
Clinical History:
A 26 year-old football player presents with severe anterior chest pain following a tackling injury. MRI of the sternum was performed. A (1A) fat-suppressed T2-weighted coronal image and (1B,C) fat-suppressed proton density-weighted axial images are provided. What are the findings? What is your diagnosis?

1a

1b

1c
Figure 1
Findings:

2a

2b

2c
Figure 2:
The (2A) fat-suppressed T2-weighted coronal image reveals a vertical fracture (arrow) involving the sternochondral junction of the left 1st rib. Sequential axial images through the area of injury reveal chondral separation (arrow) at the sternal attachment on the more cephalad slice (2B). On the more inferior slice (2C), the chondral fracture is redemonstrated and a triangular chondral fragment (arrowhead) remains firmly attached to the sternum. Soft-tissue edema compatible with contusion injury is also present (asterisks).
Diagnosis
Acute fracture of the left medial 1st costal cartilage.
Introduction
A wide variety of pathology may be seen at the ribs, including traumatic, neoplastic, infectious, and metabolic lesions.1 Following trauma, rib fractures are often suspected, and typically are readily identified on plain radiographs. The clinical presentation of costal cartilage injuries, however, may be identical to that of rib fractures, but cartilage injuries are not detectable with radiographs unless considerable costal calcification is present.2 Computed tomography and ultrasound have been reported as effective in revealing costal cartilage fractures.3 MRI, with its superior soft tissue contrast and proven ability to evaluate cartilage elsewhere in the musculoskeletal system, would be expected to be the best modality for the evaluation of costal cartilage. However, this approach has received little attention, with only a single published series by Subhas et al. found in the radiology literature.4
Anatomy and function
The anatomy of the anterior ribs and costal cartilages is not widely recognized by many physicians. Because this region is infrequently imaged, many radiologists and even orthopaedic surgeons are surprised when visualizing the size of the costal cartilages at the anterior ribs. The anatomy is consistent. The costal cartilage of the 1st rib attaches to the manubrium, and the 2nd through 7th rib costal cartilages attach to the sternal body. The costal cartilages become increasingly wide from the 1st through 7th ribs. The 8th through 10th rib costal cartilages attach indirectly via a cartilage band that courses obliquely inferolaterally from the 7th rib. The last two ribs have no direct or indirect sternal attachment. The costal cartilages are a protective shock absorber for trauma to the anterior chest. Their flexibility also allows the ribcage to expand during respiration.
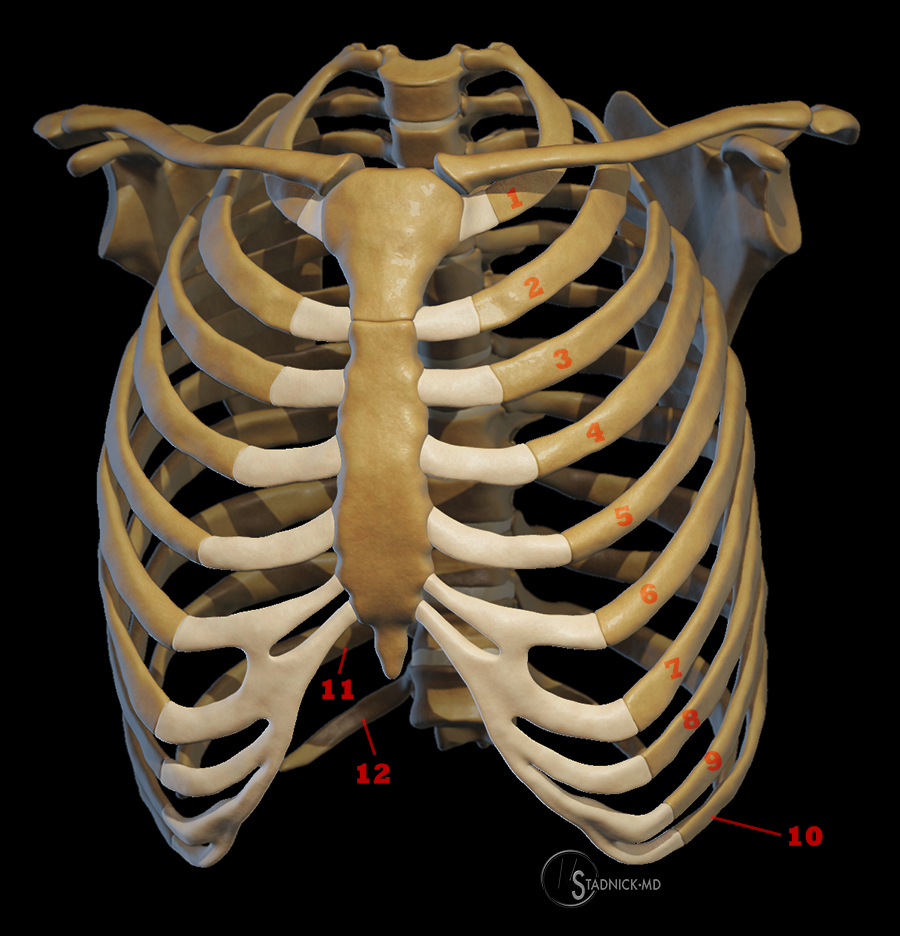
A 3D representation of the thorax demonstrates the normal anatomy of the costal cartilages. Illustration by Michael E. Stadnick, M.D.
MRI technique and normal appearance
MR imaging of costal cartilage can be challenging, as the ribs of course move with normal respiration. An effective technique in patients who can tolerate it is to position the patients prone using a spine or torso coil, which results in relatively less motion at the anterior chest. Generally acceptable results can be obtained with supine imaging as well, keeping imaging times relatively short, and when available, utilizing fast imaging techniques including breath-hold sequences. Another factor to remember is that because the chest contains the heart and great vessels, considerable pulsation artifact exists, and care must be taken to control the phase encoding direction, since pulsation artifact propagates in the phase encoding direction. As a result, axial images should be obtained with phase encoding right-left, and sagittal images with phase encoding superior-inferior, such that pulsation artifacts do not extend through the anterior chest wall (3).

