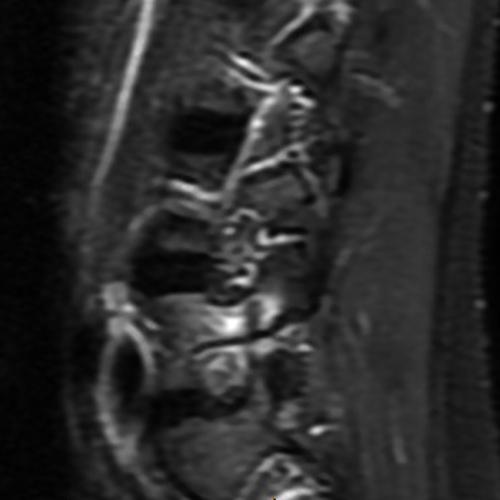
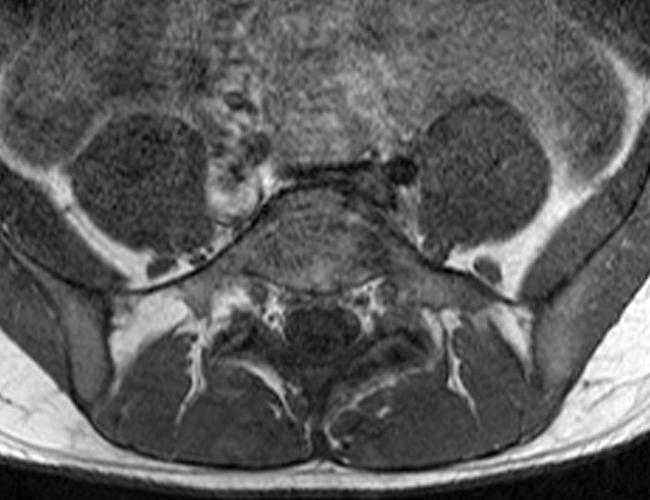
Case 1: 14-year-old female with back pain after a car accident. Axial T2-weighted (1A) and sagittal STIR (1B) images are provided. What are the findings? What is your diagnosis?

Case 2: 19-year-old male baseball player with acute onset of back pain after hitting a ball. Axial T1-weighted (2A) and T2-weighted (2B) images are provided. What are the findings? What is your diagnosis?

Findings
Case 1: T2-weighted axial (3A) and sagittal STIR (3B) sequences show marked cortical T2/STIR hyperintensity in the left pedicle of L5 surrounding a hypointense line (arrows) which begins at the inferior/medial margin of the pedicle and nearly completely traverses the pedicle.


Case 2: T1-weighted (4A) and T2-weighted (4B) axial images show T1 hypointensity and T2 hyperintensity (arrowheads) in the left lamina of L5 adjacent to a small hypointense line (arrows) which traverses the lamina.
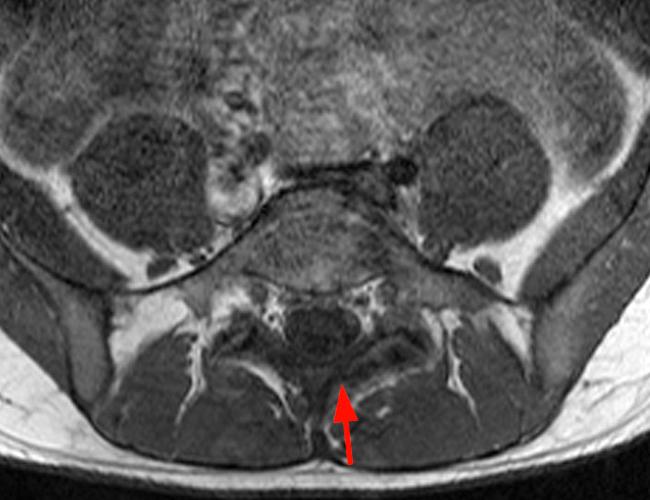
