broader demographic distribution, including older patients and women.4,5
The clinical presentation often resembles focal disc extrusion, emphasizing the importance of MRI localization and morphology.2-5
MR Imaging
MRI is the chief imaging modality for diagnosis (Figure 3) and distinguishing discal cysts from other cystic epidural lesions. Classically, discal cysts are centered along the posterior disc margin, extending into the ventral or anterolateral epidural space, and often into the subarticular zone. On axial imaging, a disc-adjacent anterolateral cyst may focally displace the traversing nerve root dorsally or dorsolaterally, while remaining separate from the facet joint.1,3,5

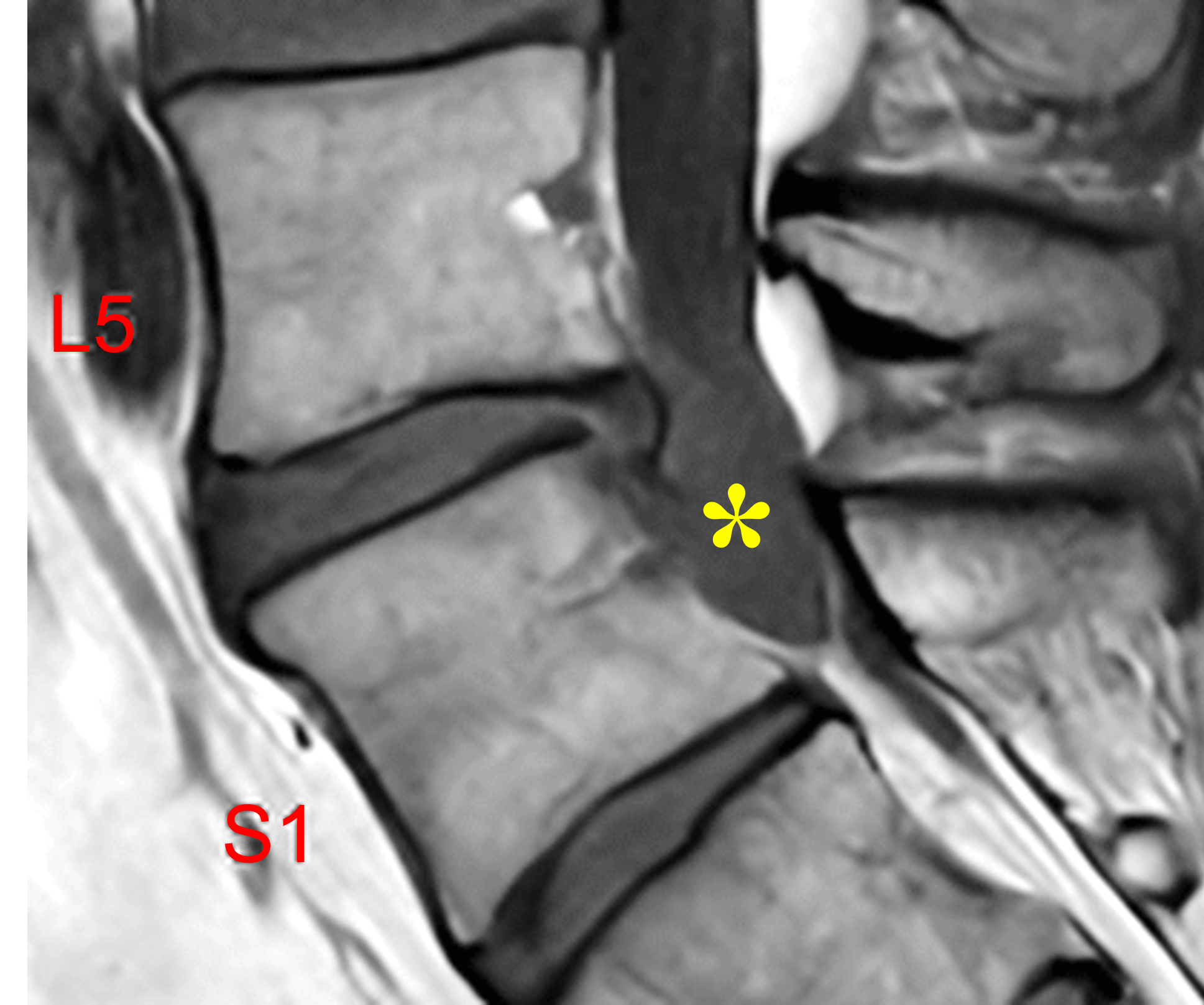
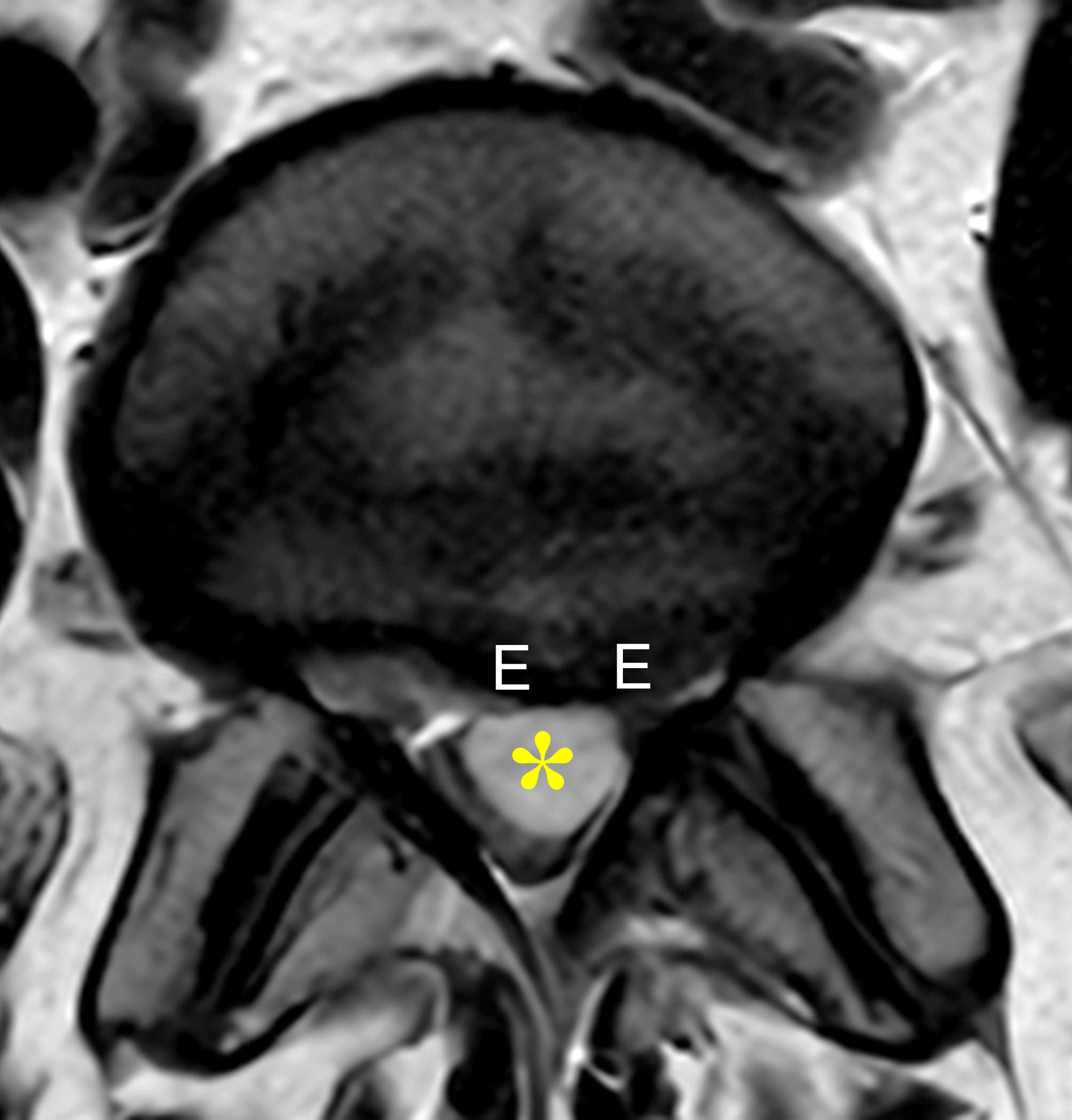

Figure 3: L5-S1 discal cyst in a 43-year-old man with low back pain for 2 years, with bilateral leg pain and numbness/tingling; no prior surgery. (3A) Sagittal T2-weighted image shows mild height loss of the L5-S1 disc, with an inferiorly directed, large, oval-shaped ventral epidural cyst (red arrows), containing heterogeneous central signal intensity slightly lower than CSF and a low-signal intensity rim, in association with an inferior disc extrusion (yellow arrow). (3B) Sagittal T1-weighted image shows the cyst (asterisk) with signal slightly hyperintense compared to CSF. (3C) Axial T2-weighted image demonstrates the ventral epidural cyst (asterisk) abutting the dorsal margin of the intervertebral disc, effacing the thecal sac and causing severe central stenosis with mass effect on the inferior nerve roots. The disc extrusion (E) and cyst result in severe left and moderate right lateral recess stenosis and encroachment of both traversing S1 nerve roots. The facet joints appear normal. (3D) Axial T1-weighted image confirms the lack of facet arthritis and redemonstrates the large discal cyst (asterisk) and disc extrusion (E).
The lesions are usually well-circumscribed with smooth margins and rounded or mildly lobulated morphology. Typical internal signal is homogeneous fluid-like, low-to-intermediate on T1-weighted images and hyperintense on T2-weighted images. A thin peripheral T2-hypointense rim may be present corresponding to the fibrous cyst wall. The presence of hemorrhagic or proteinaceous contents may produce internal complexity and increased signal on T1-weighted images, reducing specificity and increasing overlap with the appearance of sequestered disc material.1,3-5 A narrow communicating stalk may occasionally be visualized extending toward the disc space. On routine MRI, direct visualization of communication is inconsistent; its absence does not exclude the diagnosis.
When present, enhancement is classically thin and peripheral, without internal or nodular enhancement; the lack of rim enhancement does not exclude the diagnosis. Thick irregular enhancement or enhancing internal soft tissue should prompt reconsideration of the diagnosis.1,3,4
CT is less specific than MRI but may demonstrate a low-attenuation, disc-adjacent epidural lesion. In chronic cases, subtle remodeling or scalloping of the adjacent bone may be present; intralesional gas in association with a vacuum phenomenon in the adjacent disc has been reported but is an ancillary rather than definitive finding.1,5,8,9
Discography and CT discography can directly confirm disc communication but in current practice are generally reserved for equivocal cases or procedural planning. Following intradiscal contrast injection, opacification of the cyst through a communicating channel is considered diagnostic.1,2,8
Differential Diagnosis
A practical differential may be organized by lesion origin: disc-centered lesions, posterior element cysts, CSF-related cysts, hemorrhagic epidural collections, and post-operative cystic lesions.
A cyst in the posterolateral spinal canal, arising from or communicating with a degenerated facet joint, is most likely a synovial cyst (Figure 4). Large synovial cysts may extend medially into the spinal canal; tracing the lesion back to a facet joint is the most useful discriminator. Ganglion cysts resemble synovial cysts in location but lack a synovial lining and are usually centered near the facet joint, ligamentum flavum, or degenerative posterior soft tissues rather than the posterior annulus. A posterior element-centered origin favors ganglion or synovial cyst over discal cyst.1,4,5




Figure 4: Synovial cyst arising from the left L3-L4 facet joint in a 53-year-old woman with left-sided lower back pain radiating through the left side and down the back of her left leg. (4A) Sagittal T2-weighted image shows a dorsal epidural cyst at the L3-4 level, with a low signal intensity rim (arrow) that is slightly thicker compared with the previously shown discal cysts (Figures 2 and 3). (4B) Sagittal T1-weighted image demonstrates the cyst (asterisk) in the dorsal aspect of the spinal canal. (4C) Axial T2-weighted image confirms the dorsolateral location of the cyst, which arises adjacent to the degenerated left facet joint, which contains a trace joint effusion (white arrow). Note the encroachment on the traversing left L4 nerve root in the subarticular recess (yellow arrow). (4D) Axial T1-weighted image shows findings of osteoarthritis involving the facet joint (arrow).
