Clinical History
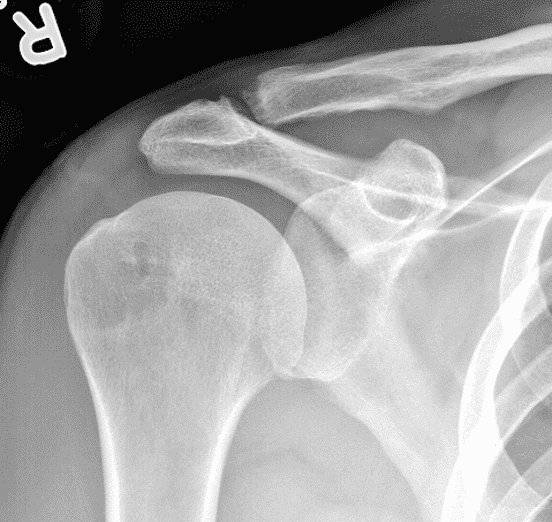
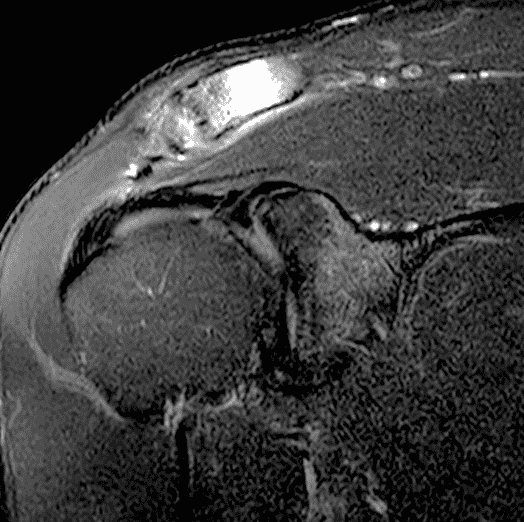
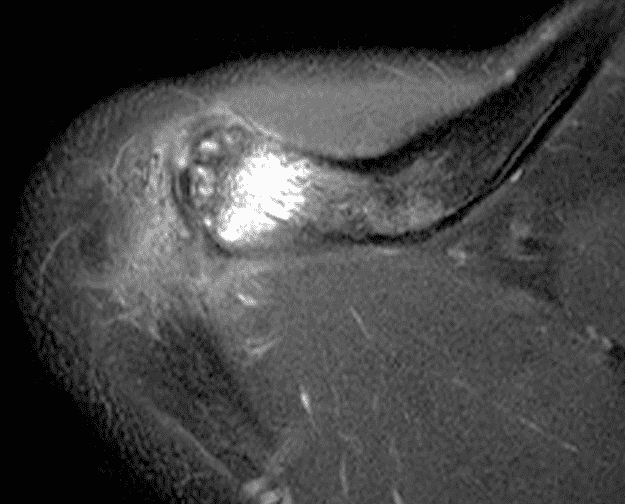
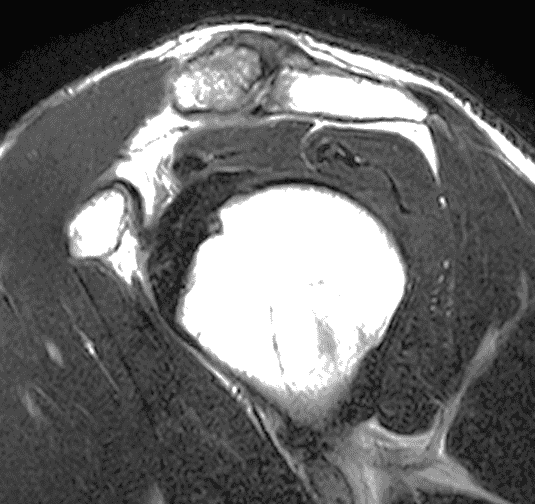
A 49-year-old male, avid weightlifter complains of chronic pain along the superior aspect of his right shoulder. He denies acute trauma. An AP radiograph (Figure 1A), as well as oblique coronal SPAIR (Figure 1B), axial fat-suppressed fluid sensitive (Figure 1C), and oblique sagittal T2-weighted images (Figure 1D) are shown. What are the findings? What is your diagnosis?
Findings

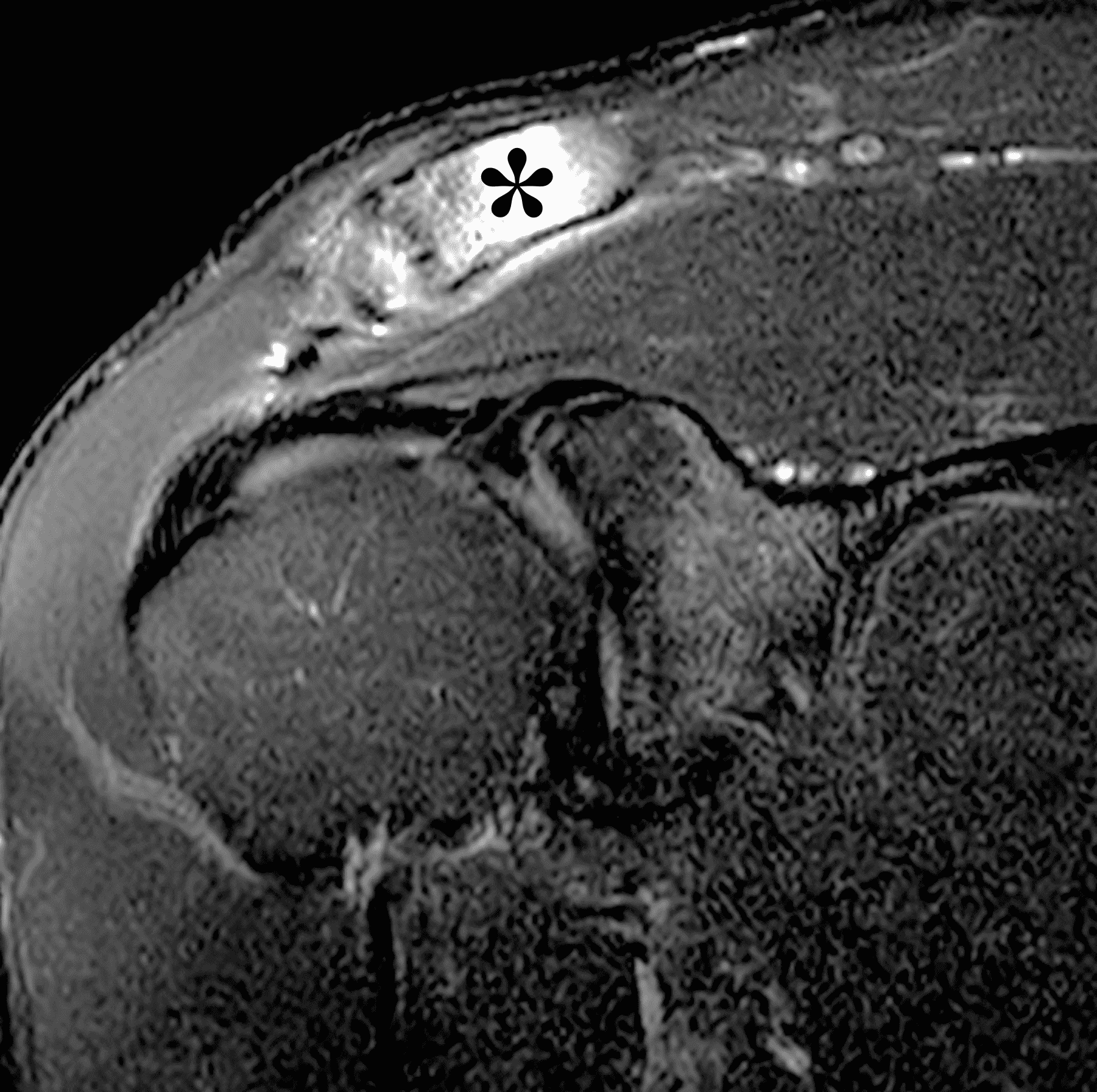
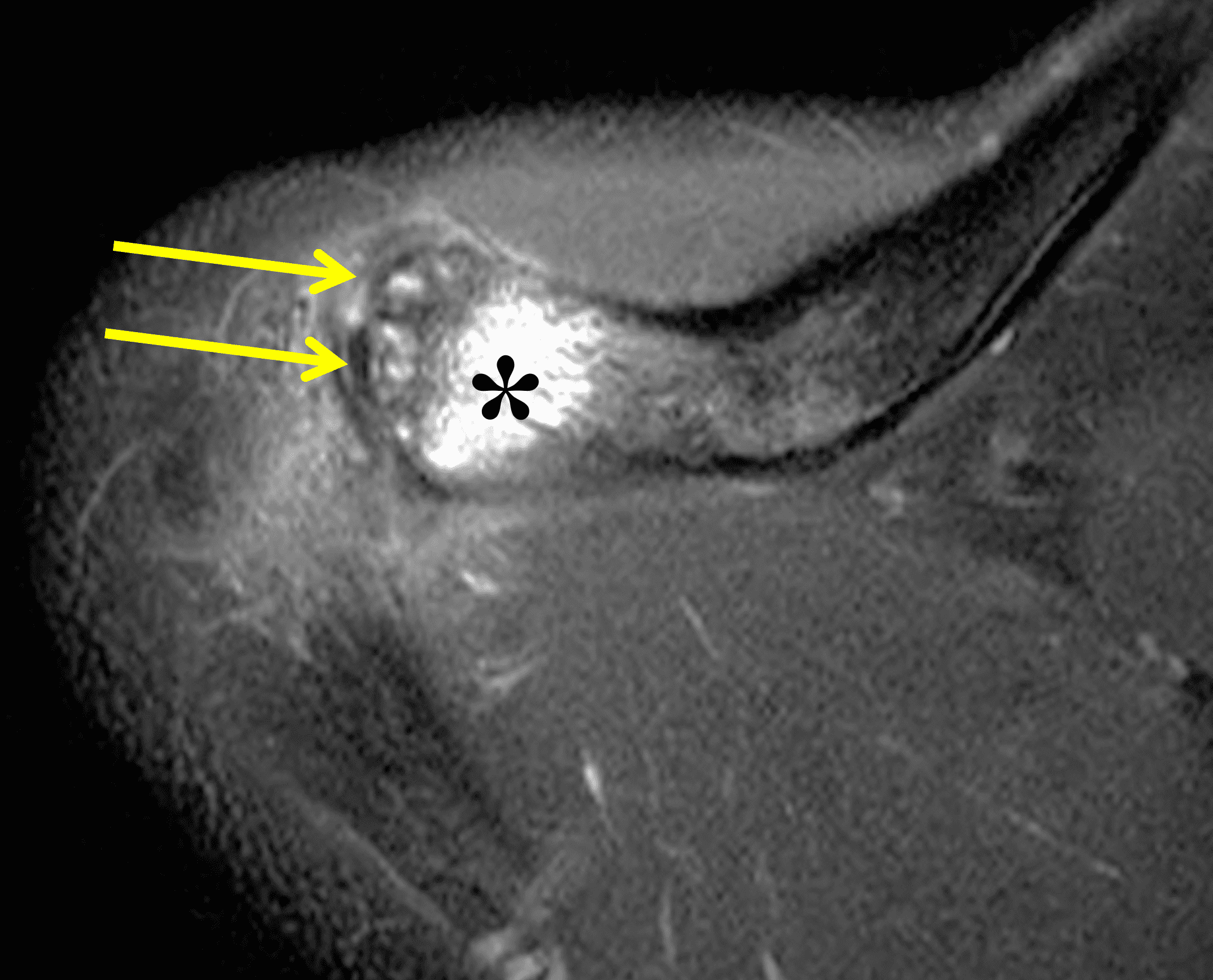
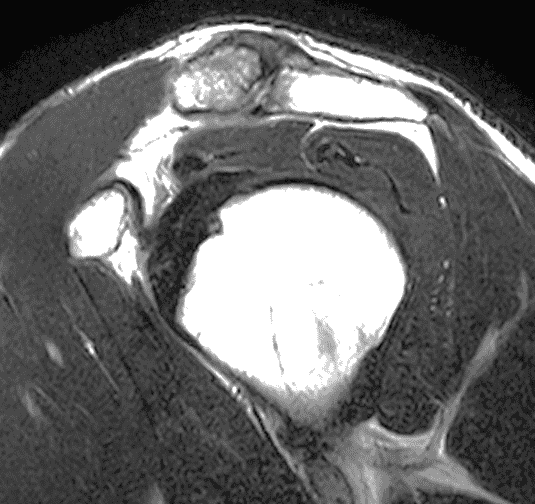
Figure 2: The radiograph (2A) shows bone resorption and small cysts in the distal clavicle (arrow) without joint narrowing or osteophytes. High signal intensity marrow edema is present in the distal clavicle (asterisk) on the oblique coronal SPAIR image (2B). The axial fat-suppressed fluid-sensitive image (2C) confirms the marrow edema (asterisk) and shows small cysts/erosions in the distal clavicle (arrows). On the oblique sagittal T2-weighted image (2D), note the lack of osteophytes.
