Clinical History
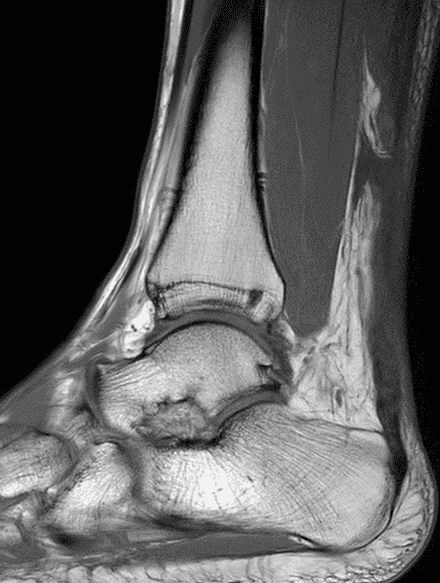
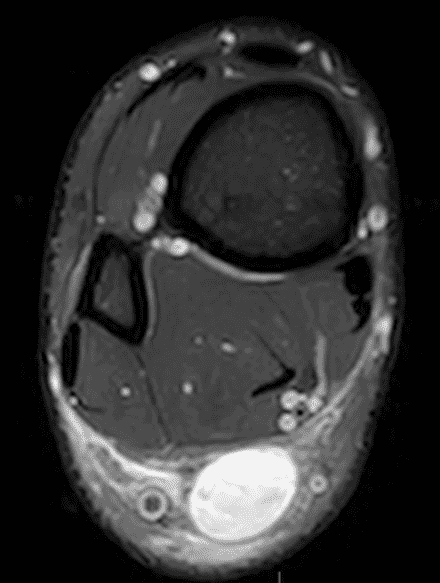
A 22 year-old male college football player presents with a “pop” and pain posterior to the right ankle during practice 1 week prior. He is unable to bear weight. Lateral radiograph (1A), sagittal fat-suppressed T2-weighted (1B), sagittal T1-weighted (1C), and transverse fat-suppressed T2-weighted images are provided. What is your diagnosis? What MRI findings affect clinical management decisions?


Findings
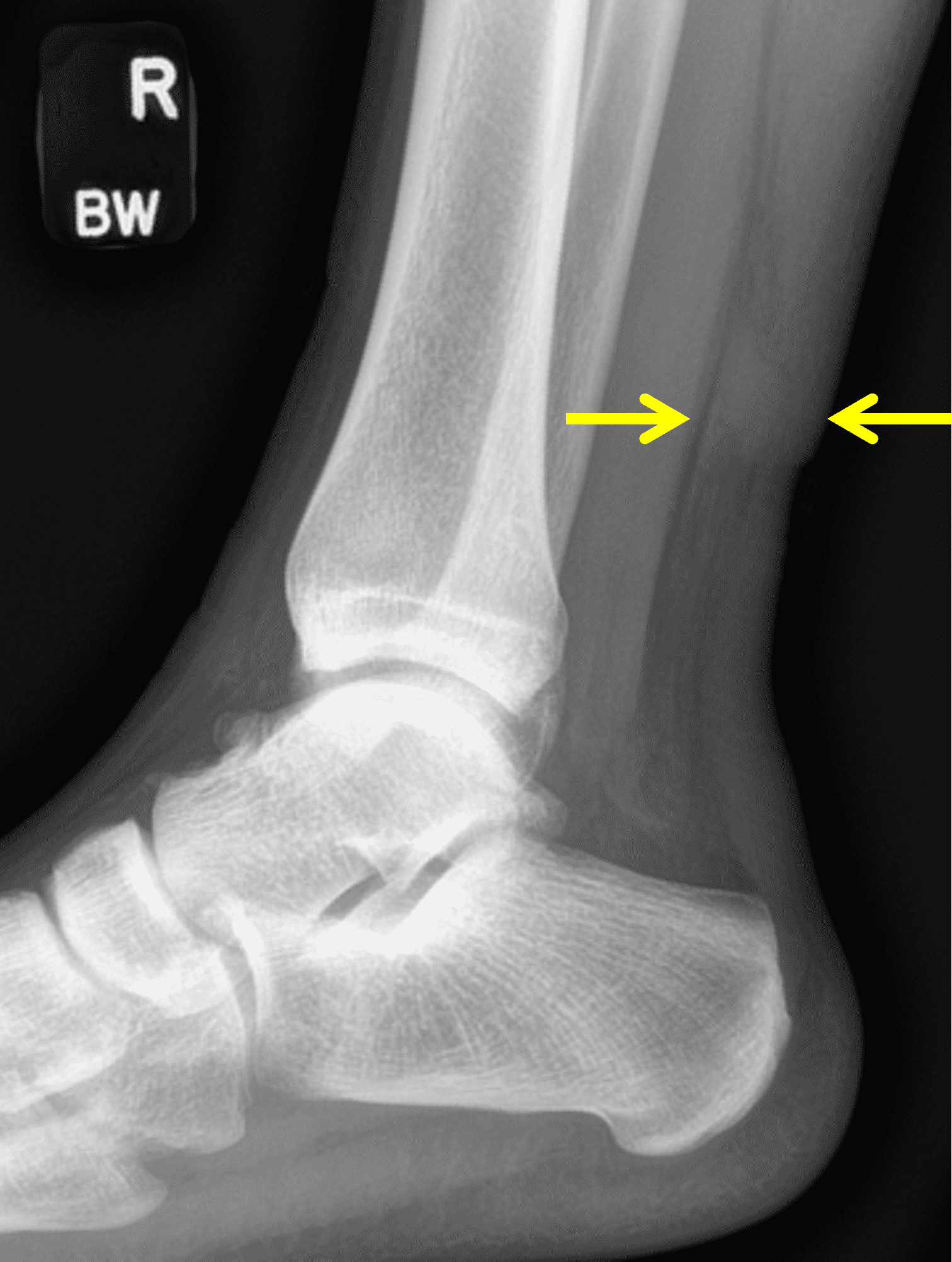
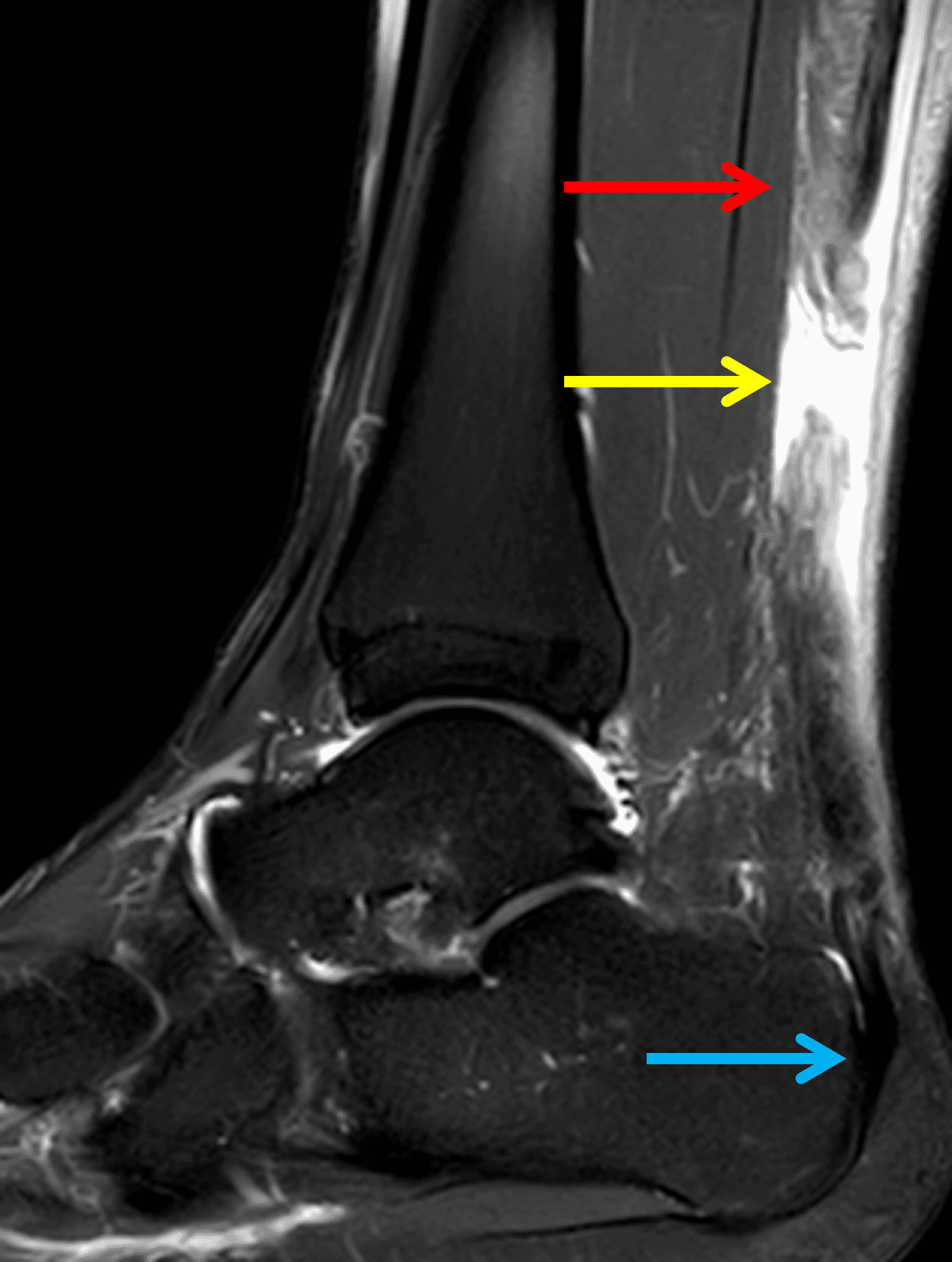
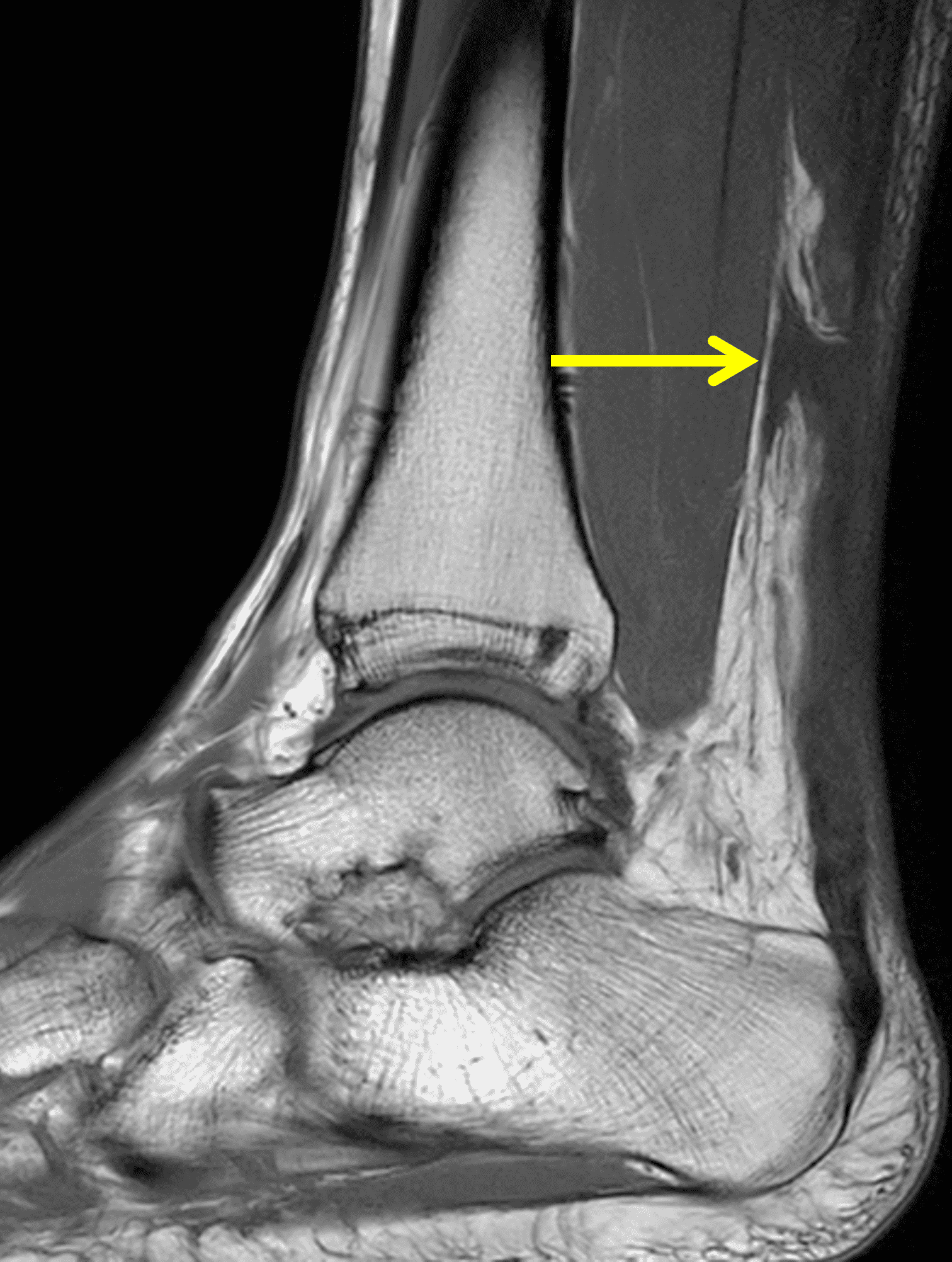
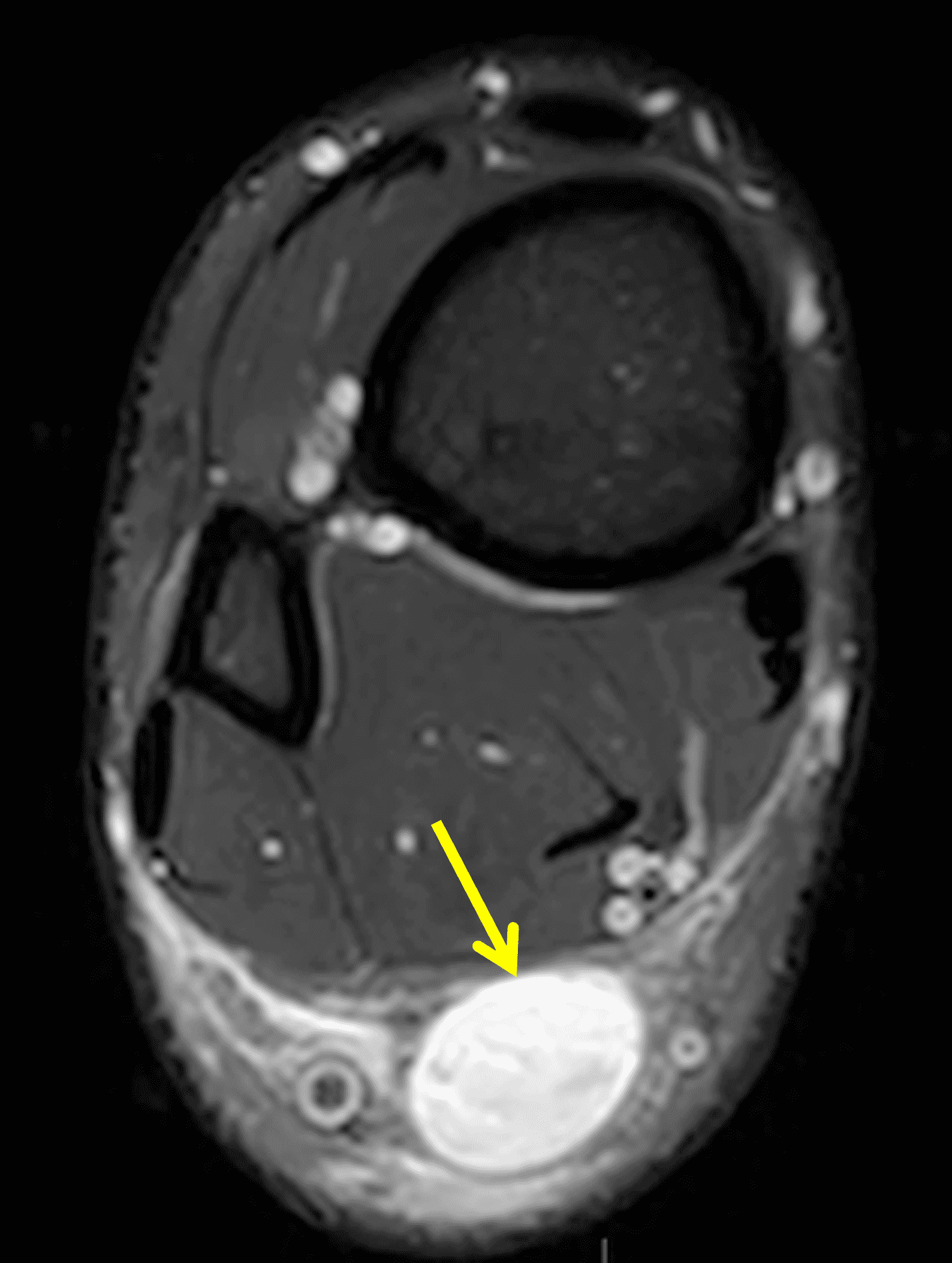
Figure 2: Complete Achilles tendon rupture. (2A) The lateral radiograph shows a thick and indistinct proximal Achilles tendon contour (arrows). (2B) A fat-suppressed T2-weighted image shows complete rupture of the tendon with a fluid-filled gap (yellow arrow) measuring 1.5 cm in length, located 10 cm cranial to the tendon insertion (blue arrow) and just distal to the edematous myotendinous junction (red arrow). The tear is superimposed on diffuse tendinosis. (2C) A sagittal T1-weighted image confirms the diffuse tendinosis. Fluid extends anteriorly into Kager’s fat pad (arrow) suggesting disruption of the anterior paratenon. (2D) A transverse fat-suppressed T2-weighted image through the proximal tendon shows no intact fibers (arrow), confirming the full-thickness rupture.