Meningeal cysts and extradural arachnoid cysts also contain CSF-like signal intensity but are distinguished from discal cysts primarily by their characteristic anatomic distribution. Tarlov cysts are perineural (Type II meningeal) cysts that typically occur in the sacral canal, with the nerve roots in the cyst wall (Figure 5). Other perineural cysts present as dilated nerve root sleeves often with the intervertebral foramen (Figure 6). These cysts may demonstrate communication with the subarachnoid space and are frequently asymptomatic.1,4,8
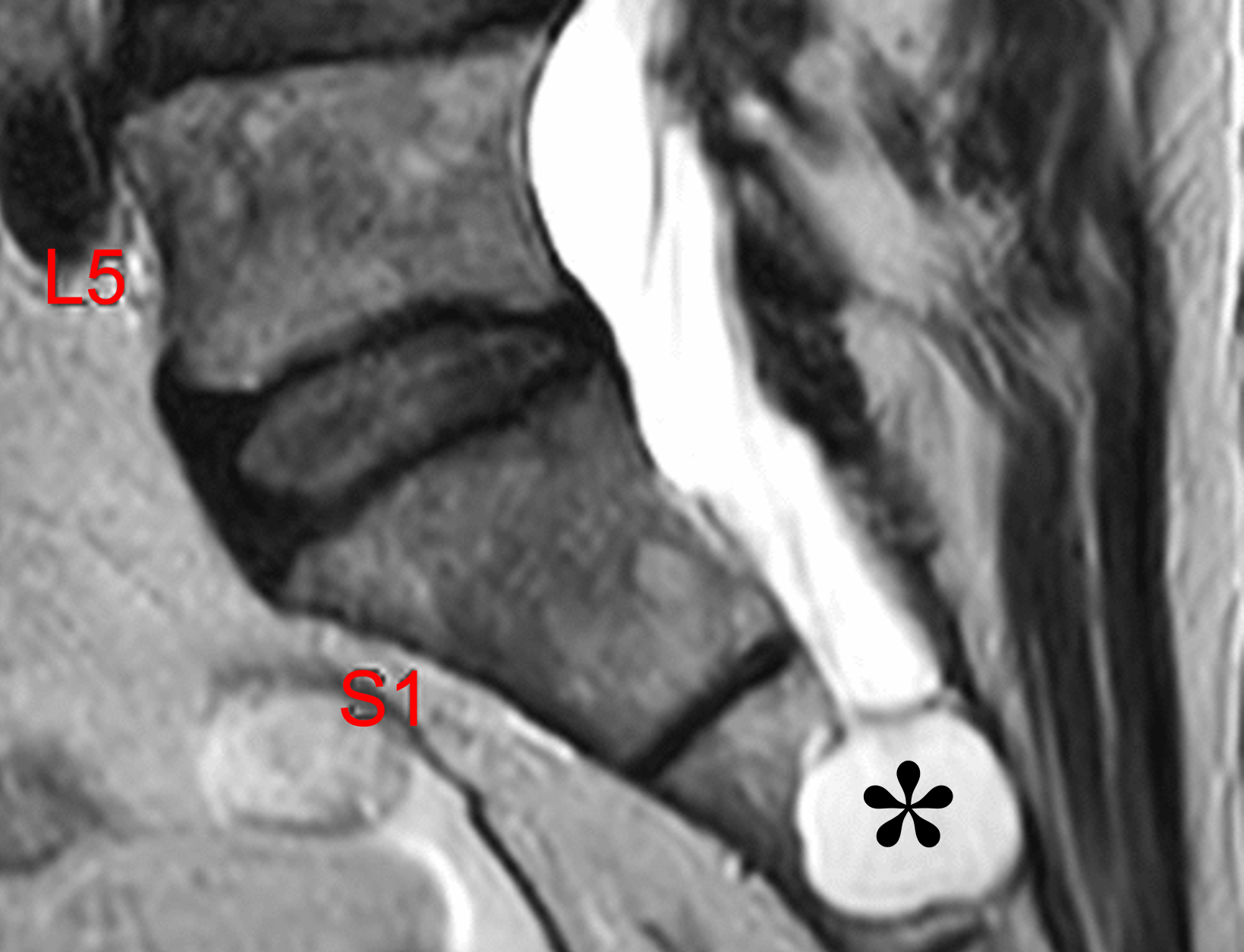
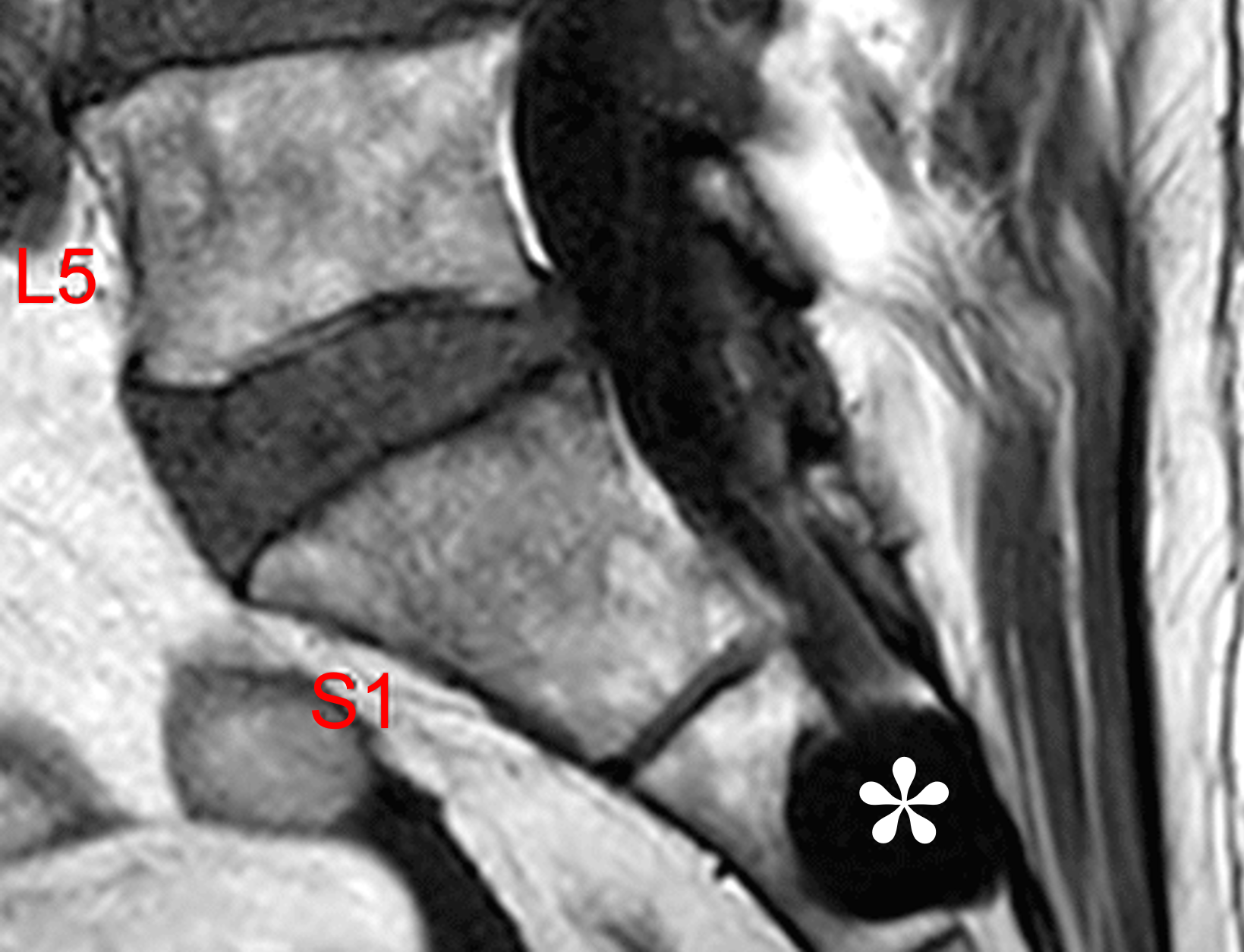
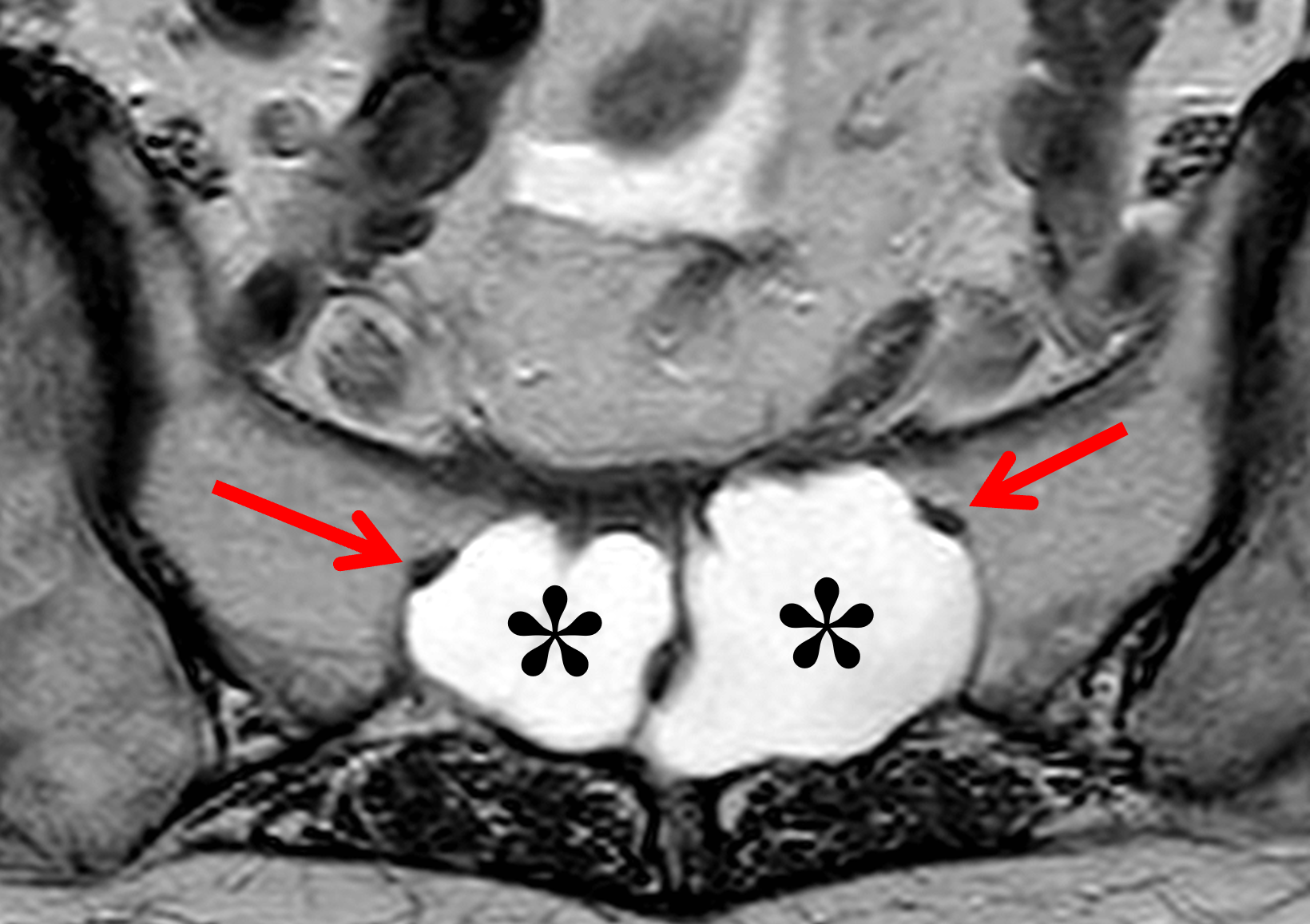
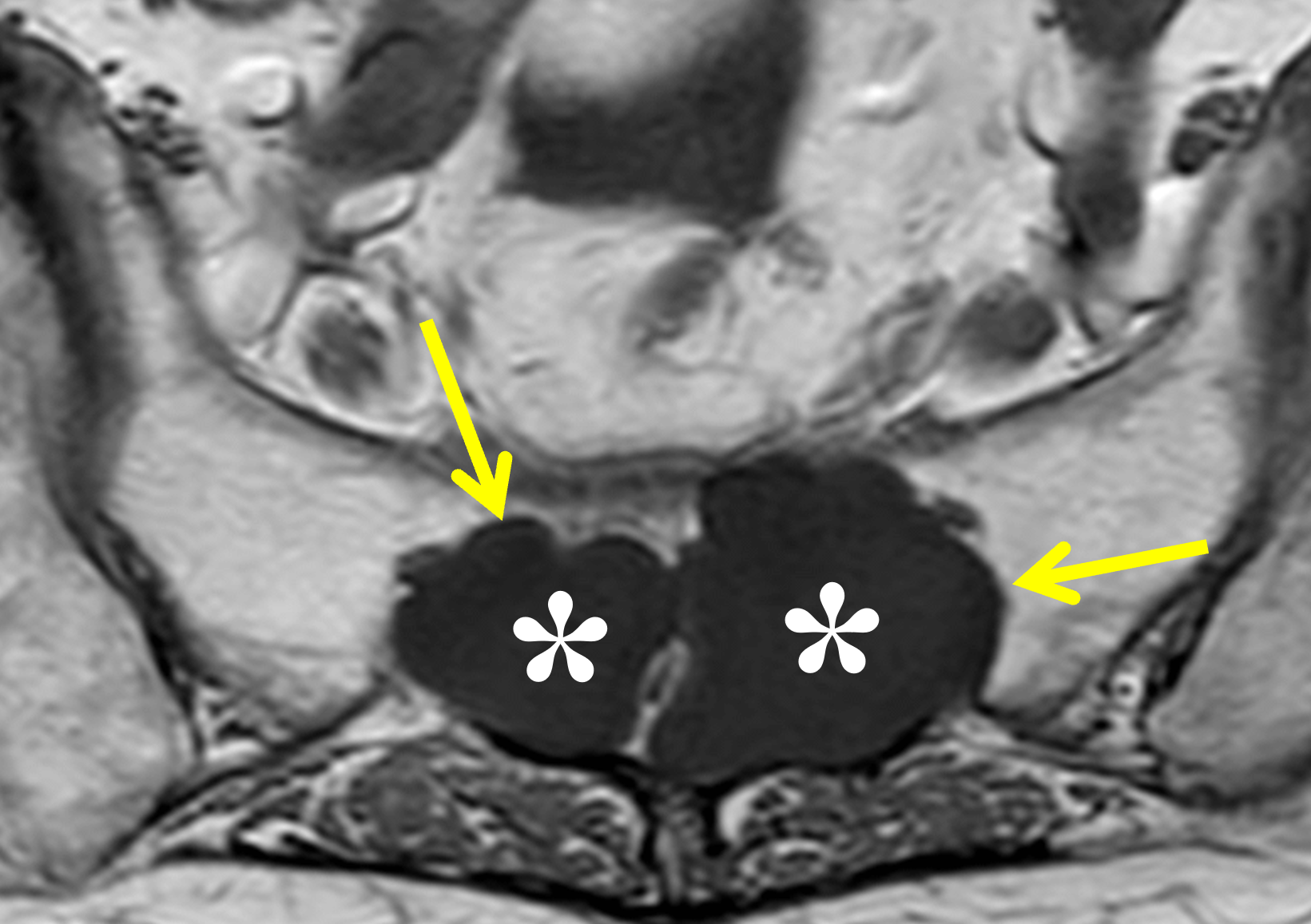
Figure 5: Sacral Tarlov cyst in an 81-year-old man with left lumbar radiculopathy and chronic pain. Sagittal (5A) T2-weighted and (5B) T1-weighted images demonstrate an intra-osseous cyst (asterisks) with contents isointense compared to