Clinical History
A 22-year-old collegiate football player presents with left proximal posterior thigh pain after sprinting. Fat-suppressed proton density-weighted axial (Figure 1A and 1B), coronal (Figure 1C), and sagittal (Figure 1D) images are shown. What are the findings? What is your diagnosis? How would you grade this injury?

Findings

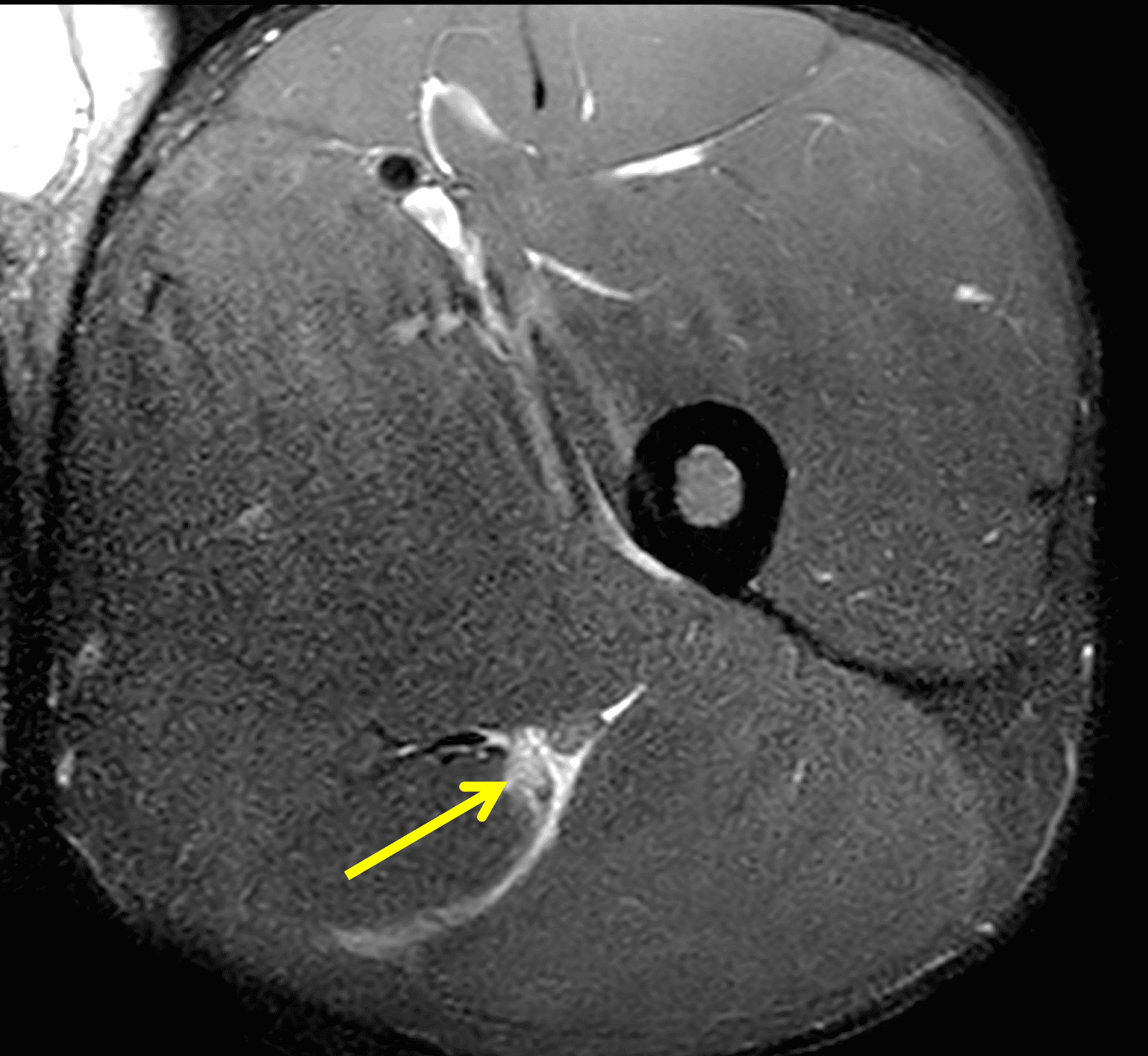

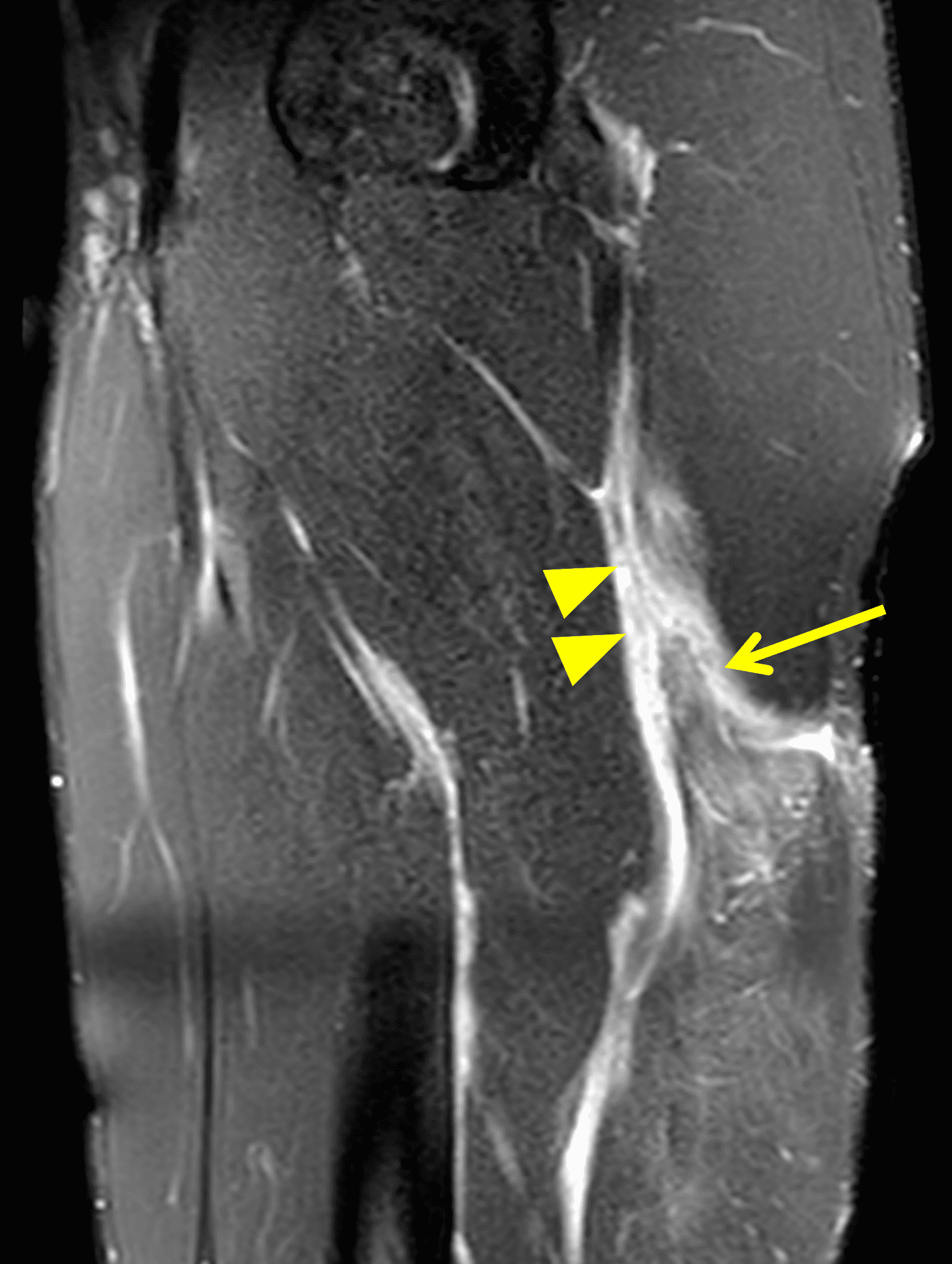
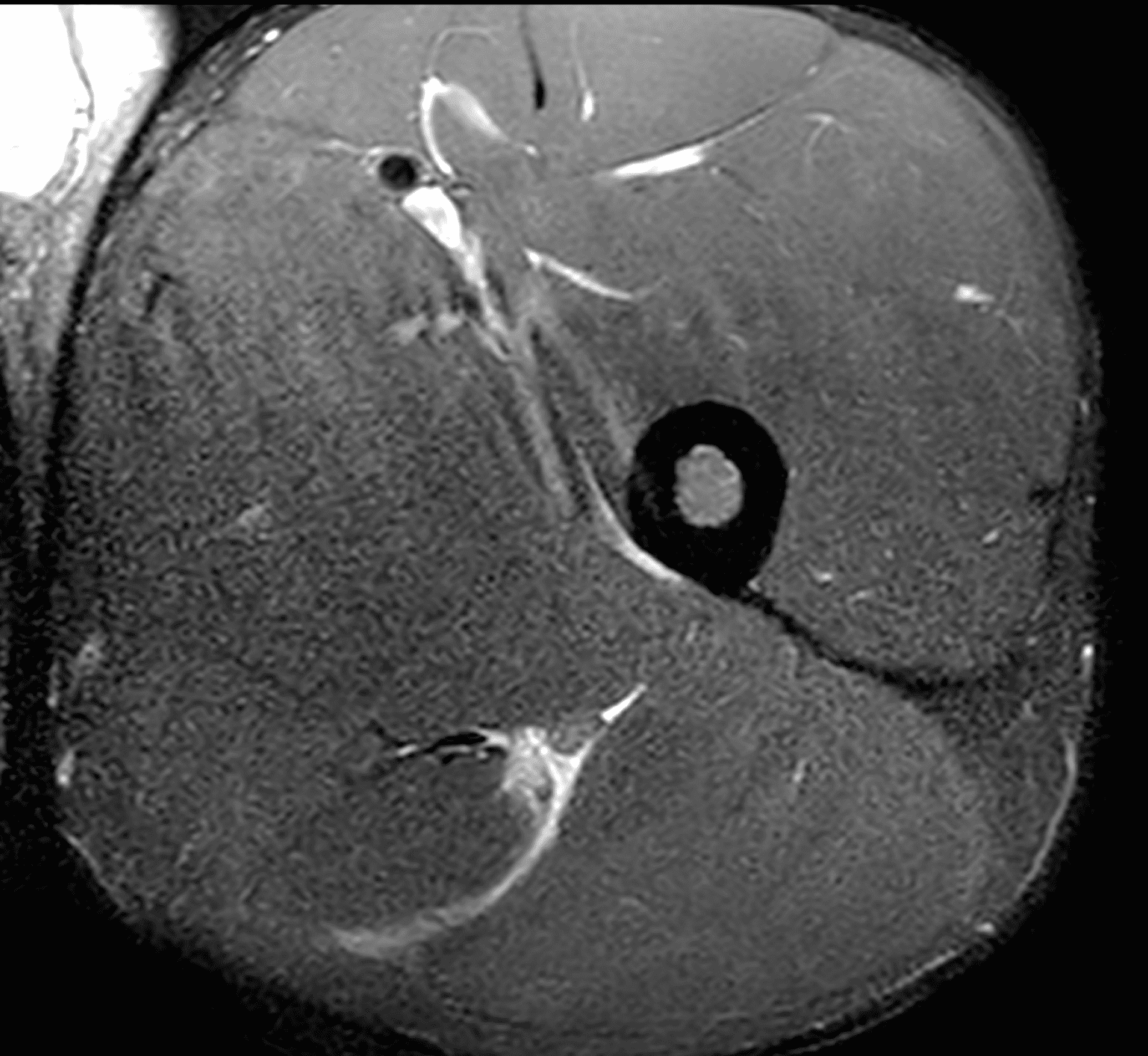
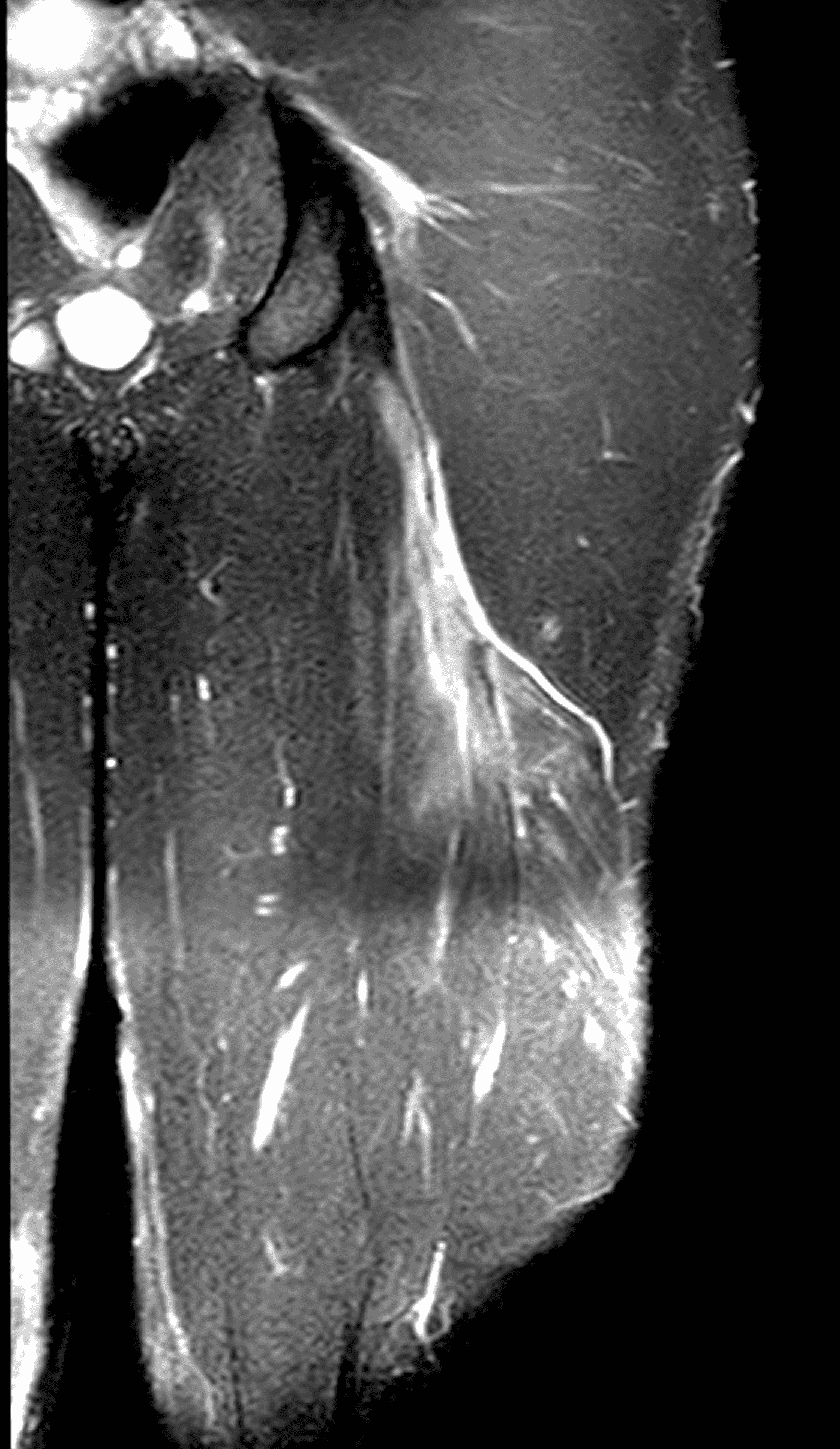
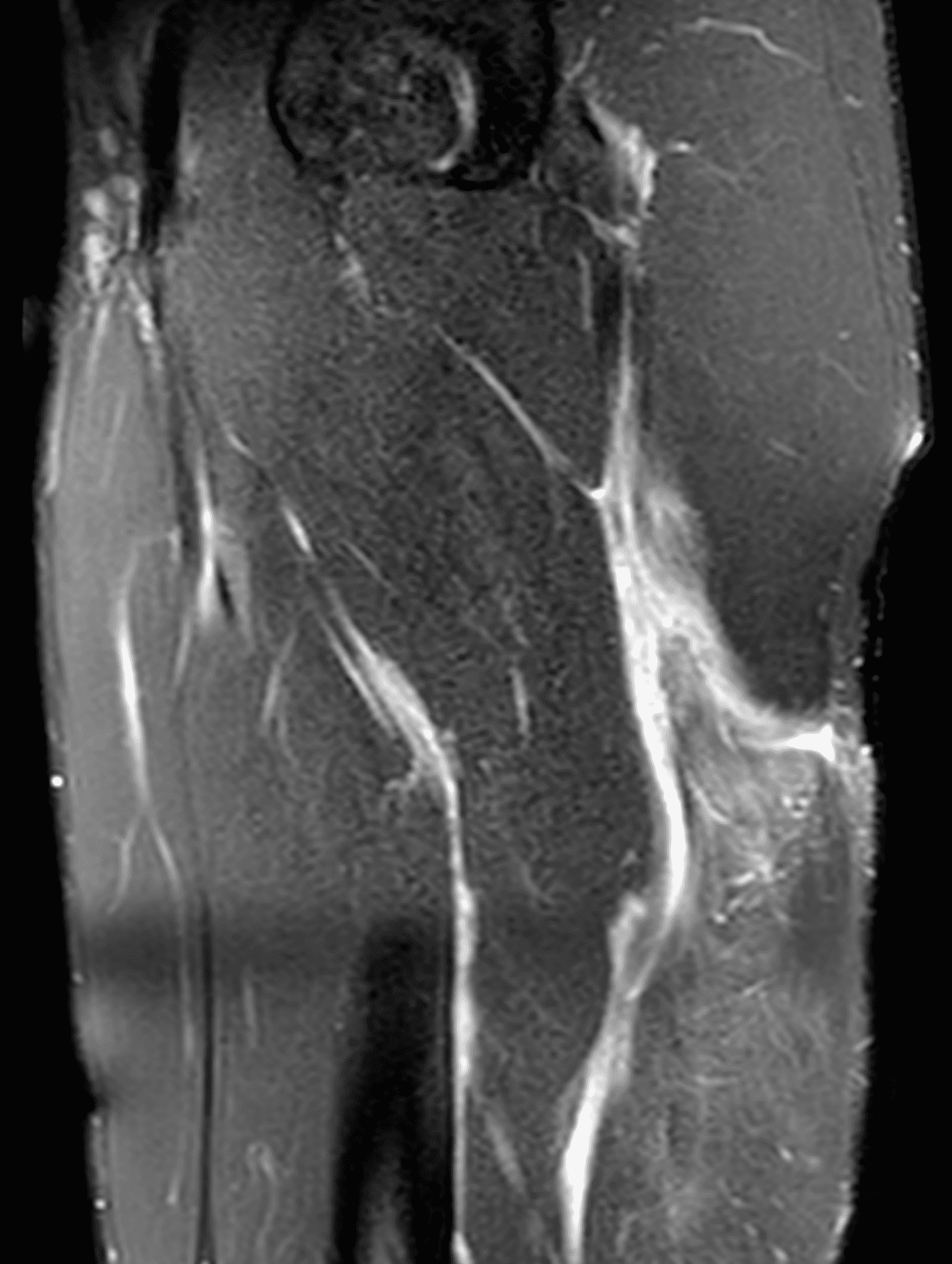
Figure 2: The first axial (2A) image shows high signal intensity edema involving greater than 50% of the long head biceps femoris muscle cross sectional area (asterisk). An axial image more proximally (2B) shows disruption involving a portion of the intra-muscular tendon (arrow). The coronal image (2C) shows the extent of the tendon fiber disruption (arrowheads), which measured 4 cm in length. The total extent of the muscle edema measured 14 cm. On the sagittal image (2D), note the disrupted fibers (arrowheads), with loss in tension distally demonstrated by the caudal retraction of the myotendinous junction (arrow). Even though the length of myotendinous involvement is less than 5 cm, the loss of tendon tension renders this a 3c injury because it is graded at the highest level.
Diagnosis
High-grade injury of the proximal biceps femoris, British Athletics Muscle Injury Classification (BAMIC) grade 3c.
Introduction
Hamstring injuries are a common concern among athletes, especially those participating in sports that require running, kicking, or explosive movements. These injuries can arise from various mechanisms, but noncontact hamstring injuries are typically linked to two primary causes: eccentric overloading and eccentric overstretching.
Eccentric overloading occurs when the hamstring muscle lengthens while actively contracting. A classic example of this is sprinting, particularly during the late swing phase of the stride, when the leg is extended and the heel is about to strike the ground. During this phase, the hamstring muscles work to decelerate the leg and control its motion, placing them under high stress and increasing the risk of injury. The long head biceps femoris is most commonly injured in this way. High-speed cutting or decelerating maneuvers are a second common mechanism of eccentric overload.