Diagnosis
Acute, complete Achilles tendon rupture just distal to the myotendinous junction, superimposed on diffuse tendinosis.
Introduction
The Achilles tendon is the largest and strongest tendon in the body yet remains one of the most frequently injured, with an estimated incidence of 5–50 ruptures per 100,000 person-years. Injury rates have risen over recent decades, particularly in older individuals. Acute ruptures most often occur in middle-aged adults, though the burden spans younger athletes as in the initial case example, as well as older sedentary groups.1,2,3
Injury reflects overlapping contributors including mechanical overuse, altered biomechanics, and intrinsic degeneration. Imaging – primarily with ultrasound or MRI –assists in confirming diagnosis but is also useful in guiding management and follow-up. MRI is particularly useful because it depicts the full heel complex including tendon, paratenon, Kager’s fat pad, retrocalcaneal bursa, marrow, and soft tissues and thus provides information that guides surgical planning.4,5,6 Furthermore, MRI can show regional pathology that may present similarly including plantar fasciitis, calcaneal stress fracture, subtalar osteoarthrosis, inflammatory arthrosis, and peroneal/flexor tendon disorders.
Normal Anatomy and Function
The Achilles tendon forms from the confluence of gastrocnemius (medial and lateral heads) and soleus aponeuroses (Figure 3A), with variable contribution from the plantaris tendon; a separate plantaris is present in most individuals.7,8 Distally, the tendon fibers spiral before inserting on the posterior calcaneus where there a three described facets: a superficial facet related to the retrocalcaneal bursa; a middle facet where the tendon fibers of the soleus insert medially and the lateral gastrocnemius insert laterally; and an inferior facet where the medial gastrocnemius tendon fibers insert (Figure 3B).9,10,11 Neonates can show fibrous continuity between the Achilles tendon and plantar fascia via the calcaneal periosteum, which attenuates with age; the fibrous connection can develop into an “ossifying bridge” in adults.12,13
Rather than a synovial sheath, the Achilles is enveloped by a vascular paratenon continuous with proximal fascia and distal calcaneal periosteum, permitting approximately 1.5 cm of longitudinal excursion. Arterial supply arises from a peritendinous network predominantly composed of posterior tibial branches medially, with peroneal contributions laterally. A hypovascular watershed zone 2-6 cm proximal to the tendon insertion, where the tendon cross-section narrows, is a common site for mid-substance tears.11,14
The retrocalcaneal bursa sits between posterior calcaneal fibrocartilage and the distal tendon. The normal bursa measures <7 mm craniocaudal, <2 mm AP, and <11 mm transverse. Kager’s fat pad is mobile and can invaginate into the bursa during plantar flexion, reducing friction.5, 6 The plantaris tendon usually courses medial to the Achilles near the musculotendinous junction with variable insertions; an accessory soleus muscle and tendon located anteromedial to the Achilles is a common normal variant and its presence may coexist with Achilles tendinosis. 8, 11,15,16 The sural nerve, a sensory nerve that innervates the skin in the distal posterolateral leg, courses along the dorsal surface of the distal gastrocnemius muscle bellies and the proximal Achilles tendon, and then along the lateral margin of the mid and distal tendon before entering the hindfoot posterior to the peroneal tendons (Figure 3A).17
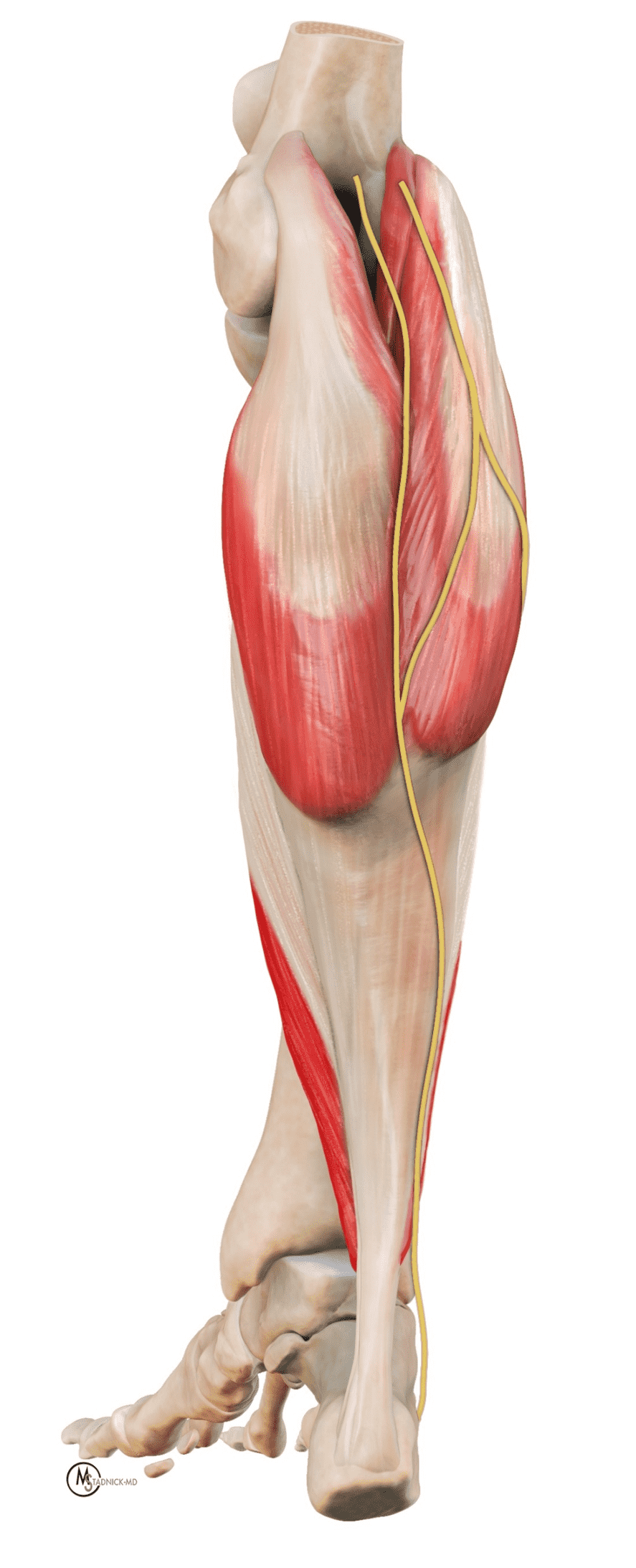

Figure 3: Illustrations of the normal anatomy related to the Achilles tendon. (3A) A posterior projection shows the tendon forming as a confluence of the gastrocnemius heads (medial and lateral) and the soleus. The sural nerve courses along the superficial surface of the proximal Achilles tendon and the lateral margin of the mid and distal tendon; the nerve is at risk of iatrogenic injury during percutaneous tendon repairs. (3B) Renditions of the Achilles insertion. The Achilles tendon components (medial gastrocnemius-blue, lateral gastrocnemius-red, soleus- green) spiral proximal to their insertions, with the retrocalcaneal bursa (yellow) located between the tendon and posterosuperior calcaneus. The lower drawing shows the respective calcaneal facets (superficial-yellow, medial aspect of the middle facet-green, lateral aspect of the middle facet-red, inferior facet-blue).
Via the Achilles tendon, the triceps surae provides primary plantar flexion for gait, running, and jumping. Additionally, the soleus stabilizes posture by resisting anterior tibial translation during quiet standing.18 Loads reach about 2-3 x body weight during walking and can exceed 10 x body weight (reported up to 12.5 x) during running.19
On MR images, the normal Achilles tendon demonstrates low signal intensity on all sequences (Figure 4). On sagittal images, the tendon should be uniform in thickness and have a sharp anterior margin where it abuts Kager’s fat pad. High-resolution images may reveal fine punctate or linear intermediate signal from normal interfascicular septa, especially in the distal tendon, which should not be misinterpreted as tendinosis, particularly when the tendon thickness is normal.6 When the tendon fibers are oriented near to 55° with respect to the B0 magnetic field, increased signal may be seen on short-TE sequences due to the magic angle effect, with decreasing artifact on longer-TE sequences. MR images obtained at higher field strengths (3-7 T) accentuate the fascicular detail and normal septations as well as magic-angle effects.5,6 On transverse images, the posterior tendon margin is typically convex; the anterior margin is flat-to-concave along most of its length but may be focally convex at the gastrocnemius–soleus convergence, which is considered a normal variant. The average tendon thickness is approximately 6 mm, with variation by body size, age, and sex.20
The normal Achilles paratenon appears as a thin low-to-intermediate signal rim.6 The retrocalcaneal bursa lies between the distal tendon and calcaneus and normally contains only minimal fluid. The contents of Kager’s fat pad should be isointense to fat on all pulse sequences, with traversing vessels and thin fascial strands that should not be mistaken for pathology.