CSF, centered at the S2 level remote from any intervertebral disc. (5C) Axial T2-weighted image shows bilateral cysts in the sacrum (asterisks). Note the S2 nerve roots in the cyst walls (arrows). (5D) Axial T1-weighted image shows the cysts (asterisks) producing pressure erosion with lobulated bone remodeling of the sacrum (arrows).


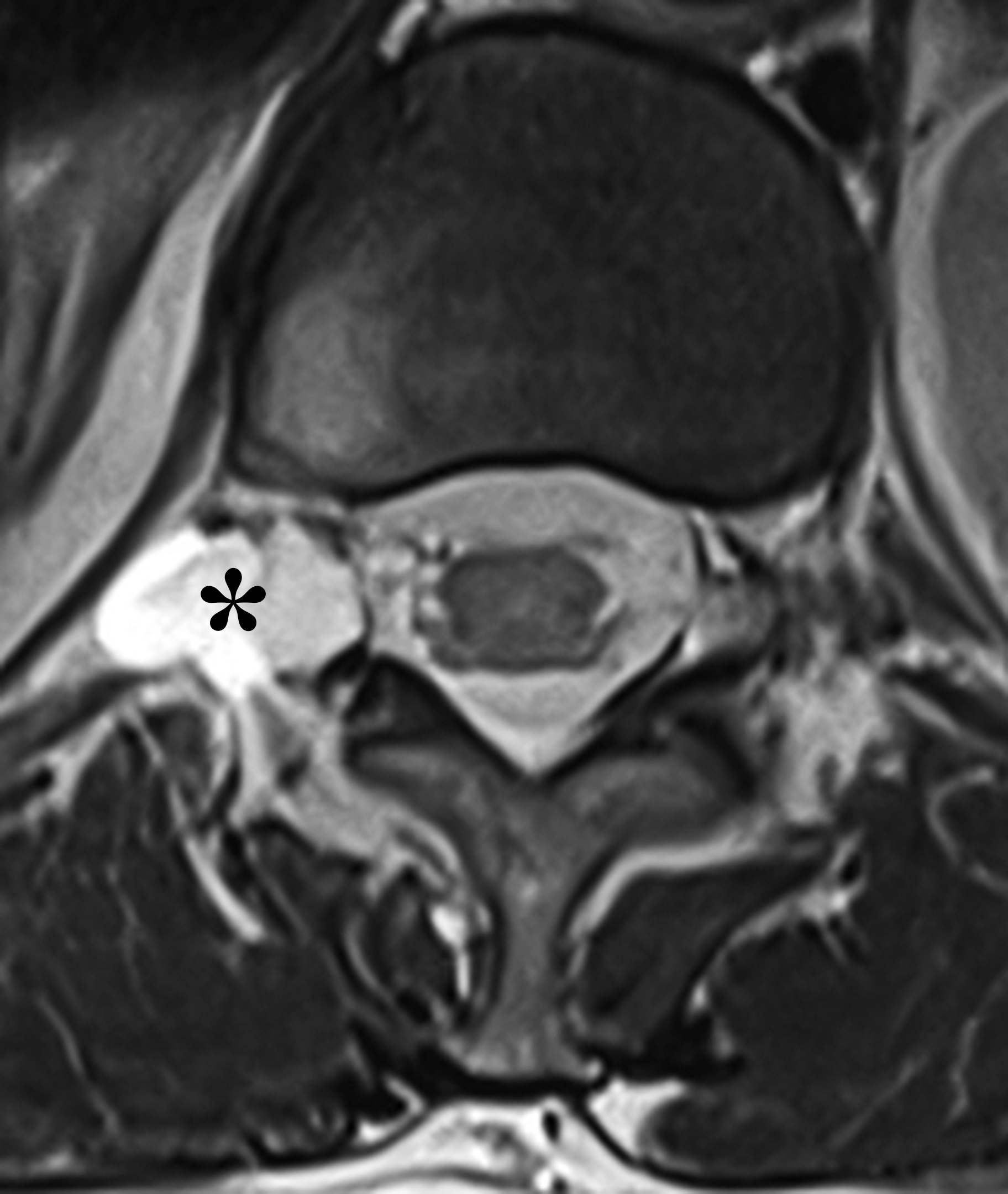

Figure 6: Right T12-L1 perineural cyst in a 74-year-old woman with low back/pelvic pain for several months. Sagittal (6A) T2-weighted and (6B) T1-weighted images demonstrate a cyst (asterisks) with signal intensity isointense to CSF, centered within the neural foramen at the T12-L1 level. A fat plane is maintained between the cyst and the intervertebral disc (arrows). Axial (6C) T2-weighted and (6D) T1-weighted images show a right-sided cyst (asterisks) extending along the exiting right T12 nerve root, centered within the neural foramen. The facet joints appear normal.