Diagnosis
Distal clavicular osteolysis with marrow edema related to stress/overuse.
Introduction
Distal clavicular osteolysis (DCO) refers to painful, post-traumatic inflammatory resorption of bone at the distal end of the clavicle. DCO primarily occurs in two contexts. Chronic resorption of the distal clavicle was initially described as a complication following acute trauma, such as an acromioclavicular dislocation.1, 2 More commonly, however, DCO is the result of overuse with repetitive microtrauma to the distal clavicle typically encountered in athletes.3 Histologic studies have shown both Inflammatory infiltrate and evidence of hyperemia.4 Predisposing activities include anterior or overhead pressing activities often encountered during weight training (especially bench press, dips, and chest flies), American football, and calisthenic workouts (e.g., pushups).5 Chronic DCO has also been described in rowers, gymnasts, and occupations that incorporate repetitive press type activities.6 The condition is most common in young adults. Men are affected more commonly than women.7 Bilateral involvement has been reported.
While the specific mechanism that leads to the development of DCO is not entirely understood, the weight and frequency of load bearing has been correlated to the development and severity of the condition in weightlifters. Also implicated is bench press technique that includes excessive shoulder extension with the elbows positioned posterior to the mid axillary line during the loading phase of the exercise.
Several authors have proposed chronic resorption during the healing response of a distal clavicle stress fracture as the underlying cause of DCO.3, 8 While controversial, this mechanism explains some of the imaging findings encountered in these patients. DCO can also be secondary to metabolic or inflammatory processes (see differential diagnosis, below).
Relevant Anatomy
Knowledge of the normal acromioclavicular (AC) joint anatomy aids in understanding the pathophysiology of DCO and recognizing relevant imaging features of the condition. The AC joint is a synovial (diarthrodial) joint at the junction between the anteromedial aspect of the acromion and the distal end of the clavicle. The articular surfaces are relatively flat and designed to allow gliding motion between the two bones during a wide range of arm movement. For most activities, the relatively mobile scapula glides with respect to a fixed clavicle.
A small articular fibrocartilage disk lies interposed between the articular surfaces, and the joint is surrounded by a tough fibrous joint capsule. The acromioclavicular ligaments are focal thickenings of the AC joint capsule that run transversely along the anterior, posterior, superior, and inferior aspects of the joint. These ligaments resist displacement of the distal clavicle and acromion with respect to one another during stress loading of the upper extremity. Additionally, the conoid and trapezoid components of the coracoclavicular ligaments resist cranial displacement of the distal clavicle with respect to the acromion.6 Finally, the AC joint capsule is lined by synovium and its joint cavity typically contains a small amount of synovial fluid.