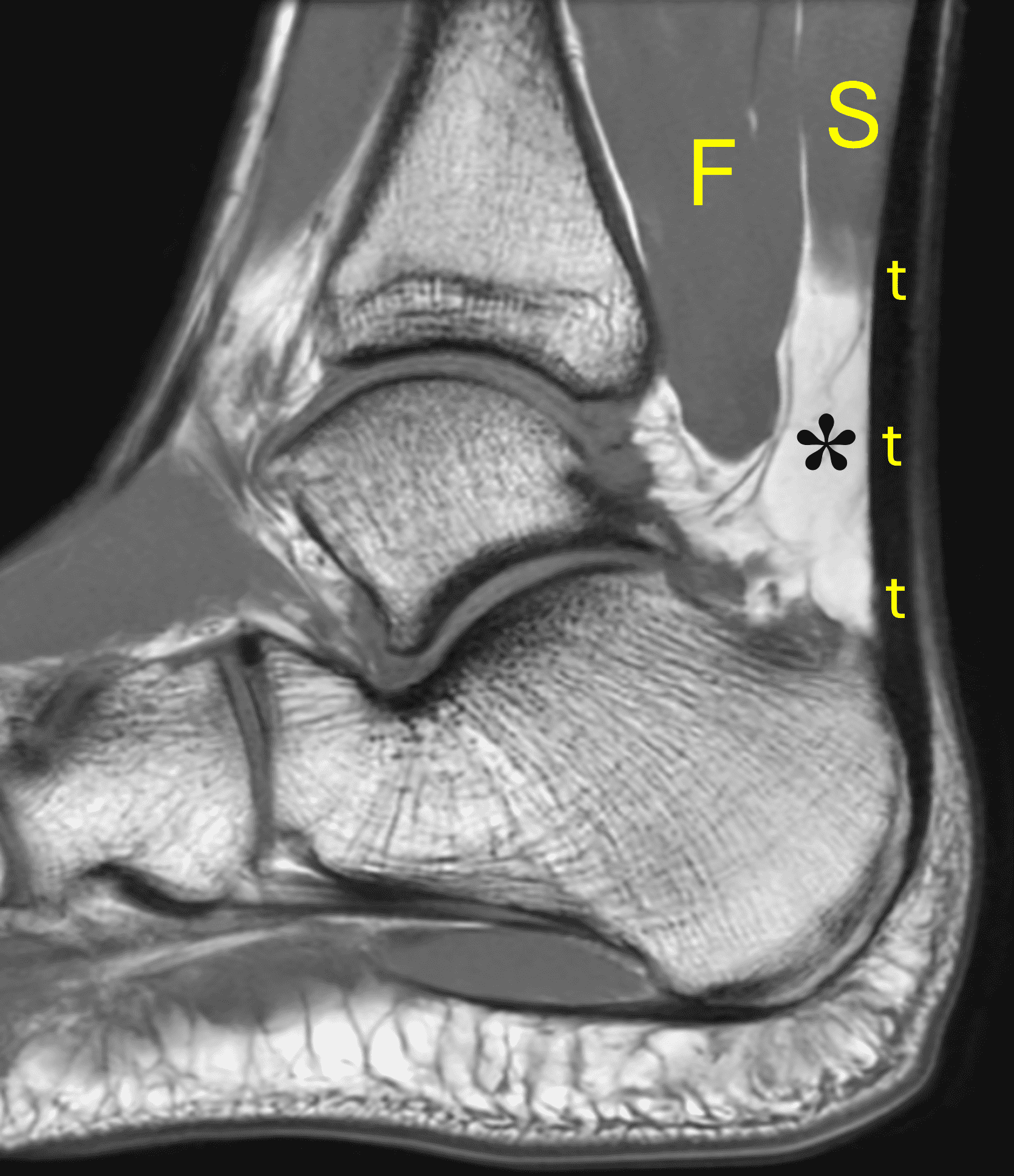
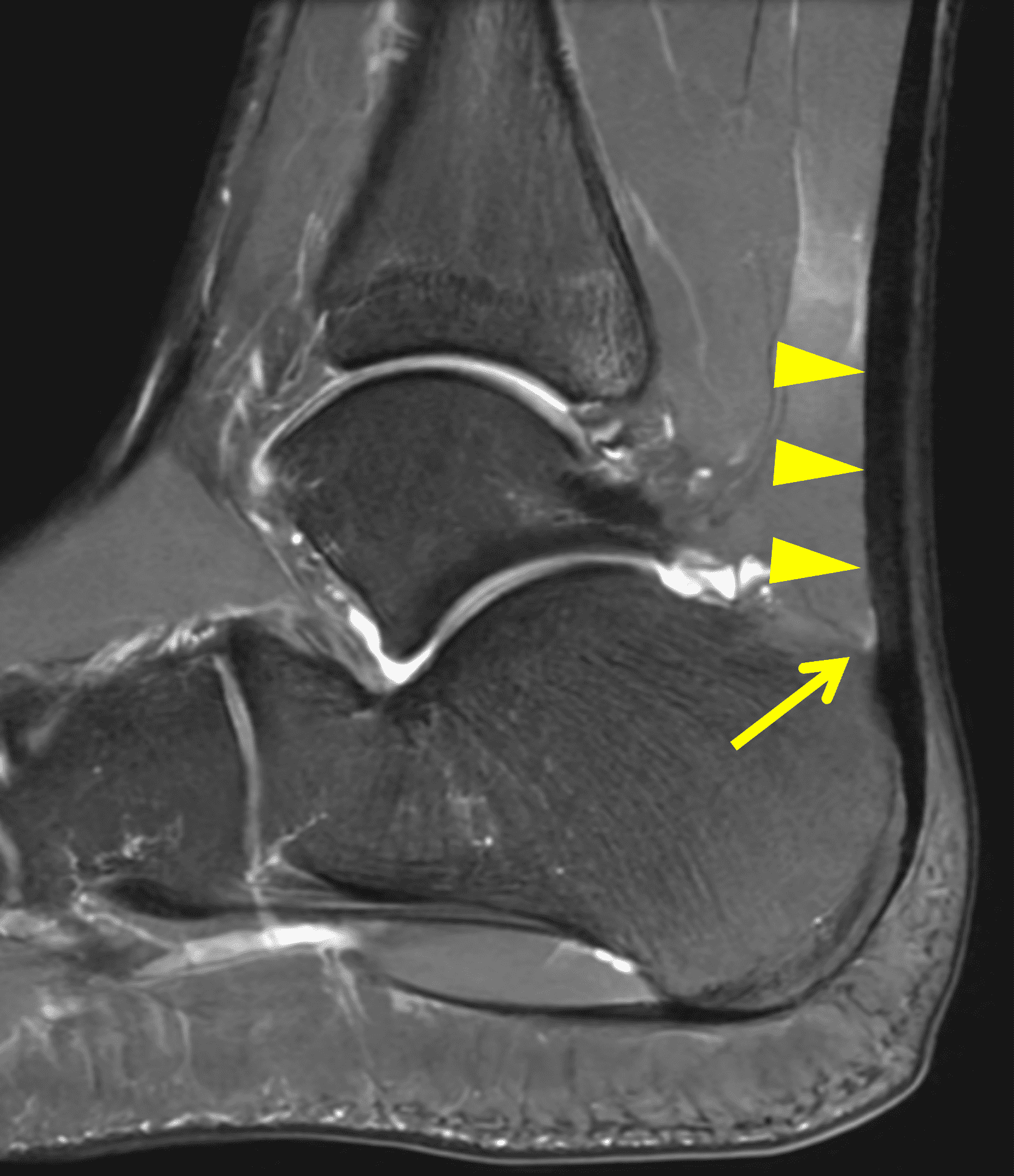
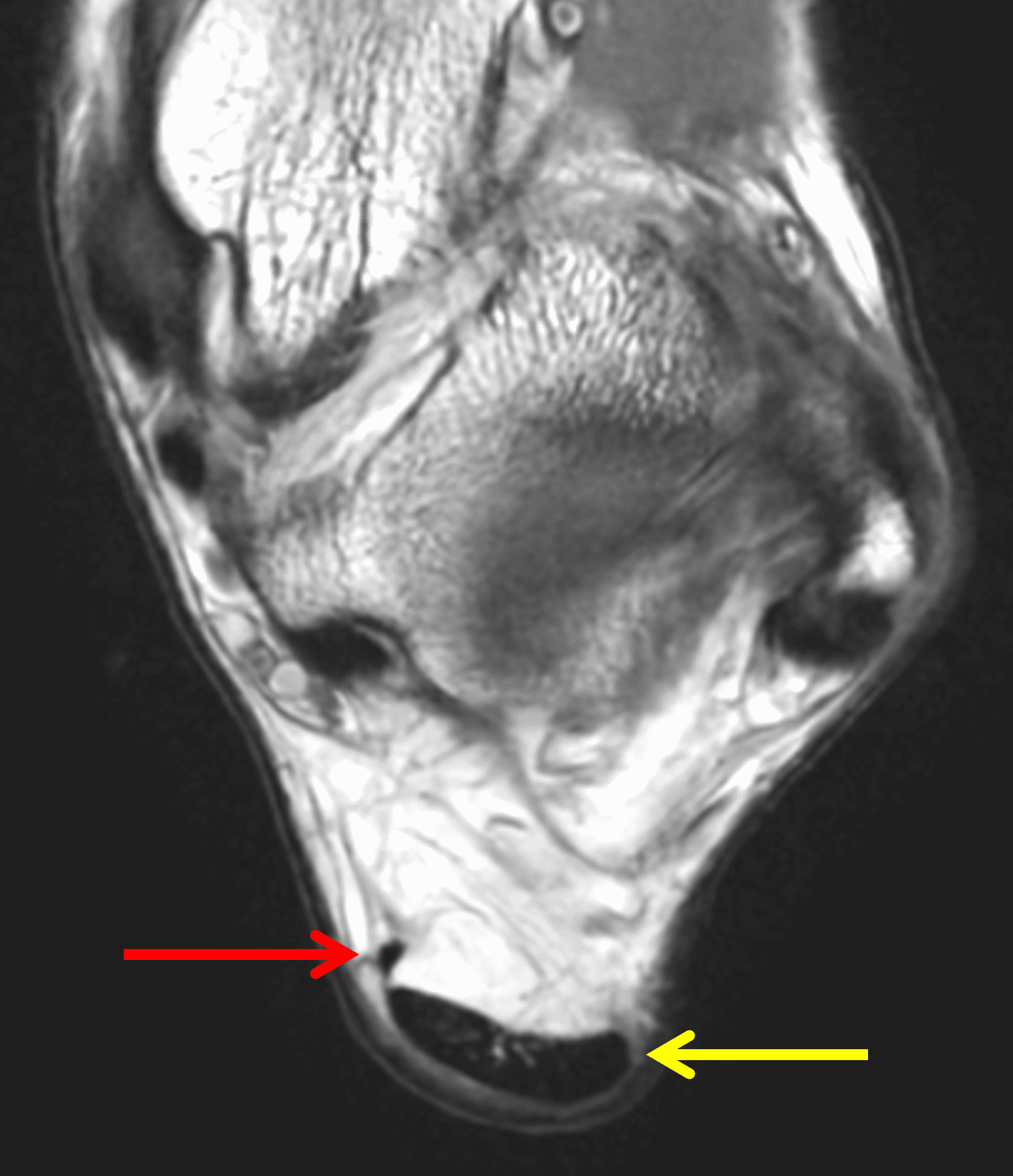

Figure 4: MRI appearance of the normal Achilles tendon. (4A) Sagittal T1-weighted image shows the low signal intensity Achilles tendon (t) with uniform thickness. Kager’s fat pad (asterisk) normally contains thin fibrous strands and vessels. S = soleus muscle, F = flexor hallucis longus muscle. (4B) Sagittal fat-suppressed fluid-sensitive sequence shows the sharp anterior tendon margin (arrowheads) and a physiologic amount of fluid in the retrocalcaneal bursa (arrow). (4C) Transverse T1-weighted image just proximal to its insertion shows the Achilles tendon (yellow arrow) with a concave anterior margin and convex posterior margin. The much smaller plantaris tendon (red arrow) lies along the anteromedial margin of the Achilles. (4D) Transverse fat-suppressed T2-weighted image shows punctate foci of higher signal intensity (arrowhead) in the distal tendon representing normal interfascicular septa.
Clinical Findings
With an acute injury, patients with a ruptured Achilles tendon may hear an audible “pop” and often report a sensation of having been kicked in the calf. Injuries typically occur with sustained plantar flexion activity. A complete tendon rupture will result in loss of plantar flexion strength, weakness, limp, inability to run or play sports, loss of heel rise, and difficulty climbing stairs.21 Physical examination is performed with the patient lying prone on the exam table with their feet overhanging the edge. The primary test is the Thompson test in which the examiner squeezes the calf muscle to elicit plantar flexion at the ankle.22 Visual inspection for decreased resting tension compared to the contralateral side is also performed, with normal plantar flexion typically 20-30 degrees. Evaluation is also performed for a palpable defect in the tendon and active plantar flexion against resistance.
Imaging Findings
In the MRI evaluation of an Achilles tendon injury, the radiologist should note the location of the tear, whether the tear is complete or partial, the size of the tendon gap, the presence and degree of underlying tendinosis, abnormalities in the surrounding soft tissues or calcaneus (such as a Haglund process), findings pointing to an acute versus chronic injury, and additional pathology in the ankle and hindfoot. An assessment of any abnormalities in potential graft donor sites (i.e. the flexor hallucis longus tendon or accessory soleus, if present) should be performed.
Classification of tear location falls into 3 categories: insertional, mid-substance, and myotendinous junction. The most common rupture location is in the mid tendon. Note that while the classic anatomic definition of a mid-substance tear is within the relatively avascular zone located 2 to 6 cm above the insertion, a large MRI review of 195 cases published in 2019 established that most tears (80%) on MRI occur between 5.0 and 8.4 cm cranial to the inferior margin of the calcaneal insertion.23
Insertional Tears
Insertional tendinosis manifests as thickening and signal abnormality involving the distal tendon fibers at or near the calcaneal attachment, often with intrasubstance calcification or enthesophytes. Haglund syndrome (Figure 5) describes a triad of insertional Achilles tendinosis, retrocalcaneal bursitis, and a prominent posterosuperior calcaneus (the Haglund deformity).5 Radiographs can depict the bone changes while MRI can show the degree of tendinosis and tendon tearing as well as retrocalcaneal bursitis and/or retro-Achilles soft-tissue edema. Initial management includes orthotics and physical therapy. Refractory cases may require Haglund resection, calcaneal osteotomy, and tendon debridement with or without augmentation using a flexor hallucis longus transfer.24 High-grade and complete insertional tears (Figure 6) and tendon avulsions are typically managed surgically.