Eccentric overstretching occurs when the muscle is subjected to substantial stretch under load, commonly seen during explosive kicking motions. In these actions, the muscle is stretched to its limit while the hip is flexed and the knee extended, placing the fibers under immense tension. The proximal semimembranosus is particularly vulnerable to this form of injury. Intense slow stretching – as when a dancer warms up at the barre – can also lead to these hamstring injuries.
MRI plays a pivotal role in evaluating muscle and tendon injuries; however, traditional clinical and imaging injury grading systems often fall short in accurately predicting recovery times. In these systems, Grade 1 injuries are considered mild, where all myotendinous fibers remain intact. Grade 2 injuries are more severe, marked by muscle fiber disruption and often accompanied by an intramuscular hematoma. Grade 3 injuries represent a complete rupture of the myotendinous cross-section.1
Hamstring injuries often lead to substantial time away from competition. Furthermore, reinjury rates may be as high as 3.6 times greater than initial injury rates.2 Given the significant impact of injury extent on recovery and treatment, various classification systems have been developed to more precisely correlate injury severity with prognostic outcomes, guiding clinical decision-making and rehabilitation strategies. The British Athletics Muscle Injury Classification (BAMIC) stands out for its ability to directly correlate injury severity with prognostic outcomes (Figures 3 and 4).3

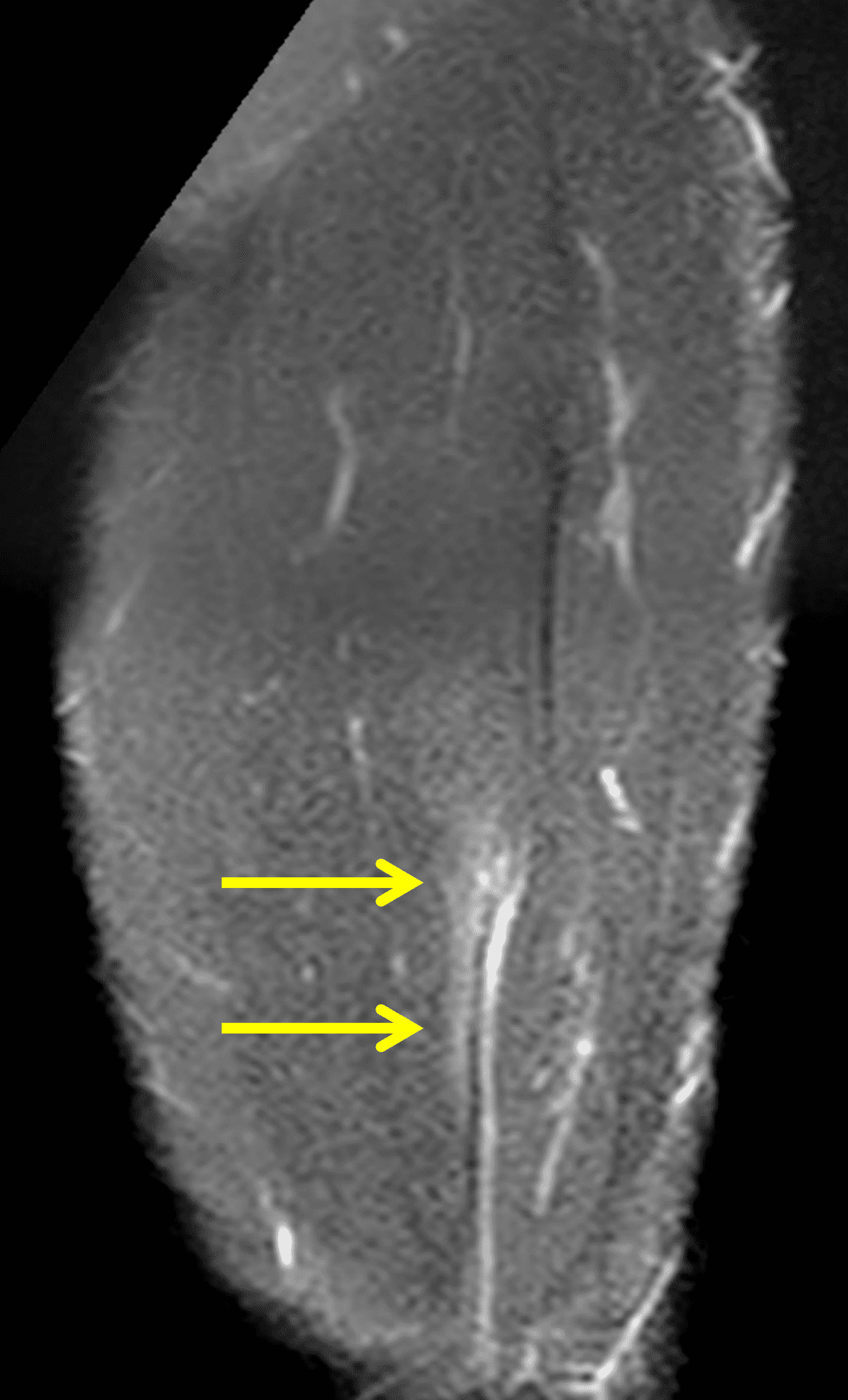
Figure 3: BAMIC grade 2b injury in a 22-year-old college football athlete. (3A) An axial fat-suppressed proton density-weighted image shows edema involving between 10% and 50% of the semitendinosus myotendinous junction (arrow). (3B) A coronal fat-suppressed proton density-weighted image shows the length of edema (arrows), which measured between 5 and 15 cm. No fiber disruption is present.

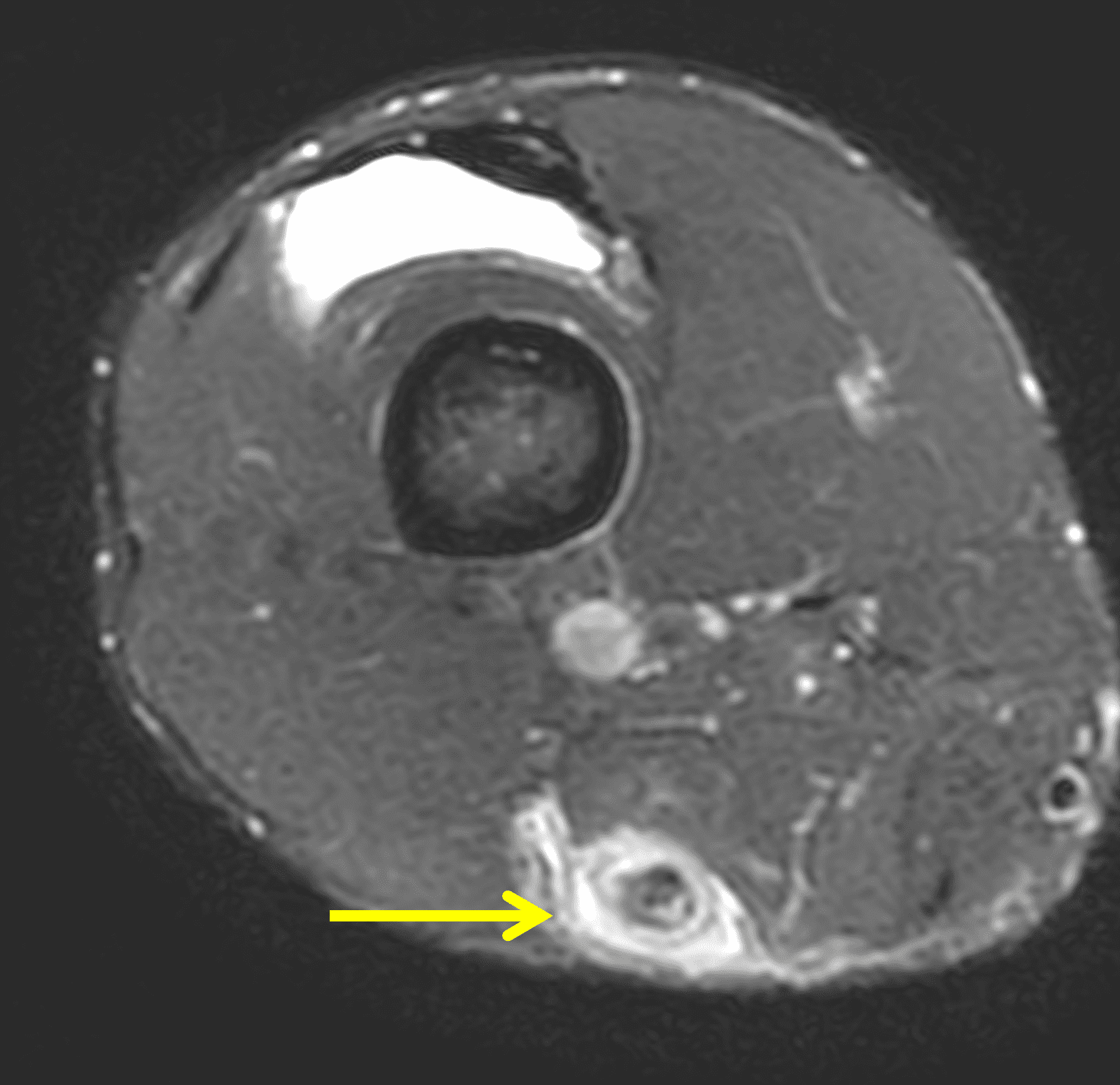

Figure 4: Recurrent injury in the same patient as Figure 3, two months later, now BAMIC grade 3b. (4A) An axial fat-suppressed proton density-weighted image through the mid thigh shows increased cross-sectional area of the semimembranosus myotendinous edema (arrow). More distally, axial (4B) and coronal (4C) fat-suppressed proton density-weighted images demonstrate near fluid-equivalent high signal intensity “gaps” (arrows) representing areas of fiber disruption in the myotendinous junction.
Anatomy
The hamstring complex consists of three primary muscles: the semimembranosus, semitendinosus, and biceps femoris (which has both long and short heads). These muscles originate from the posterolateral aspect of the ischial tuberosity. Notably, the biceps femoris and semitendinosus share a conjoint tendon origin, which is located posteromedial to the origin of the semimembranosus. The semimembranosus tendon footprint is positioned slightly anterolaterally.4,5
The conjoint tendon measures about 10 cm in length and runs between the biceps femoris long head and the semitendinosus muscle bellies. The biceps femoris long head arises from the ischial tuberosity, just distal to the semitendinosus muscle. The biceps femoris short head has a more distal separate origin from the linea aspera, a ridge on the posterior femur. These distinct origins contribute to different functions: the long head is responsible for both hip extension and knee flexion, while the short head primarily flexes the knee.