Extradural arachnoid cysts are usually dorsal or posterolateral lesions in the spinal canal, with signal intensity identical to CSF (Figure 7). These cysts are more common in the thoracic spine compared to the lumbar spine. Unlike discal cysts, arachnoid cysts do not demonstrate a disc-adjacent ventral epidural origin.1,4,10


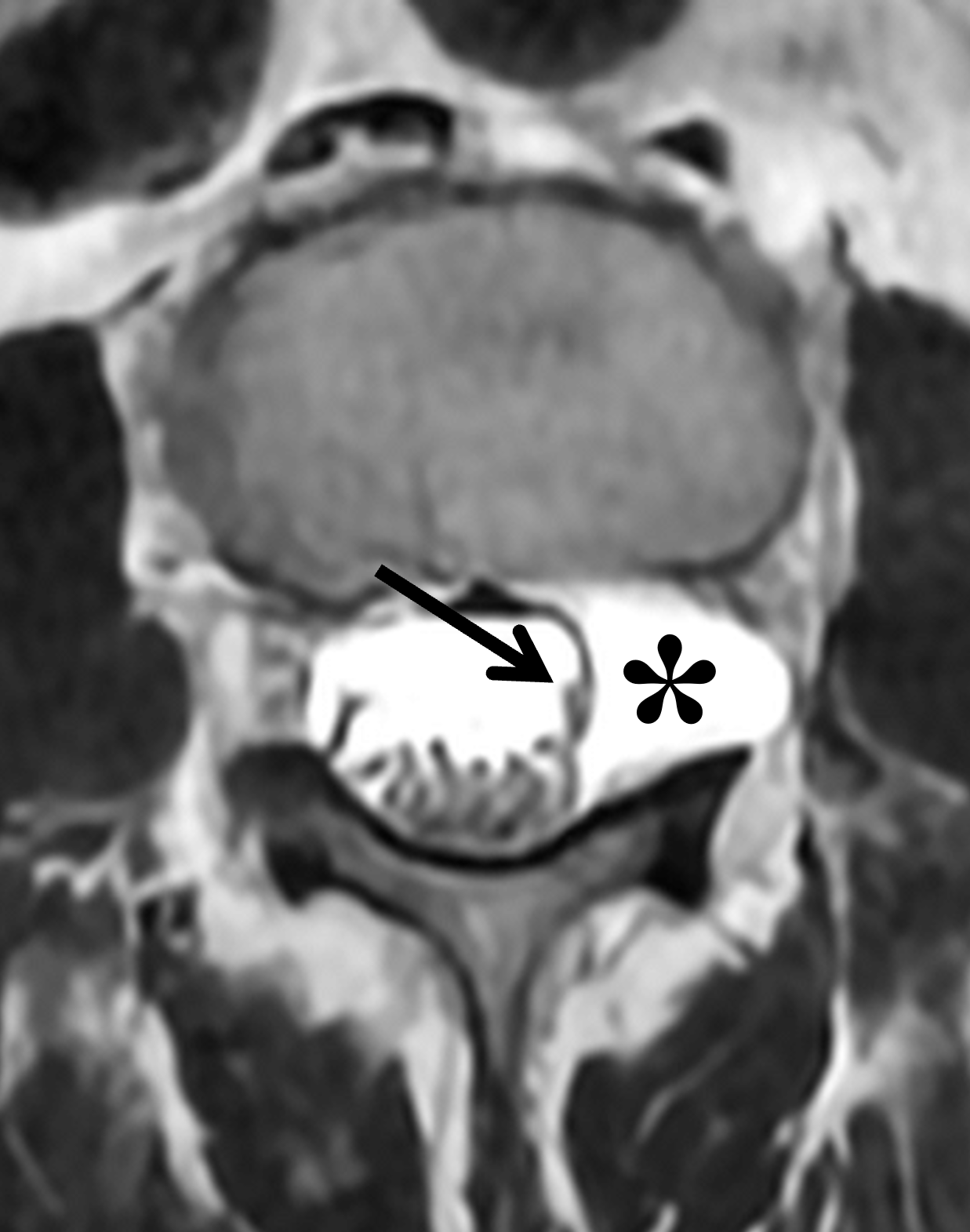
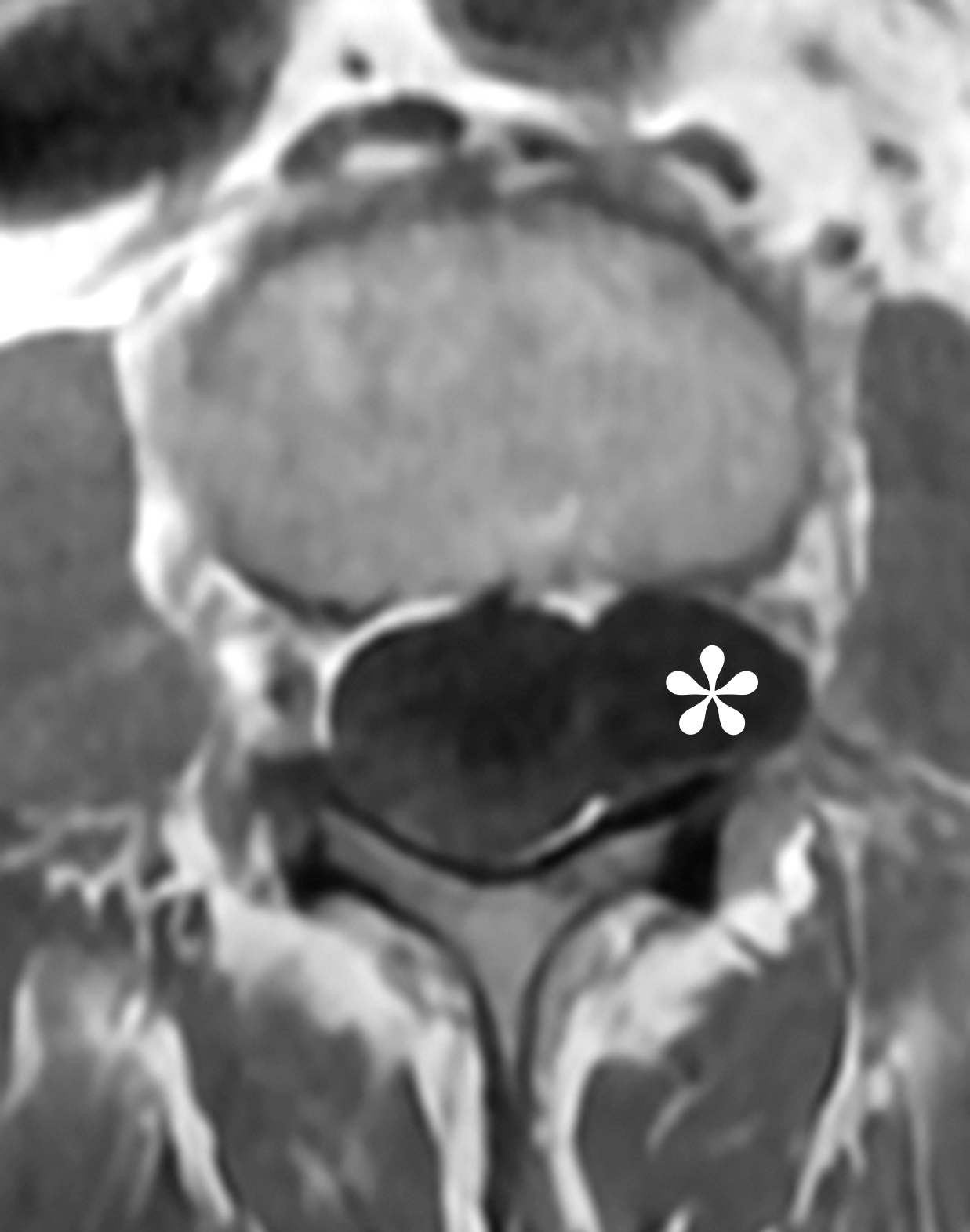
Figure 7: Extradural arachnoid cyst involving the upper lumbar in a 62-year-old woman with chronic achy lower back pain. Sagittal (7A) T2-weighted and (7B) T1-weighted images demonstrate an extra-thecal lobulated cyst (asterisks) centered within the lateral spinal canal at the L2 level, with signal intensity isointense compared to CSF. Note the adjacent smooth remodeling/scalloping of the posterior L2 vertebral body (arrows). The adjacent facet joints appear normal. Axial (7C) T2-weighted and (7D) T1-weighted images show the left-sided extradural cyst (asterisks) in the left lateral spinal canal, extending into the left neural foramen. The cyst produces mass effect on the thecal sac with medial displacement of the left nerve roots (arrow).
Similar to a discal cyst, a sequestered disc fragment also arises within the ventral epidural space and may demonstrate peripheral enhancement on MRI and radiculopathy clinically. Sequestered fragments typically retain disc-like soft tissue signal (Figure 8), irregular contours, and heterogeneous enhancement, in contrast to the sharply-marginated, uniform fluid-signal cavity and thin wall that characterize a discal cyst.1,3-5

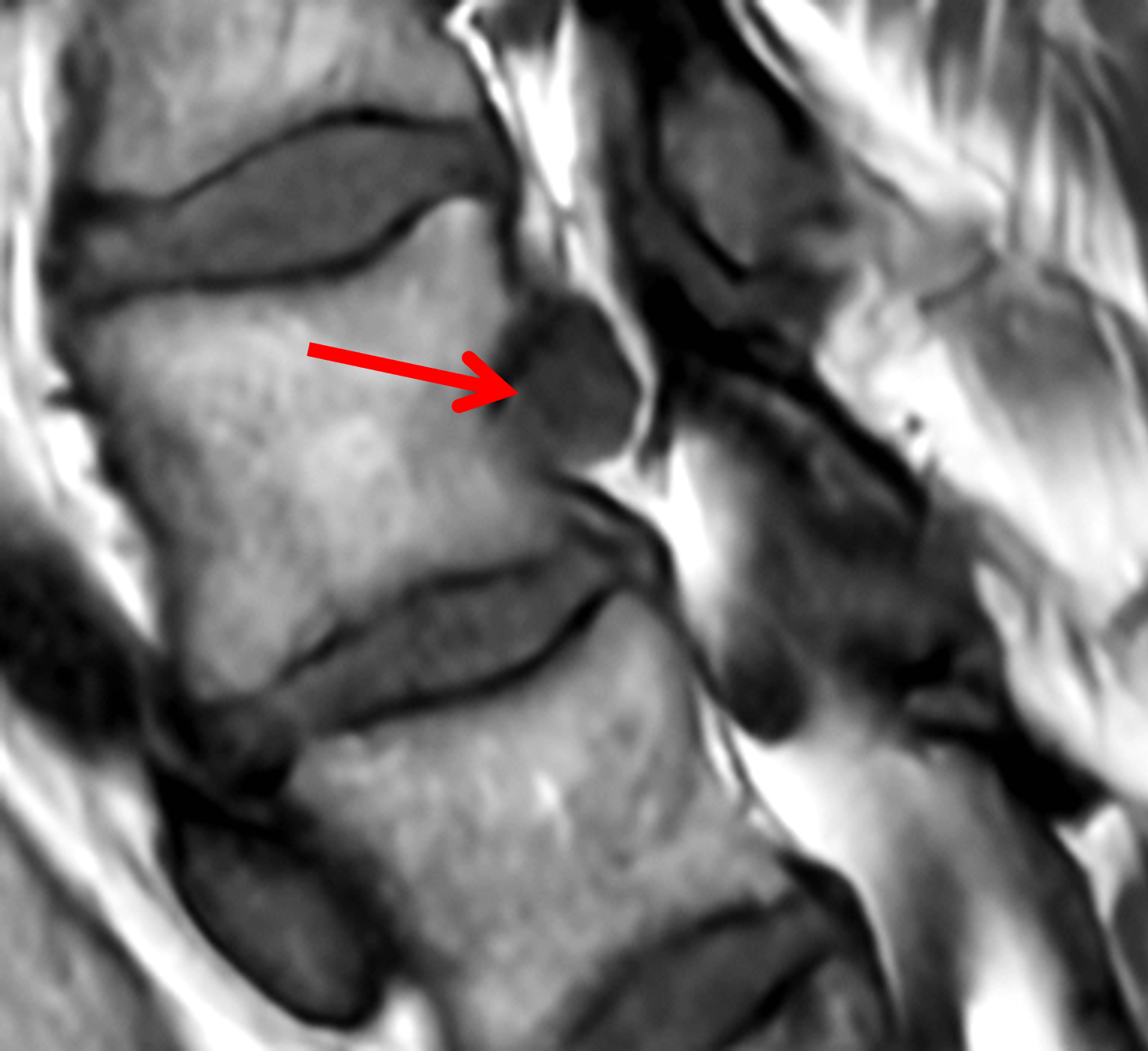

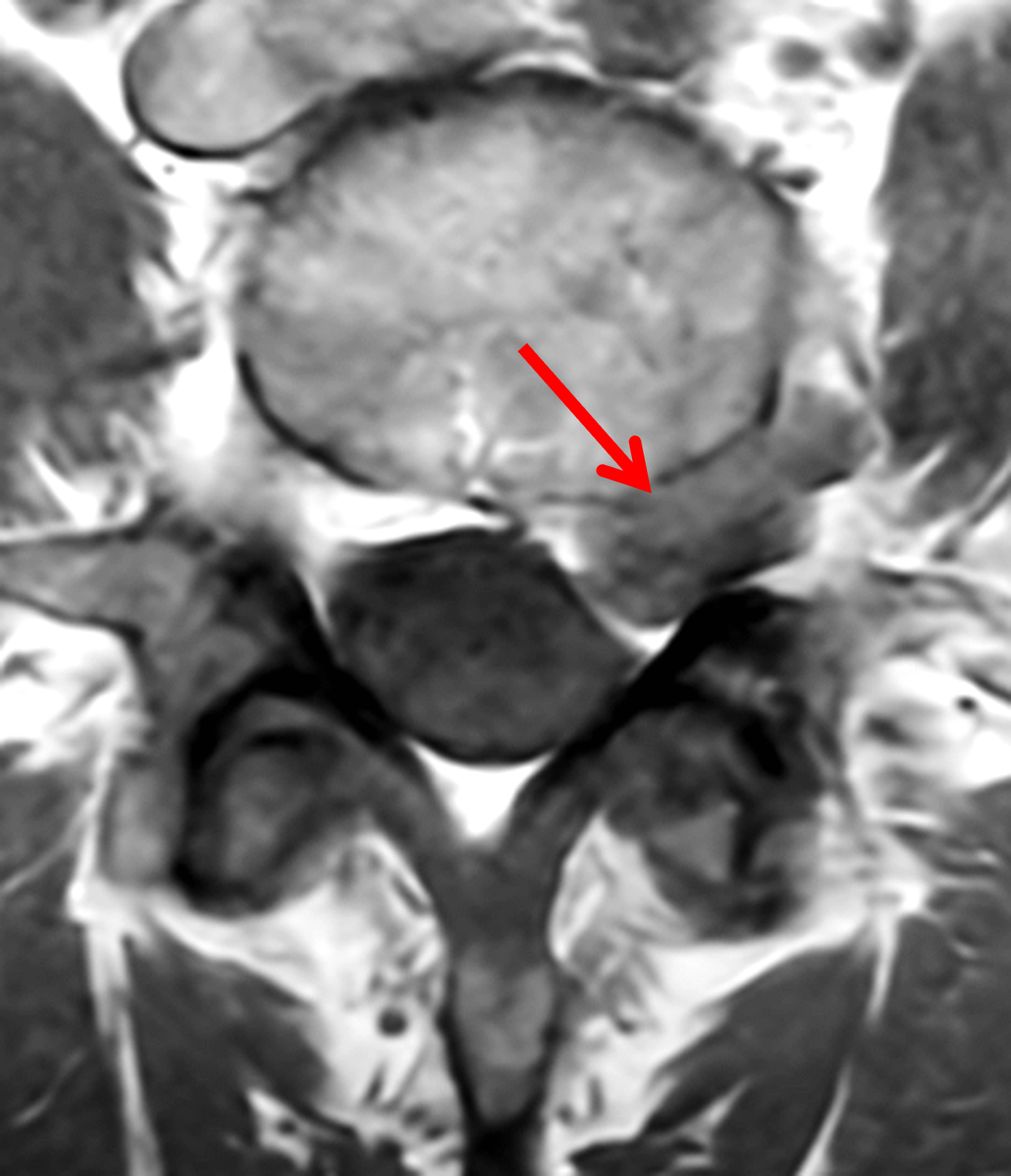
Figure 8: Sequestered disc fragment at the L4 level in a 56-year-old woman with sharp, stabbing, and aching pain localized to the lumbar spine and radiating down the anterolateral left thigh, as well as numbness & tingling in the left lower extremity. Sagittal (8A) T2-weighted and (8B) T1-weighted images demonstrate an ovoid mass with soft tissue signal intensity (arrows) in the ventral epidural space at the mid L4 vertebral body level, without a connection to an intervertebral disc. (8C) Axial T2-weighted image shows the disc fragment with signal less intense compared to CSF (red arrow). The fragment extends along the left ventral epidural space and superior aspect of the left L4-5 neural foramen, contacting the traversing left L5 nerve root (white arrow) and encroaching upon the extra-foraminal portion of the left L4 nerve root (yellow arrow). (8D) Axial T1-weighted image shows the disc fragment (arrow) with signal hyperintense compared to CSF. Mild facet osteoarthritis is present without a joint effusion.