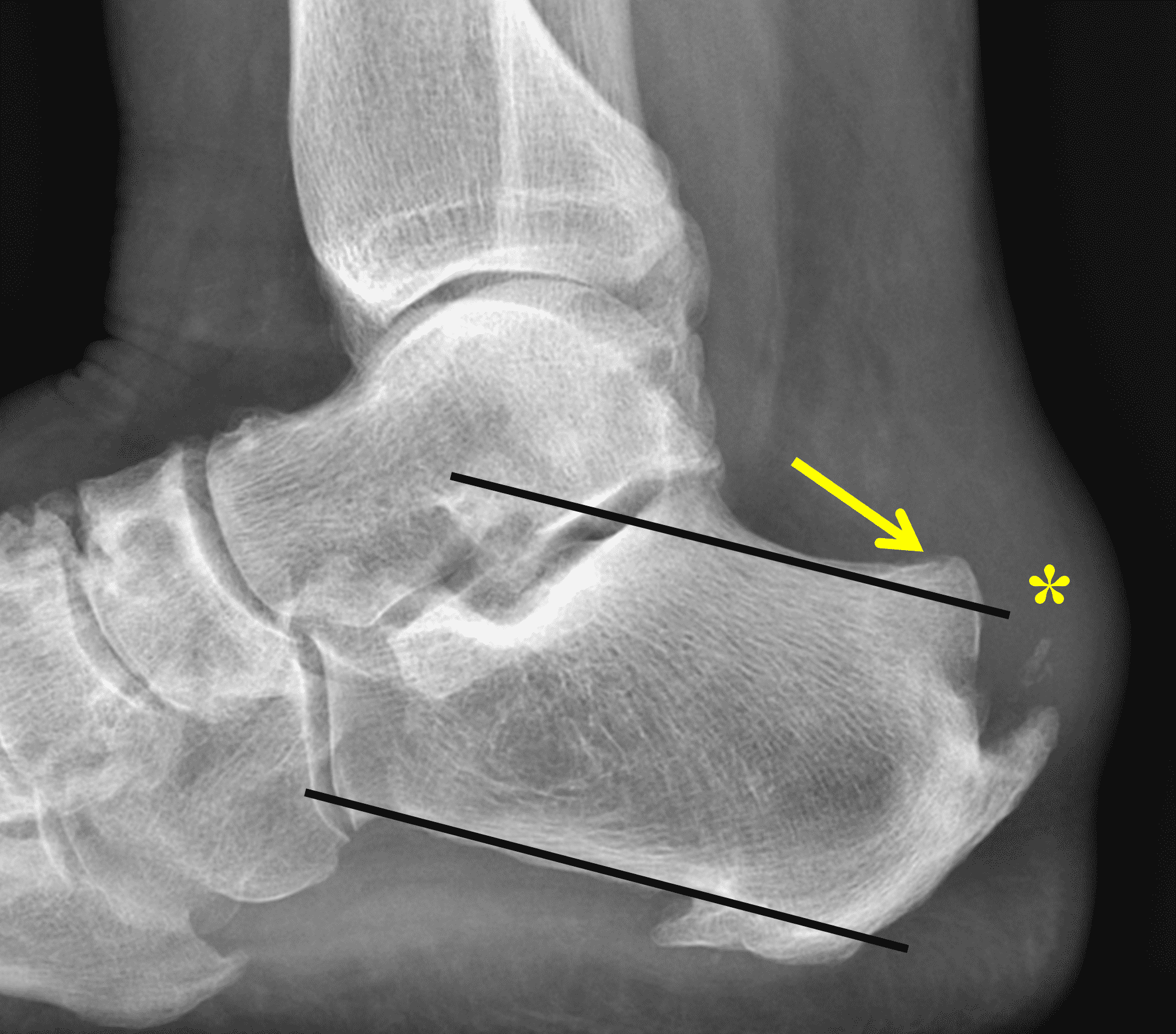
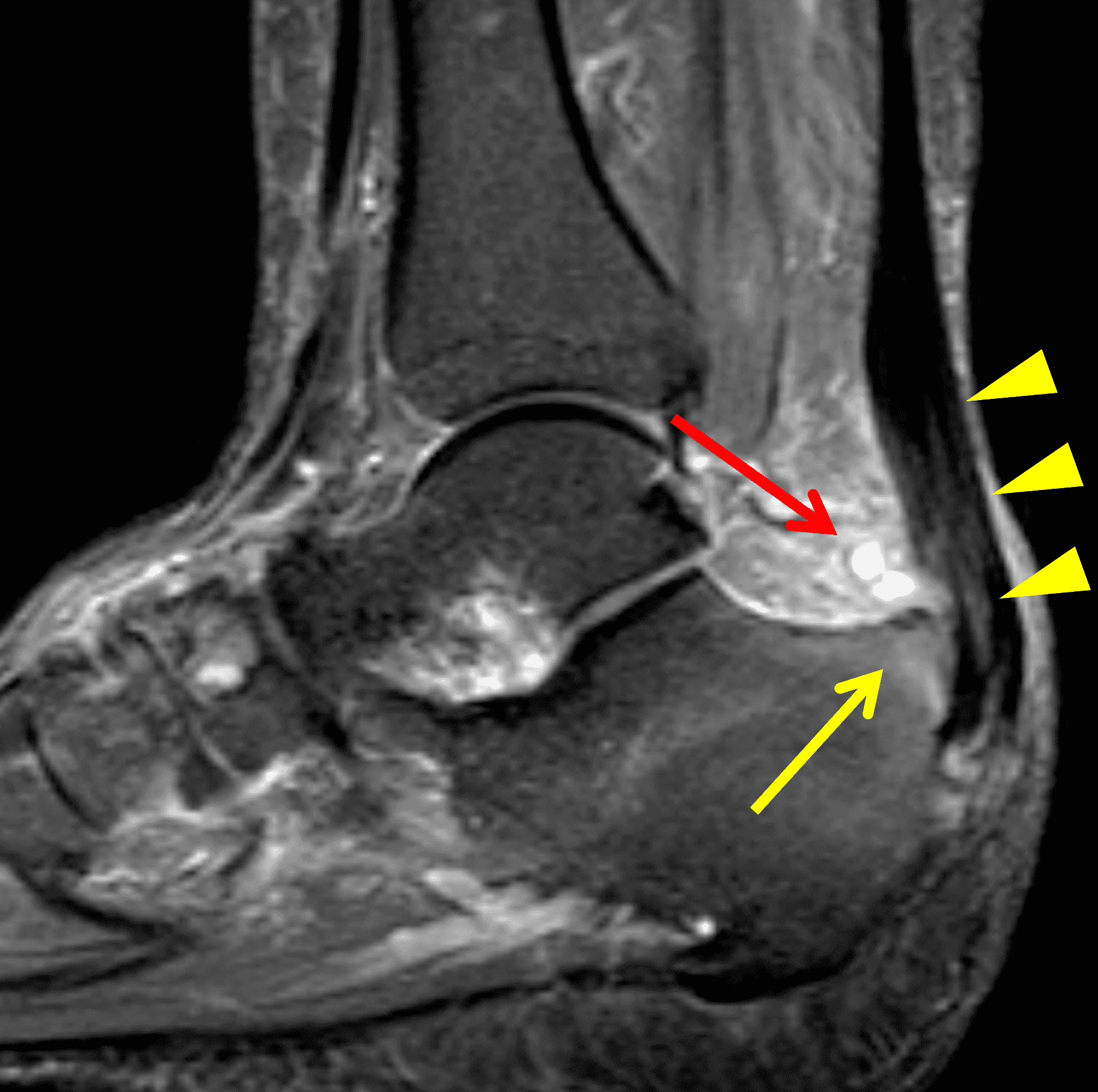
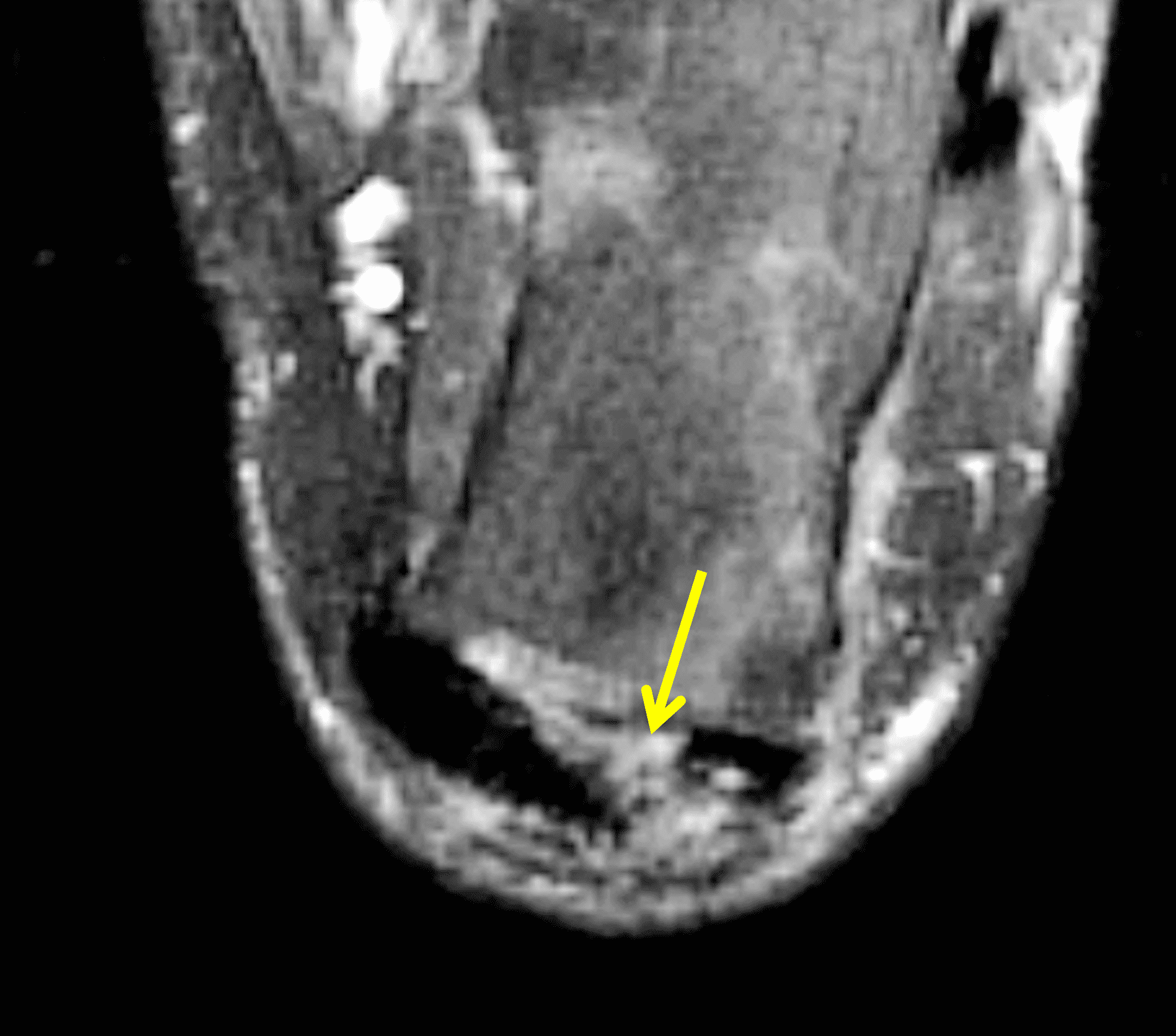

Figure 5: 69 year-old woman with Haglund syndrome and low-grade insertional Achilles tendon tear. (5A) Lateral radiograph demonstrates a hypertrophied osseous excrescence of the posterosuperior calcaneus (arrow) rising above a pitch line drawn parallel to the inferior calcaneal body. Note the soft tissue swelling (“pump bump,” asterisk) as well as the posterior heel spur and soft tissue calcification. (5B) Sagittal STIR image reveals moderate tendinosis with thickening and increased signal in the distal tendon (arrowheads), mild retrocalcaneal bursitis (red arrow), and the Haglund process with mild adjacent marrow edema (yellow arrow). (5C) Transverse fat-suppressed, fluid-sensitive image shows partial tendon tearing at the calcaneal insertion (arrow). (5D) Post-operative lateral radiograph following resection of the Haglund process and Achilles reinsertion.
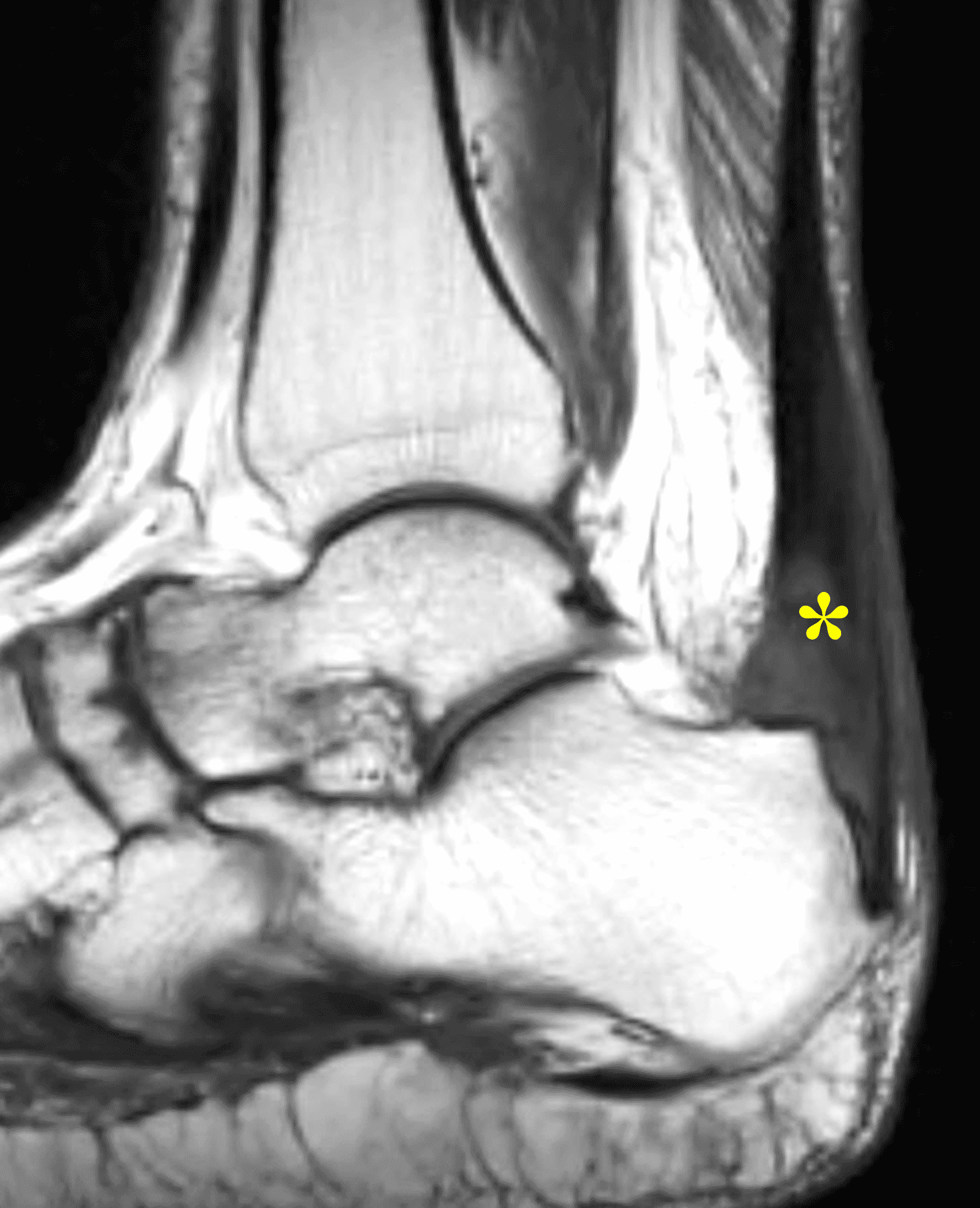
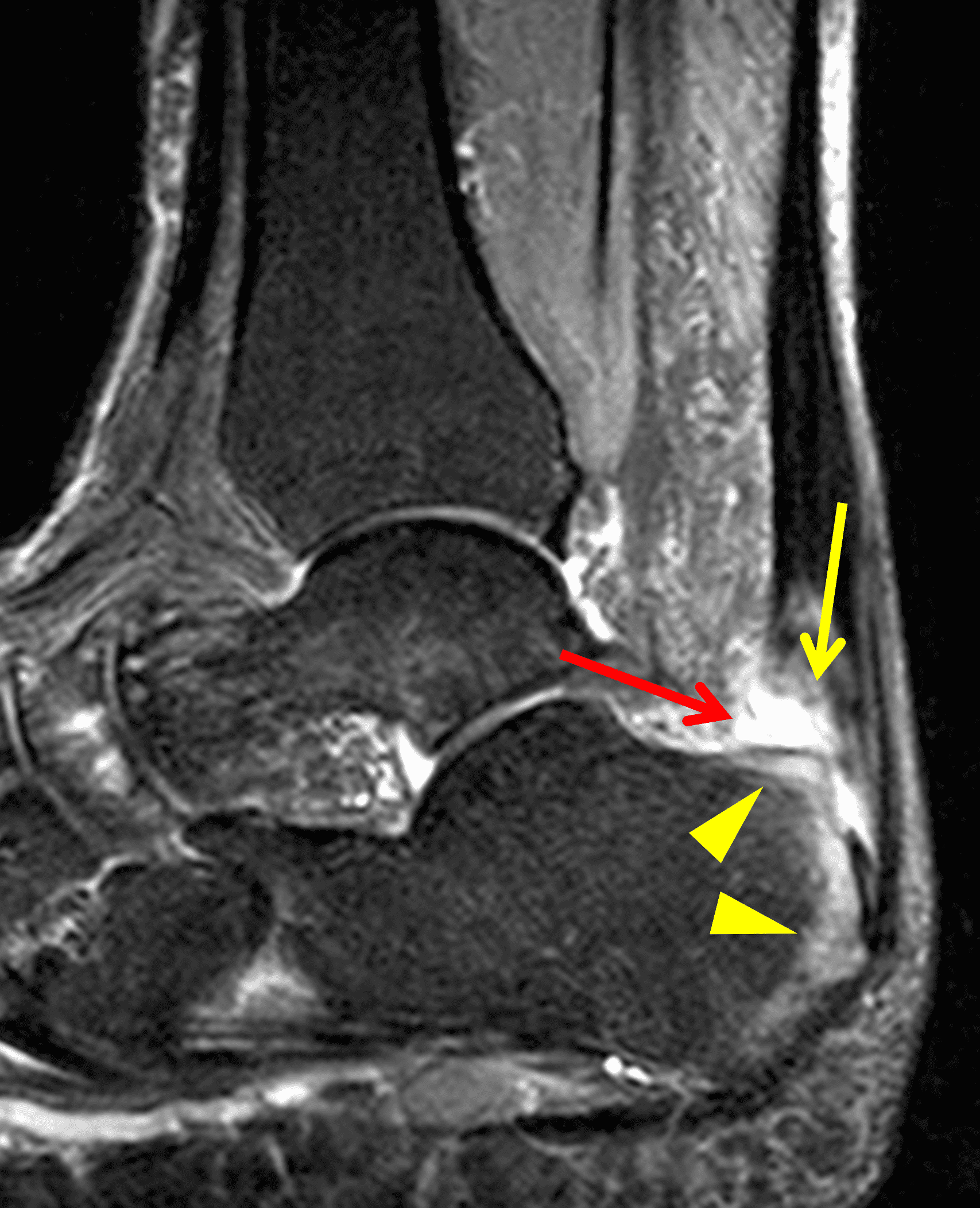
Figure 6: 40 year-old man with a high-grade, partial-thickness insertional Achilles tendon tear. (6A) Sagittal T1-weighted image shows severe tendinosis in the distal Achilles tendon with tendon thickening and increased signal intensity (asterisk). (6B) Sagittal STIR image demonstrates a high-grade, partial-thickness tendon tear (yellow arrow), as well as moderate retrocalcaneal bursitis (red arrow) and marrow edema in the periphery of the posterior calcaneus representing enthesitis (arrowheads).