Imaging findings
Patients with DCO often present with shoulder pain that is exacerbated by pressing movements and localizes to the region of the AC joint. These symptoms are often nonspecific and can mimic rotator cuff disease, impingement, and subacromial-subdeltoid bursitis, in addition to more common disorders of the AC joint such as osteoarthritis.
Radiographs: Initial radiographs may be normal or show features of other common unrelated AC joint pathology such as osteoarthritis. As inflammation and hyperemia in the distal clavicle progresses, bone density in the distal clavicle can decrease with indistinctness or discontinuity of the subchondral bone plate (Figure 3). This so-called resorptive phase may also include frank erosions in the distal clavicle or a faint sclerotic line in the medullary space of the distal clavicle parallel to the bone end. Varying degrees of surrounding soft tissue swelling may be visible. Later, during the late healing phase when symptoms have usually resolved, the distal clavicle may return to a normal radiographic appearance; a sclerotic line parallel to the distal bone end is visible after healing in some cases (Figure 4). In patients with severe initial bone loss, re-cortication of the resorbed bone and erosions can occur leaving residual bone loss and contour defects in the distal clavicle. While it is typically not a primary modality for the diagnosis of DCO, CT demonstrates the same bone findings as radiographs.
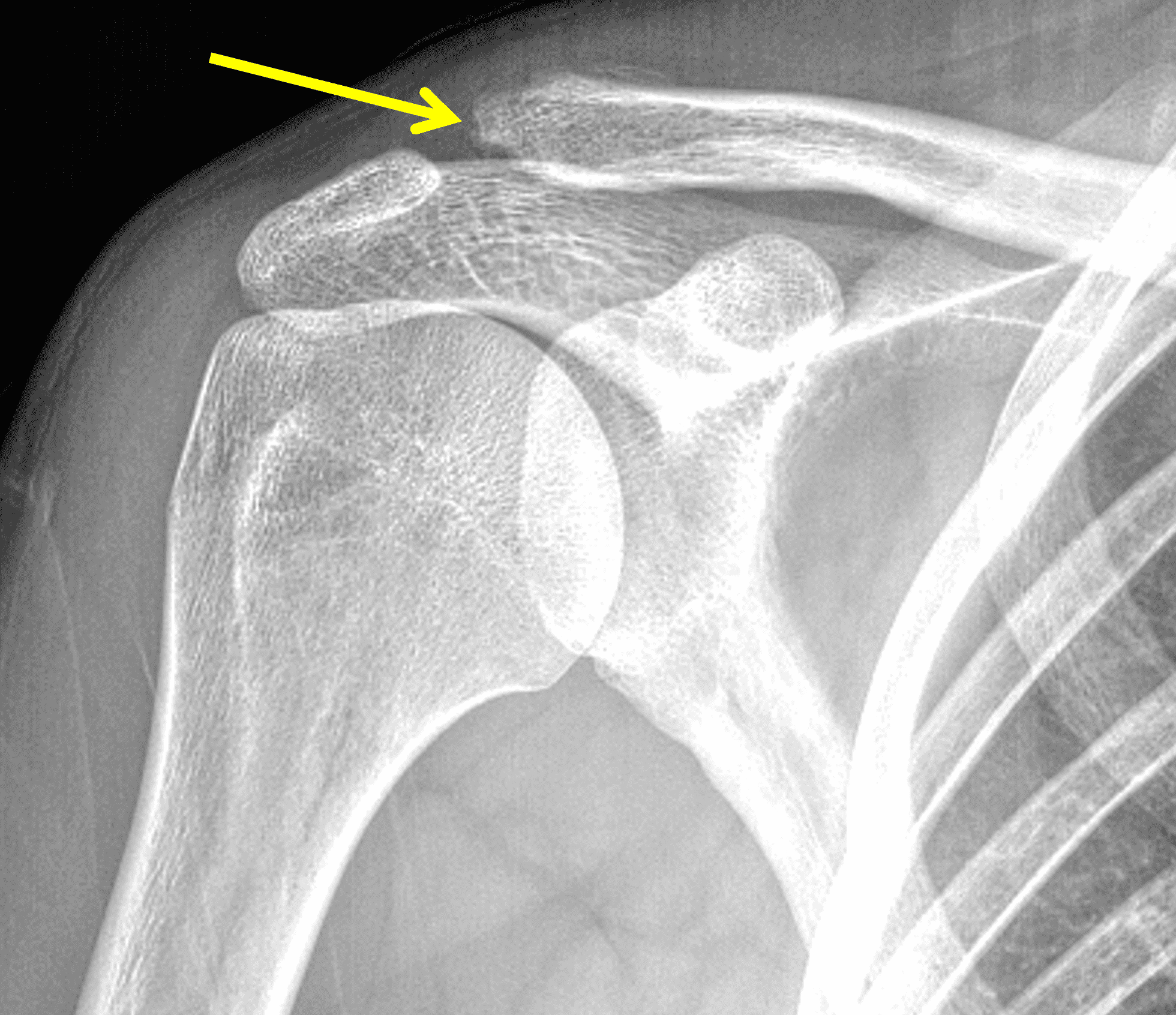
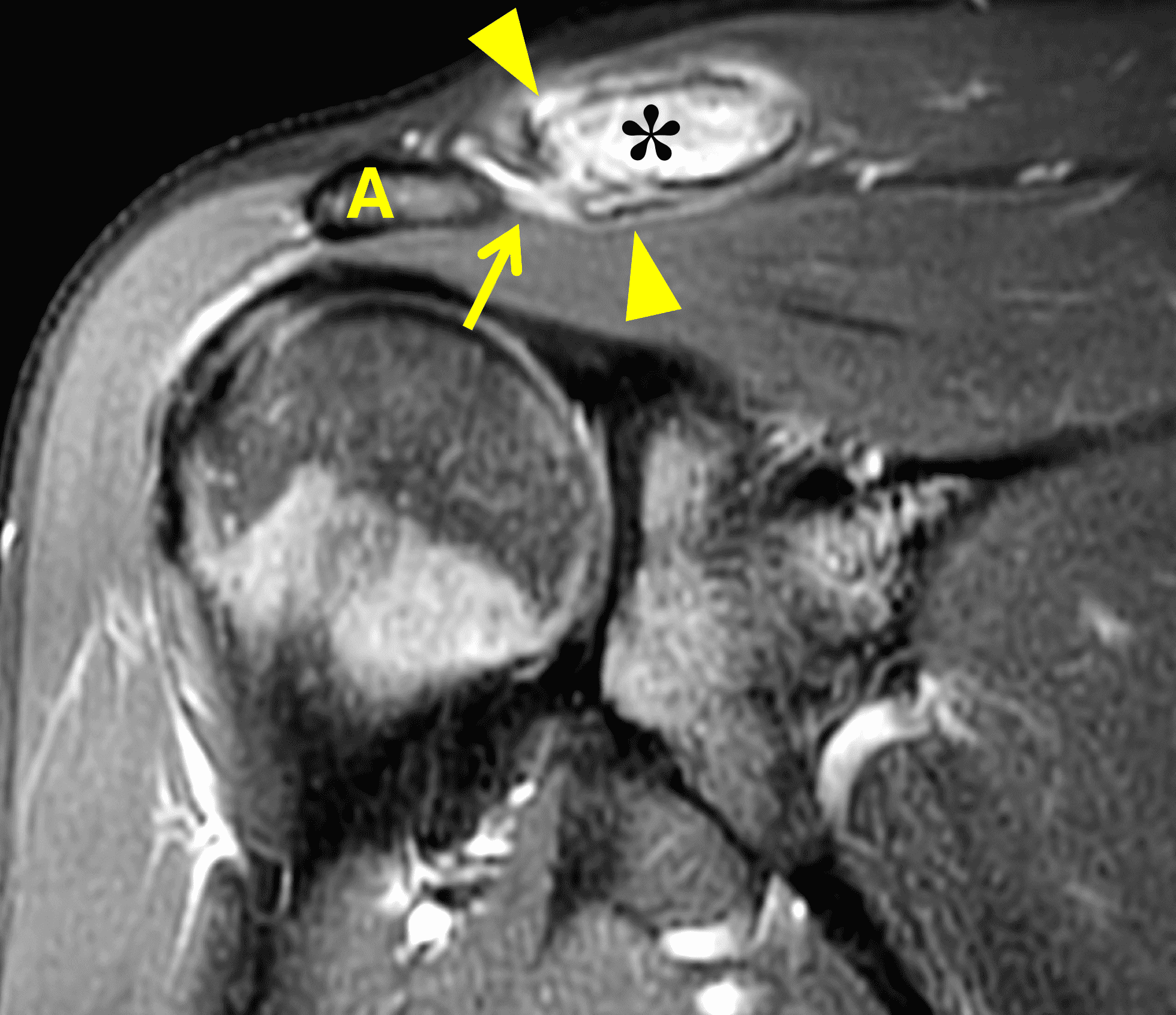
Figure 3: 18-year-old female soccer goalie with chronic pain over the acromioclavicular (AC) joint. (3A) An AP radiograph shows a “whittled” appearance to the distal clavicle (arrow) due to cortical and trabecular bone resorption. (3B) An oblique coronal fat-suppressed proton-density weighted image shows marrow edema in the distal clavicle (asterisk), with associated surrounding periosteal edema (arrowheads) and a small effusion or mild synovitis in the AC joint (arrow). The adjacent acromion (A) appears normal. Distal clavicular osteolysis is much less common in female compared to male athletes.
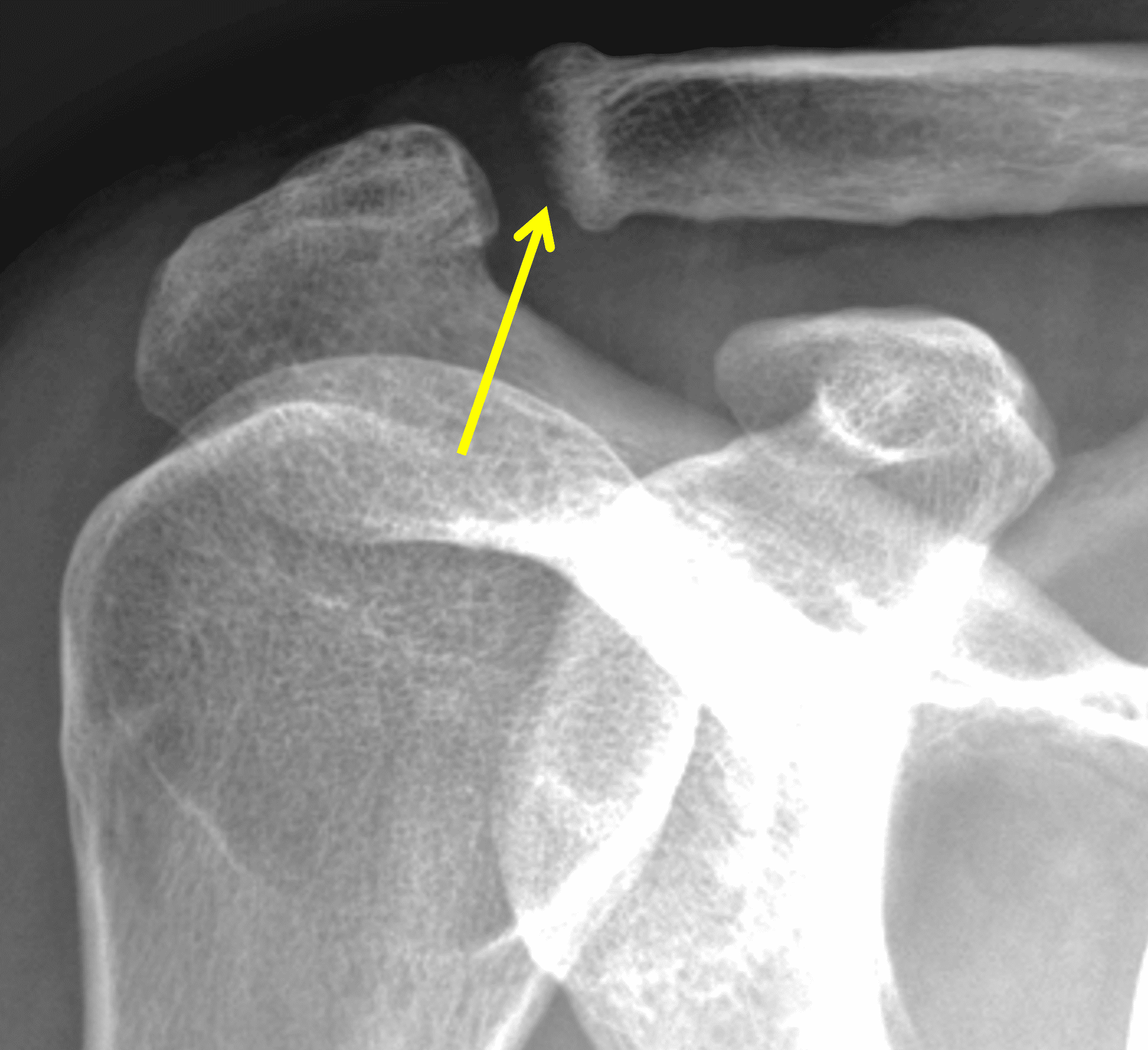

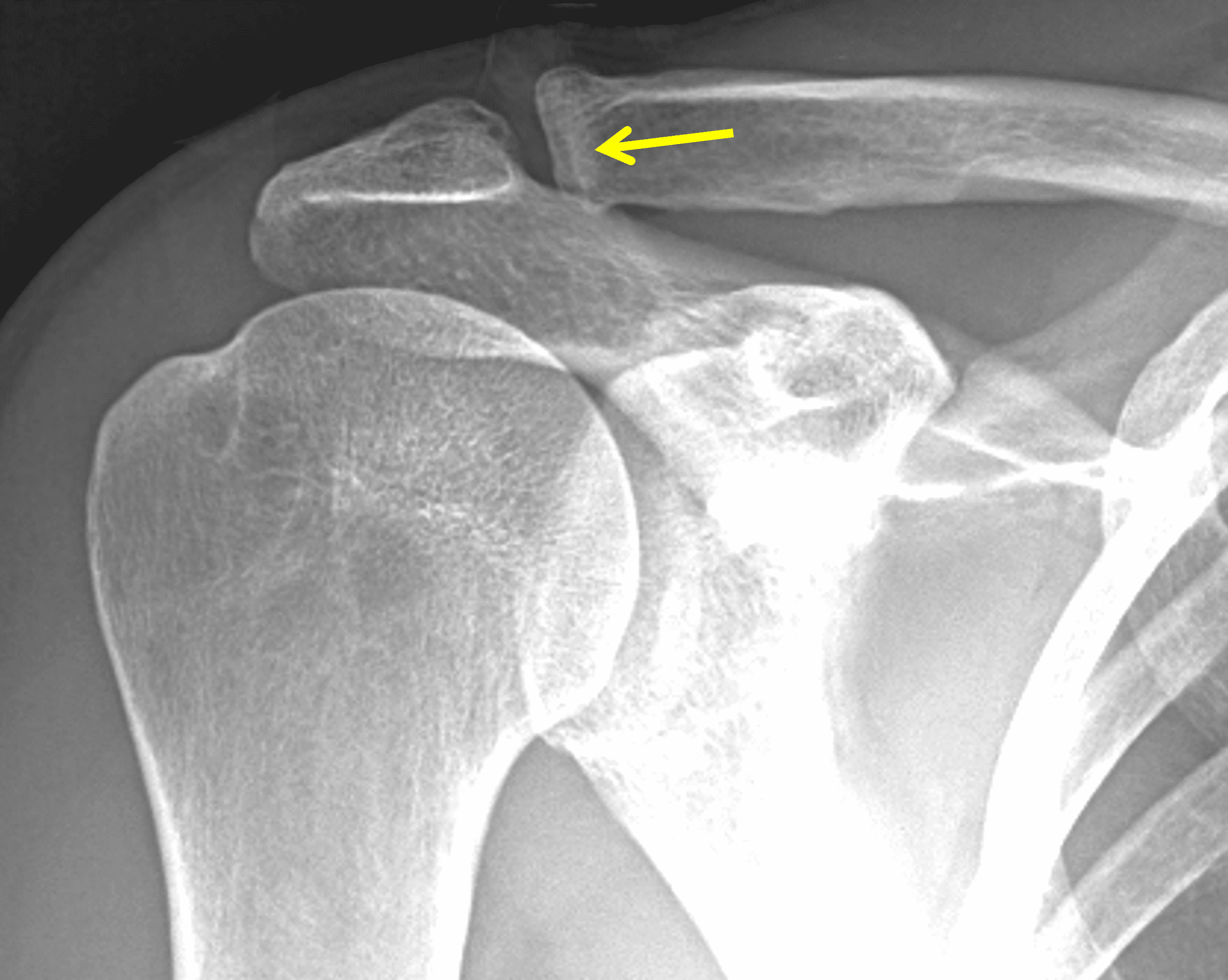
Figure 4: Distal clavicular osteolysis in a 47-year-old tennis player. (4A) The initial AP radiograph shows apparent widening of the acromioclavicular (AC) joint due to resorption of the distal clavicle subchondral bone plate (arrow). (4B) Distal clavicular marrow edema (asterisk) is apparent on an oblique sagittal fat-suppressed fluid-sensitive image. The anterior acromion (A) appears normal. Symptoms resolved after decreasing weight training. (4C) An AP radiograph 4 years later shows restoration of the AC joint and a sclerotic line adjacent to the distal clavicle subchondral bone plate (arrow) representing trabecular healing.