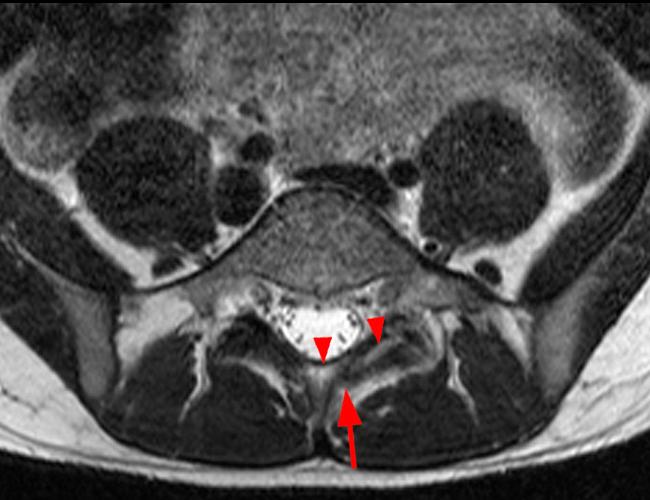
Case 1: Acute left-sided pediculolysis
Case 2: Acute left-sided laminolysis
Introduction
Spondylolysis is a commonly seen finding in lumbar imaging and classically involves unilateral or bilateral defects of the pars interarticularis (isthmus) of the vertebral body. However, an isthmic defect is only one of several recognized clefts that can occur in the lumbar vertebrae. Some of these clefts, such as the midline spinous cleft seen in spina bifida occulta, are congenital; others likely represent stress injuries. This article discusses two rare, less commonly recognized forms of non-isthmic stress-related spondylolysis: pediculolysis (also known as a retrosomatic cleft, or pedicular cleft), and laminolysis (also known as a retroisthmic cleft, or laminar cleft).1
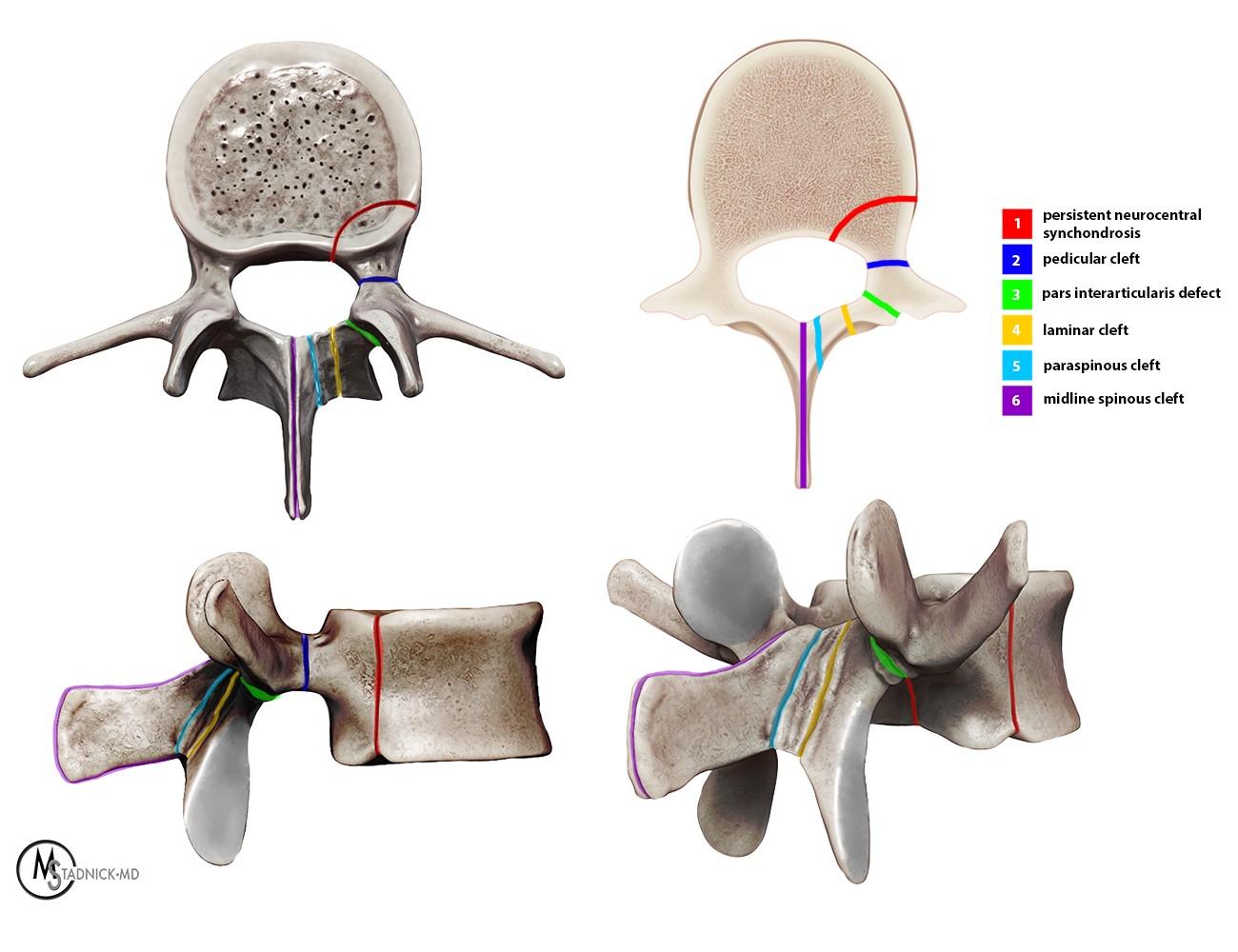
Figure 5: Axial, cross-sectional axial, lateral, and posterior oblique 3D views of a lumbar vertebral body demonstrate the six types of neural arch defects in the lumbar spine. 