Clinical History
A 54-year-old man presents with left shoulder pain and decreased range of motion following an injury 3 months prior. Fat-suppressed, proton-density-weighted axial (1A) and coronal images (1B), and an oblique sagittal T2-weighted image (1C) are provided. What are the findings? What is your diagnosis?



Findings

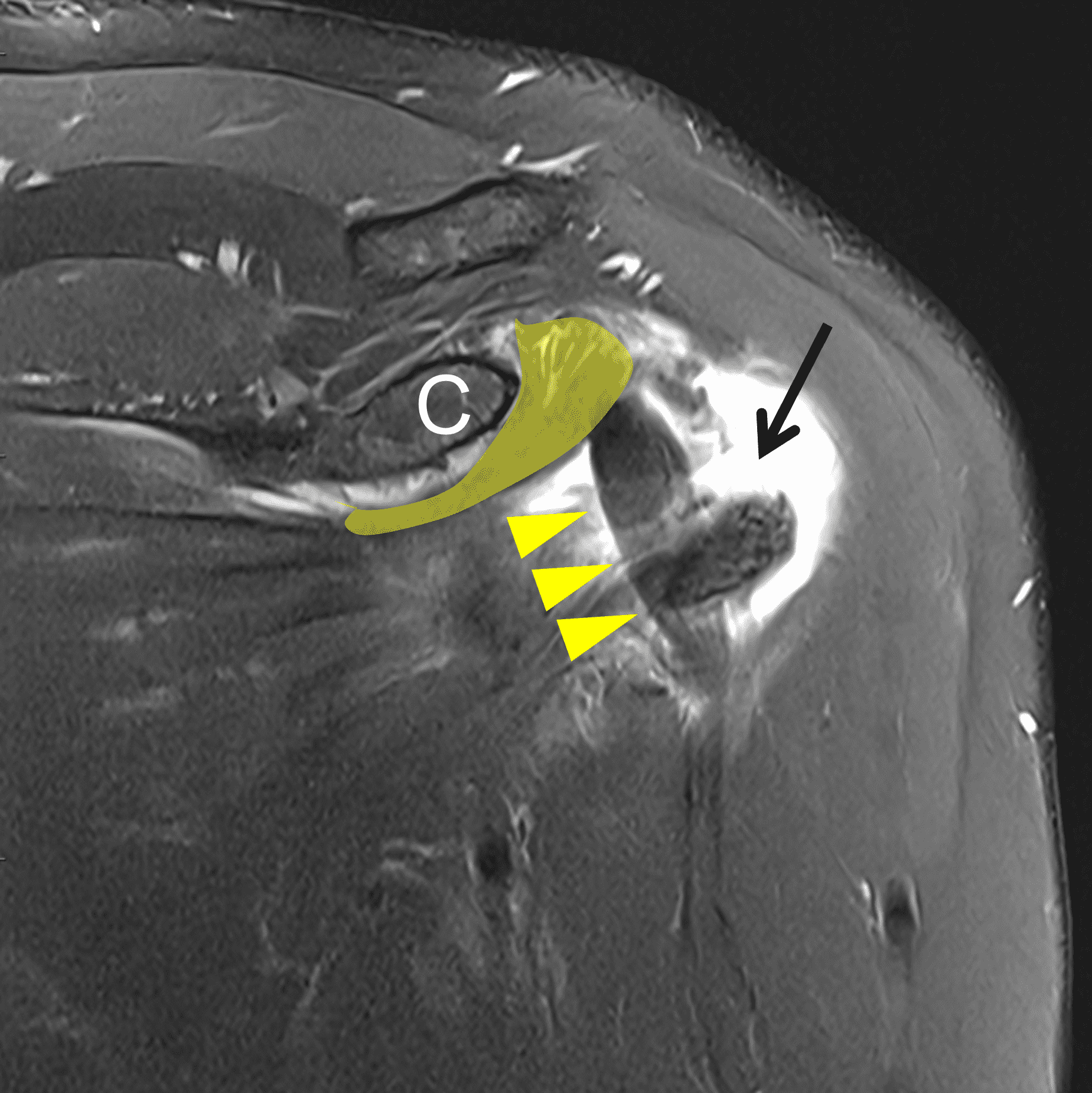

Figure 2: (2A) Axial image demonstrates a torn and retracted subscapularis tendon (solid arrow), empty bicipital groove (dotted arrow), and tendinosis of the medially dislocated long head biceps tendon (arrowhead). (2B) Oblique coronal image shows a fluid filled gap at the superior subscapularis tendon insertion (arrow), medially dislocated biceps tendon (arrowheads), and the comma sign (shaded) – a vertically-oriented curved band of soft tissue that partly wraps around the coracoid (C). The ‘comma’ is composed of the detached superior glenohumeral ligament, coracohumeral ligament, and medially retracted superolateral subscapularis. (2C) Oblique sagittal image shows the torn, retracted superior subscapularis tendon (shaded) displaced superomedially within the rotator interval.
Diagnosis
Subscapularis tendon tear with comma sign and medial dislocation of the long head biceps tendon.
Introduction
The subscapularis is the largest of the rotator cuff muscles. Its complex structure permits it to assist with both active and passive stabilization of the shoulder.1 Historically, subscapularis tears were thought to be uncommon.2 Advances in surgical techniques and imaging have increased awareness of subscapularis tears, with reported incidence ranging from 19–49%.2,3 These developments have highlighted the tendon’s role in stabilizing the glenohumeral joint and the biceps tendon,4,5 and have underscored the incidence of combined supraspinatus and subscapularis tears — termed “anterosuperior tears.”6 The clinical diagnosis of subscapularis tears remains challenging.7,8 A thorough understanding of the subscapularis anatomy, a systematic approach to evaluation of the MR images, and knowledge of common pitfalls in the assessment of the subscapularis tendon will improve the pre-operative diagnosis of this once hidden lesion.6,7,9
Isolated tears of the subscapularis tendon are uncommon.10 Subscapularis tears are typically chronic and combined with supraspinatus tears. Acute tears of the subscapularis may occur with forced hyperextension and abduction or external rotation, and with direct impact to the anterior shoulder as seen in football, rugby, and wrestling.8,10 Alternatively, a tear may occur due to repetitive overhead activity, impingement with microtrauma, resulting in tendon degeneration and subsequent tears as seen in swimming, tennis, and baseball.8 Impingement may occur between the tendon and anterior glenoid or with subcoracoid impingement.10 However, it should be noted that a narrowed coracohumeral interval, 10.5-11.5 mm, is a poor predictor of coracohumeral impingement.11 Additional studies conclude that narrowing of the subcoracoid space may be the result, rather than cause, of large cuff tears involving both the infraspinatus and subscapularis tendon, suggesting the combination of infraspinatus tear with muscle atrophy and subscapularis tear were requirements for narrowing of the coracohumeral distance, which is in part due to anterior translation of the humeral head.10,12,13
The comma sign (Figure 3) is a well-known arthroscopic finding initially described in 2003 by Lo and Burkhart.14 The sign is less well known amongst radiologists but can be accurately identified on pre-operative MR imaging.2,15 The comma sign serves as a surgical indicator of a full-thickness, retracted subscapularis tear. The tissue that comprises the comma sign is composed of the torn insertional fibers of the superior subscapularis, which is separated from the more caudal fibers and superiorly and medially displaced together with the superior glenohumeral ligament, and coracohumeral ligament. The torn fibers are pulled superiorly and cranially by a concomitant retracted supraspinatus tear.2 The concavity of the comma should be the coracoid process of the scapula (Figures 2 and 3).