In the distal posterolateral thigh, the biceps femoris muscles converge, and the dense connective tissue surrounding each muscle (the epimysium) condenses to form a superficial aponeurosis, with an inconstant component of the aponeurosis extending between the two muscle bellies forming a T-shaped junction (Figure 5). While the anatomy of the distal biceps myotendinous junction is somewhat variable, in general after the long muscle belly terminates, the short head becomes the dominant component. The aponeurotic components of the distal biceps femoris tendon then split around the lateral collateral ligament of the knee, with multiple insertions onto the fibula and lateral tibia.
Figure 5. Left click, hold, and drag to scroll through images. Sequential axial T1-weighted images and 3-D rendered drawing of distal biceps femoris anatomy. The short head (light red) and long head (dark red) muscle are each invested by a superficial, thin aponeurosis (yellow). A variable aponeurotic extension (green) extends between the two muscle heads.
The semimembranosus tendon is the longest of the proximal hamstring tendons, measuring about 30 cm in length. As it descends, it flattens and lies anterior to the semitendinosus muscle belly, posterior to the adductor magnus muscle, and medial to the sciatic nerve. The proximal semimembranosus muscle originates as a small, triangular-shaped muscle from the medial aspect of this flattened tendon. As the semimembranosus muscle extends caudally, it enlarges and has the largest cross-sectional area of the hamstrings, allowing it to generate the greatest force.6
The distal semimembranosus tendon has multiple insertions including along the posteromedial proximal tibia and other components of the posteromedial corner of the knee. The semitendinosus muscle ends in the distal third of the thigh, forming a long distal tendon that attaches to the anteromedial aspect of the proximal tibia, contributing to the pes anserine complex along with the gracilis and sartorius tendons.
The innervation of the hamstring muscles is as follows: the semimembranosus, semitendinosus, and the long head of the biceps femoris are innervated by the tibial division of the sciatic nerve, while the short head of the biceps femoris is innervated by the peroneal division of the sciatic nerve. This difference in innervation is believed to play an important role in the distinct functional contributions of each muscle, particularly between the long and short heads of the biceps femoris.
Classification Criteria
Hamstring injuries can affect various structures within the muscle group, including the fascia, muscle belly, myotendinous junction, or tendon. The healing process for these injuries varies depending on the tissue involved. Tendons typically heal more slowly than the myotendinous junction, and myofascial injuries tend to recover more quickly. Identifying the specific tissue affected is critical for tailoring rehabilitation strategies, as treatment will differ based on the injury’s severity and location.
A particularly vulnerable area in the muscle-tendon-bone unit is the musculotendinous junction, where the muscle transitions into the tendon. This junction plays a crucial role in transferring the force generated by muscle contraction to the tendon and ultimately to the bone, making it especially susceptible to strain during high-intensity movements.
Tendon tears and avulsions are distinct from injuries affecting the musculotendinous or myofascial junctions. Injuries to the proximal tendon origin or distal insertion typically result from extreme forces or direct trauma and often require surgical intervention for recovery. Underlying degenerative tendinosis is a predisposing factor in tendon ruptures.
Initially validated in elite track and field athletes, BAMIC classifies hamstring injuries within the first 48 hours into five distinct grades, with further subclassification based on anatomic location. This system not only highlights the severity of the injury but also its location, providing a critical framework for determining rehabilitation protocols and guiding return-to-play decisions. This structured approach helps optimize recovery timelines and ensures athletes are ready to safely return to their sport.
The term “muscle injury” is generally preferred over “muscle strain,” and for injuries classified as grades 1-4, the term “tear” is commonly used. The anatomic classifications for muscle injuries are as follows:
- A = Myofascial
- B = Musculotendinous
- C = Intratendinous
In this classification scheme, intratendinous (type “C”) refers to injuries that affect the portion of a tendon or aponeurosis that lies within a muscle belly, not the free tendons at the ends of the muscle that attach to bone. When describing hamstring injuries, the proximal third refers to the region above gluteus maximus, while the distal third pertains to the area below the origin of the short head of the biceps femoris muscle.
The BAMIC classification assigns grades based on the anatomic extent of injury on the MRI images (Figure 6). Grade 0 injuries either have no MRI abnormality (but clinical findings of muscle injury) or patchy muscle edema. For grade 1-3 injuries, the amount of muscle edema (both as a percentage of the cross-sectional area on axial images and as a cranial-caudal length on long axis images) is used to assign a grade. Additionally, the length of disrupted fibers (if any) and the presence or absence of lost tension in the myotendinous unit proximal or distal to the injury is an additional factor. Grade 4 injuries show complete disruption of the myotendinous unit.
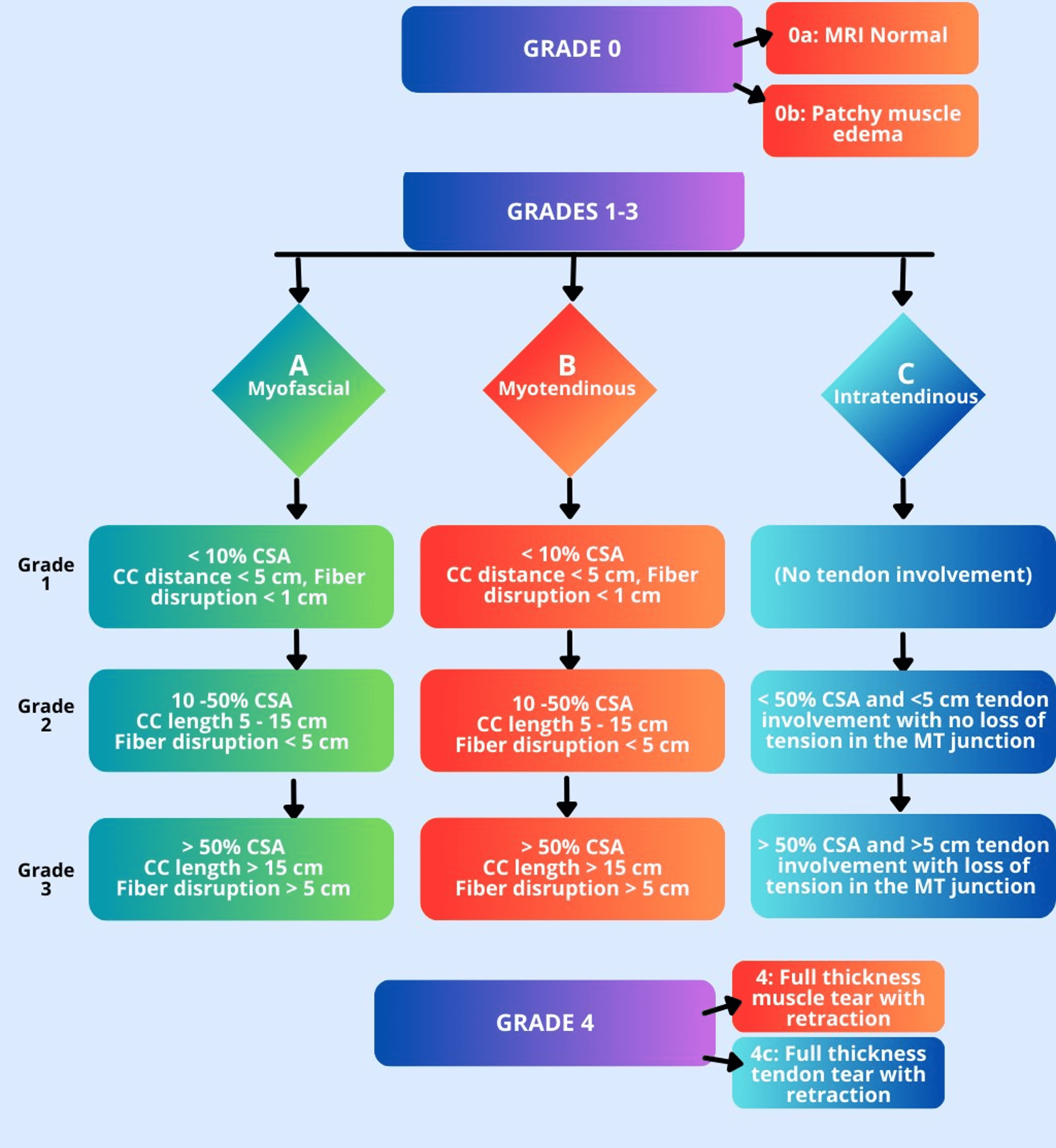
Figure 6: Diagram indicating the major criteria for applying the BAMIC classification. Grade 1-3 injuries are based on the maximum extent of injury on MRI, including how much of the muscle’s cross-sectional area (CSA) is affected by muscle edema (on the axial images), the maximum cranial-caudal (CC) extent of the muscle edema (on the long axis images), and the length of fiber disruption, if present.
Discussion
The long head of the biceps femoris is the most frequently injured muscle within the hamstring group, both in the case of initial and recurrent injuries.7 As discussed above, eccentric overloading is the primary mechanism responsible for biceps femoris injury (Figure 7). Proximal injuries tend to be more severe, and combined injuries to both the biceps femoris and semitendinosus have been associated with the greatest number of days missed among NFL athletes, highlighting the significant impact of these injuries on performance and recovery.8 In general, return to play times are greatest for grade 3 and 4 injuries, and shortest for grade 0 and 1 injuries (Figure 8).