1: persistent neurocentral synchondrosis; 2: pedicular cleft (pediculolysis or retrosomatic cleft); 3: classic pars interarticularis (isthmic) defect; 4: laminar cleft (laminolysis or retroisthmic cleft); 5: paraspinous cleft; 6: midline spinous cleft (spina bifida or spina bifida occulta).
As in typical isthmic spondylolysis, pediculolysis and laminolysis most commonly affect the L5 vertebral body, followed by L4 in frequency of involvement. Pediculolysis can occur anywhere in the spine, but laminolysis has not been reported above the level of L3.2 Although isthmic spondylolysis is reported in 5-8% of the adult population, the incidence of pediculolysis and laminolysis is not known.
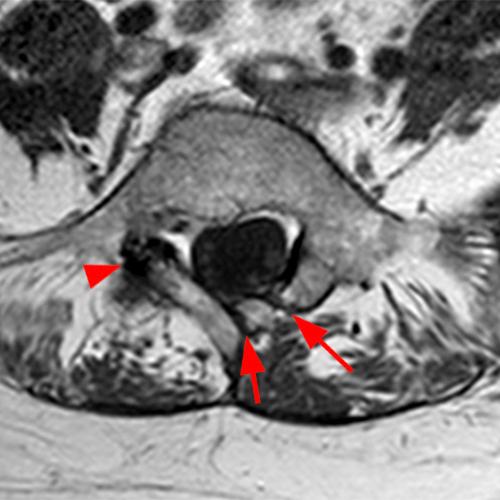
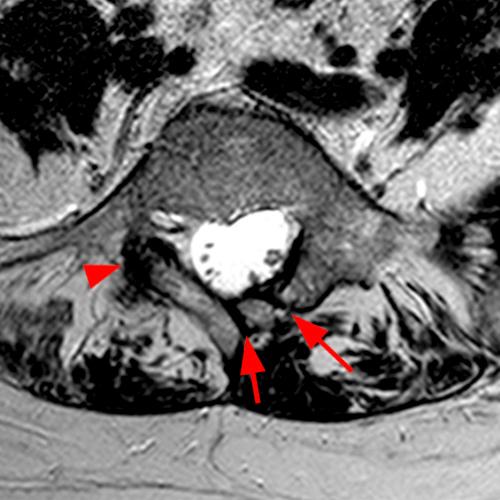
Figure 6: 55-year-old female with lower back pain. Axial T1-weighted (6A) and T2-weighted (6B) images show chronic left-sided paraspinous (short arrow) and laminar (arrow) clefts and a chronic right-sided isthmic defect (arrowheads) at L5.