A postoperative discal pseudocyst should be considered after discectomy when a rim-enhancing cystic lesion develops at the operative disc level. These may resemble a conventional discal cyst, but a history of disc surgery and adjacent granulation tissue are important clues; a demonstrable disc communication is not required for the diagnosis.5,8,11
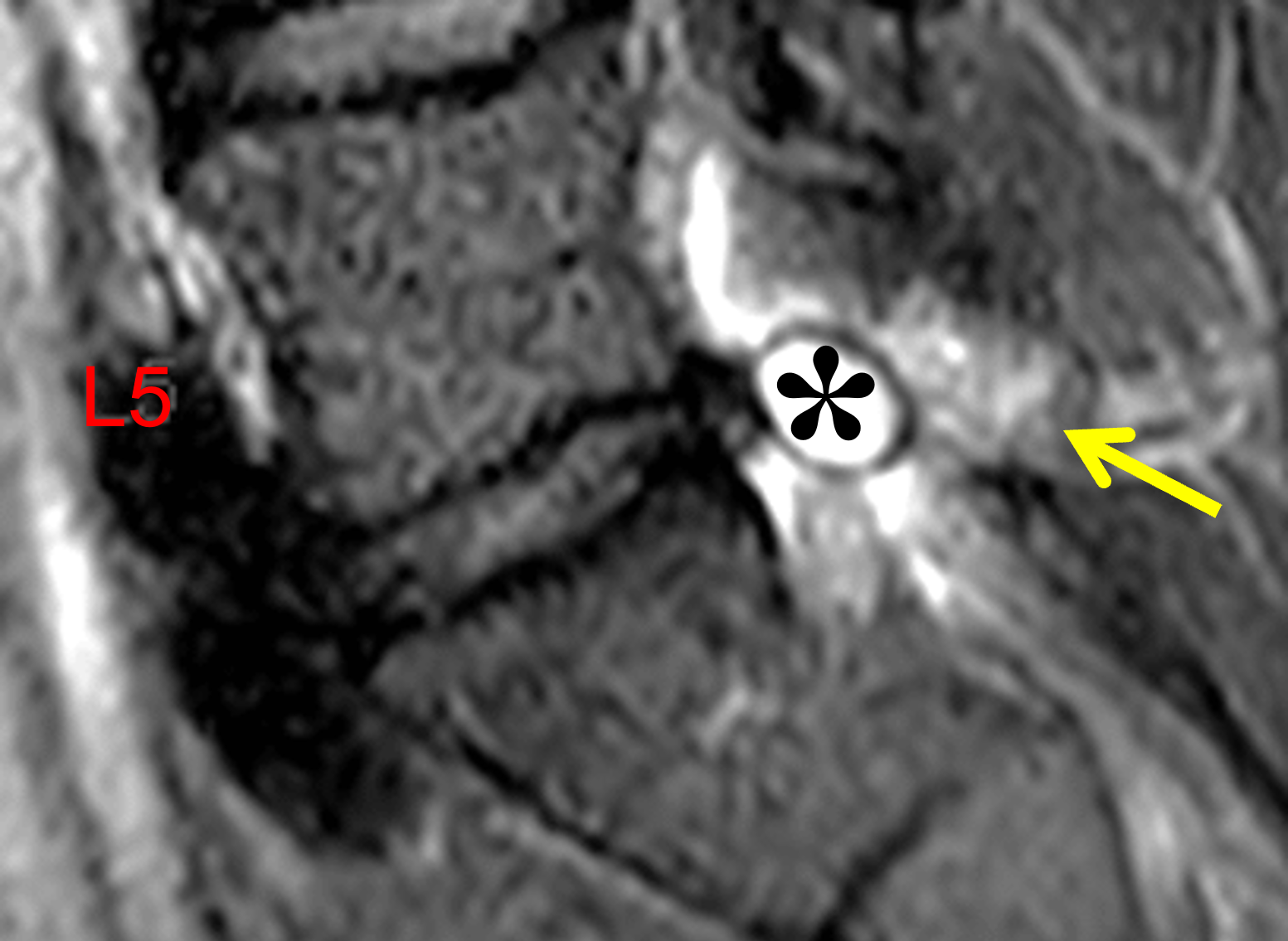
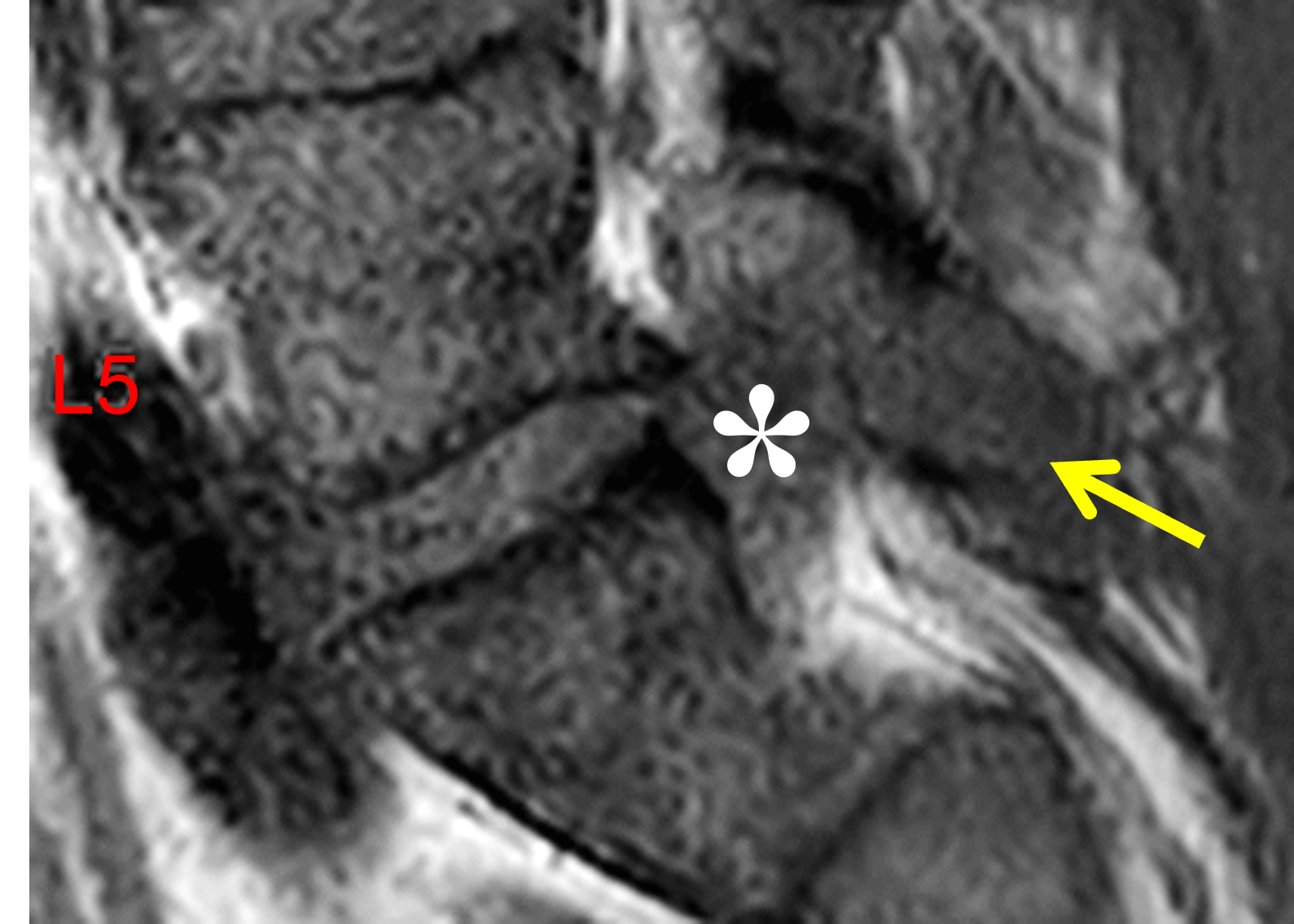
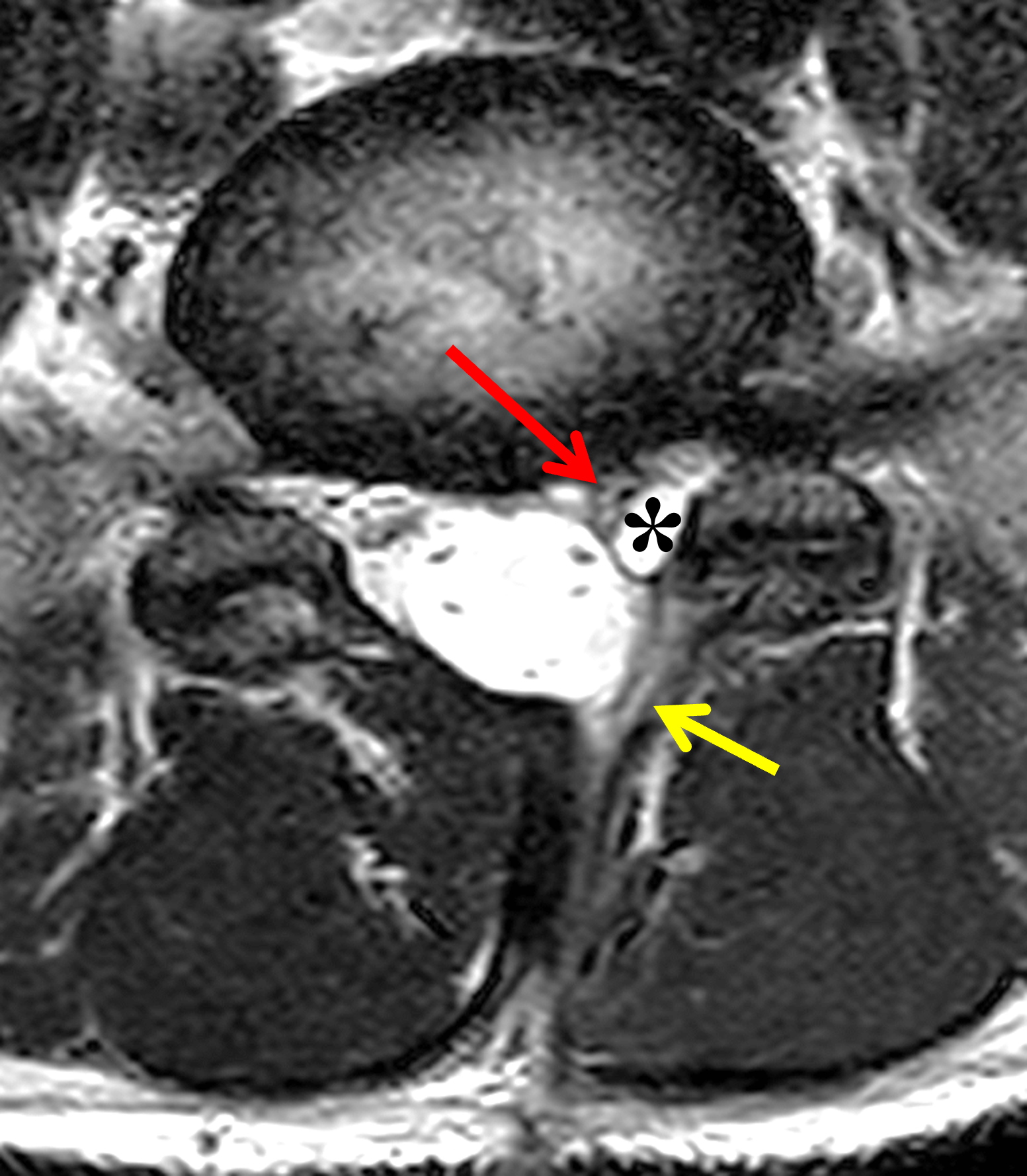
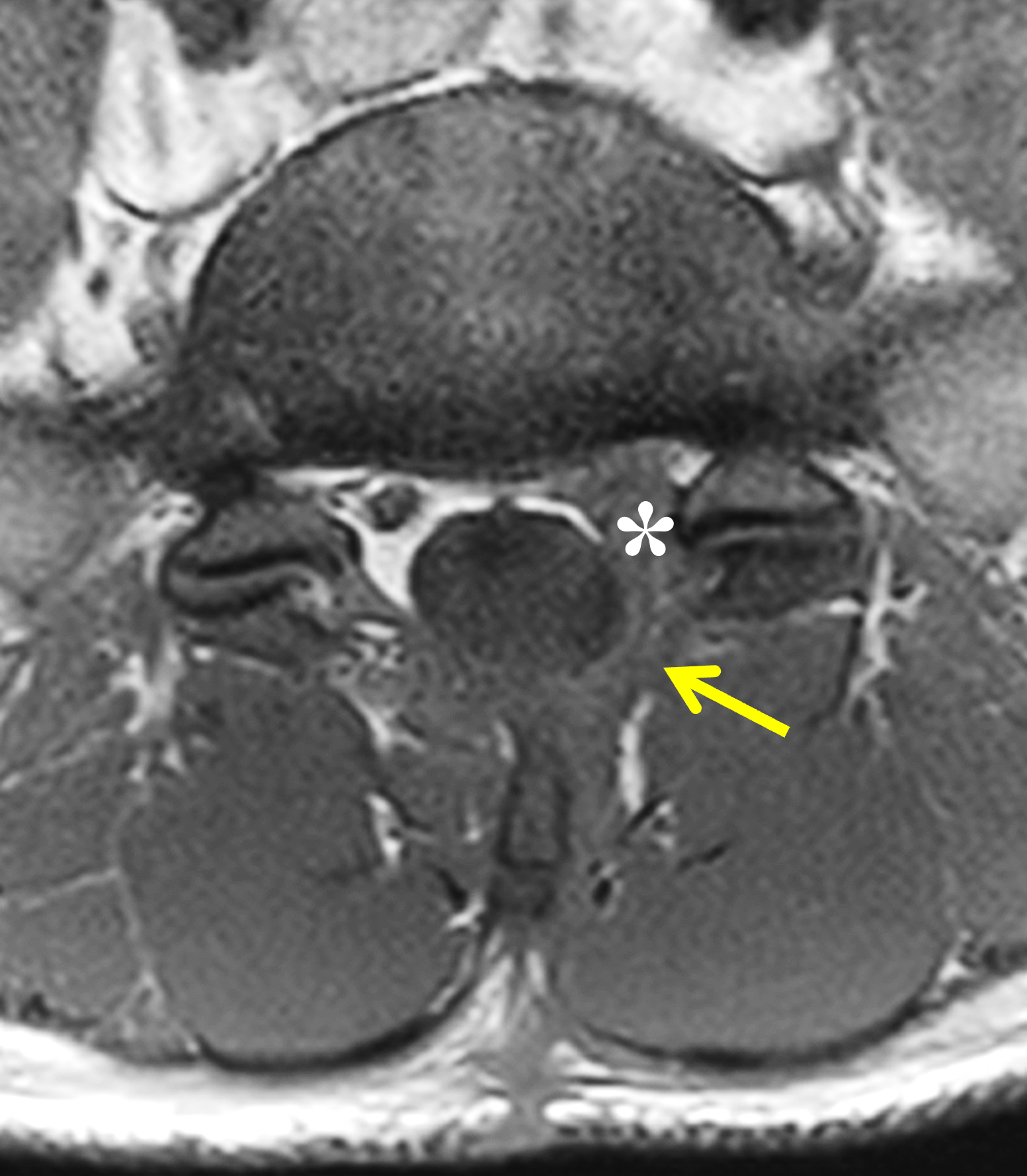
Figure 9: Post-operative discal pseudocyst in a 36-year-old man with low back and left lower extremity pain for 3 weeks. History of surgery three months ago. Sagittal (9A) T2-weighted and (9B) T1-weighted images demonstrate an oval-shaped ventral epidural cyst (asterisks) abutting the dorsal margin of the L5-S1 intervertebral disc, with central signal intensity isointense to CSF, and a low-signal intensity rim on the T2-weighted image. A laminectomy defect