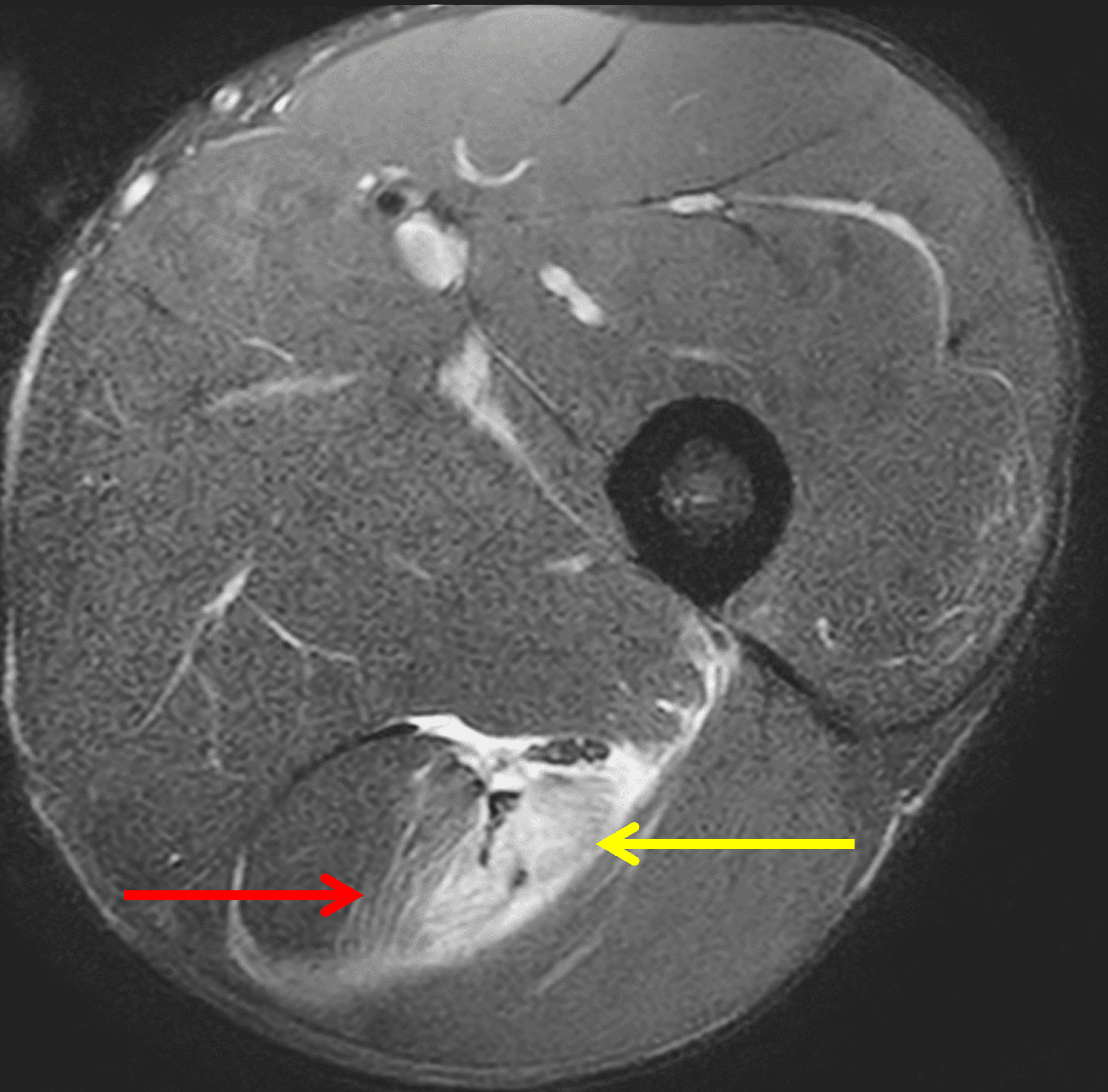

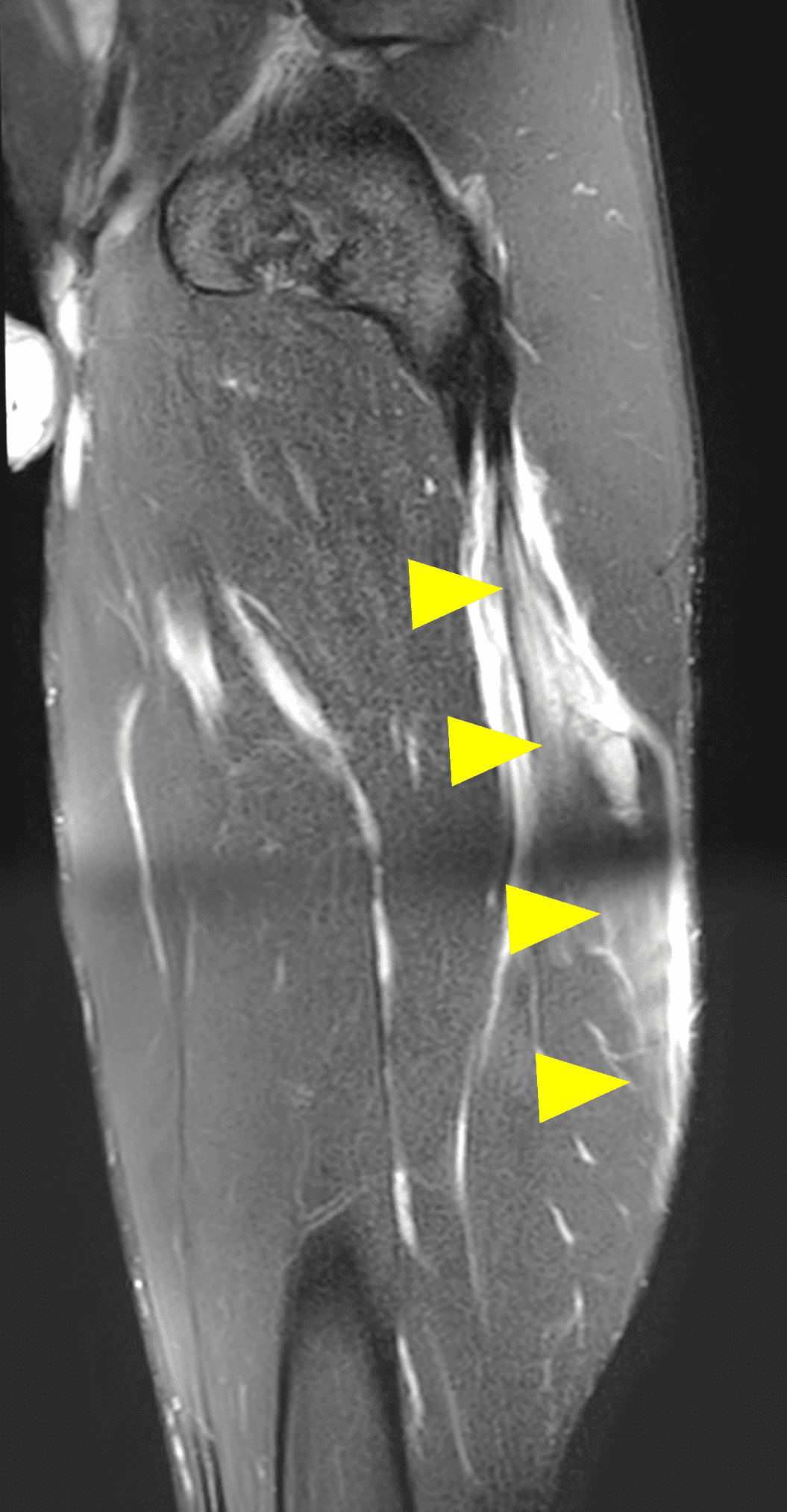
Figure 7: BAMIC Grade 3b injury in a 21-year-old collegiate football player with left proximal posterior thigh pain following a tackle during a game, which was accompanied by knee hyperextension. (7A) Axial fat-suppressed proton density weighted image shows myotendinous edema involving 100% of the long head biceps femoris cross-sectional area (yellow arrow). A low-grade injury is also present in the semitendinosus muscle (red arrow). Fat-suppressed proton density weighted (7B) coronal and (7C) sagittal images demonstrate the length of the biceps femoris muscle edema (arrowheads), which measured greater than 15 cm.