MRI: MRI is the primary imaging modality used for the diagnosis of DCO and identifies relevant findings earlier than radiographs or CT. To differentiate DCO from similar conditions, it is important to identify underlying findings that are isolated to or more pronounced in the distal clavicle compared to other structures. Osseous changes along both the acromial and distal clavicular margins of the joint often point to a different diagnosis.2
The principle MRI finding of DCO is distal clavicular marrow edema and surrounding inflammation on fluid-sensitive pulse sequences, especially with fat suppression (Figures 3 and 4).2, 9 Marrow changes can occur in patients with normal radiographs,10 in which case a term like “stress/overuse related marrow edema,” might be preferable to “osteolysis.” On MRI, more severe cases may show erosions or cysts in the distal clavicle and loss of the subchondral bone plate in addition to more pronounced marrow and soft tissue edema. A band of low signal paralleling the distal bone end may be present, suggesting a stress fracture line (Figure 5).8 However, a similar appearance can be due to the sclerotic rim surrounding distal clavicle cysts or small erosions (Figure 6). A small effusion or mild synovitis is often present in the AC joint. Soft tissue edema within and surrounding the AC joint capsule and distal clavicular periosteum may be visible (Figure 3). Some patients may also show marrow edema (or even erosions) in the anterior acromion, but the changes are typically more severe in the distal clavicle (Figures 5 and 7).2
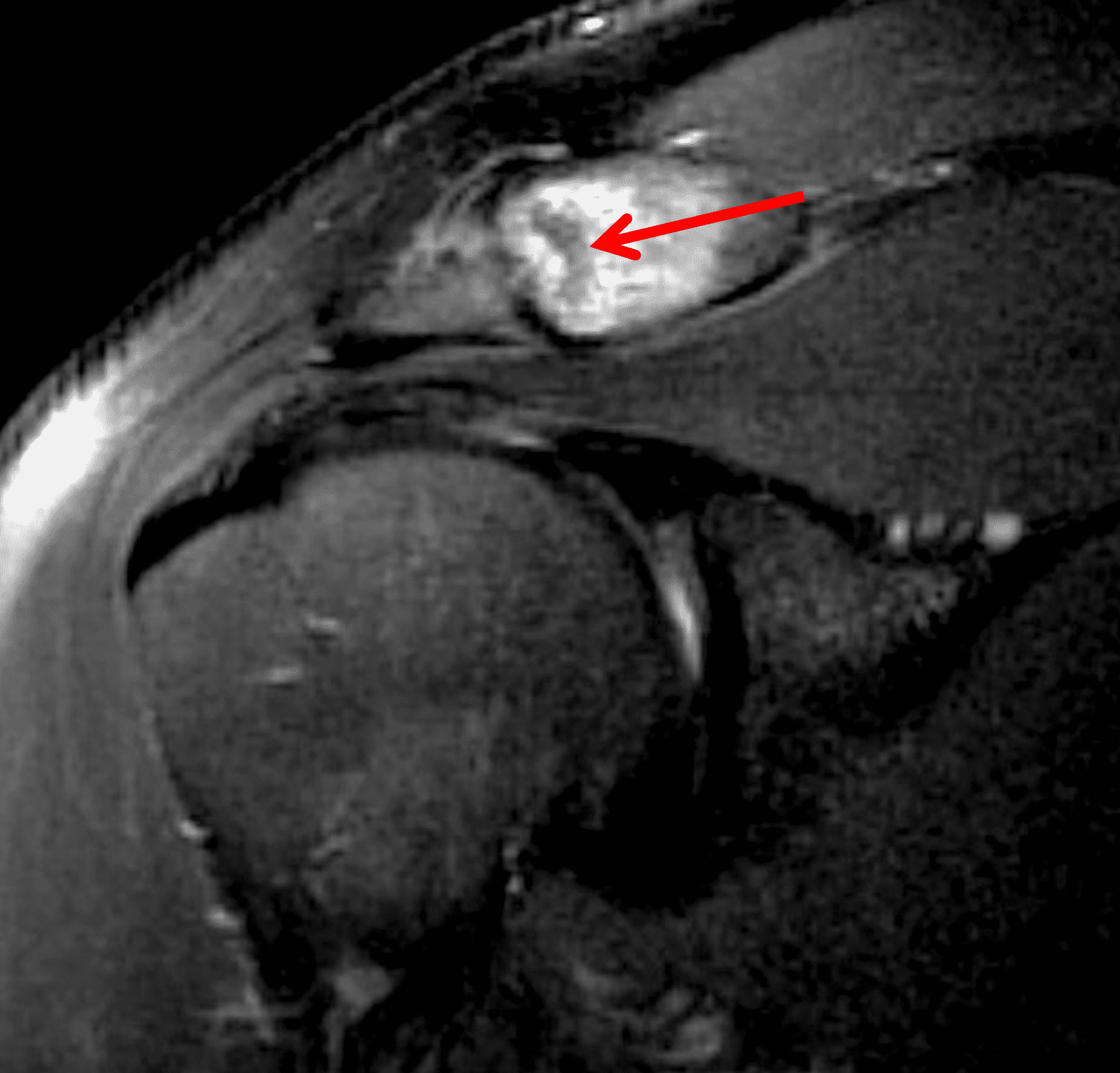

Figure 5: 28-year-old weightlifter with chronic superior shoulder pain. (5A) Oblique coronal and (5B) axial fat-suppressed T2-weighted images show a low-signal intensity line (arrows) within the distal clavicle, paralleling the distal bone end and surrounded by marrow edema. Some authors consider this finding evidence for a stress fracture being part of the pathophysiology of distal clavicular osteolysis in some patients. On the axial image, note the marrow edema in the acromion (A), less extensive compared to the distal clavicle.