Although some cases likely have a congenital component, pediculolysis and laminolysis are generally accepted as representing stress injuries in a majority of patients.3 Laminolysis can be associated with isthmic spondylolysis (Figure 6) or congenital anomalies of the vertebral body such as contralateral hypoplastic pedicle. Repetitive extension loading has also been proposed as a mechanism for laminolysis. Pediculolysis is commonly seen in athletes who engage in sports with a repetitive shearing or rotational component, such as volleyball players, ballet dancers, weightlifters, gymnasts, and baseball players. Pediculolysis (Figure 7) is also frequently associated with unilateral or bilateral isthmic spondylolysis, most likely due to secondary altered biomechanics.4,5
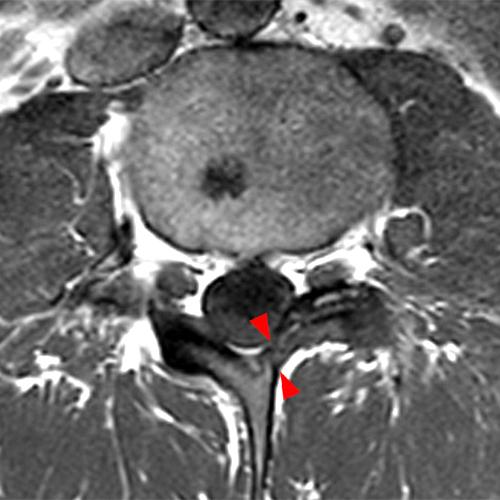
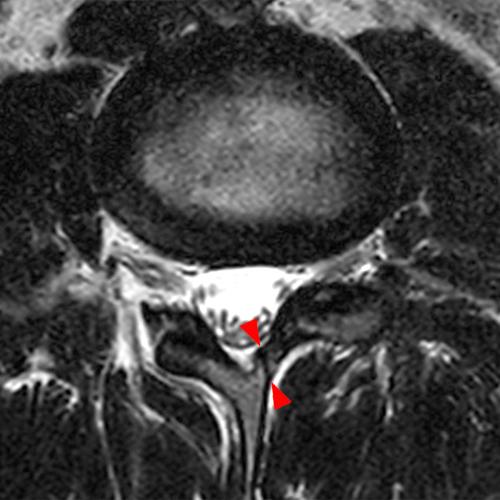
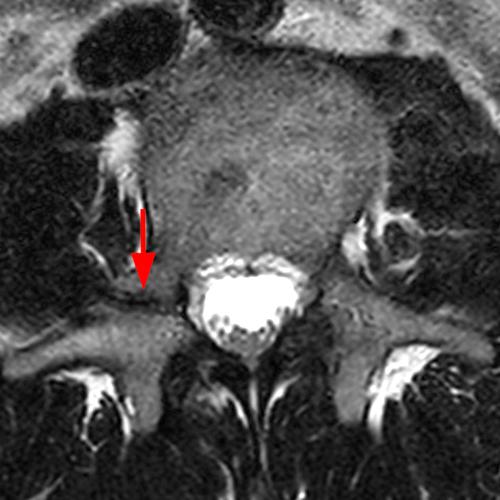

Figure 7: Rare case of chronic left-sided laminolysis and chronic right-sided pediculolysis at L3 in a 31-year-old male firefighter with hip pain. Axial T-weighted (7A) and T2-weighted (7B) images show a small, well-demarcated cleft (arrowheads) with minimal associated bony hypertrophy in the left lamina of L3, and axial T2-weighted (7C) and sagittal T1 weighted (7D) images show a well-demarcated cleft (arrows) with bony hypertrophy in the right pedicle of L3. No significant edema is present.
Clinical presentation
Spondylolysis typically presents as activity related lower back pain in people between the ages of 5 and 20, although cases of pediculolysis have been reported in older patients.6 The clinical presentation of pediculolysis and laminolysis does not significantly differ from that of isthmic spondylolysis.7 Chronic pediculolysis or laminolysis can also be an asymptomatic incidental finding.
Patients with underlying diseases that cause weakening of the bones, such as osteoporosis, osteopetrosis, or osteogenesis imperfecta, are more susceptible to pediculolysis or laminolysis. Pediculolysis has also been reported after laminectomies or microdiscectomies, and in association with compression fractures.8 Other conditions that cause increased or abnormal stress on the spine, such as cerebral palsy or Scheuermann’s disease, can also predispose patients to various types of spondylolysis.