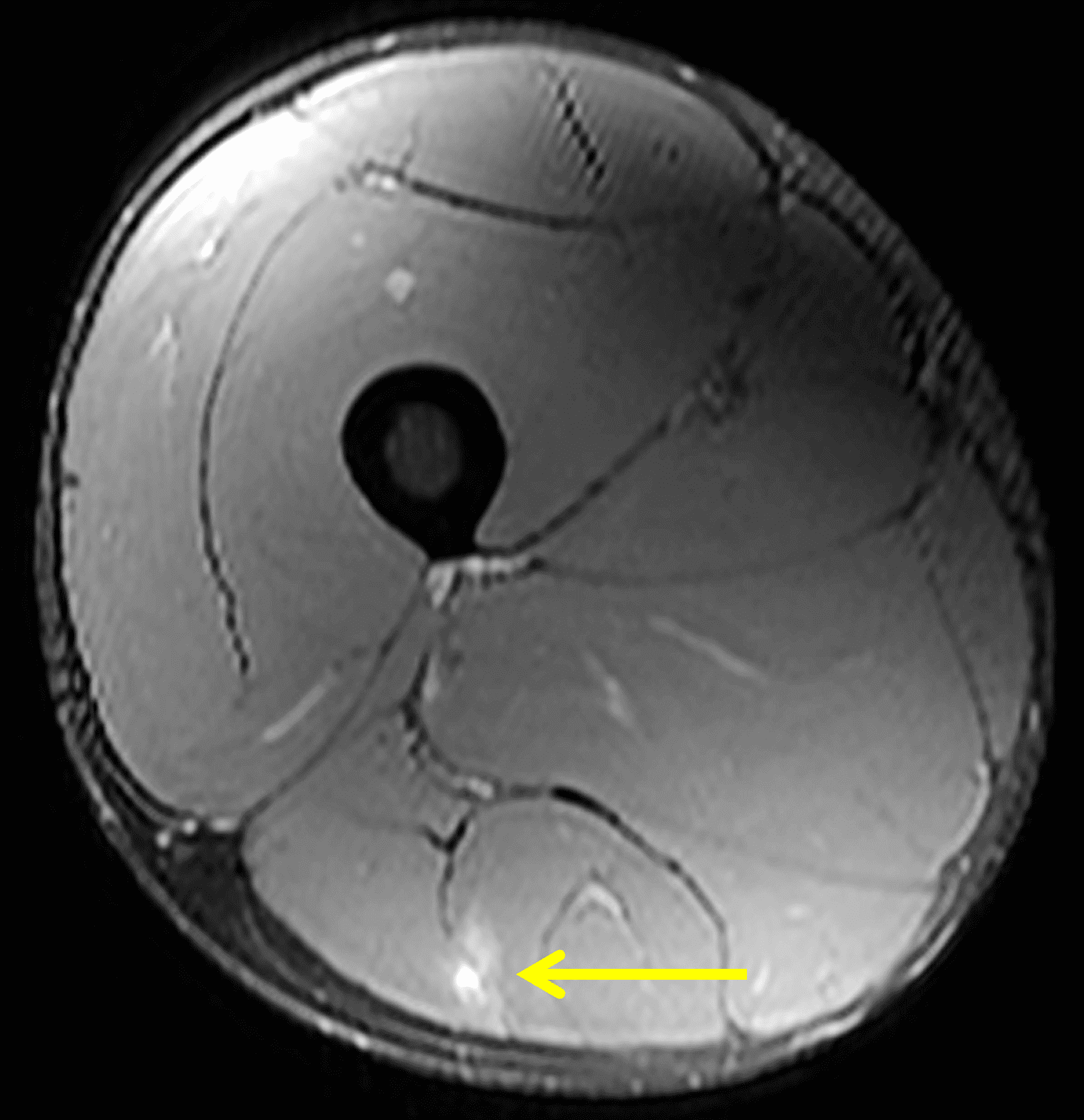
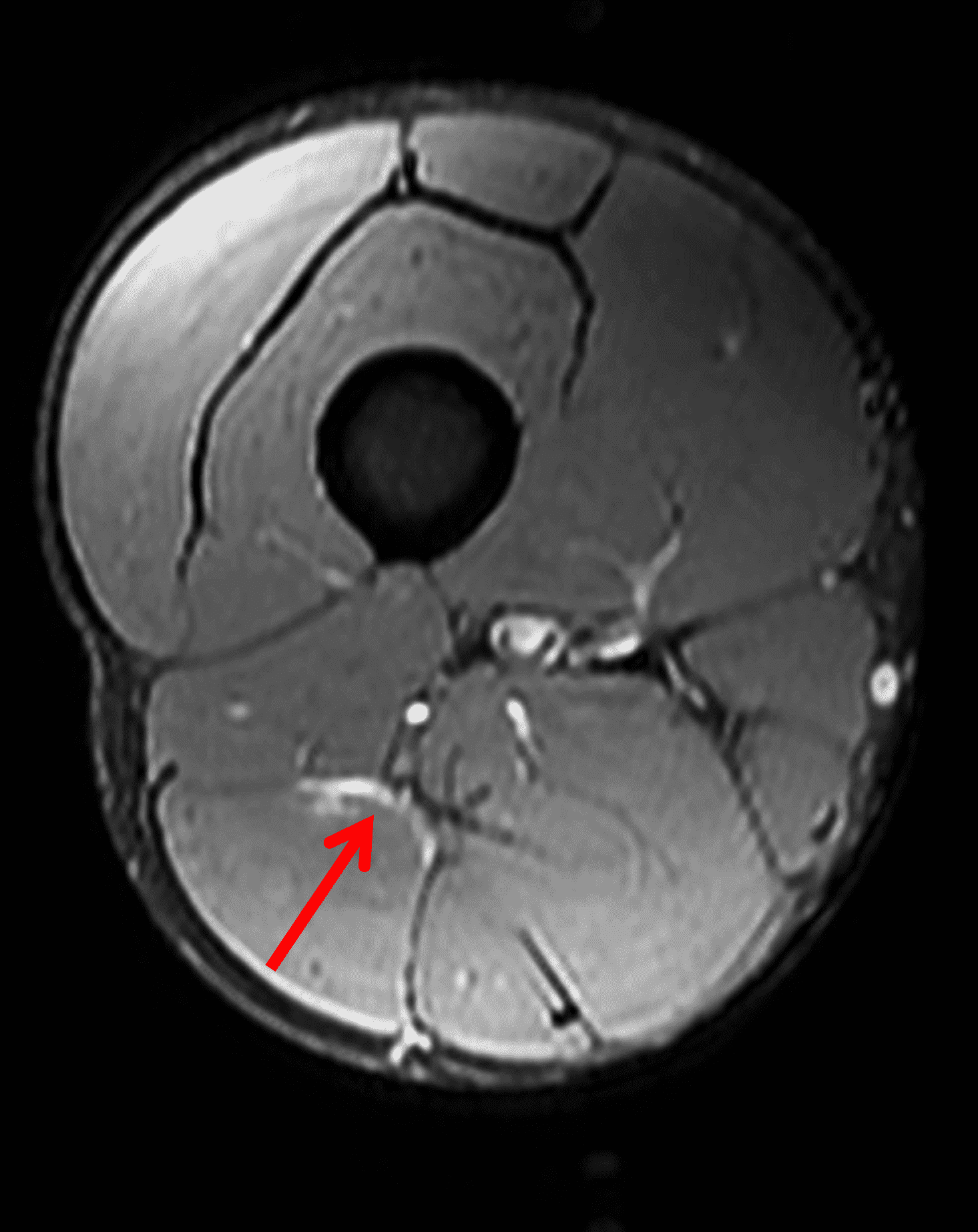
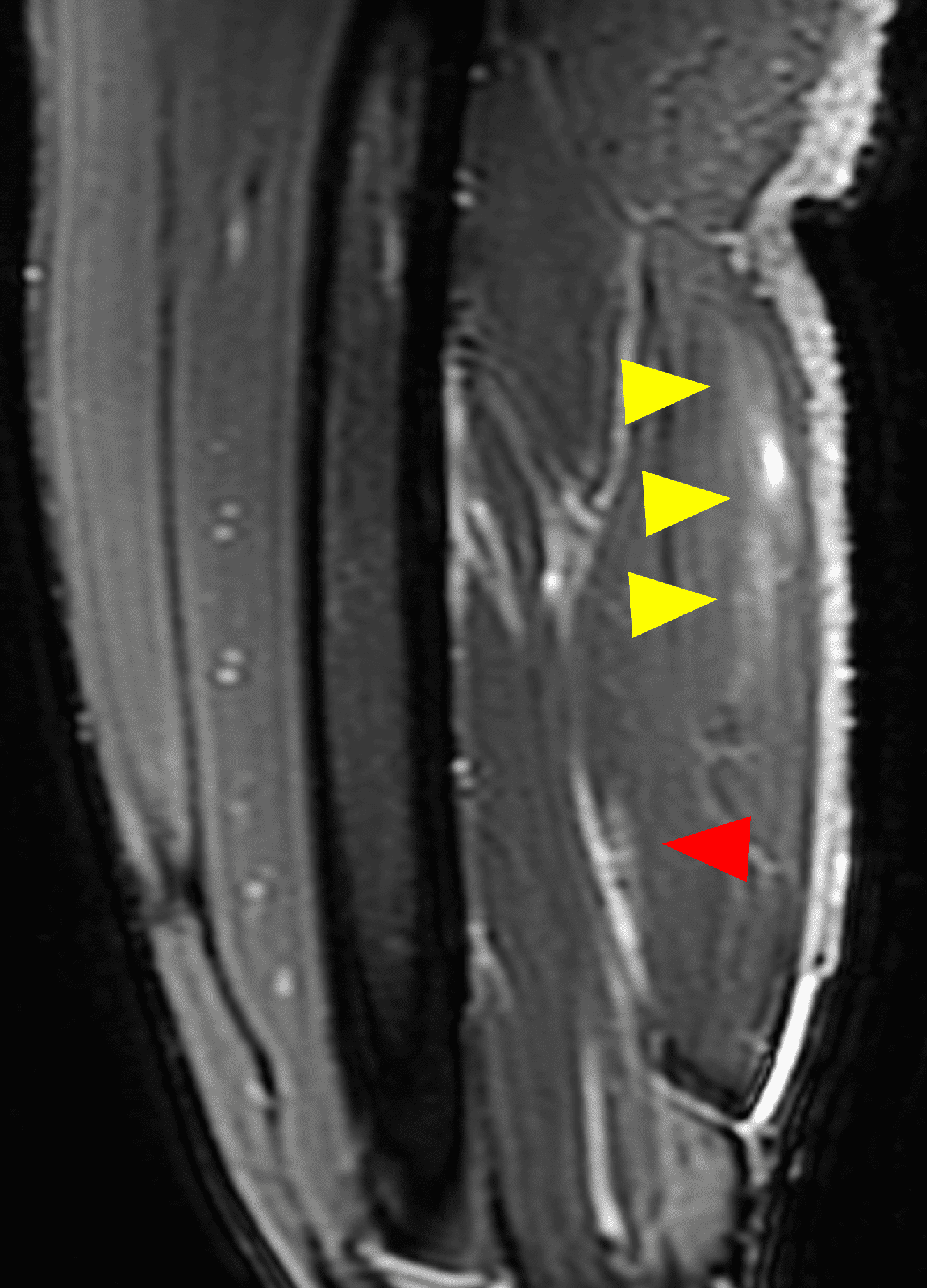
Figure 8: Low-grade long head biceps femoris injury in a 23-year-old professional football player. (8A) Axial STIR image in the mid-thigh shows edema centered at the myotendinous junction involving less than 10% of the cross-sectional area (yellow arrow). (8B) Axial STIR image in the distal thigh shows a second focus of peripheral edema at the myofascial junction (red arrow), again involving less than 10% of the cross section. (8C) Sagittal STIR image shows the length of the proximal injury between 5 and 15 cm (yellow arrowheads) and the distal injury less than 5 cm in length (red arrowhead). The proximal injury is grade 1b-2b, while the distal injury is grade 1a. The athlete returned to play 6 weeks later.