3a
Figure 3:
3A. A STIR axial image was performed with the phase encoding direction mistakenly set up as anterior-posterior. Although costal cartilage is visible (asterisks), it is suboptimally visualized, particularly on the left, as cardiac pulsation artifact propagates through the anterior chest wall.
In general, costal cartilage injuries are best evaluated with a combination of T1-weighted and fat-suppressed T2-weighted or STIR image contrast (4). Proton density fat-suppressed views are also effective for costal cartilage pathology. T1-weighted images reveal normal anatomy and are useful for marrow evaluation in ossified regions. The coronal plane tends to be the most effective though pathology can be confirmed with sagittal or axial views.

4a

4b
Figure 4:
4A.B. Costal cartilages of the 2nd and 3rd ribs bilaterally demonstrate normal low signal intensity on T1 and fat-suppressed T2-weighted coronal images.
MR Imaging of Costochondral Injury
Costal cartilage injuries are most common in younger patients, as significant trauma, frequently sports-related, is a typical etiology.5,6 In our practice at Radsource, the most frequent cause we see is a direct blow to the chest in American football players. The most frequently reported site of injury is the 1st or 2nd rib, and injuries commonly occur at the sternochondral or costochondral junctions. Subhas et al. reported a characteristic pattern of injury at the sternochondral junction of the 1st rib, in which a small triangular chondral fragment remains attached to the sternum. As in the test case and the case below, we have also recognized this pattern in our practice (5).

5a

5b
Figure 5:
5A,B. Fat-suppressed T2-weighted coronal images from a NFL cornerback injured in a game. The upper image reveals sternochondral separation at the left clavicle (arrow) and a costal cartilage fracture at the left 1st rib with the typical attached triangular fragment (asterisk). An adjacent coronal slice reveals an irregular fracture of costal cartilage lateral to the sternal junction of the right 1st rib (arrow).
Costal cartilage fractures are thought to be common at the sternal junction of the upper ribs due to the relative immobility of the upper ribs, and such injuries often include a rotational component. In contrast, costal cartilage fractures of the lower ribs are more likely to be midsubstance and the result of a direct blow.6,7

6a
Figure 6:
6A. A fat-suppressed T2-weighted coronal image from a 49 year-old male who fell while water skiing at high speed. Linear mid-substance defects are present within the left 6th and 7th costal cartilages (arrowheads). The 6th rib cartilage fracture is mildly displaced. Associated soft tissue edema is also apparent.