MRI findings
MRI is indicated in patients who have back pain and negative plain films, but a high degree of clinical suspicion for spondylolysis. MRI is the modality of choice for evaluation of acute to subacute pediculolysis or laminolysis due to its ability to detect cortical edema. In acute pediculolysis, linear T1/T2 hypointensity is commonly seen beginning at the inferior margin of the pedicle, with adjacent T1 hypointensity and T2/STIR hyperintensity due to cortical edema (Figure 8). Over time, the defect can heal with osseous bridging, or progress to a chronic defect, with development of sclerotic, T1/T2 hypointense margins and resolution of cortical edema (Figure 9).
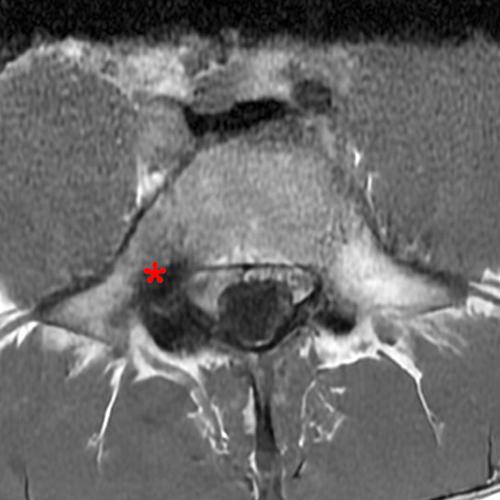
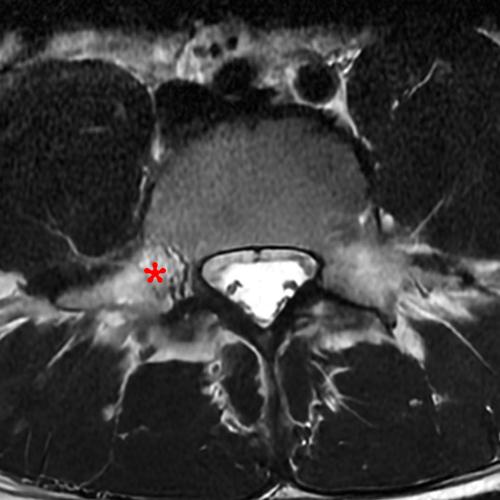

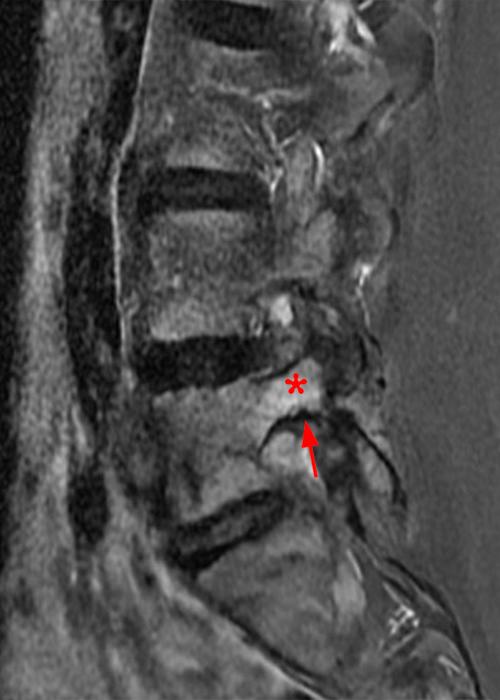
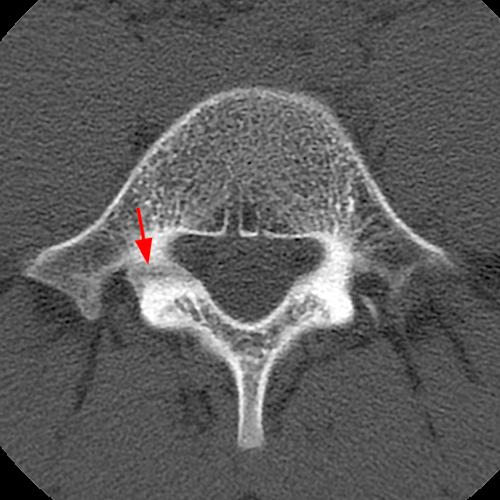
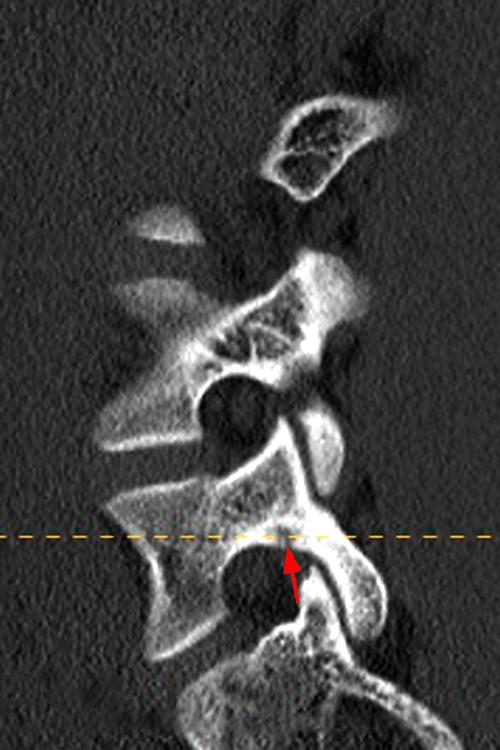