Distal tendon avulsions, with or without an accompanying calcaneal fracture, can also occur after acute trauma (Figure 7). Additionally, spontaneous or low-energy posterior calcaneal avulsions have been reported in patients with longstanding diabetes mellitus and neuropathy.25 Repair techniques for avulsion fractures depend on the fragment size with larger fracture fragments transfixed by cannulated cancellous screw and Kirschner wires to varying success. Smaller bone fragments are debrided with reinsertion of the tendon to the remaining calcaneus.26,27
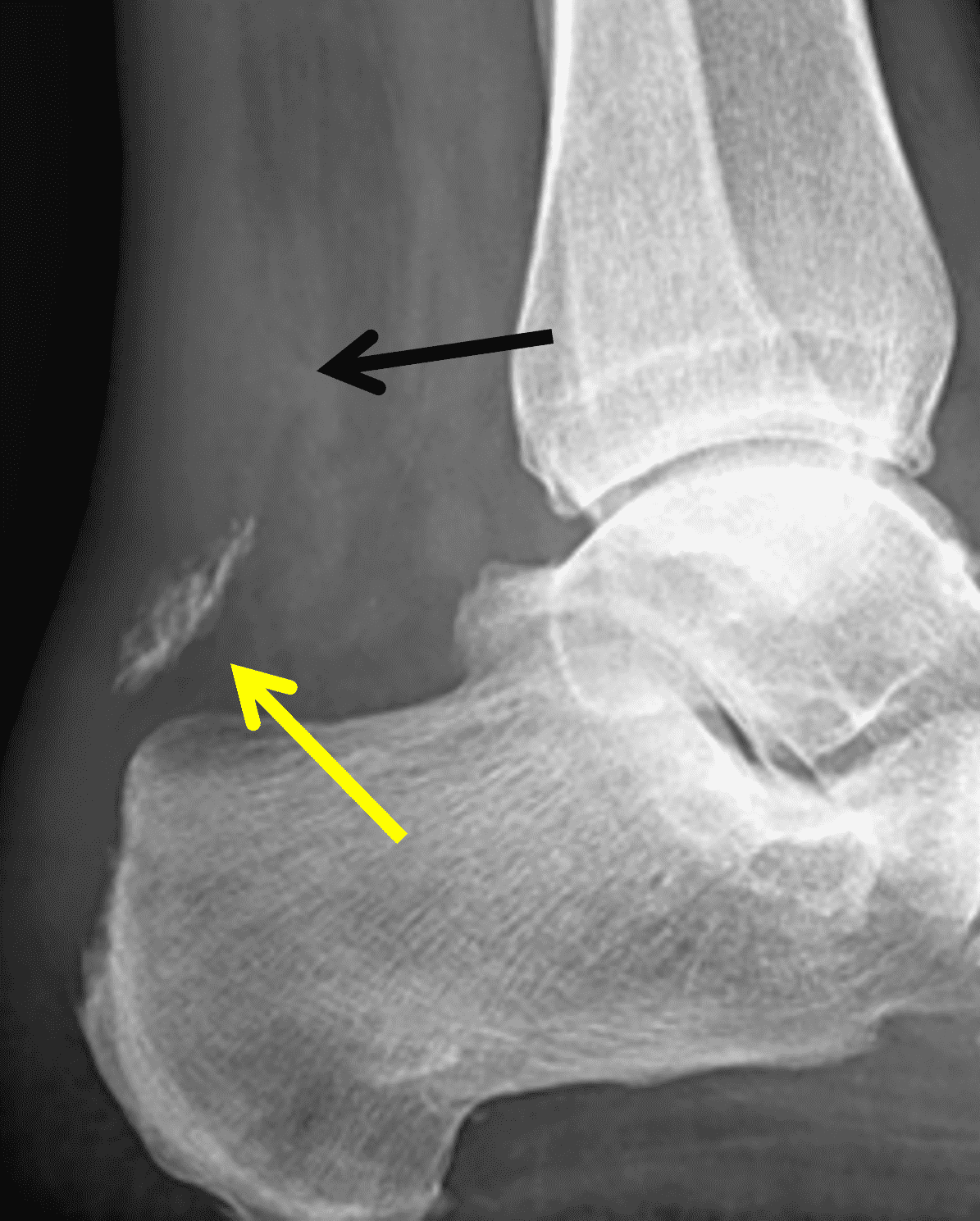
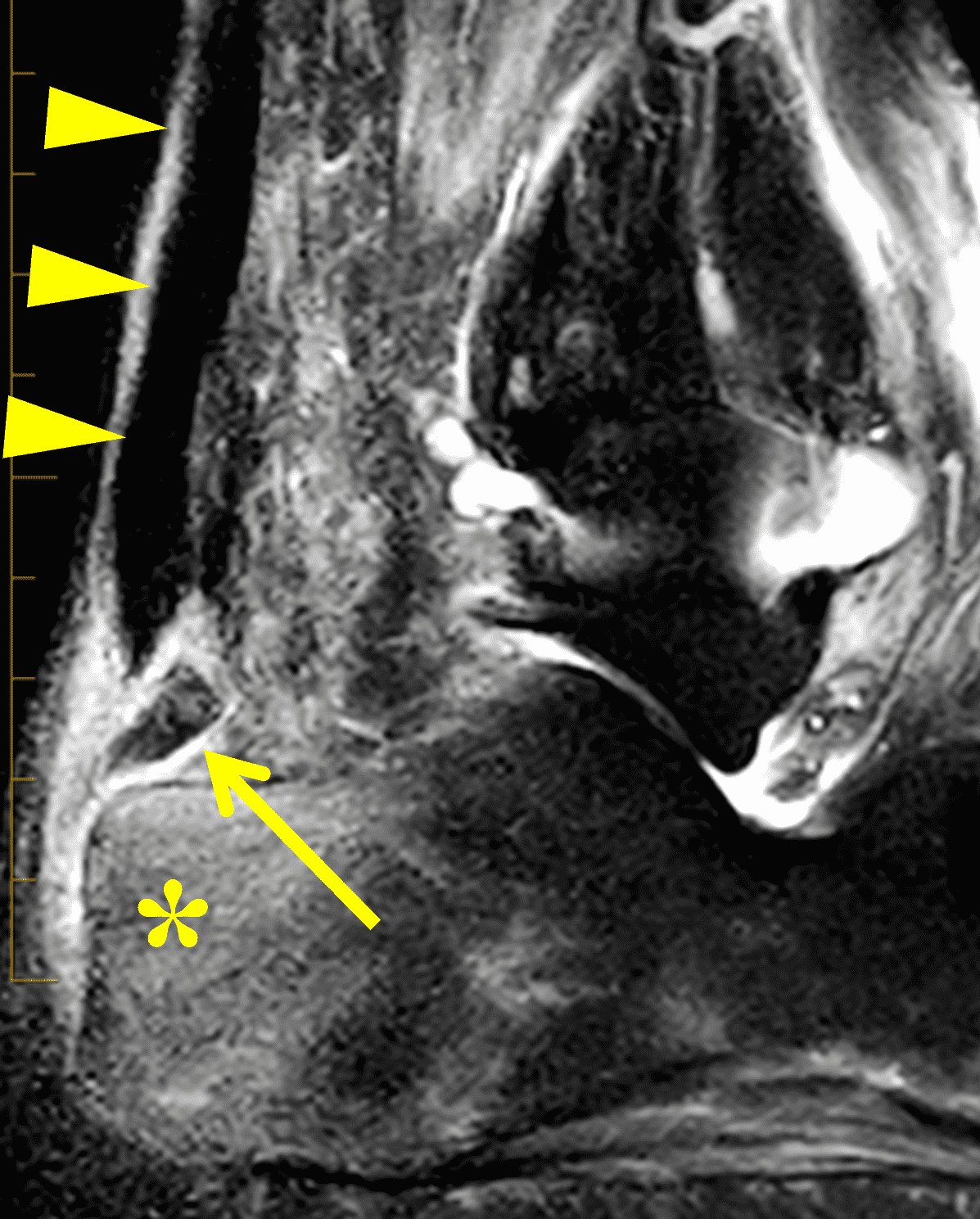
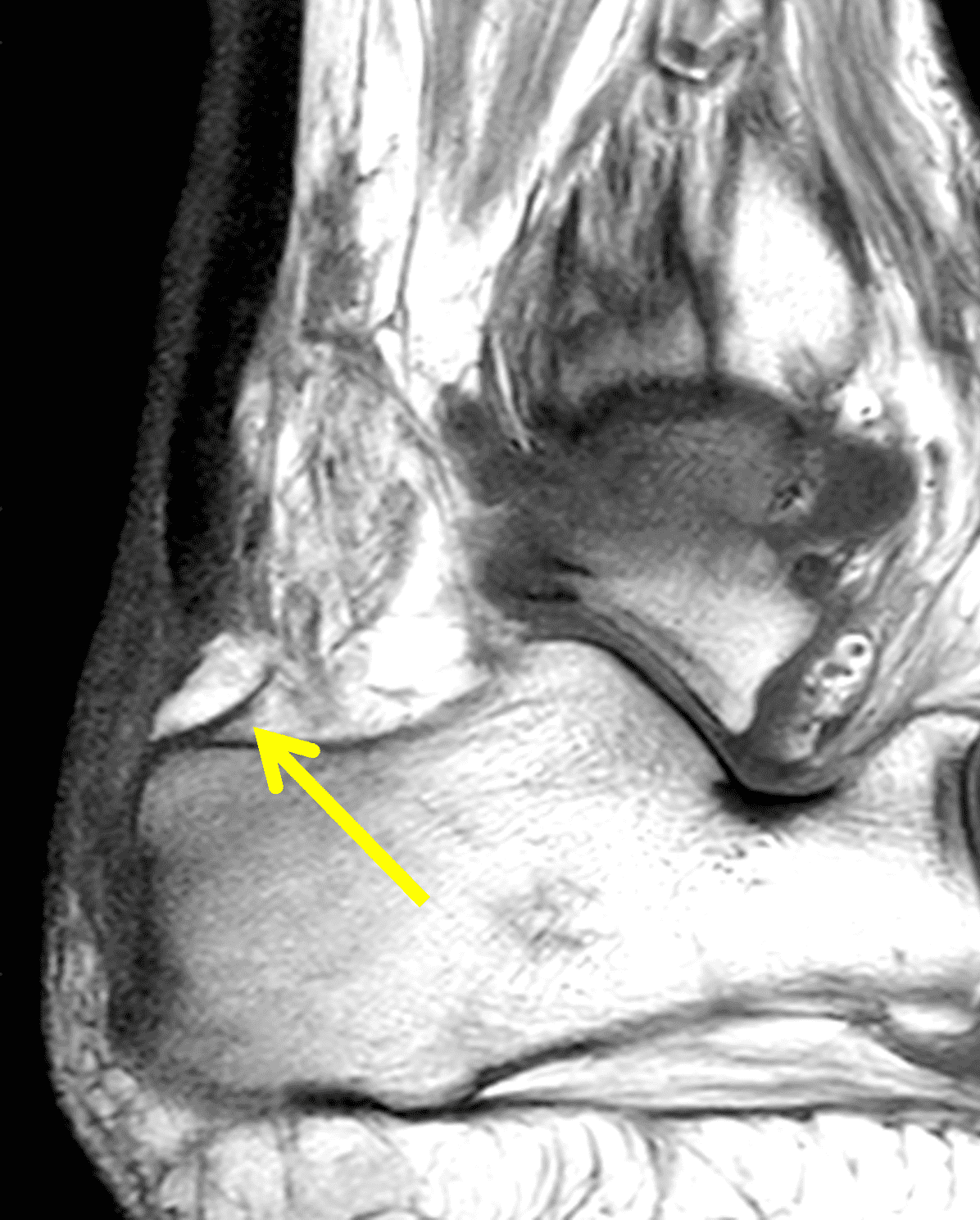
Figure 7: Distal Achilles tendon avulsion fracture in a 56 year-old man who stepped off his deck and felt a “pop” in his ankle with subsequent pain and swelling. (5A) Lateral radiograph demonstrates a retracted and rotated fracture fragment of the posterosuperior calcaneus (yellow arrow). Note the soft tissue swelling and indistinct contour of the Achilles tendon (black arrow). (5B) Sagittal fat-suppressed, T2-weighted image shows no tendinosis of the Achilles (arrowheads), soft tissue edema surrounding the fracture fragment (arrow), and marrow edema in the posterior calcaneus (asterisk). (7C) Sagittal T1-weighted image shows the retracted fracture fragment, rotated 180°, with cortical bone along the anterior aspect of the fragment (arrow).