with granulation tissue is present posteriorly (arrows). (9C) Axial T2-weighted image shows the left-sided extradural cyst (asterisk) in the left anterolateral spinal canal encroaching upon the traversing left S1 nerve root (red arrow). A left laminectomy defect is present (yellow arow). (9D) Axial T1-weighted image redemonstrates the discal cyst (asterisk) and laminectomy defect (arrow). Mild left-sided facet degeneration is present without a facet joint effusion.
Epidural hematoma may enter the differential when a disc-adjacent epidural lesion has hemorrhagic or T1-hyperintense contents (Figure 10). Hematoma is favored by acute clinical context, expected blood-product signal evolution, broad or multilevel epidural extent, and absence of disc communication on discography.4,5,8

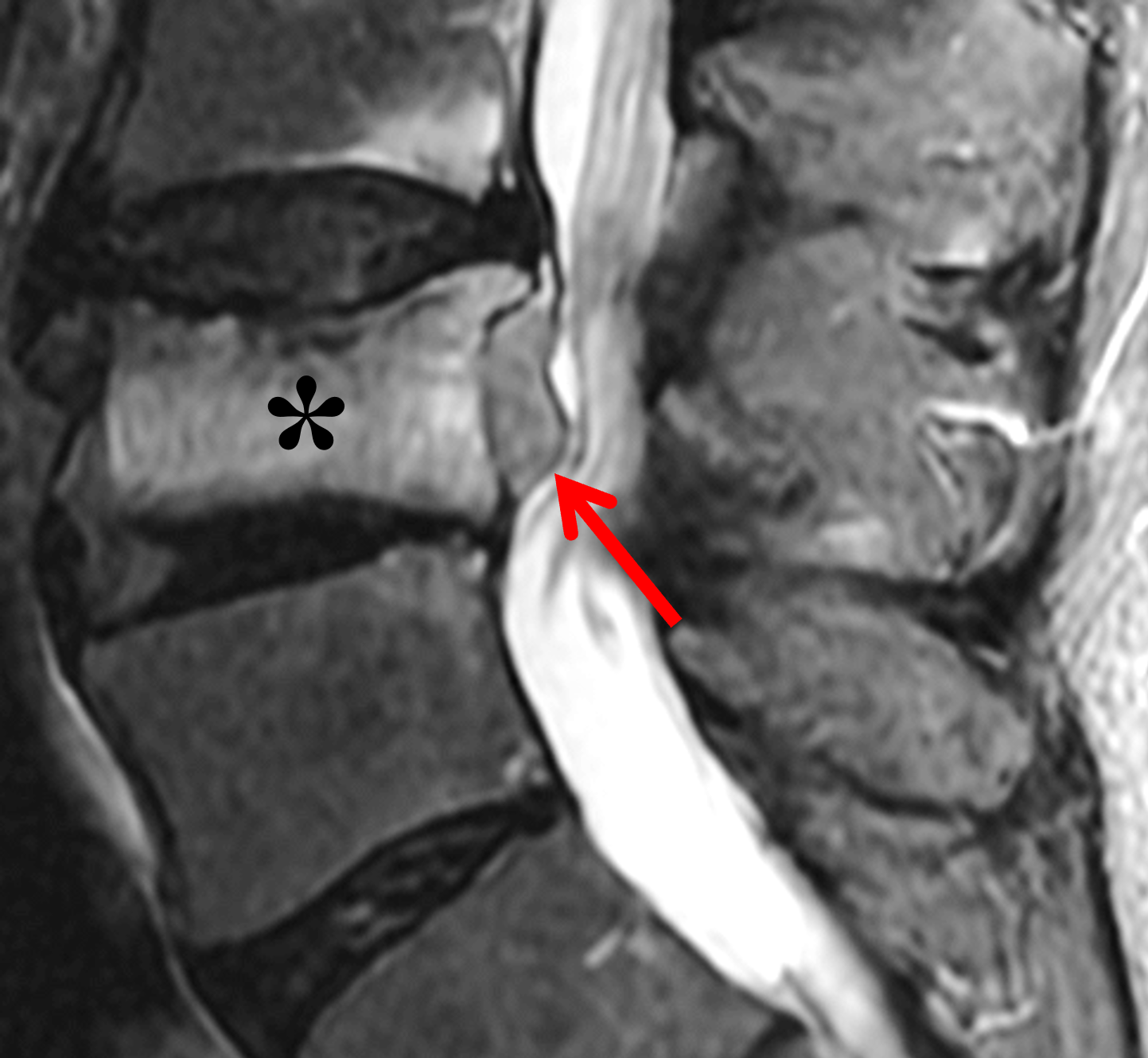
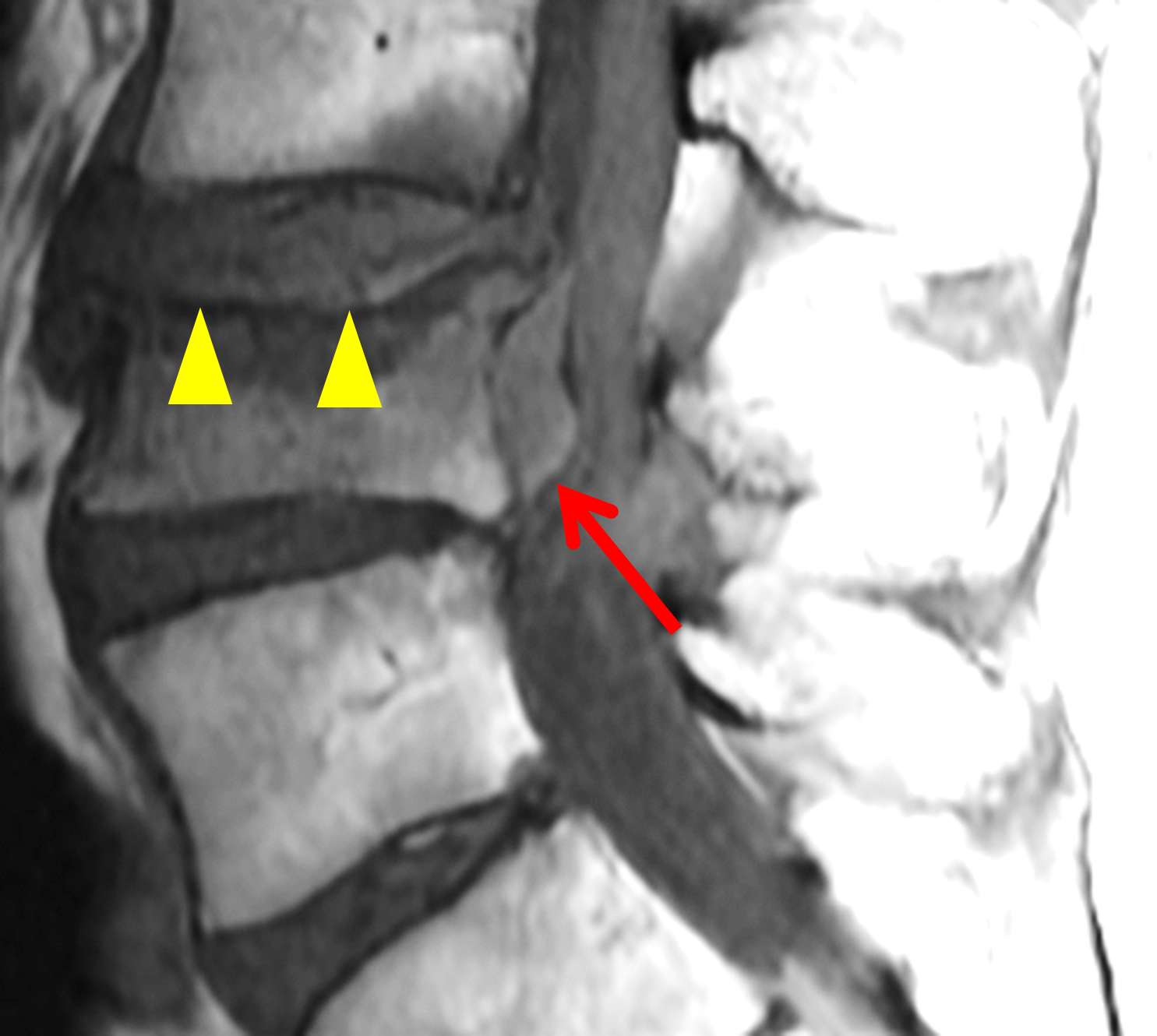
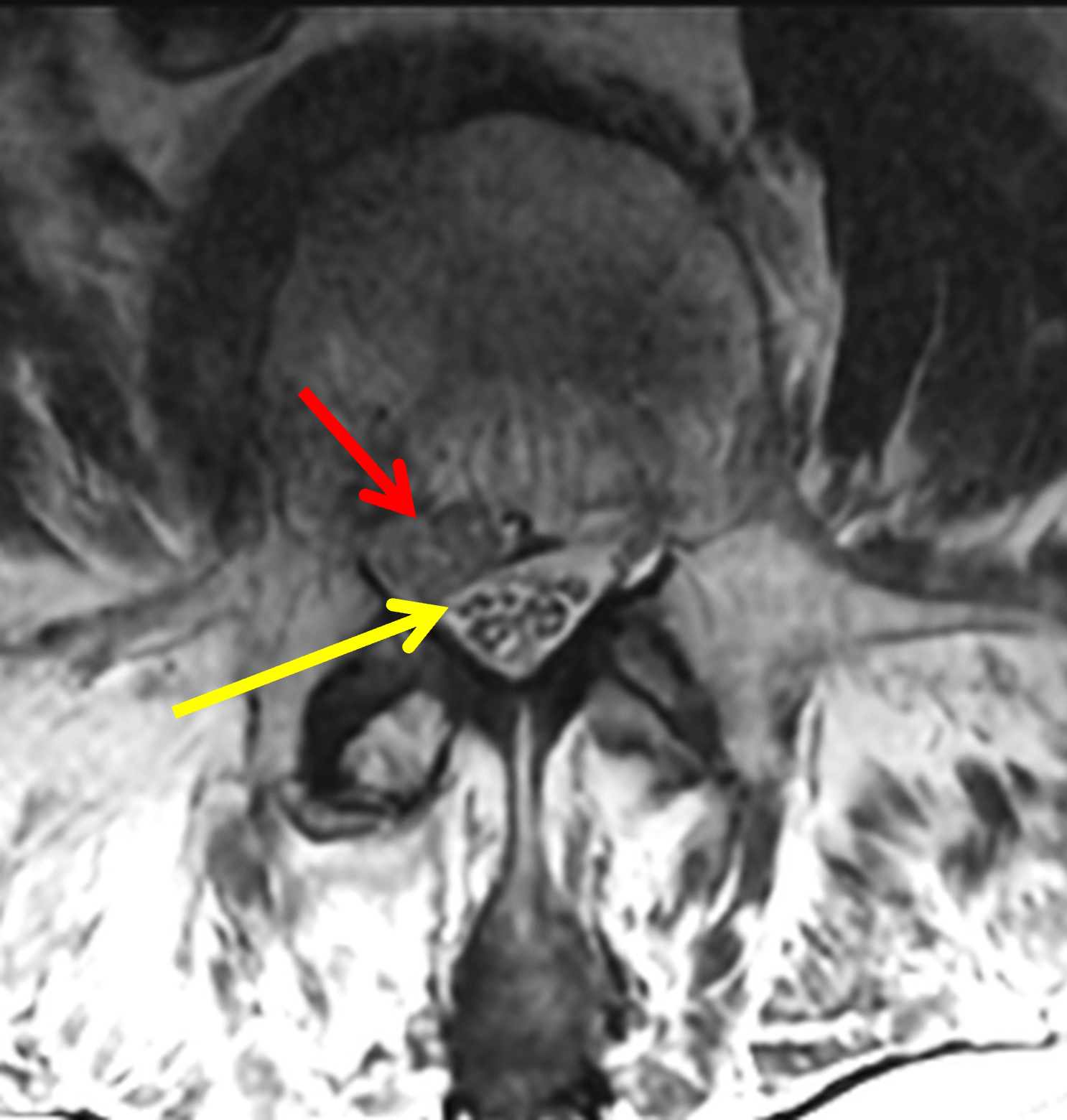
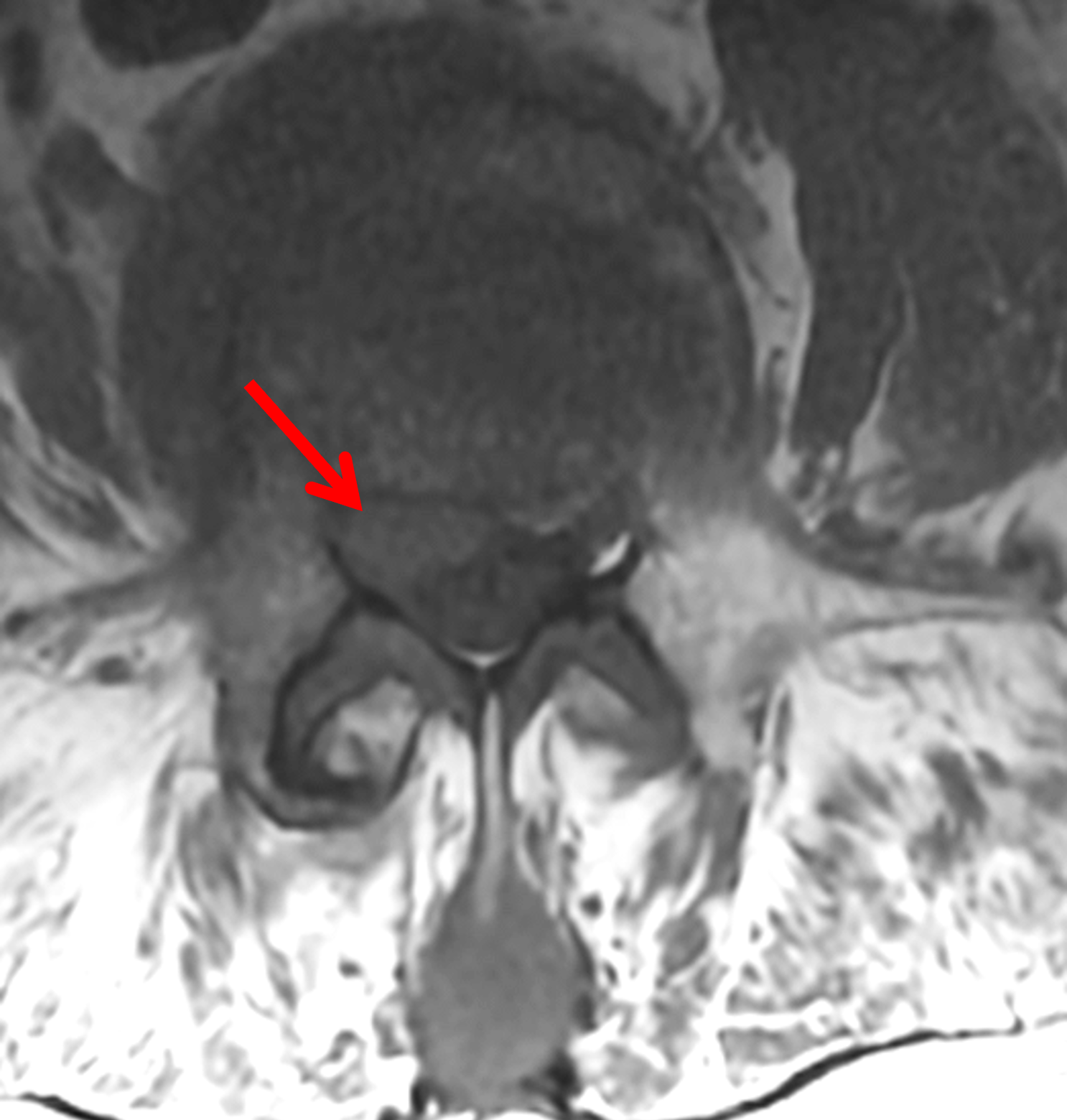
Figure 10: Epidural hematoma in an 87-year-old man with low back pain and compression fracture. (10A) Sagittal T2-weighted image shows an L4 superior endplate compression fracture (arrowheads) with mild retropulsion of the posterosuperior endplate, and an epidural soft tissue mass along the posterior vertebral body (arrow). (10B) Sagittal STIR image shows marrow edema in the vertebral body (asterisk) and the lobulated epidural mass (arrow), which is hyperintense, but not as bright as CSF. (10C) Sagittal T1-weighted image shows the compression fracture (arrowheads) and hyperintense signal in the epidural mass (arrow) representing subacute blood products. (10D) Axial T2-weighted image shows the hematoma in right lateral ventral epidural space (red arrow), effacing the thecal sac and posteriorly displacing the traversing right L4 nerve root (yellow arrow). (10E) Axial T1-weighted image demonstrates signal mildly hyperintense compared to skeletal muscle within the subacute hematoma (arrow).