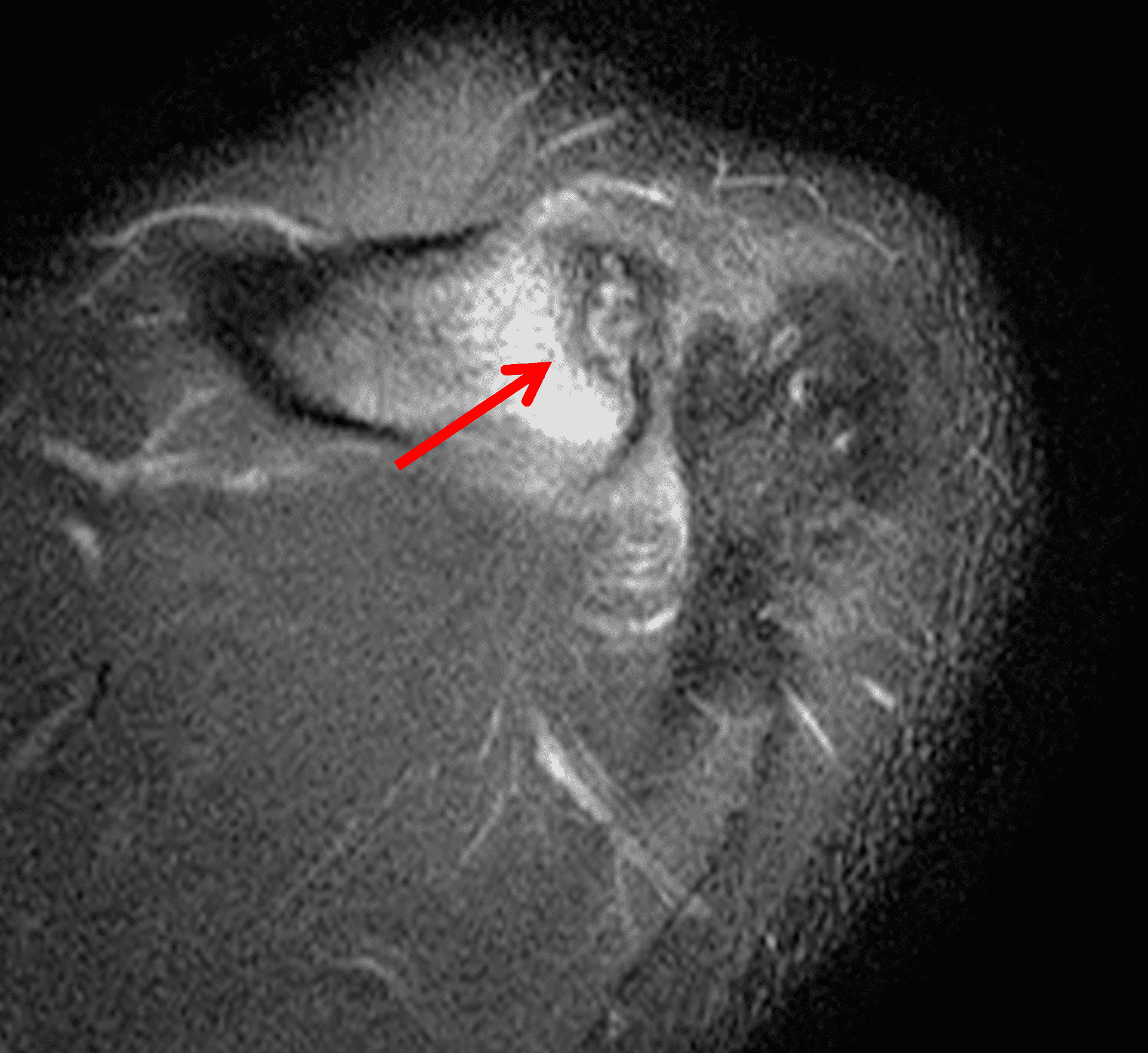
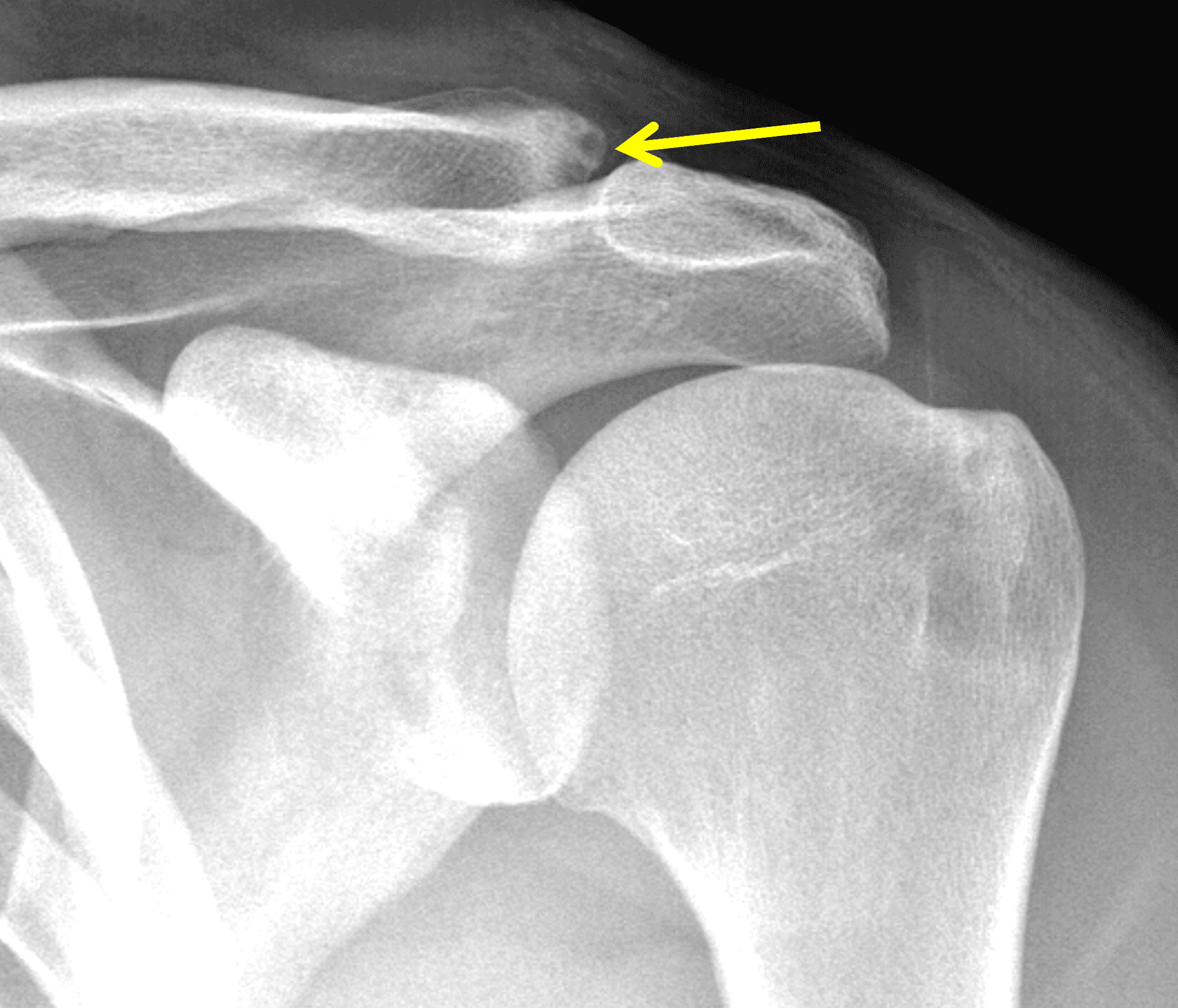
Figure 6: 36-year-old man with distal clavicular osteolysis. (6A) An axial fat-suppressed fluid-sensitive image shows marrow edema in the distal clavicle with a low signal intensity line (arrow), similar to Figure 5. However, the radiograph (6B) demonstrates several well-defined cysts or erosions in the distal clavicle (arrow) with sclerotic rims, which account for the low signal line on the MRI image.
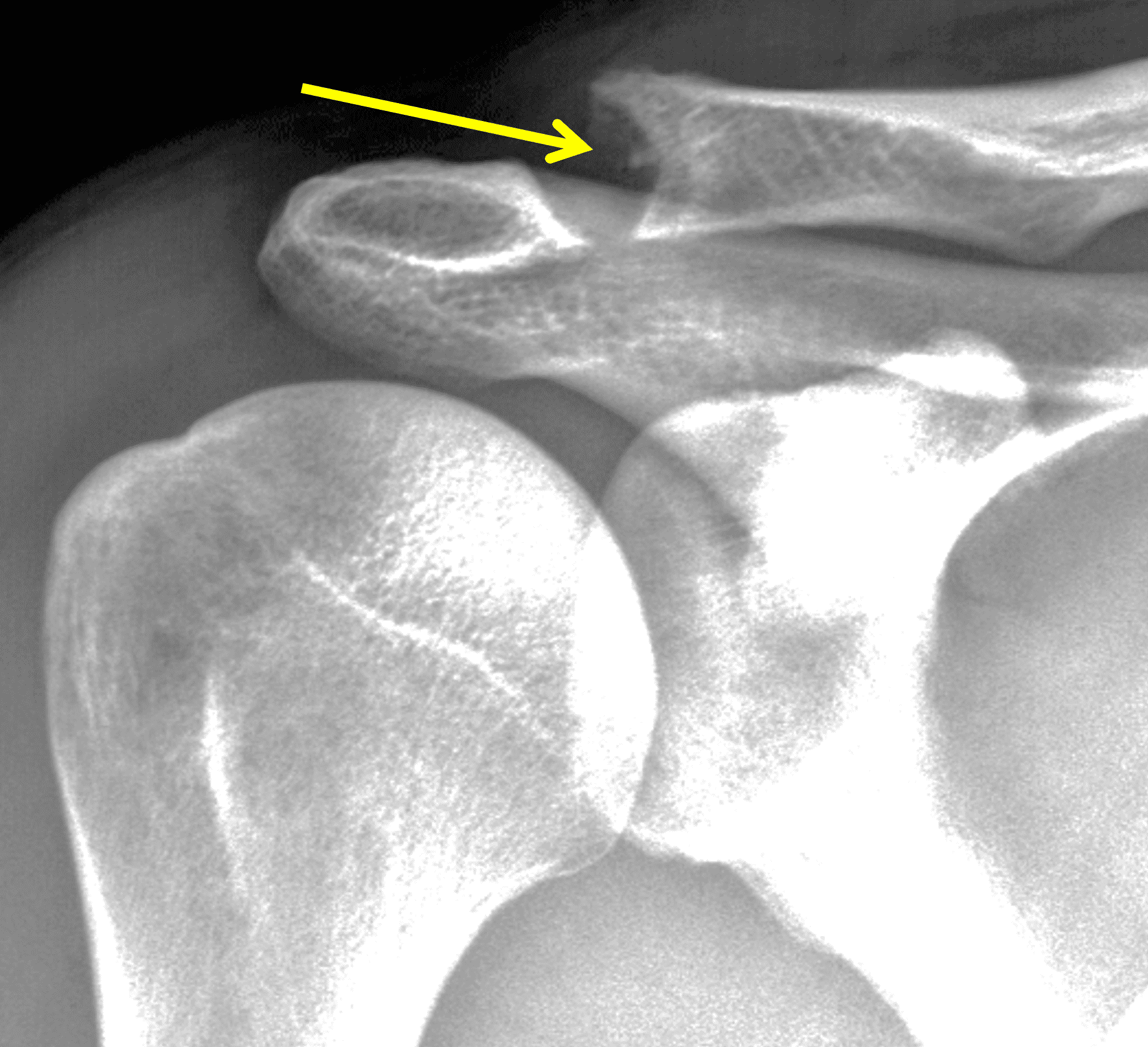

Figure 7: 31-year-old competitive body builder with severe distal clavicular osteolysis. (7A) AP Radiograph shows severe bone resorption of the distal clavicle. (7B) Axial fat-suppressed fluid-sensitive image demonstrates marrow edema in both the distal clavicle (C) and adjacent acromion (A), although the edema is more prominent in the clavicle.
While isolated DCO does not produce osteophytes, it may occur in patients with pre-existing osteoarthritis; in these cases, the marrow edema is typically out of proportion to the osteophytosis. When DCO occurs following an acute traumatic event like an AC joint separation, the MRI findings of that condition (e.g., widening or subluxation of the joint, disruption of the coracoclavicular ligaments) may be evident (Figure 8).1 Osteolysis can also develop following fractures of the distal clavicle, due to post-traumatic resorption of small, comminuted fracture fragments. In these cases, residual deformity of the clavicle or the presence of the original fracture lines may be evident on imaging studies. Additionally, because resorption of the fracture fragments typically occurs during the chronic healing after inflammation has resolved, marrow and soft tissue edema may not be present on MRI when the distal clavicular bone loss is seen.