Mid-Substance Tendon Tears
Mid-substance ruptures comprise the majority of Achilles tendon tears.28 Imaging evaluation of the mid-substance tear focuses on the completeness of the tear, defect size and location, surrounding tendon quality, identification of findings suggesting an acute or chronic injury, and surrounding soft tissue inflammation to help guide the surgeon in selecting appropriate management. Tears can be partial thickness (Figure 8) or full thickness (Figure 9). For full-thickness tears with a tendon gap less than 2 cm, primary repair is the standard treatment. For tears with gaps between 2 and 6 cm, a gastrocnemius lengthening procedure and/or a tendon graft (commonly using the flexor hallucis longus) are often necessary. Tears of greater than 6 cm have been addressed in a variety of manners including central third fascia slide with flexor hallucis longus transfer and turndown flap procedure.29
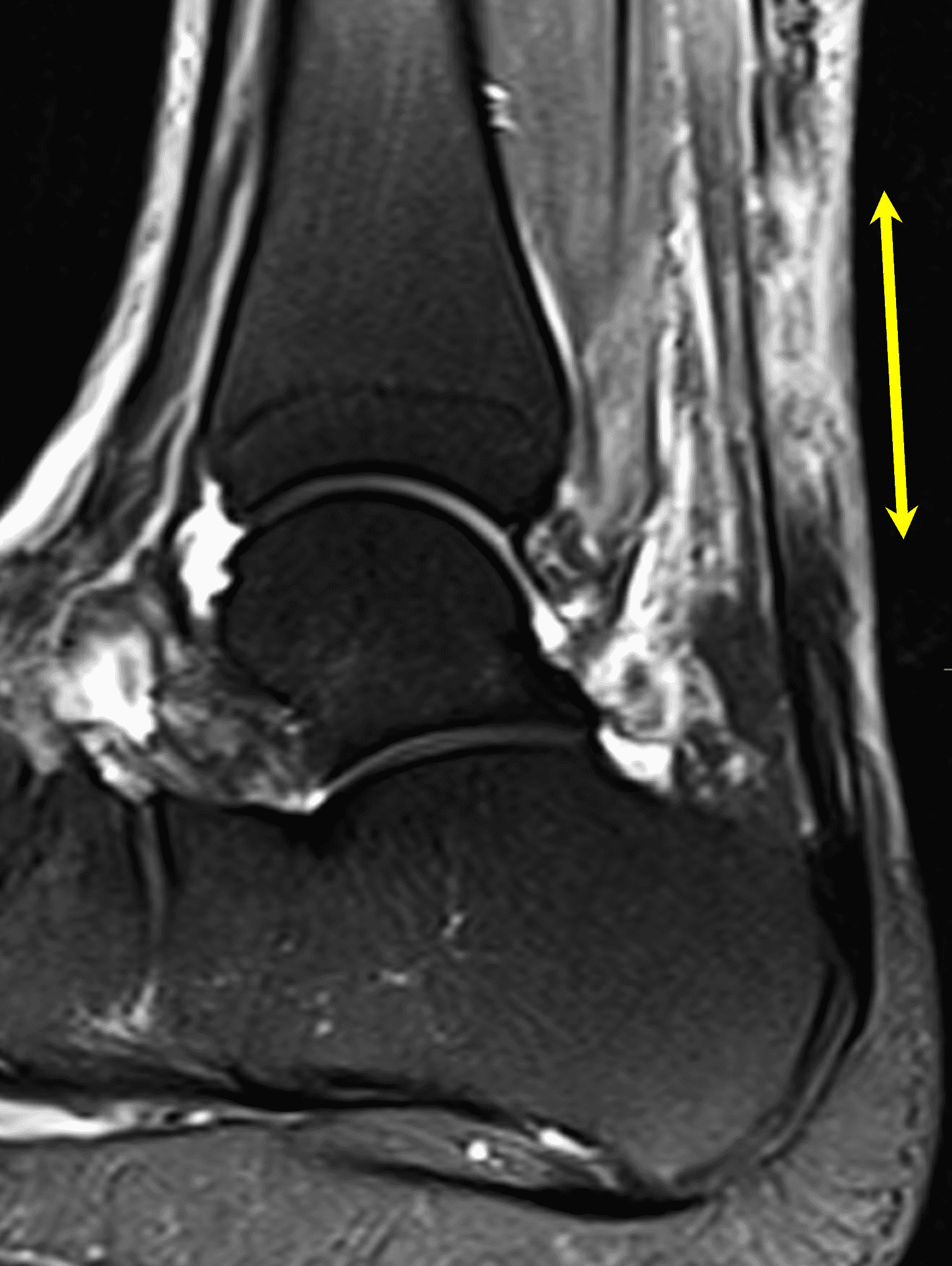
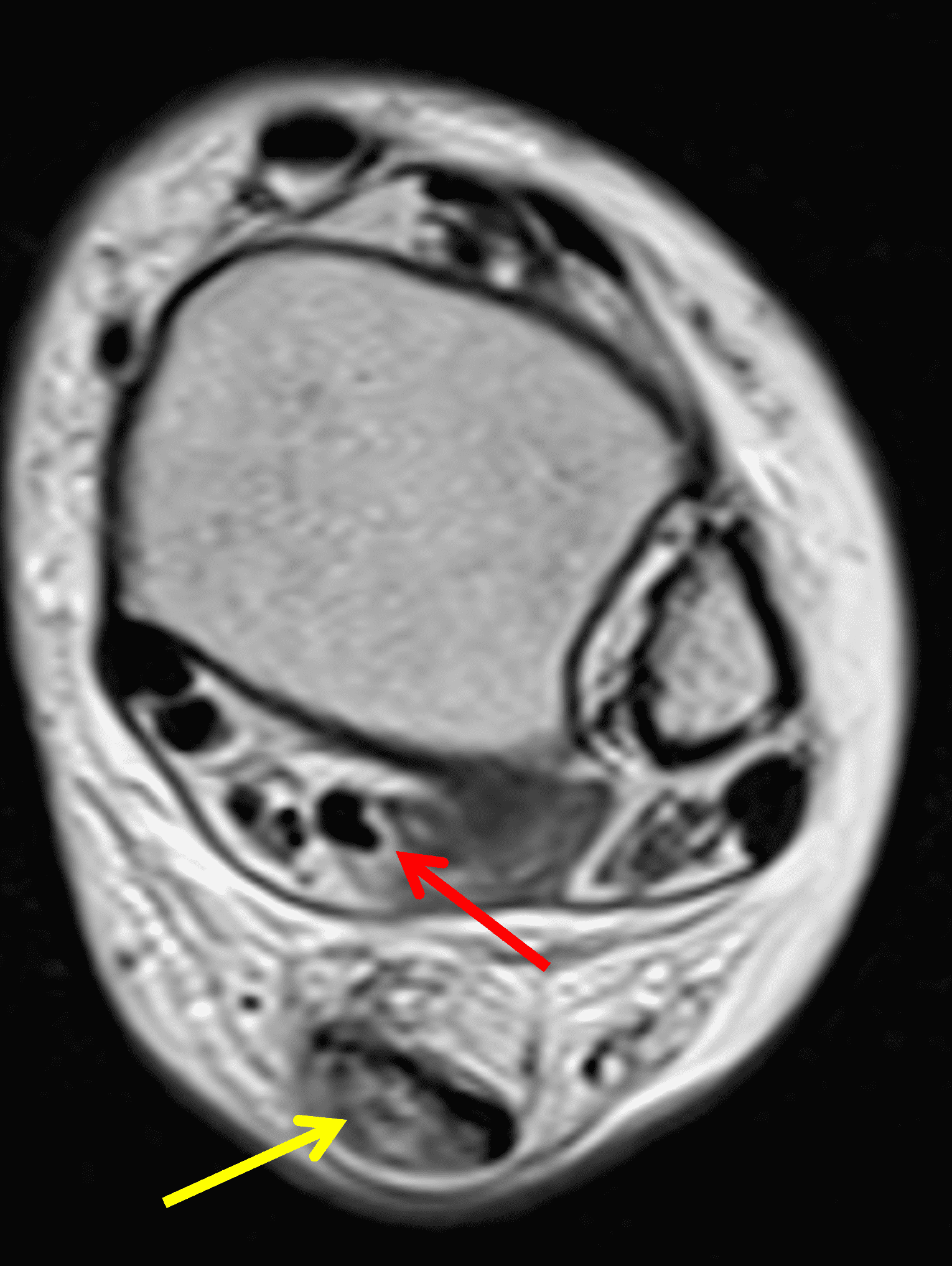
Figure 8: High-grade partial-thickness mid-substance Achilles tendon tear in a 50 year-old man who felt a “pop” while moving boxes 10 days prior. (8A) Sagittal fat-suppressed, T2-weighted image shows an ill-defined high-grade, partial tear of the mid tendon with a defect measuring 4.4 cm in length (arrow) and a background of moderate tendinosis. (8B) Transverse T2-weighted image demonstrates that the tear involves greater than 75% of the tendon cross section (yellow arrow). Note the normal-appearing flexor hallucis longus tendon (red arrow) that may be needed as a graft.
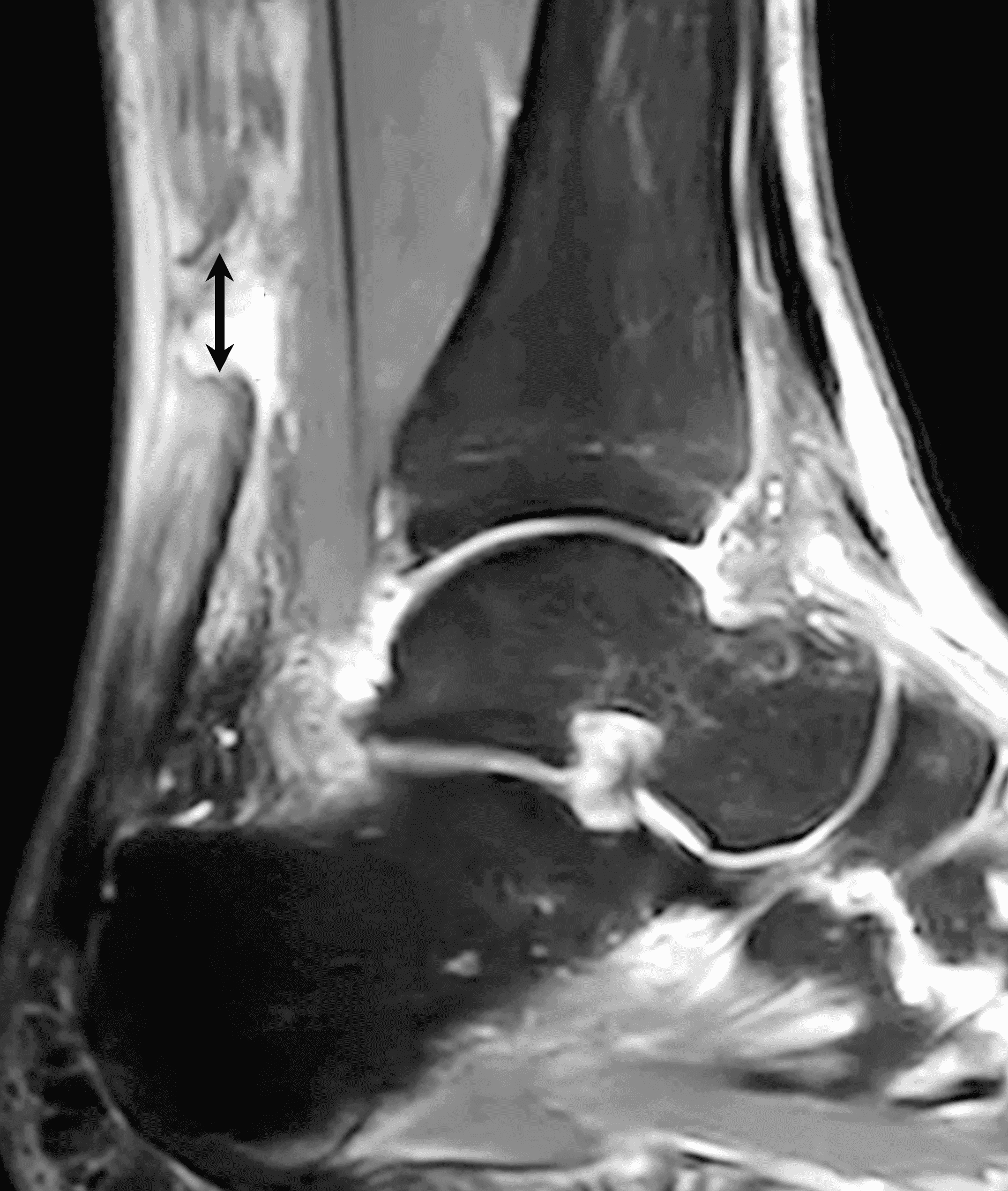
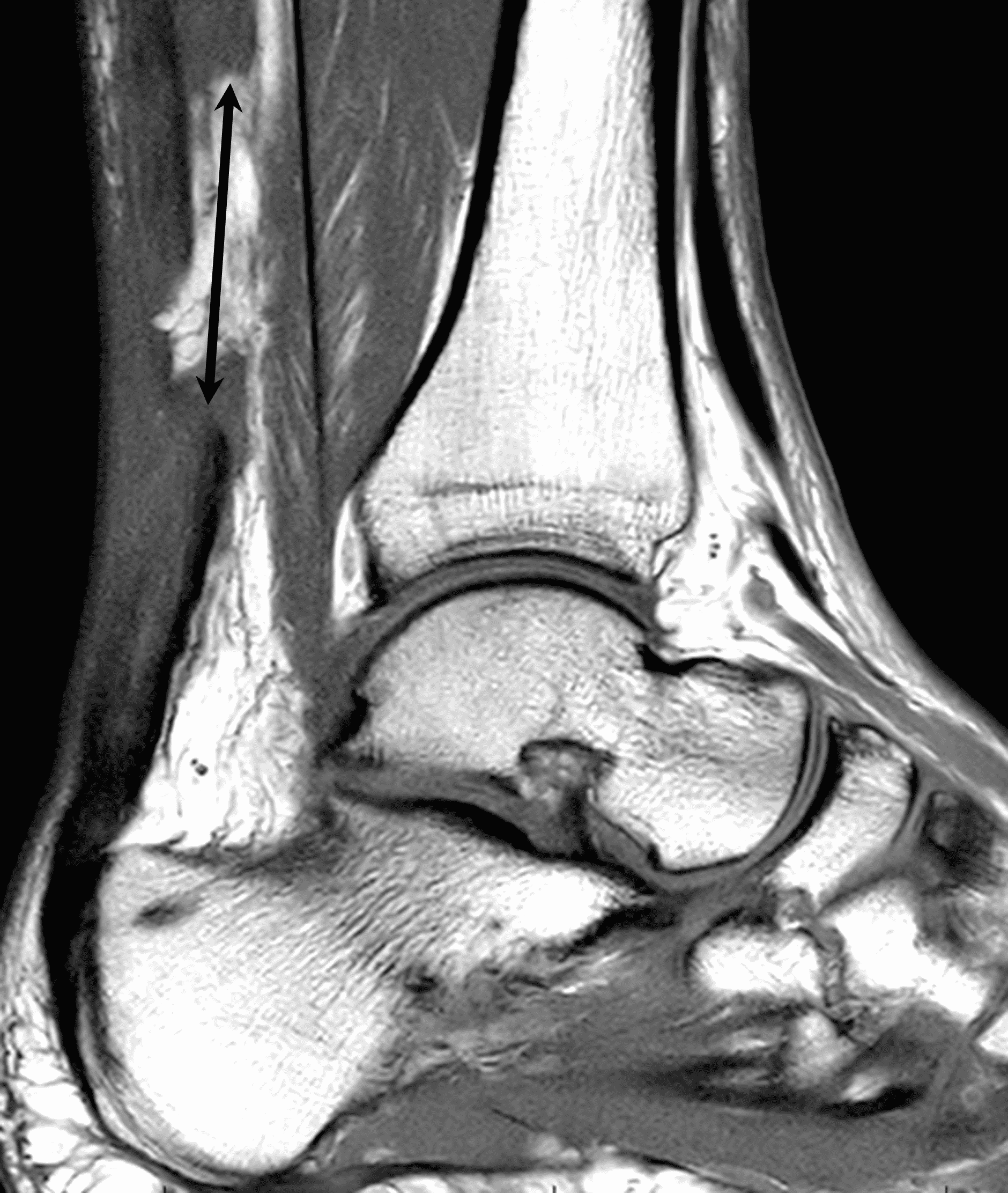
Figure 9: Full-thickness mid-substance Achilles tendon tear in a 48 year-old woman who felt a “pop” while running 11 days prior. (9A) Sagittal fat-suppressed, T2-weighted image reveals complete rupture of the mid tendon with a 1 cm fluid filled gap (arrow). The underlying tendon quality is poor with extensive degeneration. (9B) Sagittal T1-weighted image better estimates the effective tendon gap (2.5 cm, arrow) that the surgeon may need to close between the healthier-appearing tissue stumps.