7a

7b
Figure 7:
7A,B. A 54 year-old male presents for abdominal MRI following a MVA resulting in left upper quadrant and anterior abdominal pain. (7A) T2-weighted and (7B) fat-suppressed T2-weighted anterior axial images reveal an unexpected midsubstance fracture of the costal cartilage of the left 8th rib (arrows).
When imaged with MR, costal cartilage injuries are typically seen early due to the pain associated with a traumatic event. In some cases, however, patients delay seeking treatment and present with persistent pain and swelling at the anterior chest (8). It has been speculated that chronic pain following a costal cartilage injury may be caused by an ineffective chondrocyte response to a cartilage fracture.7

8a
Figure 8:
8A. A fat-suppressed T2-weighted coronal image in a 66 year-old male who complains of pain and swelling in the clavicle region following a fall 3 months earlier. A fracture near the sternochondral junction of the left 1st rib is apparent (arrow). Small adjacent fluid collections (arrowheads) are present and may be secondary to hemorrhage and/or instability.
Differential Diagnosis
Following a traumatic event, patients with anterior chest pain may of course have true osseous fractures rather than costal cartilage fractures. Similar MR imaging techniques can identify the fractures and confirm normal costal cartilage (9,10). Soft-tissue injuries in the region of the costal cartilages can also be readily identified with MRI (11).

9a
Figure 9:
9A. A fat-suppressed T2-weighted coronal image in a patient 2 weeks following MVA with persistent chest wall pain reveals a comminuted sternal fracture (arrows). Costal cartilages demonstrate normal low signal intensity. A non-displaced fracture is present within the anterior left 3rd rib near the costochondral junction (arrowhead).

10a

10b
Figure 10:
10B. Fat-suppressed T2-weighted images are provided from a 23 year-old male with right sided chest pain following an MVA. The (10A) straight coronal image demonstrates marrow edema within the anterior 7th and 8th ribs adjacent to the costochondral junction (arrows). An oblique coronal image (10B) through this area of interest reveals small fracture lines within both ribs (arrows) with normal appearing adjacent costal cartilage.

11a

11b
Figure 11:
11A,B. Fat-suppressed proton density-weighted axial (11A) and sagittal (11B) images are provided from a 26 year-old professional football player with severe pain following a blow to the lower chest. Edema and fluid (arrows) surround a normal appearing left 9th costal cartilage. The findings are compatible with soft tissue contusion and hemorrhage.
Treatment
Treatment of costal cartilage fractures is typically conservative, consisting of rest, ice, and nonsteroidal anti-inflammatory medications. Athletes are usually restricted from a return to the sport until pain has significantly subsided, and the length of time required varies from 2 weeks to several months. In professional athletes, rib protective clothing and anesthetic blocks may allow a more rapid return to play.8
Conclusion
Costal cartilage fractures are an under-recognized cause of anterior chest pain following traumatic events, as they are typically not detectable on plain radiographs. This injury is thought to be relatively rare, but it is likely that it is more common than believed and that the entity is simply underdiagnosed. PACS Radiology with MRI is an effective tool for the evaluation of these injuries, providing greater conspicuity of injuries as compared to CT, and obviating the need for the specialized skill set required to make this diagnosis with ultrasound.
References
- Guttentag AR, Salwen JK. Keep your eyes on the ribs: the spectrum of normal variants and diseases that involve the ribs. Radiographics 1999; 19:1125-1142. ↩
- Griffith JF, Rainer TH, Ching AS, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR 1999; 173:1603 –1609. ↩
- Malghem J, Vande Berg B, Lecouvet F, Maldague B. Costal cartilage fractures as revealed on CT and sonography. AJR 2001; 176:429 –432. ↩
- Subhas N, Kline MJ, Moskal MJ et al. MRI evaluation of costal cartilage injuries. American Journal of Roentgenology 2008. 191:129-132. ↩
- Kemp SP, Targett SG. Injury to the first rib synchondrosis in a rugby footballer. Br J Sports Med 1999; 33:131–132. ↩
- Miles JW, Barrett GR. Rib fractures in athletes. Sports Med 1991; 12:66 –69. ↩
- Buckwalter JA, Cruess RL. Healing of the musculoskeletal tissues. In: Rockwood CA Jr, Green DP, Bucholz RW, eds. Rockwood and Green’s fractures in adults, 3rd ed. Philadelphia: Lippincott,1991:181–222. ↩
- McAdams TR, Deimel JF, Ferguson J, et al. Chondral rib fractures in professional American football: two cases and current practice patterns among NFL team physicians. Orthopaedic Journal of Sports Medicine 2016; 4(2). ↩