Figure 8: 14-year-old male with activity-related back pain. T1-weighted axial (8A) and sagittal (8C) and T2-weighted axial (8B) and sagittal (8D) MRI images demonstrate moderate cortical edema in the right pedicle of L5 (asterisks) with a minimal focus of hypointensity (arrows) at the inferior cortical margin of the pedicle. Axial (8E) and sagittal (8F) reconstructed CT images performed one week after the MRI reveal a small lucency (arrows) at the inferior margin of the pedicle, confirming the diagnosis of early, acute pediculolysis. Note that the extensive cortical edema seen on MRI is not appreciated on CT.
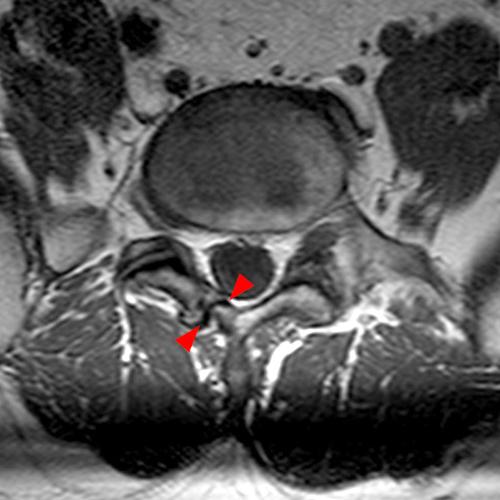
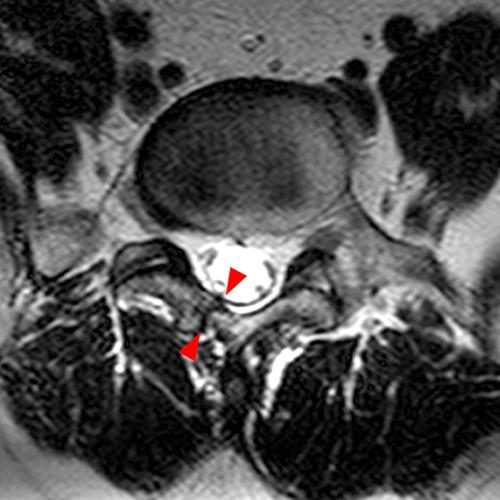

Figure 9: 55-year-old male with chronic back pain and numbness. Axial T1-weighted (8A) and T2 weighted (8B) images show a well-demarcated defect (arrowheads) in the right lamina of L5 with hypointense margins, bony hypertrophy, and no associated cortical edema, consistent with chronic laminolysis. The patient also has bilateral chronic isthmic spondylolysis at L5 (arrow) demonstrated on the sagittal T2-weighted image.