Importantly, the radiologist should consider not only of the measurement of the fluid-filled defect, but also a functional “effective-gap” that takes into account the adjacent tendon quality. If the tendon stumps adjacent to the gap show severe degeneration, they may not be robust enough to hold sutures and the surgeon may need to debride the tendon ends before repair, creating a larger gap to address (Figure 9). Some surgeons also take into consideration whether the gap reduces with plantar flexion – in those patients, ultrasound examination may be useful to measure the gap in neutral position and with plantar flexion.
In patients with a prolonged clinical history, management of a mid-substance tear will differ depending on whether the tear is subacute or chronic. MRI findings suggesting that an injury is recent include fluid in the tendon gap, edema in Kager’s fat pad and the surrounding subcutaneous tissues, a strain in the distal soleus muscle belly, and the presence of subacute blood products. Conversely, a tendon gap that is filled with low signal-intensity granulation tissue or fibrosis, a torn tendon that is scarred to the surrounding structures (like the flexor hallucis longus muscle belly), or fatty atrophy in the distal soleus muscle belly are findings favoring chronicity. Heterotopic ossification in the Achilles tendon can be the result of a scarred, remote tear that has undergone metaplasia or may represent ossific tendinosis. Tendon ossification is commonly due to recurrent trauma and/or surgery, but may also be associated with medical conditions like diabetes, fluorosis, DISH, seronegative arthropathy, Wilson disease, renal failure, gout, and retinoid therapy.28 One relatively unusual pattern of chronic tendon tear on MRI is characterized by a central “core” of high-signal intensity replacing the tendon surrounded by an cylinder of low-signal intensity tissue that mimics intact tendon or thickened paratenon. In these cases, the peripheral tissue may represent chronic, elongated scar tissue (Figure 10).
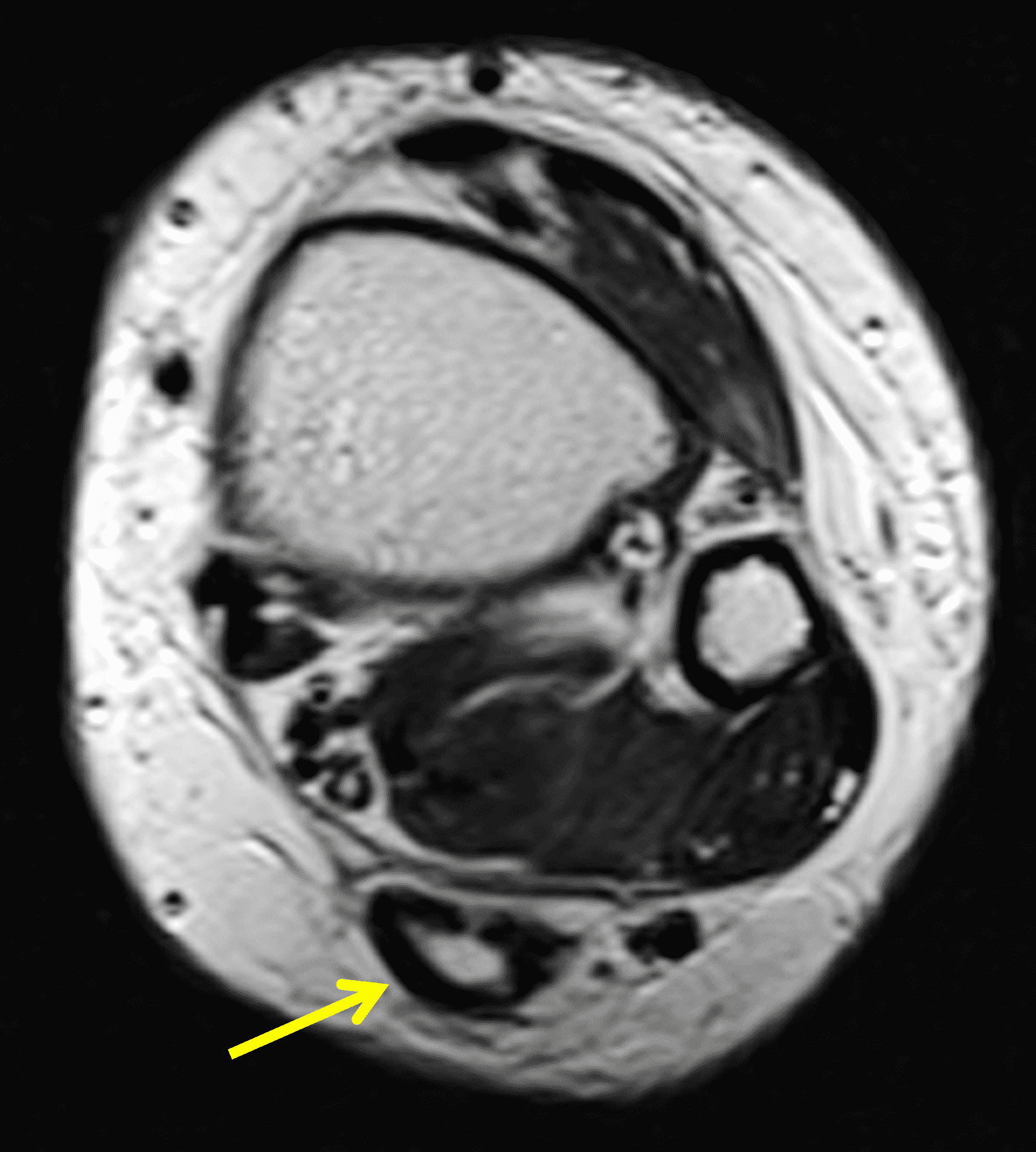
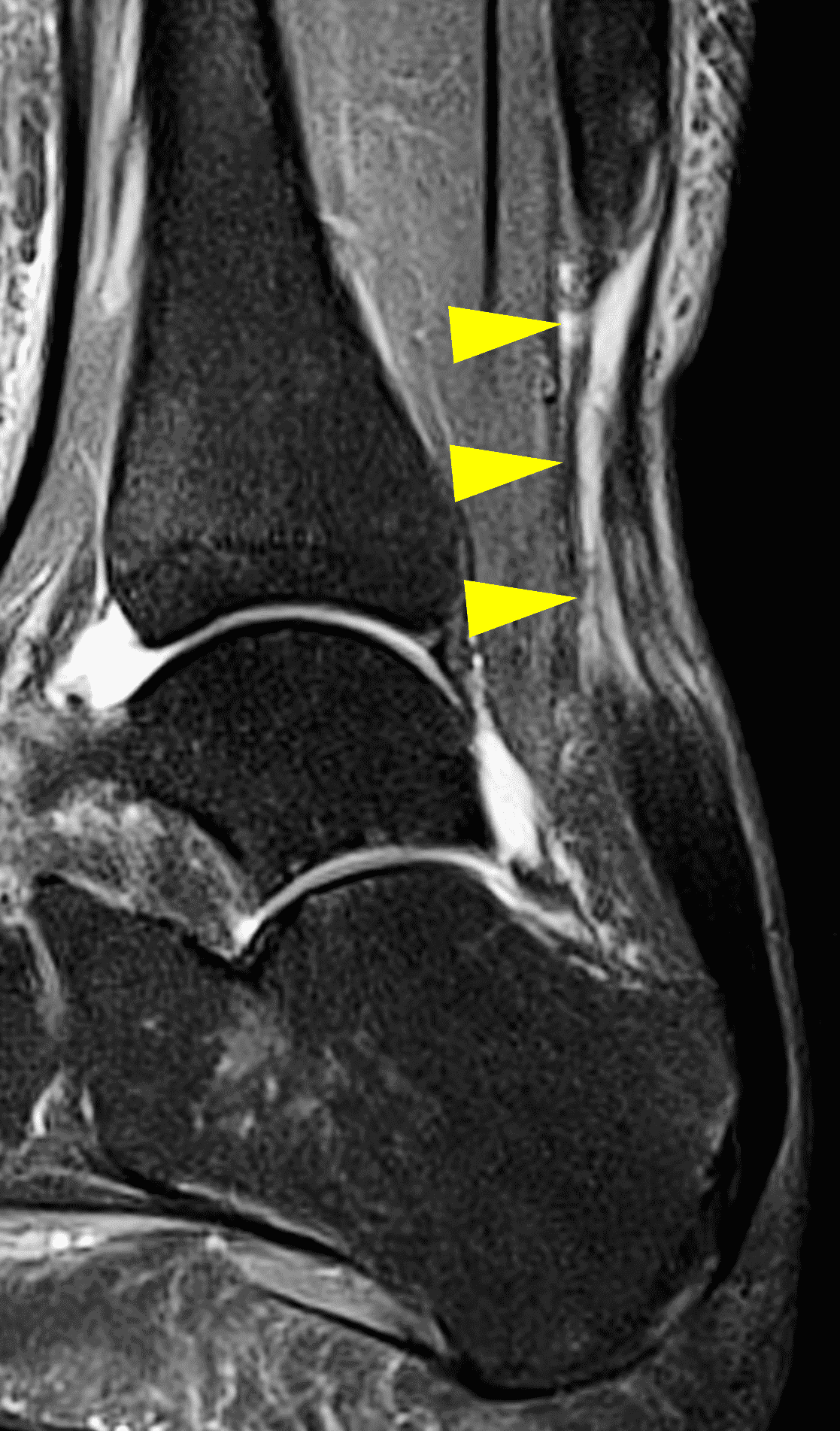

Figure 10: Chronic mid-substance Achilles tendon tear in a 57 year-old woman. (10A) Transverse T2-weighted image shows a central core of fluid-like signal surrounded by a shell of low signal intensity tissue (arrow). (10B) Sagittal STIR image shows a long, tubular defect in the central tendon with peripheral atrophic-appearing tissue (arrowheads). (10C) Surgery reveled a chronic “neglected” tear with extensive healing between the tendon stumps. Intra-operative photograph courtesy of John Hewitt, MD.
Myotendinous Junction Tears
The third important injury location is in the proximal Achilles at the myotendinous junction. While the initial clinical example was at the cranial aspect of the proximal tendon and was amenable to a mini-open or open procedure, tears located at the myotendinous junction are typically treated conservatively except in high-level athletes. A recent meta-analysis confirmed this practice pattern with 67 out 70 cases being treated non-operatively albeit with typical return to function of approximately 80% as assessed by heel rise. The three patients managed surgically were high-level athletes, two of whom returned to full sport and the third who resumed sport at 80% strength.30
In myotendinous tears, it is important to note the size of the gap and the appearance of the myotendinous junction (Figure 11). Recognize that proximal tears may not be completely included in the field-of-view of a standard ankle MR examination. In these cases, it may be necessary to move the coil more proximally and obtain additional images in the distal leg (Figure 12).


Figure 11: Achilles myotendinous junction tear in a 36 year-old. (11A) Sagittal STIR image shows a complete proximal tendon tear at the myotendinous junction with a 2 cm gap (arrow) and moderate diffuse tendinosis in the more distal tendon (arrowheads). (11B) Transverse fat-suppressed fluid-sensitive image also shows edema and degeneration of the myotendinous proximal stump (arrow). Due to the proximal location and extensive underlying tissue degeneration, the patient was not a candidate for surgical repair.