Due to the anatomic complexity of the biceps femoris T-shaped distal muscle-tendon junction, this region is also believed to be particularly susceptible to reinjury.9
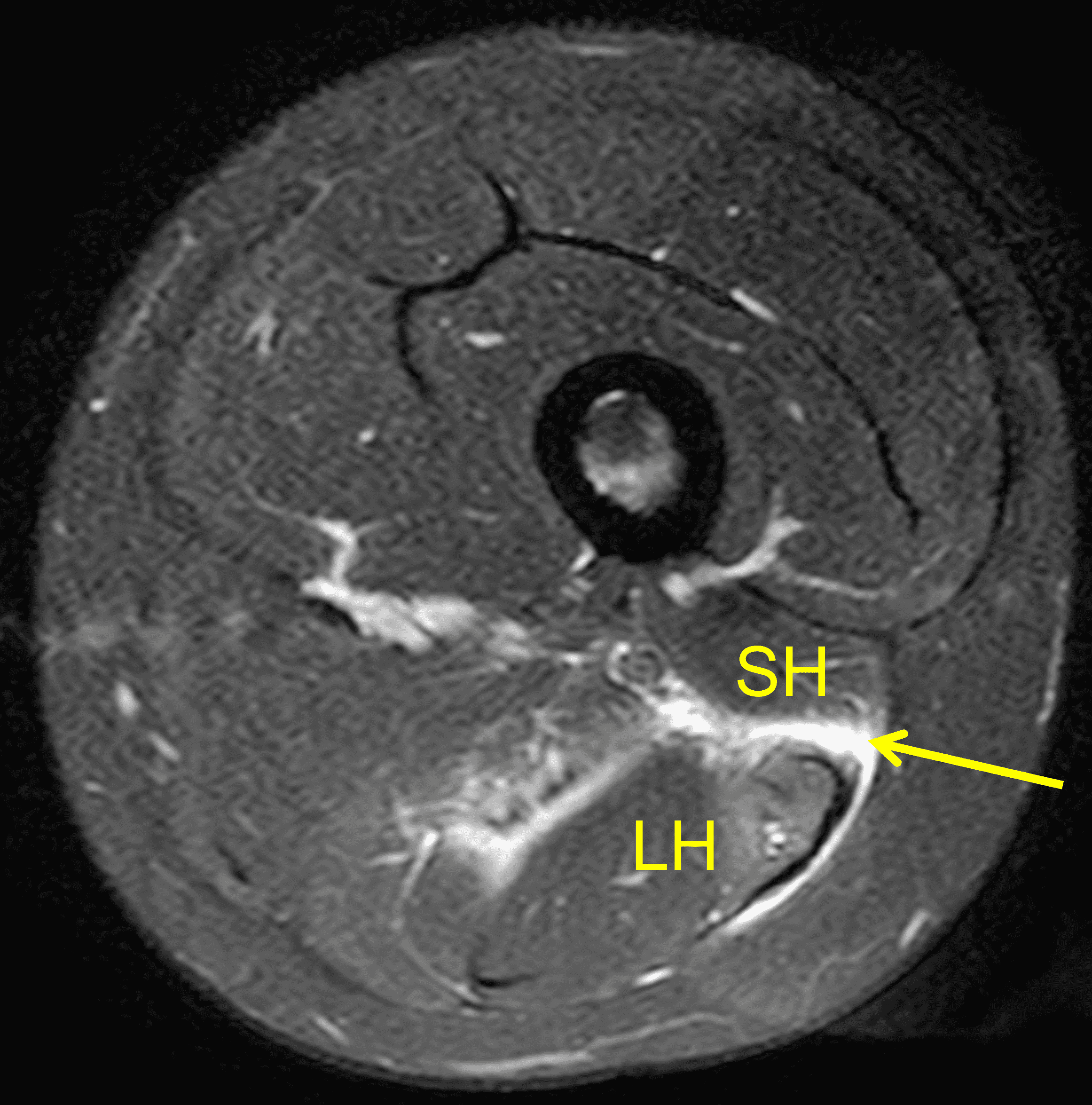
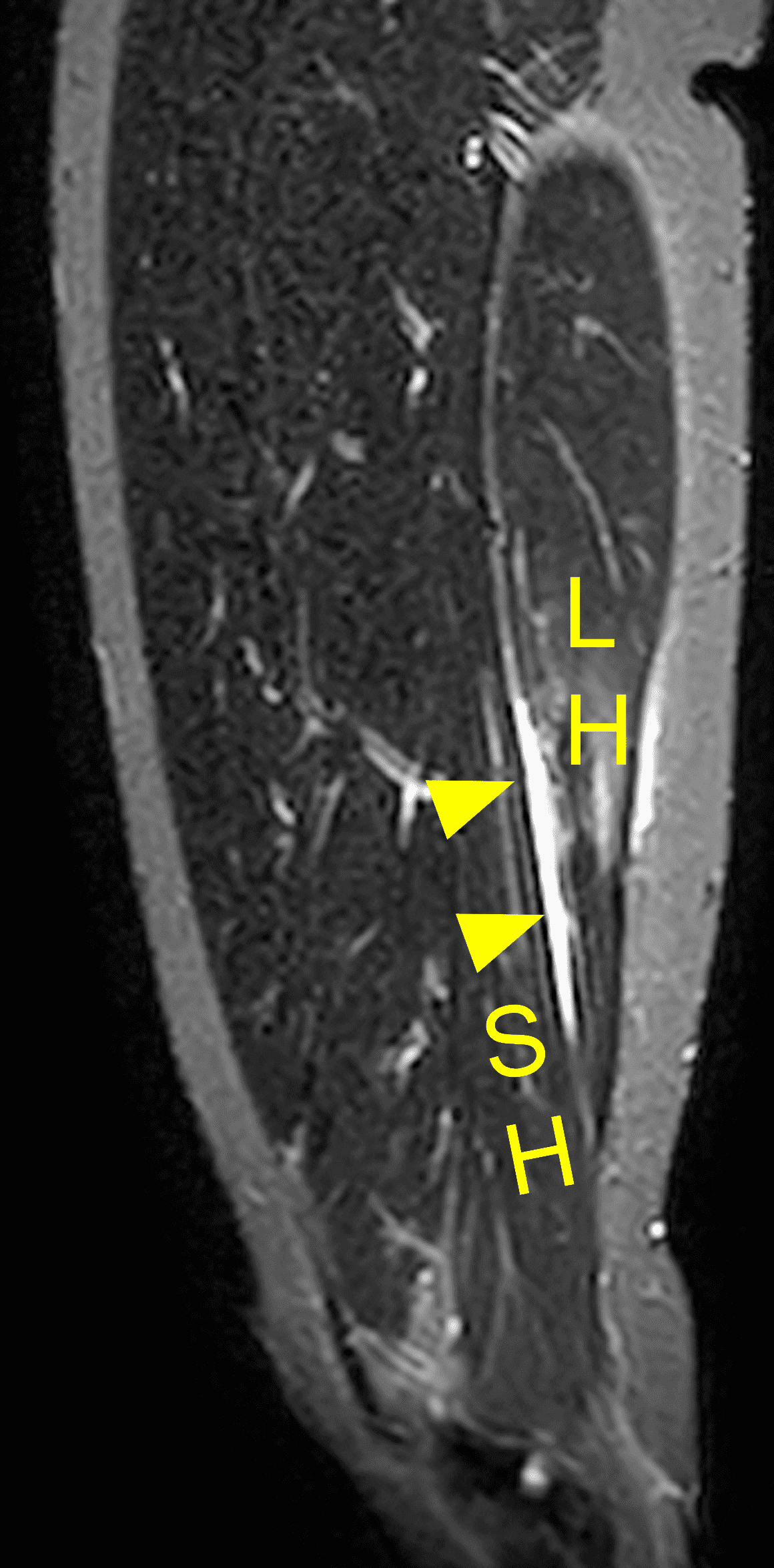
Figure 9: High-grade (BAMIC 3c) injury to the distal biceps femoris T-junction in a 22-year-old female who felt a pop during a long jump competition. (9A) Axial fat-suppressed proton density weighted image through the distal thigh shows disruption of the tendinous “T” (arrow) between the short head (SH) and long head (LH) muscle bellies. Edema involves approximately 30% of the LH cross-sectional area. (9B) Sagittal STIR image shows the tendinous disruption (arrowheads) measuring 6.6 cm between the long head (LH) and short head (SH) muscle bellies. Compare with Figure 5.
Debate exists whether intramuscular tendon involvement in hamstring injuries is associated with longer recovery times and a poorer prognosis.10 When the intramuscular tendon is injured (a type “c” lesion), some factors that appear to affect the recovery timeline include whether the tendon injury is classified based on the cross-sectional area of the tendon involved or the length of the affected tendon. This variation may stem from the orientation of the tear: longitudinal tears, which run parallel to the tendon fibers, tend to preserve tendon tension. On the other hand, tears that occur perpendicular to the tendon fibers can lead to tendon laxity, disrupting the tension and resulting in a prolonged recovery period. Interestingly, the distance of the injury from the tendon origin appears to have less significance in predicting recovery time compared to other factors. 11
While BAMIC was developed to classify hamstring injuries, it can also be applied to other muscle injuries.12
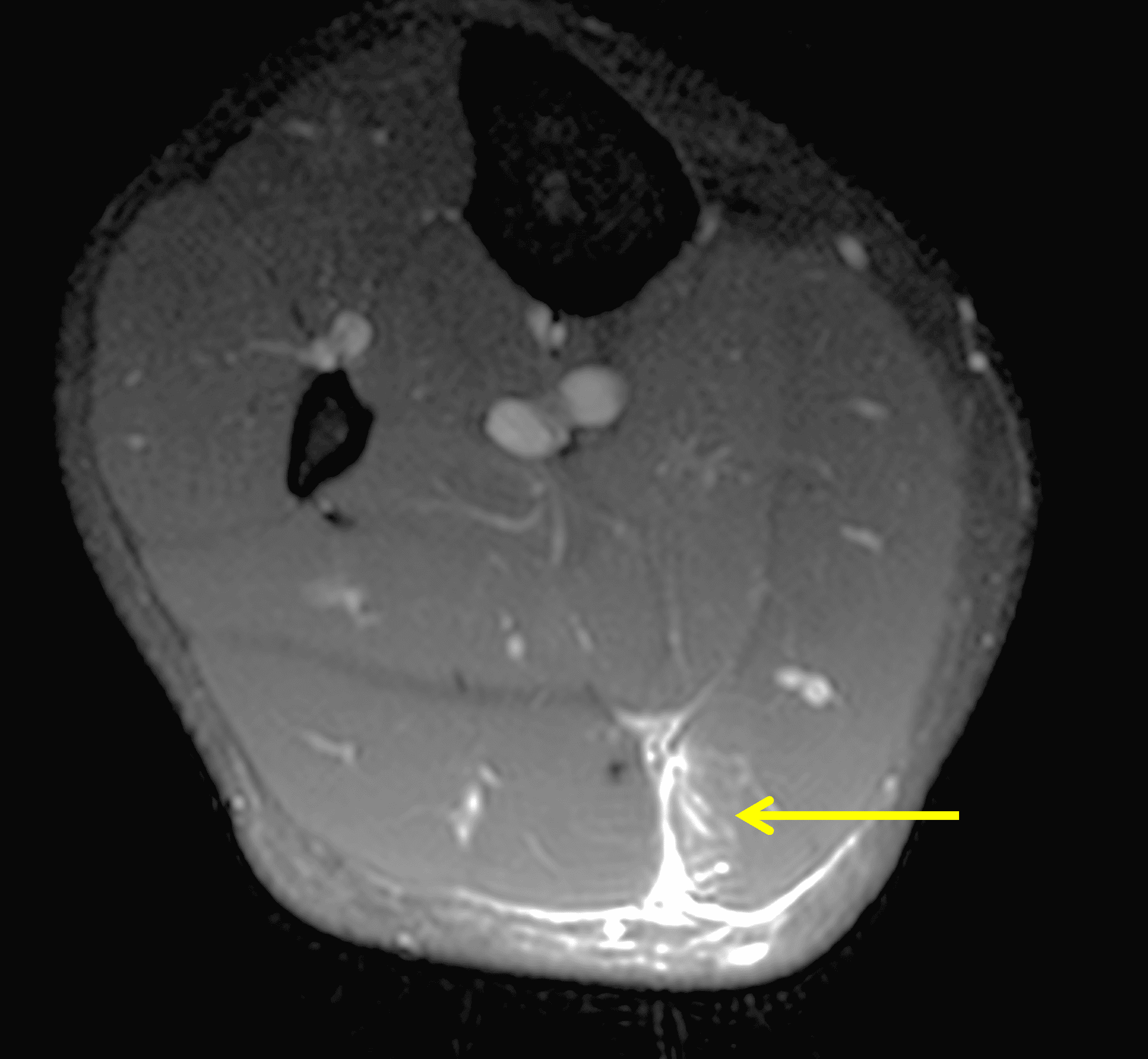
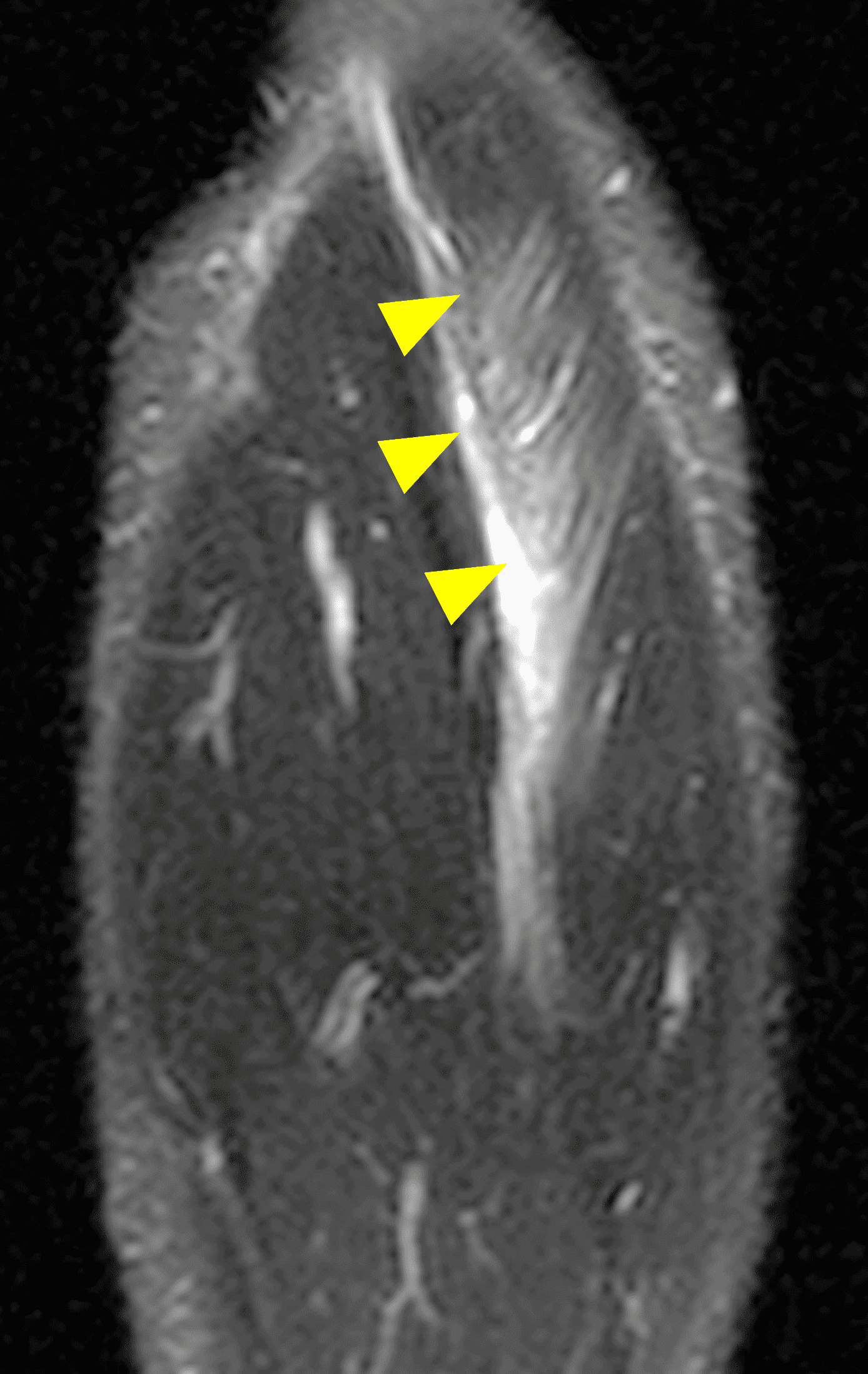
Figure 10: BAMIC grading applied to a proximal medial gastrocnemius injury in a 22-year-old football player who developed calf pain after feeling a pop. (10A) Axial proton density weighted SPAIR image shows a peripheral injury at the medial gastrocnemius myofascial junction (arrow). (10B) A coronal STIR image shows edema extending 7 cm in length (arrowheads). This injury is grade 2a using the BAMIC system, which was originally designed for hamstring injuries.
Conclusion
Hamstring muscle injuries are common in athletes, especially in running and kicking sports. Although MRI plays a vital role in assessing injury, it is just one component of a broader strategy aimed at achieving clear performance goals and guiding the rehabilitation process.
BAMIC is one of several MRI classification systems used to assess injury, but MRI alone cannot reliably predict when an athlete will return to sport after a hamstring injury.13 Additionally, variability in grading between different observers can undermine the accuracy and effectiveness of any classification system, reducing the ability to predict prognosis. Although BAMIC was originally developed for athletes who undergo MRI within 48 hours of injury, the timing of the MRI can vary for many patients, and the appearance of muscle edema and hemorrhage evolves over time.14