Acute laminolysis is more difficult to detect and can present as isolated T2 hyperintensity in the lamina without an obvious defect or linear sclerosis. The natural course of laminolysis is less well understood, but normalization of the appearance of the lamina or progression to a chronic, well-marginated laminar defect can be seen. A laminolysis defect is typically solitary, although multiple synchronous laminar defects have been reported.9
Viswanathan et al. describe a progression of the MRI appearance of pediculolysis and laminolysis consisting of an acute healing phase with T1 hypointensity and T2/STIR hyperintensity followed by a “chronic hypertrophic fibrous union” with T1/T2 hypointensity and bony hypertrophy.10
CT findings
CT is not a first line imaging modality for diagnosis of acute pediculolysis or laminolysis due to its inability to demonstrate cortical edema but is an excellent modality for evaluation of chronic defects, which appear on CT as a well-circumscribed lucent line with sclerotic margins that traverses the pedicle or lamina (Figure 9). Bony hypertrophy can also be seen (Figure 10).

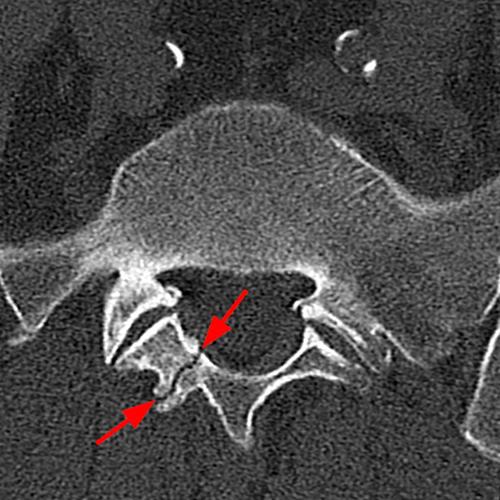

Figure 10: A 66-year-old male with severe back pain. Axial CT images (10A and 10B) demonstrate a well-circumscribed linear defect in the right lamina of L5 with sclerotic borders and bony hypertrophy, consistent with chronic laminolysis. A chronic left-sided isthmic spondylolysis (arrowheads) is also noted at L5 on a sagittal reconstructed CT image.
Other imaging modalities
Plain films are not adequate for the detection of acute pediculolysis or laminolysis. Chronic pediculolysis may be detected on plain films, but CT and MRI are preferred modalities for diagnosis due to superior anatomic resolution.
SPECT studies are highly sensitive for the diagnosis of active lesions of pediculolysis or laminolysis. SPECT is useful in determining whether a lesion is causing symptoms, with increased radiotracer uptake typically seen in active lesions. However, the spatial resolution of SPECT is not ideal for localization of lesions, and supplemental imaging with CT or MRI is usually indicated. The sensitivity of SPECT for detection of chronic lesions is low. SPECT imaging can be useful in monitoring treatment response.11
Treatment
Young patients with pediculolysis and laminolysis demonstrating T2 hyperintensity on MRI respond well when treated conservatively with bracing, rest, and abstinence from sports. In laminolysis, reduction of extension loading is specifically indicated. A trial of 3-6 months of conservative treatment is generally recommended before surgical intervention is considered.12,13 Surgical repair of symptomatic chronic defects, especially those with associated instability, may involve direct repair of the defect with compression screws, and/or lumbar fusion.14,15 The age and activity level of the patient are also taken into consideration; most defects in the elderly are treated conservatively, frequently including the use of medications that treat osteoporosis.
Conclusion
Pediculolysis and laminolysis are uncommon causes of symptomatic spondylolysis and should be considered in adolescents with activity related back pain and normal plain films. Accurate and early diagnosis is critical to allow initiation of conservative management for symptomatic relief and prevention of progression to chronic spondylolysis.