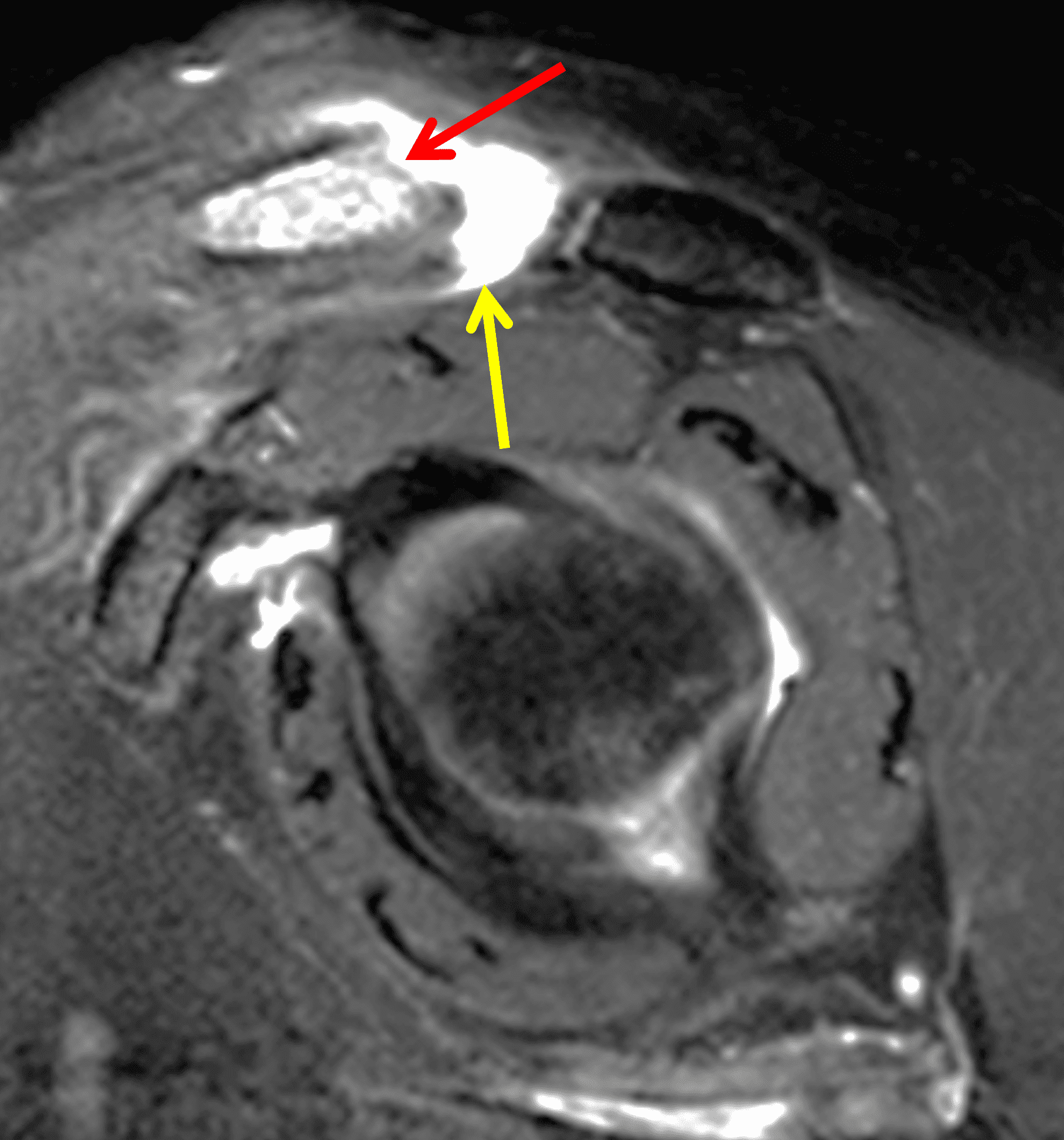
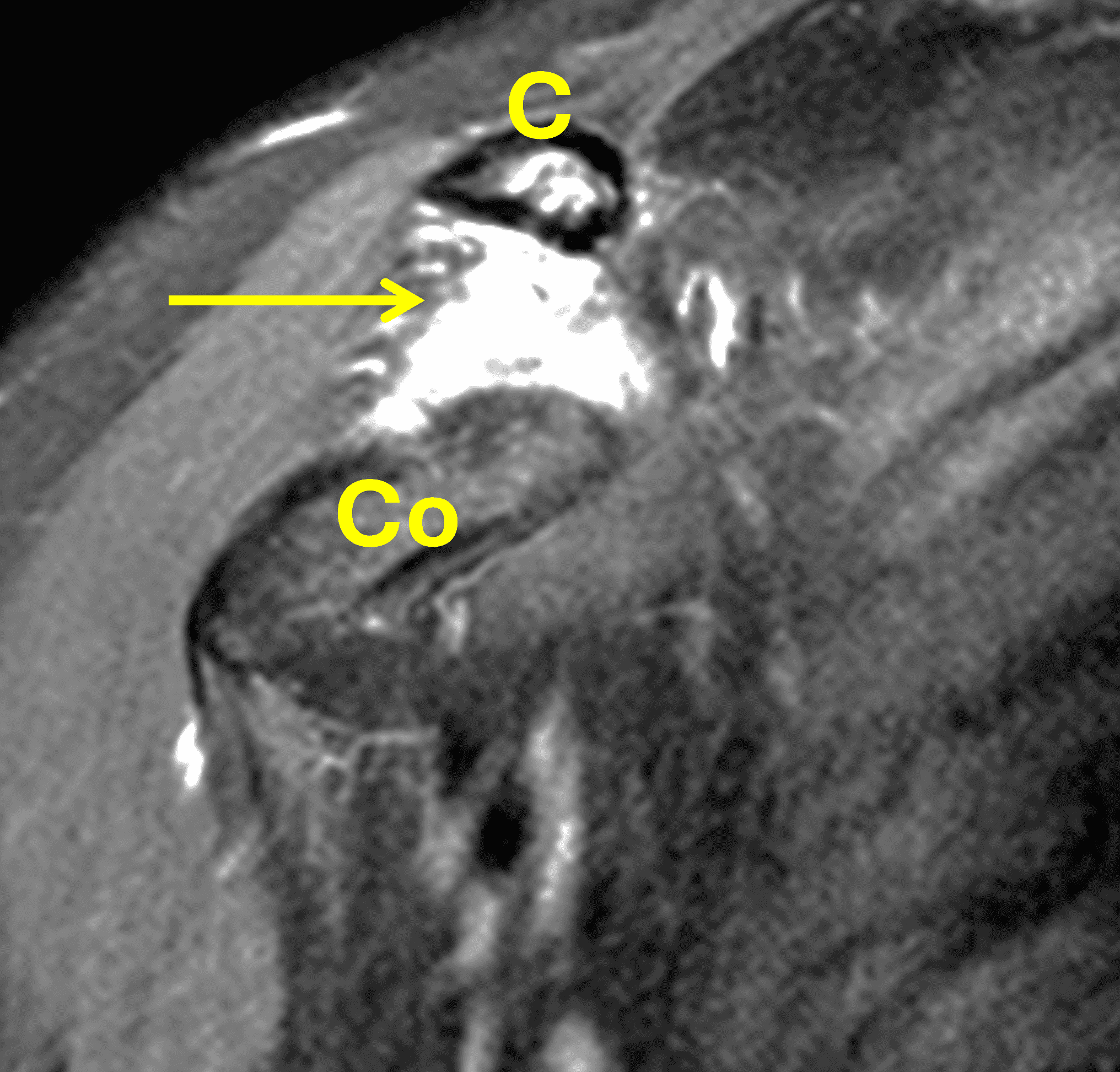
Figure 8: 48-year-old woman who suffered a grade 3 acromioclavicular (AC) joint separation approximately 6 weeks prior, with continued pain. (8A) A radiographic Grashey projection shows widening of the AC joint and inferior subluxation of the acromion, as well as bone resorption of the distal clavicle (arrow). Oblique coronal (8B) and oblique sagittal (8C) fat-suppressed fluid-sensitive sequences demonstrate marrow edema in the distal clavicle with loss of the distal subchondral bone plate (red arrows), and an effusion (yellow arrow) in the disrupted AC joint. (8D) An oblique coronal image more anteriorly shows complete rupture of the coracoclavicular ligaments (arrow) between the clavicle (C) and coracoid (Co).
Ultrasound: Ultrasound has also been shown to effectively identify soft tissue edema, hyperemia, and secondary joint fluid and inflammation in DCO. However, changes isolated to the bone marrow (as occurs in early or mild cases) will not be visible on ultrasound.
Differential Diagnosis
Several other disease processes have symptoms and imaging findings that may overlap with DCO. Attention to the clinical history and additional imaging findings in the shoulder can usually distinguish these conditions from DCO.
Osteoarthritis is the most common abnormality in the AC joint, which increases with age.11 Patients may be asymptomatic despite imaging findings.12 On MRI, when subchondral cyst formation and subchondral marrow edema are present, the findings can overlap with those of DCO (Figure 9). The bone changes in osteoarthritis often involve both the acromial and clavicular sides of the joint, unlike in DCO. Furthermore, joint narrowing and marginal osteophyte formation are characteristic features of osteoarthritis that are not expected with DCO.13 Surrounding soft tissue inflammation also tends to be less pronounced or absent with osteoarthritis.