Regardless of the classification system used, it is essential to adopt a system that incorporates both anatomy and severity to more effectively identify prognostic indicators of recovery. To reduce confusion and ensure clear communication, radiologists should specify which classification system they are using when reporting their findings. It’s also important to recognize that some injuries have imaging characteristics that do not neatly fit into a single BAMIC category (e.g., the injury depicted in Figure 8), underscoring the need for a more descriptive approach in communicating severity.
References
- Rubin DA. Imaging diagnosis and prognostication of hamstring injuries. AJR Am J Roentgenol. 2012;199(3):525-533. doi:10.2214/AJR.12.8784 ↩
- Martin RL, Cibulka MT, Bolgla LA, et al. Hamstring Strain Injury in Athletes. J Orthop Sports Phys Ther. 2022;52(3):CPG1-CPG44. doi:10.2519/jospt.2022.0301 ↩
- Pollock N, James SL, Lee JC, Chakraverty R. British athletics muscle injury classification: a new grading system. Br J Sports Med. 2014;48(18):1347-1351. doi:10.1136/bjsports-2013-09330 ↩
- Linklater JM, Hamilton B, Carmichael J, Orchard J, Wood DG. Hamstring injuries: anatomy, imaging, and intervention. Semin Musculoskelet Radiol. 2010;14(2):131-161. doi:10.1055/s-0030-1253157 ↩
- Bertiche P, Mohtadi N, Chan D, Hölmich P. Proximal hamstring tendon avulsion: state of the art. J ISAKOS. 2021;6(4):237-246. doi:10.1136/jisakos-2019-000420 ↩
- Schache AG, Dorn TW, Blanch PD, Brown NA, Pandy MG. Mechanics of the human hamstring muscles during sprinting. Med Sci Sports Exerc. 2012;44(4):647-658. doi:10.1249/MSS.0b013e318236a3d2 ↩
- Macdonald B, McAleer S, Kelly S, Chakraverty R, Johnston M, Pollock N. Hamstring rehabilitation in elite track and field athletes: applying the British Athletics Muscle Injury Classification in clinical practice. Br J Sports Med. 2019;53(23):1464-1473. doi:10.1136/bjsports-2017-098971 ↩
- Day MA, Karlsson LH, Herzog MM, et al. Correlation of Player and Imaging Characteristics With Severity and Missed Time in National Football League Professional Athletes With Hamstring Strain Injury: A Retrospective Review. Am J Sports Med. 2024;52(11):2709-2717. doi:10.1177/03635465241270281 ↩
- Entwisle T, Ling Y, Splatt A, Brukner P, Connell D. Distal Musculotendinous T Junction Injuries of the Biceps Femoris: An MRI Case Review. Orthop J Sports Med. 2017;5(7):2325967117714998. Published 2017 Jul 20. doi:10.1177/2325967117714998 ↩
- Beattie CE, Barnett RJ, Williams J, Sim J, Pullinger SA. Are return-to-play times longer in lower-limb muscle injuries involving the intramuscular tendon? A systematic review. J Sci Med Sport. 2023;26(11):599-609. doi:10.1016/j.jsams.2023.10.002 ↩
- Pollock N, Kelly S, Lee J, et al. A 4-year study of hamstring injury outcomes in elite track and field using the British Athletics rehabilitation approach. Br J Sports Med. 2022;56(5):257-263. doi:10.1136/bjsports-2020-103791 ↩
- Pezzotta G, Querques G, Pecorelli A, Nani R, Sironi S. MRI detection of soleus muscle injuries in professional football players. Skeletal Radiol. 2017;46(11):1513-1520. doi:10.1007/s00256-017-2729-z ↩
- Wangensteen A, Guermazi A, Tol JL, et al. New MRI muscle classification systems and associations with return to sport after acute hamstring injuries: a prospective study. Eur Radiol. 2018;28(8):3532-3541. doi:10.1007/s00330-017-5125-0 ↩
- de Visser HM, Reijman M, Heijboer MP, Bos PK. Risk factors of recurrent hamstring injuries: a systematic review. Br J Sports Med. 2012;46(2):124-130. doi:10.1136/bjsports-2011-090317 ↩