References
- Viana, S. L., De Carvalho Barbosa Viana, M. A., & De Alencar, E. L. C. (2015). Atypical, unusual, and misleading imaging presentations of pondylolysis. Skeletal Radiology, 44(9), 1253–1262. https://doi.org/10.1007/s00256-015-2138-0 ↩
- Nakayama, T., & Ehara, S. (2014). Spondylolytic spondylolisthesis: various imaging features and natural courses. Japanese Journal of Radiology, 33(1), 3–12. https://doi.org/10.1007/s11604-014-0371-4 ↩
- Wick, L. F., Kaim, A., & Bongartz, G. (2000). Retroisthmic cleft: a stress fracture of the lamina. Skeletal Radiology, 29(3), 162–164. https://doi.org/10.1007/s002560050586 ↩
- Johansen, J. G., & Lilleås, F. G. (1991). Nonspondylolytic lateral clefts in the lumbar vertebral arch. In Springer eBooks (pp. 474–475). https://doi.org/10.1007/978-3-642-49329-4_172 ↩
- Kim, K. S., Kim, Y. W., & Kwon, H. D. (2006). Unilateral spondylolysis combined with contralateral lumbar pediculolysis in a military parachutist. Journal of Spinal Disorders & Techniques, 19(1), 65–67. https://doi.org/10.1097/01.bsd.0000161230.87271.f3 ↩
- Viswanathan, V. K., Shetty, A. P., Jakkepally, S., Kanna, R. M., & Rajasekaran, S. (2020). Symptomatic Unilateral Pediculolysis Associated with Contralateral Spondylolysis and Spondylolisthesis in Adults—Case Report and Review of Literature. World Neurosurgery, 143, 339–345. https://doi.org/10.1016/j.wneu.2020.08.055 ↩
- Sakai, T., Sairyo, K., Takao, S., Kosaka, H., & Yasui, N. (2010). Adolescents with symptomatic laminolysis: report of two cases. Journal of Orthopaedics and Traumatology, 11(3), 189–193. https://doi.org/10.1007/s10195-010-0101-3 ↩
- Smith, J. L., Goorman, S. D., Baron, J. M., Curtin, S. L., & Lewandrowski, K. (2006). Three-level bilateral pediculolysis following osteoporotic lumbar compression fracture. The Spine Journal, 6(5), 539–543. https://doi.org/10.1016/j.spinee.2006.01.013 ↩
- Sakai, T., Sairyo, K., Mase, Y., & Dezawa, A. (2012). Synchronic multiple stress fractures of L5 left hemilamina: a case of an unusual type of lumbar spondylolysis. European Journal of Orthopaedic Surgery & Traumatology, 22(S1), 41–43. https://doi.org/10.1007/s00590-012-0953-8 ↩
- Viswanathan, V., Manoharan, S. R. R., & Subramanian, S. (2016). Symptomatic unilateral spondylolysis associated with nonspondylolytic lateral clefts in adults: Review of an infrequently reported pathology. Cureus. https://doi.org/10.7759/cureus.928 ↩
- Abraham, T., Holder, L., & Silberstein, C. (1997). The retroisthmic cleft scintigraphic appearance and clinical relevance in patients with low back pain. Clinical Nuclear Medicine, 22(3), 161–165. https://doi.org/10.1097/00003072-199703000-00005 ↩
- Miyagi, R., Sairyo, K., Sakai, T., Yoshioka, H., Yasui, N., & Dezawa, A. (2012). Two types of laminolysis in adolescent athletes. Journal of Orthopaedics and Traumatology, 13(4), 225–228. https://doi.org/10.1007/s10195-012-0206-y ↩
- Desouza, C., Jani, C., & Patil, V. (2022). Non-Isthmic spondylolysis imaging features: a case report. Journal of Orthopaedic Case Reports, 12(02), 42–44. https://doi.org/10.13107/jocr.2022.v12.i02.2658 ↩
- Kim, J., Kim, K., Suk, K., Lee, J., Lee, S., & Eoh, J. (2008). Fusion of pedicular cleft using pedicle screw fixation – a case report -. Journal of Korean Society of Spine Surgery, 15(2), 106. https://doi.org/10.4184/jkss.2008.15.2.106 ↩
- Parvataneni, H. K., Nicholas, S. J., & McCance, S. E. (2004). Bilateral pedicle stress fractures in a female athlete. Spine, 29(2), E19–E21. https://doi.org/10.1097/01.brs.0000105988.43472.2b ↩