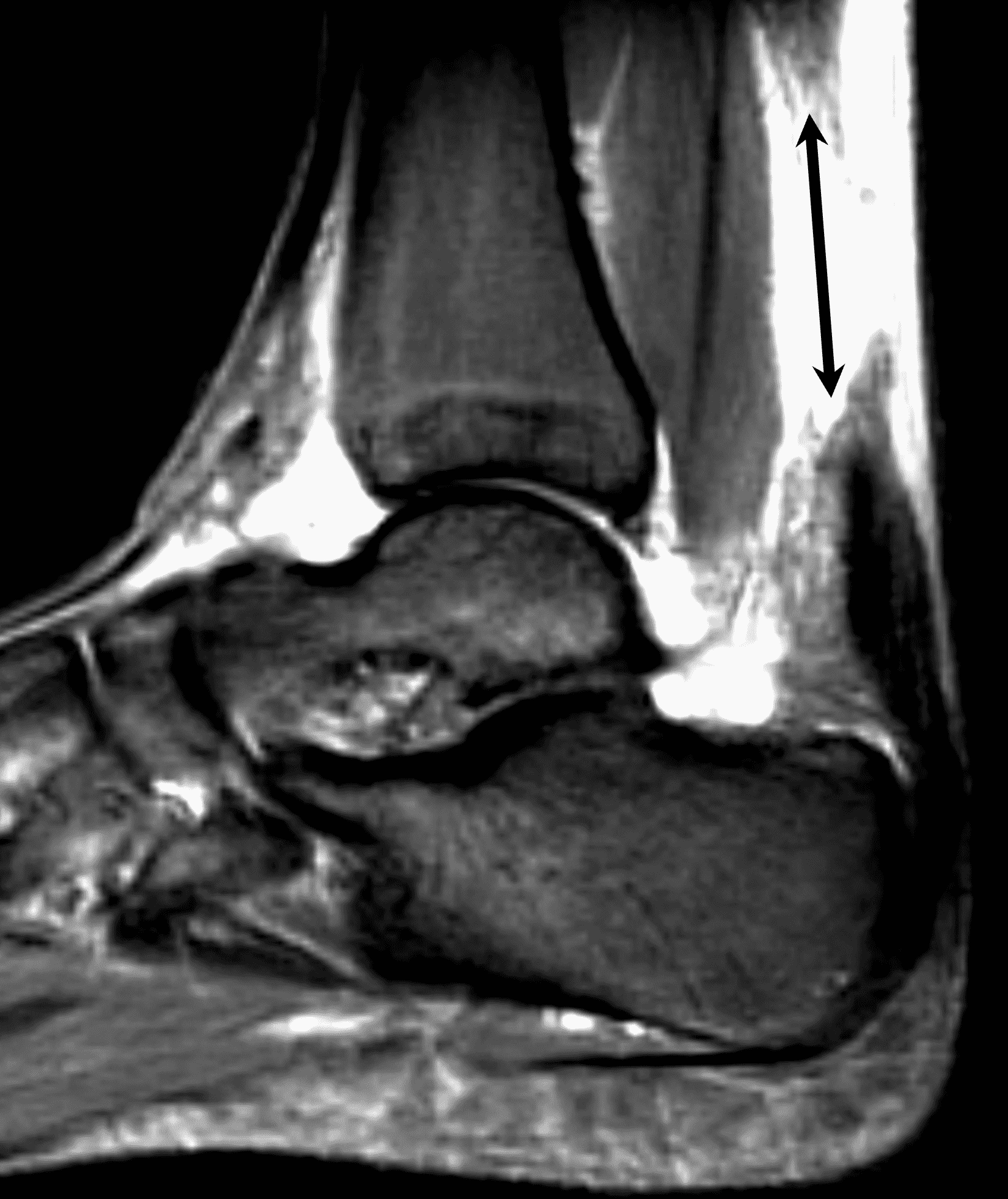

Figure 12: Complete myotendinous Achilles tear in a 17 year-old elite female gymnast. (12A) Initial sagittal STIR image from an ankle MRI shows a complete tendon rupture with a large tendon gap. The tissue proximal to the tear is not completely included, so it is unclear whether the tear is in the tendon substance or myotendinous. (12B) The patient returned for imaging of the distal leg where a sagittal STIR image more proximally shows that the tear is located at the myotendinous junction. m = distal soleus muscle, t = proximal tendon stump. Surgical repair was performed because the patient was a high-level athlete, but an open repair was necessary due to the myotendinous location.
Treatment
The treatment of Achilles tendon tears varies by location and is influenced by the patient’s clinical status. High-grade or persistent insertional tears are primarily treated with resection of any Haglund process and re-attachment of Achilles, but can also be allowed to heal without surgery if the tear is not retracted in poor operative candidates.24 Management of distal avulsions depends on the size of the fracture fragment with both open reduction, internal fixation and tenodesis employed.26,27 Tears at the myotendinous junction are typically treated conservatively outside of high-level athletes.30 If a myotendinous tear does undergo operative repair, an open procedure is usually needed. Options for treating mid-substance tears include non-operative management, open surgery, minimally invasive (mini-open) and percutaneous repairs.
Nonoperative management traditionally involved 6-8 weeks of cast immobilization in plantarflexion followed by gradual loading; current protocols emphasize early controlled motion and progressive weight-bearing to reduce re-rupture risk. Open surgery involves a 10 cm incision medial to the Achilles allowing excellent visualization of the tendon and is most useful in managing large defects. But open surgery comes with a greater risk of wound complications compared to procedures with a smaller incision, and wound complications can be particularly debilitating given the minimal soft tissue envelop surrounding the tendon.29,31,32 A variety of mini-open procedures, such as the percutaneous Achilles repair system (PARS) or Mini-SpeedBridge technique (which places anchors at the calcaneus), utilize a 3 cm incision located medial to the tendon at the level of rupture and can be used for smaller defects where primary end-to-end repair is possible, with resultant reduction in post-operative complications but comparable outcomes to open procedures.31,32,33,34 Percutaneous approaches have evolved over the past 3 decades with similar functional outcomes compared to open and mini-open procedures and decreased rates of infection compared to open procedures, but at the cost of greater sural nerve complications.30,35 A recently described percutaneous technique may reduce the risk of sural injury. 35
Both nonoperative and operative approaches can achieve favorable outcomes, although the optimal treatment strategy remains debated. A recent multicenter randomized trial of 526 patients found no significant differences in patient-reported outcomes (Achilles Tendon Total Rupture Score) at 12 months between nonoperative treatment, open repair, and minimally invasive surgery.36 Meta-analyses consistently show higher re-rupture rates with nonoperative treatment (range 2–12%) compared to surgery (1–2%), though nonoperative management avoids surgical complications such as wound breakdown, infection, and sural nerve injury.36,37 Patient selection considers activity level, medical comorbidities, soft tissue quality, and the degree of tendon retraction. Active individuals and elite athletes often opt for surgery, whereas sedentary patients or those with significant comorbidities may favor non-operative treatment.
Summary
The Achilles is the largest and strongest tendon as well as one of the most frequently injured in a wide range of ages. Tear location can be categorized as insertional, mid-substance, or myotendinous junction. Imaging should evaluate the tear location, defect size, degree of underlying tendon degeneration, and adjacent soft tissues as well as findings of chronicity. Proper MRI evaluation can assist the surgeon in selecting the most appropriate treatment.
References
- Huttunen TT, Kannus P, Rolf C, Felländer-Tsai L, Mattila VM. Acute achilles tendon ruptures: incidence of injury and surgery in Sweden between 2001 and 2012. Am J Sports Med. 2014;42(10):2419–2423. doi:10.1177/0363546514540599 ↩
- Jarvinen TA, Kannus P, Maffulli N, Khan KM. Achilles tendon disorders: etiology and epidemiology. Foot Ankle Clin. 2005;10(2):255–266. doi:10.1016/j.fcl.2005.01.013 ↩
- Hess GW. Achilles tendon rupture: a review of etiology, population, anatomy, risk factors, and injury prevention. Foot Ankle Spec. 2010;3(1):29–32. doi:10.1177/1938640009355191 ↩
- Gould HP, Bano JM, Akman JL, Fillar AL. Postoperative Rehabilitation Following Achilles Tendon Repair: A Systematic Review. Sports Med Arthrosc Rev. 2021;29(2):130–145. doi:10.1097/JSA.0000000000000309 ↩
- Flores DV, Goes PK, Damer A, Huang BK. The Heel Complex: Anatomy, Imaging, Pathologic Conditions, and Treatment. Radiographics. 2024;44(4):e230163. doi:10.1148/rg.230163 ↩
- Marshall H, Howarth C, Larkman DJ, Herlihy AH, Oatridge A, Bydder GM. Contrast-enhanced magic-angle MR imaging of the Achilles tendon. AJR Am J Roentgenol. 2002;179(1):187–192. doi:10.2214/ajr.179.1.1790187 ↩
- O’Brien M. The anatomy of the Achilles tendon. Foot Ankle Clin. 2005;10(2):225–238. doi:10.1016/j.fcl.2005.01.011 ↩
- Cummins EJ, Anson BJ, et al. The structure of the calcaneal tendon (of Achilles) in relation to orthopedic surgery, with additional observations on the plantaris muscle. Surg Gynecol Obstet. 1946;83107–116. ↩
- Edama M, Kubo M, Onishi H, Takabayashi T, Inai T, Yokoyama E, et al. The twisted structure of the human Achilles tendon. Scand J Med Sci Sports. 2015;25(5):e497–503. doi:10.1111/sms.12342 ↩
- Ballal MS, Walker CR, Molloy AP. The anatomical footprint of the Achilles tendon: a cadaveric study. Bone Joint J. 2014;96-B(10):1344–1348. doi:10.1302/0301-620X.96B10.33771 ↩
- Mahan J, Damodar D, Trapana E, Barnhill S, Nuno AU, Smyth NA, et al. Achilles tendon complex: The anatomy of its insertional footprint on the calcaneus and clinical implications. J Orthop. 2020;17221–227. doi:10.1016/j.jor.2019.06.008 ↩
- Snow SW, Bohne WH, DiCarlo E, Chang VK. Anatomy of the Achilles tendon and plantar fascia in relation to the calcaneus in various age groups. Foot Ankle Int. 1995;16(7):418–421. doi:10.1177/107110079501600707 ↩
- Zwirner J, Zhang M, Ondruschka B, Akita K, Hammer N. An ossifying bridge – on the structural continuity between the Achilles tendon and the plantar fascia. Sci Rep. 2020;10(1):14523. doi:10.1038/s41598-020-71316-z ↩
- Chen TM, Rozen WM, Pan WR, Ashton MW, Richardson MD, Taylor GI. The arterial anatomy of the Achilles tendon: anatomical study and clinical implications. Clin Anat. 2009;22(3):377–385. doi:10.1002/ca.20758 ↩
- Sookur PA, Naraghi AM, Bleakney RR, Jalan R, Chan O, White LM. Accessory muscles: anatomy, symptoms, and radiologic evaluation. Radiographics. 2008;28(2):481–499. doi:10.1148/rg.282075064 ↩
- Luck MD, Gordon AG, Blebea JS, Dalinka MK. High association between accessory soleus muscle and Achilles tendonopathy. Skeletal Radiol. 2008;37(12):1129–1133. doi:10.1007/s00256-008-0554-0 ↩
- Jackson LJ, Serhal M, Omar IM, Garg A, Michalek J, Serhal A. Sural nerve: imaging anatomy and pathology. Br J Radiol. 2023;96(1141):20220336. doi:10.1259/bjr.20220336 ↩
- Cohen JC. Anatomy and biomechanical aspects of the gastrocsoleus complex. Foot Ankle Clin. 2009;14(4):617–626. doi:10.1016/j.fcl.2009.08.006 ↩
- Komi PV. Relevance of in vivo force measurements to human biomechanics. J Biomech. 1990;23 Suppl 123–34. doi:10.1016/0021-9290(90)90038-5 ↩
- Koivunen-Niemela T, Parkkola K. Anatomy of the Achilles tendon (tendo calcaneus) with respect to tendon thickness measurements. Surg Radiol Anat. 1995;17(3):263–268. doi:10.1007/BF01795061 ↩
- Garras DN, Raikin SM, Bhat SB, Taweel N, Karanjia H. MRI is unnecessary for diagnosing acute Achilles tendon ruptures: clinical diagnostic criteria. Clin Orthop Relat Res. 2012;470(8):2268–2273. doi:10.1007/s11999-012-2355-y ↩
- Thompson TC, Doherty JH. Spontaneous rupture of tendon of Achilles: a new clinical diagnostic test. J Trauma. 1962;2126–129. doi:10.1097/00005373-196203000-00003 ↩
- Park YH, Lim JW, Choi GW, Kim HJ. Quantitative Magnetic Resonance Imaging Analysis of the Common Site of Acute Achilles Tendon Rupture: 5 to 8 cm Above the Distal End of the Calcaneal Insertion. Am J Sports Med. 2019;47(10):2374–2379. doi:10.1177/0363546519858990 ↩
- Tourne Y, Baray AL, Barthelemy R, Karhao T, Moroney P. The Zadek calcaneal osteotomy in Haglund’s syndrome of the heel: Clinical results and a radiographic analysis to explain its efficacy. Foot Ankle Surg. 2022;28(1):79–87. doi:10.1016/j.fas.2021.02.001 ↩
- El-Khoury GY, Kathol MH. Neuropathic fractures in patients with diabetes mellitus. Radiology. 1980;134(2):313–316. doi:10.1148/radiology.134.2.7352207 ↩
- Takahashi Y, Takegami Y, Tokutake K, Asami Y, Takahashi H, Kato M, et al. Analysis of Calcaneal Avulsion Fractures Treated Surgically and Nonsurgically: A Retrospective Multicenter Study. JB JS Open Access. 2024;9(3). doi:10.2106/JBJS.OA.23.00127 ↩
- Liu Z, Hou G, Zhang W, Lin J, Yin J, Chen H, et al. Calcaneal tuberosity avulsion fractures – A review. Injury. 2024;55(2):111207. doi:10.1016/j.injury.2023.111207 ↩
- Arora AJ, Arora R. Ossification of the bilateral Achilles tendon: a rare entity. Acta Radiol Open. 2015;4(9):2058460115599184. doi:10.1177/2058460115599184 ↩
- Roebke LJ, Alvarez PM, Curatolo C, Palumbo R, Martin KD. Chronic Achilles Tendon Avulsion Repair: Central Third Fascia Slide Technique with Flexor Hallucis Longus Transfer. JBJS Essent Surg Tech. 2024;14(1). doi:10.2106/JBJS.ST.22.00036 ↩
- Lameire DL, Ramelli L, Halai M, Wasserstein D, Park SS. Outcomes of operative and nonoperative management of myotendinous Achilles tendon ruptures: a systematic review. BMC Musculoskelet Disord. 2025;26(1):71. doi:10.1186/s12891-025-08286-8 ↩
- Meulenkamp B, Woolnough T, Cheng W, Shorr R, Stacey D, Richards M, et al. What Is the Best Evidence to Guide Management of Acute Achilles Tendon Ruptures? A Systematic Review and Network Meta-Analysis of Randomized Controlled Trials. Clin Orthop Relat Res. 2021;479(10):2119–2131. doi:10.1097/CORR.0000000000001861 ↩
- Miller CP, Stanwood K, Williams C, Zhao J, Raduan F. The Medial Mini-Open Supine Achilles Repair: Outcomes of a Medially Based Mini-Open Technique Compared With Prone Techniques. J Am Acad Orthop Surg Glob Res Rev. 2025;9(3). doi:10.5435/JAAOSGlobal-D-24-00390 ↩
- Peabody JJ, Hadley SM, Jr., Bergman R, Westvold SJ, Olamigoke FO, Chang S, et al. Functional outcomes following minimally invasive Achilles rupture repair: a retrospective comparative study of PARS and midsubstance speedbridge techniques. J Orthop Surg Res. 2025;20(1):390. doi:10.1186/s13018-025-05748-6 ↩
- Lawson J, Tarapore R, Sequeira S, Imbergamo C, Tarka M, Guyton G, et al. Open and Percutaneous Approaches Have Similar Biomechanical Results for Primary Midsubstance Achilles Tendon Repair: A Meta-analysis. Arthrosc Sports Med Rehabil. 2024;6(3):100924. doi:10.1016/j.asmr.2024.100924 ↩
- Maffulli N, Sammaria G, Ziello S, Migliorini F, Oliva F. Percutaneous cruciate repair of ruptured Achilles tendon. J Orthop Surg Res. 2023;18(1):677. doi:10.1186/s13018-023-04167-9 ↩
- Myhrvold SB, Brouwer EF, Andresen TKM, Rydevik K, Amundsen M, Grun W, et al. Nonoperative or Surgical Treatment of Acute Achilles’ Tendon Rupture. N Engl J Med. 2022;386(15):1409–1420. doi:10.1056/NEJMoa2108447 ↩
- Ochen Y, Beks RB, van Heijl M, Hietbrink F, Leenen LPH, van der Velde D, et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ. 2019;364k5120. doi:10.1136/bmj.k5120 ↩