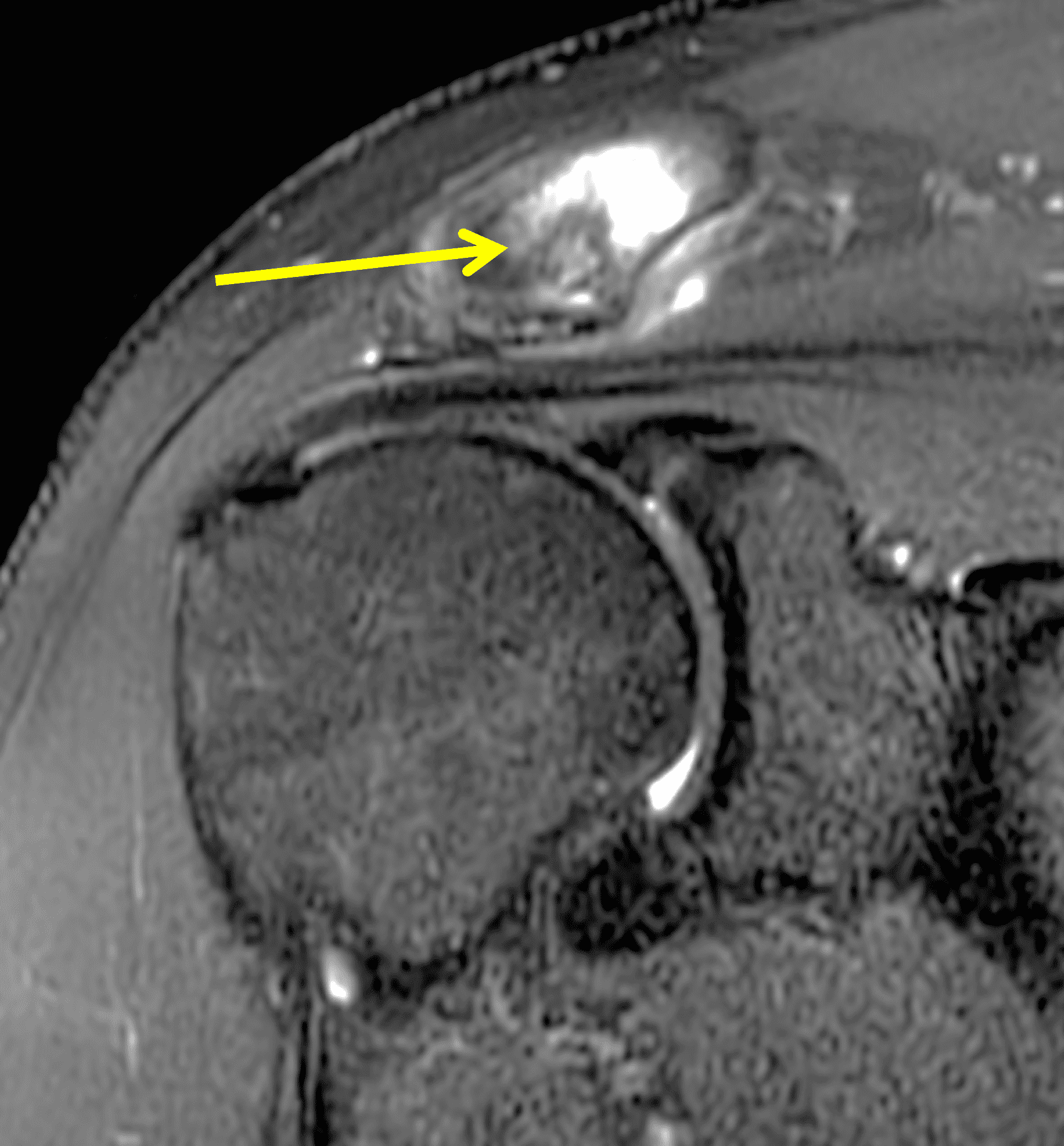


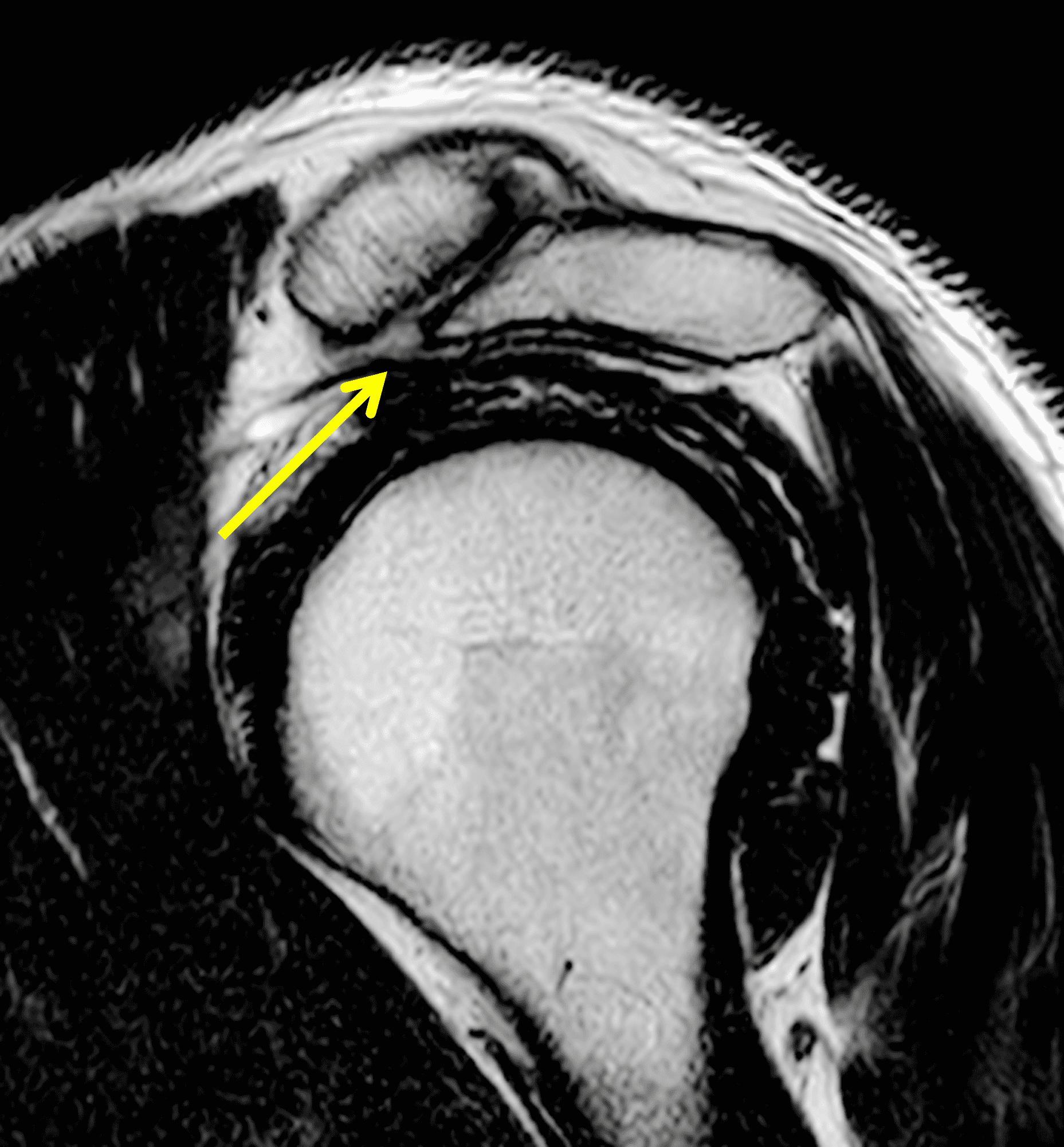
Figure 9: 39-year-old man with symptomatic acromioclavicular (AC) joint osteoarthritis. (9A) An oblique coronal fat-suppressed fluid-sensitive image shows marrow edema and a cyst or erosion in the distal clavicle (arrow), similar to findings in distal clavicular osteolysis. (9B) On the axial fat-suppressed fluid-sensitive sequence, note that marrow edema and erosions are present to a similar degree in the acromion and distal clavicle, which would be atypical for osteolysis. The outlet radiograph (9C) and oblique sagittal T2-weighted image (9D) show an osteophyte emanating from the inferior acromion (arrows) and narrowing of the AC joint, confirming osteoarthritis.
Rheumatoid arthritis (RA) is a systemic inflammatory disease primarily targeting synovial-lined structures, including the acromioclavicular joint. In most joints, the imaging findings are characterized by uniform joint space loss, marginal erosions, synovitis, and joint distension. However, in the AC joint bone destruction and erosions, which are often visible radiographically, may produce an appearance of apparent joint widening that can mimic DCO.14 On MRI, the inflammatory changes in RA (such as marrow edema or “osteitis”) typically involve both sides of the joint equally and are usually clearly centered at the joint space.15 This is also true in cases of septic arthritis. Septic arthritis characteristically progresses much faster than the other items on this differential diagnosis. In septic arthritis, extensive surrounding soft tissue inflammation and contrast enhancement of thickened synovium in the AC joint and subacromial bursa are often clues to the diagnosis (Figure 10).16 In equivocal cases, joint aspiration should be diagnostic.


Figure 10: 68-year-old man with septic arthritis of the acromioclavicular (AC) joint and septic bursitis after a rotator cuff repair. (10A) Coronal fat-suppressed fluid-sensitive image shows marrow edema in both the acromion and distal clavicle (yellow arrow) centered at the AC joint. Also note the extensive surrounding soft tissue inflammation including distention of the subacromial-subdeltoid bursa (red arrow). (10B) A fat-suppressed, T1-weighted image obtained after intravenous contrast administration shows non-enhancing fluid in the AC joint and bursa. Thick enhancing synovium lines the AC joint (yellow arrow) and subacromial-subdeltoid bursa (red arrow).
Hyperparathyroidism is a metabolic disorder that can lead to subchondral bone resorption, including at the distal clavicle, as well as subchondral marrow edema. Like RA, bone resorption tends to involve both sides of the AC joint relatively symmetrically, producing an appearance of joint widening (Figure 11).17 While some of the imaging findings can mimic DCO, hyperparathyroidism is a systemic process involving multiple skeletal sites and must be considered in the context of broader clinical and laboratory findings.