A spinal epidural abscess may occasionally mimic a discal cyst when a ventral epidural collection demonstrates fluid signal intensity and peripheral enhancement. Unlike discal cysts, however, epidural abscesses typically occur in the setting of systemic inflammatory symptoms, elevated inflammatory markers, recent infection, bacteremia, or spinal intervention. On MRI, a spinal epidural abscess more often demonstrates thick or irregular peripheral enhancement, surrounding inflammatory change, adjacent spondylodiscitis, or vertebral marrow edema, and can have more extensive epidural spread rather than a sharply marginated focal ventrolateral cyst adjacent to the posterior annulus (Figure 11). Central restricted diffusion and accompanying paraspinal abscesses or phlegmonous soft-tissue abnormality further favor abscess over a localized disc-related cystic lesion.1,3,4
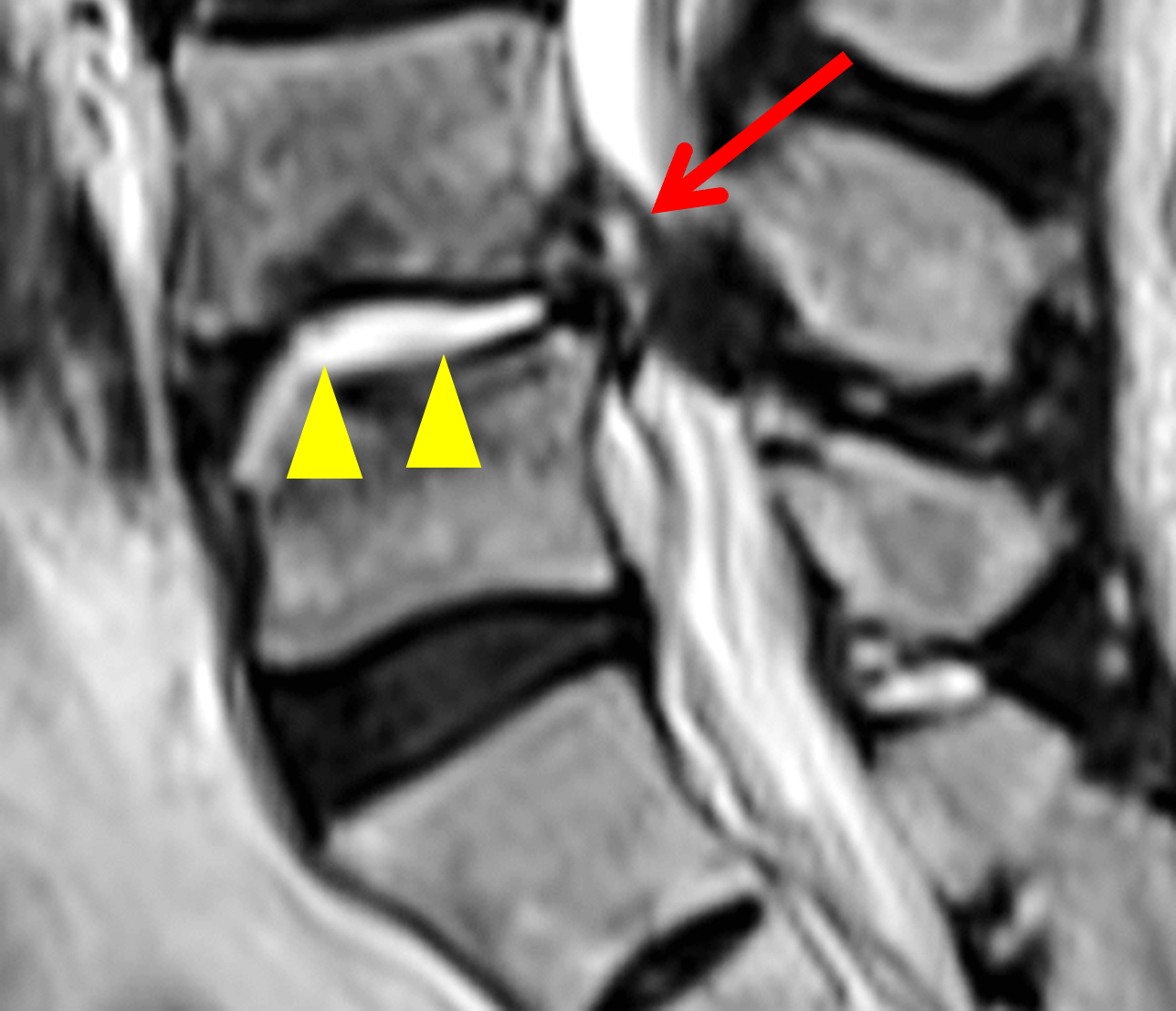




Figure 11: Spinal epidural abscess related to discitis/osteomyelitis in a 95-year-old man with chronic right low back and hip pain and that radiates down the leg, and intermittent leg numbness. (11A) Sagittal T2-weighted image shows fluid-intensity signal within the L4-5 intervertebral disc (arrowheads) and an adjacent heterogeneous ventral epidural fluid collection representing an abscess (arrow). Severe central canal stenosis is present. (11B) Sagittal STIR image demonstrates the epidural abscess (arrow) and extensive marrow edema (asterisks) in the vertebral bodies. (11C) Sagittal T1-weighted image shows destruction of the superior L5 endplate (yellow arrow) and mild epidural fat stranding (white arrow) superior to the abscess. Axial (11D) T2-weighted and (11E) T1-weighted images show the small ventral epidural fluid collection (arrows) indenting the ventral thecal sac and contributing to severe central stenosis in combination with facet arthrosis and ligamentum flavum hypertrophy.
Treatment
In patients without progressive neurologic deficit, initial management of a discal cyst may be conservative and similar to that of disc herniation, including analgesics, anti-inflammatory therapy, selective nerve root block, or epidural steroid injection. Because symptoms are frequently driven by focal lateral recess compression, imaging findings play an important role in determining candidacy for intervention.4,5,10
CT-guided aspiration and fenestration are minimally invasive treatment options that may be used in selected patients. Imaging is central to these procedures because safe access requires careful delineation of the relationship between the cyst, dura, and traversing nerve root. Post-discography CT may be particularly useful for procedural planning.5,7,8,10
In the absence of standardized guidelines, surgical resection remains the most definitive option for persistent radiculopathy, progressive neurologic deficit, or recurrence after nonsurgical treatment.4-6,11,12
Conclusion
Discal cysts are distinctive ventral epidural disc-related cystic lesions that most commonly occur within the lateral recess of the lower lumbar spine. Although reportedly uncommon, they often demonstrate a recognizable MRI pattern: a sharply marginated disc-adjacent ventrolateral epidural cyst with central T2 hyperintensity, often with thin rim enhancement and displacement of the traversing nerve root(s).1,3,5
Recognition depends primarily on anatomy-based MRI interpretation rather than direct visualization of disc communication. Careful evaluation of lesion origin – disc-centered versus posterior element-centered – narrows the differential diagnosis and helps separate the diagnosis of a discal cyst from entities like synovial cyst, ganglion cyst, or arachnoid cyst. Analysis of the lesion signal intensity, enhancement pattern, and associated disc or vertebral pathology helps distinguish discal cysts from sequestered disc fragments, hematomas, and abscesses.1,3,5
References
- Kono K, Nakamura H, Inoue Y, Okamura T, Shakudo M, Yamada R. Intraspinal extradural cysts communicating with adjacent herniated disks: imaging characteristics and possible pathogenesis. AJNR Am J Neuroradiol. 1999;20(7):1373–1377. ↩
- Chiba K, Toyama Y, Matsumoto M, Maruiwa H, Watanabe M, Nishizawa T. Intraspinal cyst communicating with the intervertebral disc in the lumbar spine: discal cyst. Spine (Phila Pa 1976). 2001;26(19):2112–2118. doi:10.1097/00007632-200110010-00014 ↩
- Lee HK, Lee DH, Choi CG, Kim SJ, Suh DC, Kahng SK, et al. Discal cyst of the lumbar spine: MR imaging features. Clin Imaging. 2006;30(5):326–330. doi:10.1016/j.clinimag.2006.05.026 ↩
- Aydin S, Abuzayed B, Yildirim H, Bozkus H, Vural M. Discal cysts of the lumbar spine: report of five cases and review of the literature. Eur Spine J. 2010;19(10):1621–1626. doi:10.1007/s00586-010-1395-9 ↩
- Gorolay VV, Fields BKK, Shah VN. Discal cysts and pseudocysts: Single center experience. Interv Pain Med. 2023;2(3):100278. doi:10.1016/j.inpm.2023.100278 ↩
- Hwang JH, Park IS, Kang DH, Jung JM. Discal cyst of the lumbar spine. J Korean Neurosurg Soc. 2008;44(4):262–264. doi:10.3340/jkns.2008.44.4.262 ↩
- Kang H, Liu WC, Lee SH, Paeng SS. Midterm results of percutaneous CT-guided aspiration of symptomatic lumbar discal cysts. AJR Am J Roentgenol. 2008;190(5):W310–314. doi:10.2214/AJR.07.2195 ↩
- Endo Y, Miller TT, Saboeiro GR, Cooke PM. Lumbar discal cyst: Diagnostic discography followed by therapeutic computed tomography-guided aspiration and injection. J Radiol Case Rep. 2014;8(12):35–40. doi:10.3941/jrcr.v8i12.2087 ↩
- Perillo T, Vitiello A, Perrotta M, Serino A, Manto A. Discal cyst: a rare cause of low back pain and sciatica. Radiol Case Rep. 2022;17(10):3678–3680. doi:10.1016/j.radcr.2022.07.018 ↩
- Yu HJ, Park CJ, Yim KH. Successful Treatment of a Symptomatic Discal Cyst by Percutaneous C-arm Guided Aspiration. Korean J Pain. 2016;29(2):129–135. doi:10.3344/kjp.2016.29.2.129 ↩
- Nabeta M, Yoshimoto H, Sato S, Hyakumachi T, Yanagibashi Y, Masuda T. Discal cysts of the lumbar spine. Report of five cases. J Neurosurg Spine. 2007;6(1):85–89. doi:10.3171/spi.2007.6.1.17 ↩
- Park JW, Lee BJ, Jeon SR, Rhim SC, Park JH, Roh SW. Surgical Treatment of Lumbar Spinal Discal Cyst: Is It Enough to Remove the Cyst Only without Following Discectomy? Neurol Med Chir (Tokyo). 2019;59(6):204–212. doi:10.2176/nmc.oa.2018-0219 ↩