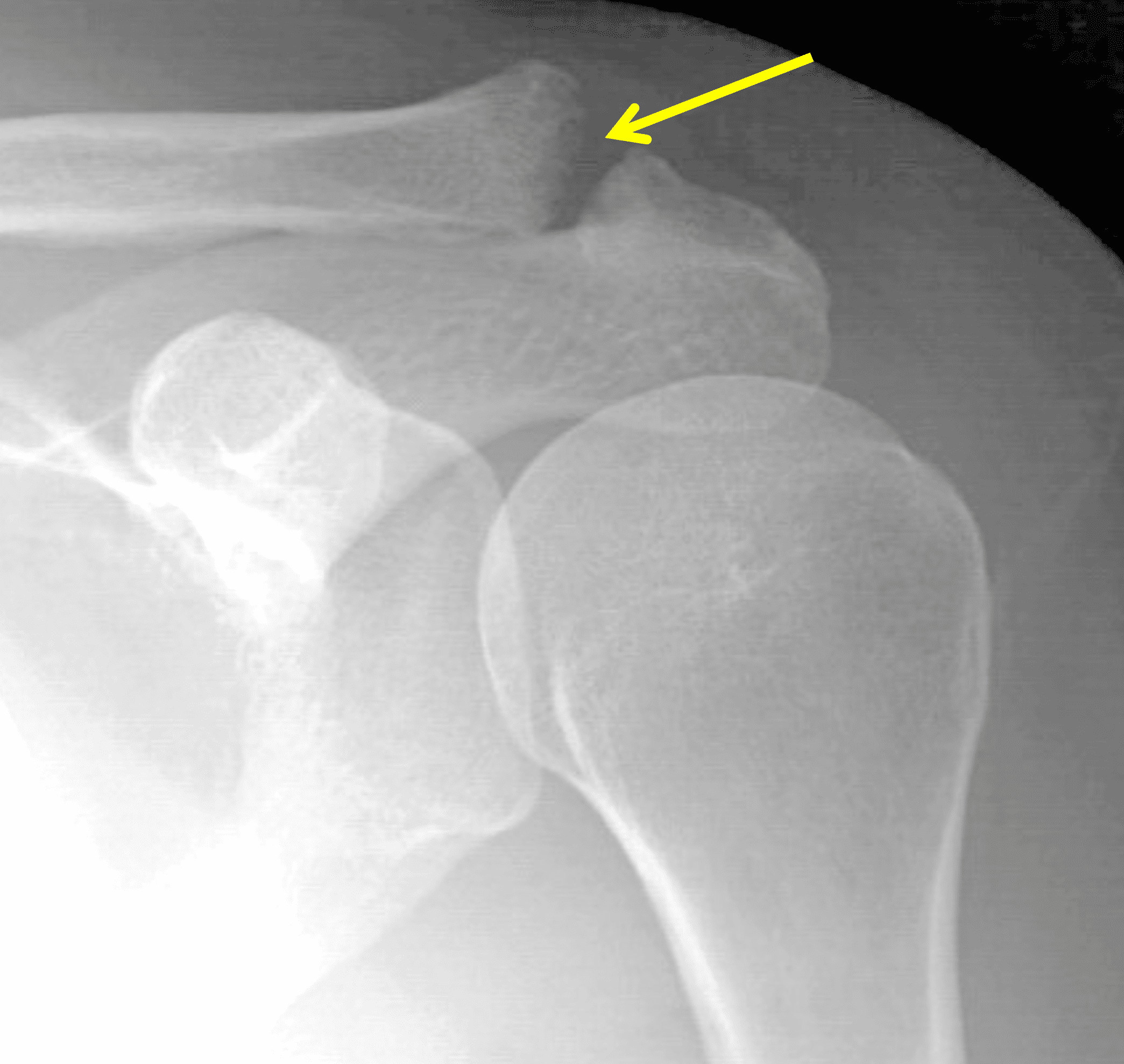


Figure 11: 55-year-old man with a parathyroid adenoma and hyperparathyroidism involving the acromioclavicular (AC) joint. (11A) An AP radiograph shows apparent widening of the AC joint (arrow) and bone resorption in the distal clavicle and anterior acromion. (11B) Oblique coronal and (11C) axial fat-suppressed T2-weighted images show marrow edema and regions of subchondral bone resorption in both the clavicle (C) and acromion (A).
Gorham-Stout disease, is a rare and poorly understood condition that often appears on the classic imaging differential diagnosis of DCO. This is a systemic condition characterized by progressive idiopathic bone loss. Although it may involve the clavicle, it tends to be more aggressive and widespread compared to DCO, with bone loss that extends beyond the confines of the acromioclavicular joint.18
Several imaging pitfalls should also be kept in mind. AC joint separation can produce widening and malalignment of the joint and clavicular edema can be present if there is also a bone contusion. However, osteolysis does not occur acutely, and evidence of capsular and coracoclavicular ligament disruption should lead to the correct diagnosis. Acute distal clavicle fractures or bone contusions may produce marrow edema and subcortical signal changes that resemble early DCO, but careful inspection often reveals cortical disruption or fracture lines that clarify the diagnosis. A clinical history of acute trauma should accompany an AC separation or clavicle fracture, while DCO most often develops subacutely and insidiously. In cases of DCO following acute trauma, the osteolysis occurs several weeks after the initial injury.2 Lastly, a surgical distal clavicle excision can produce a distal clavicle contour deformity that can be mistaken for DCO, including with marrow edema in the early post-operative period. After the resection has healed, the deformity will remain while marrow edema should resolve (Figure 13). Correlation with surgical history and a search for artifact or scarring related to the surgery will help to avoid diagnostic mistakes.
In summary, accurate diagnosis depends on careful correlation of imaging findings with clinical context, focusing on the laterality, distribution, and progression of osseous and soft tissue changes. Recognizing the imaging hallmarks of DCO — particularly when isolated to the distal clavicle — remains key in differentiating it from these mimics.
Treatment
Treatment of DCO will almost always initially include temporary cessation or restriction of the inciting activities. NSAIDs are useful in addressing pain and inflammation. Corticosteroid injection into the AC joint with local anesthetic has been shown to be effective in patients who do not respond to rest and medications.19 Once the inflammation has decreased, physical therapy may be prescribed to improve strength and range of motion. In high level athletes with recalcitrant symptoms, arthroscopy and distal clavicle excision (Mumford procedure) is effective in eradicated pain symptoms without significant residual functional or performance deficits,20 with return to activity typically within 6 weeks.21
References
- Yu YS, Dardani M, Fischer RA. MR observations of postraumatic osteolysis of the distal clavicle after traumatic separation of the acromioclavicular joint. J Comput Assist Tomogr. 2000;24(1):159-164. doi:10.1097/00004728-200001000-00028 ↩
- de la Puente R, Boutin RD, Theodorou DJ, Hooper A, Schweitzer M, Resnick D. Post-traumatic and stress-induced osteolysis of the distal clavicle: MR imaging findings in 17 patients. Skeletal Radiol. 1999;28(4):202-208. doi:10.1007/s002560050501 ↩
- Cahill BR. Osteolysis of the distal part of the clavicle in male athletes. J Bone Joint Surg Am. 1982;64(7):1053-1058. ↩
- Asano H, Mimori K, Shinomiya K. A case of post-traumatic osteolysis of the distal clavicle: histologic lesion of the acromion. J Shoulder Elbow Surg. 2002;11(2):182-187. doi:10.1067/mse.2002.122229 ↩
- Nevalainen MT, Ciccotti MG, Morrison WB, Zoga AC, Roedl JB. Distal clavicular osteolysis in adults: association with bench pressing intensity. Skeletal Radiol. 2016;45(11):1473-1479. doi:10.1007/s00256-016-2446-z ↩
- DeFroda SF, Nacca C, Waryasz GR, Owens BD. Diagnosis and Management of Distal Clavicle Osteolysis. Orthopedics. 2017;40(2):119-124. doi:10.3928/01477447-20161128-03 ↩
- Roedl JB, Nevalainen M, Gonzalez FM, Dodson CC, Morrison WB, Zoga AC. Frequency, imaging findings, risk factors, and long-term sequelae of distal clavicular osteolysis in young patients. Skeletal Radiol. 2015;44(5):659-666. doi:10.1007/s00256-014-2092-2 ↩
- Kassarjian A, Llopis E, Palmer WE. Distal clavicular osteolysis: MR evidence for subchondral fracture. Skeletal Radiol. 2007;36(1):17-22. doi:10.1007/s00256-006-0209-y ↩
- Allen H, Chan BY, Davis KW, Blankenbaker DG. Overuse Injuries of the Shoulder. Radiol Clin North Am. 2019;57(5):897-909. doi:10.1016/j.rcl.2019.03.003 ↩
- Fiorella D, Helms CA, Speer KP. Increased T2 signal intensity in the distal clavicle: incidence and clinical implications. Skeletal Radiol. 2000;29(12):697-702. doi:10.1007/s002560000284 ↩
- Rajagopalan D, Abdelaziz A, Ring D, Slette E, Fatehi A. MRI findings of acromioclavicular joint osteoarthritis are the norm after age 40. Orthop Traumatol Surg Res. 2023;109(4):103526. doi:10.1016/j.otsr.2022.103526 ↩
- Singh B, Gulihar A, Bilagi P, Goyal A, Goyal P, Bawale R, et al. Magnetic resonance imaging scans are not a reliable tool for predicting symptomatic acromioclavicular arthritis. Shoulder Elbow. 2018;10(4):250-254. doi:10.1177/1758573217724080 ↩
- Veen EJD, Donders CM, Westerbeek RE, Derks RPH, Landman EBM, Koorevaar CT. Predictive findings on magnetic resonance imaging in patients with symptomatic acromioclavicular osteoarthritis. J Shoulder Elbow Surg. 2018;27(8):e252-e258. doi:10.1016/j.jse.2018.01.001 ↩
- Lehtinen JT, Lehto MU, Kaarela K, Kautiainen HJ, Belt EA, Kauppi MJ. Radiographic joint space in rheumatoid acromioclavicular joints: a 15 year prospective follow-up study in 74 patients. Rheumatology (Oxford). 1999;38(11):1104-1107. doi:10.1093/rheumatology/38.11.1104 ↩
- McDonald S, Hopper MA. Acromioclavicular joint disease. Semin Musculoskelet Radiol. 2015;19(3):300-306. doi:10.1055/s-0035-1549323 ↩
- Iyengar KP, Gudena R, Chitgopkar SD, Ralte P, Hughes P, Nadkarni JB, et al. Primary septic arthritis of the acromio-clavicular joint: case report and review of literature. Arch Orthop Trauma Surg. 2009;129(1):83-86. doi:10.1007/s00402-008-0747-y ↩
- Nathanson L, Slobodkin M. Acromioclavicular changes in primary and secondary hyperparathyroidism. Radiology. 1950;55(1):31-35. ↩
- Liu Y, Zhong DR, Zhou PR, Lv F, Ma DD, Xia WB, et al. Gorham-Stout disease: radiological, histological, and clinical features of 12 cases and review of literature. Clin Rheumatol. 2016;35(3):813-823. doi:10.1007/s10067-014-2780-2 ↩
- Sopov V, Fuchs D, Bar-Meir E, Groshar D. Stress-induced osteolysis of distal clavicle: imaging patterns and treatment using CT-guided injection. Eur Radiol. 2001;11(2):270-272. doi:10.1007/s003300000529 ↩
- Zawadsky M, Marra G, Wiater JM, Levine WN, Pollock RG, Flatow EL, et al. Osteolysis of the distal clavicle: long-term results of arthroscopic resection. Arthroscopy. 2000;16(6):600-605. doi:10.1053/jars.2000.5875 ↩
- Charron KM, Schepsis AA, Voloshin I. Arthroscopic distal clavicle resection in athletes: a prospective comparison of the direct and indirect approach. Am J Sports Med. 2007;35(1):53-58. doi:10.1177/0363546506294855 ↩