Figure 3: A 3D rendering of the shoulder from an anterolateral oblique perspective. The central part of the coracoacromial ligament has been sectioned to better demonstrate the anatomy. The torn superolateral subscapularis tendon is displaced medially and cranially, wrapped around the base of the coracoid (C). The torn subscapularis tendon, coracohumeral ligament, and superior glenohumeral ligament are attached to the torn supraspinatus tendon and form the “comma sign” (asterisks).
Anatomy and function
The subscapularis muscle arises from the subscapularis fossa on the anterior portion of the scapula with a complex insertion on the proximal humerus.1 It is the largest rotator cuff muscle, accounting for 53% of the rotator cuff muscle mass.6 The superior and inferior portions of the muscle are innervated by the upper and lower subscapularis nerves respectively, each arising from the posterior cord of the brachial plexus.1,10 The multipennate tendinous, superior portion of the subscapularis is composed of 4 to 6 tendons that coalesce and account for approximately 60% of the tendon footprint (Figure 4).6 The tendinous insertion has a trapezoidal shape – wider superiorly and tapering distally – at the lesser tuberosity.1 The superior-most fibers of the subscapularis interdigitate with the anterior supraspinatus fibers, coracohumeral ligament, and the superior glenohumeral ligament to form the biceps pulley (Figure 5). Additionally, the superior subscapularis fibers contribute to the transverse humeral ligament.4,8,10 The inferior muscular portion inserts directly on the anterior humeral metaphysis distal to the lesser tuberosity.1

Figure 4: 19-year-old male with traumatic shoulder dislocation. Oblique sagittal T1-weighted image demonstrates the normal multipennate structure of the superior subscapularis with multiple tendons (arrowheads), which coalesce to the larger tendinous insertion on the lesser tuberosity, and the inferior portion (asterisk), which has a muscular insertion distal to the lesser tuberosity.

Figure 5: 3D rendering of the shoulder from an anterolateral oblique perspective. A “window” has been created in the coracohumeral ligament to better demonstrate the contributions of the coracohumeral ligament, superior glenohumeral ligament, anterior aspect of the supraspinatus, and superior subscapularis to form the biceps pulley. The pulley stabilizes the long head biceps tendon as it enters the bicipital groove where it continues deep to the transverse humeral ligament.
The subscapularis is the only rotator cuff muscle that internally rotates the arm, working synergistically with the pectoralis major, teres major, and latissimus dorsi.1,6,10 The superior subscapularis muscle assists with abduction while the inferior fibers contribute to adduction.10 The subscapularis muscle provides passive stability to the glenohumeral joint, buttressing the anterior joint capsule, particularly in abduction and external rotation.1,6 The subscapularis muscle actively stabilizes the joint by opposing the superior force of the deltoid muscle in the coronal plane and opposing the infraspinatus in the axial plane, maintaining appropriate glenohumeral alignment throughout a broad range of motion.1,6,10
The subscapularis insertion on the lesser tuberosity can be divided into 4 facets, with the larger, superior tendonous portion inserting on the first and second facets, occupying 34% and 28% of the entire footprint respectively (Figure 6).16 On MR imaging the superior (first) facet is wide and flat in the axial plane. A bony ridge, seen on oblique sagittal images, demarcates the first and second facet, with the second facet being more vertical on the sagittal images and a narrow prominence on the axial images. The third facet can be distinguished from the second as the subscapularis insertion transitions from muscular to tendinous and an additional osseous ridge.16,17

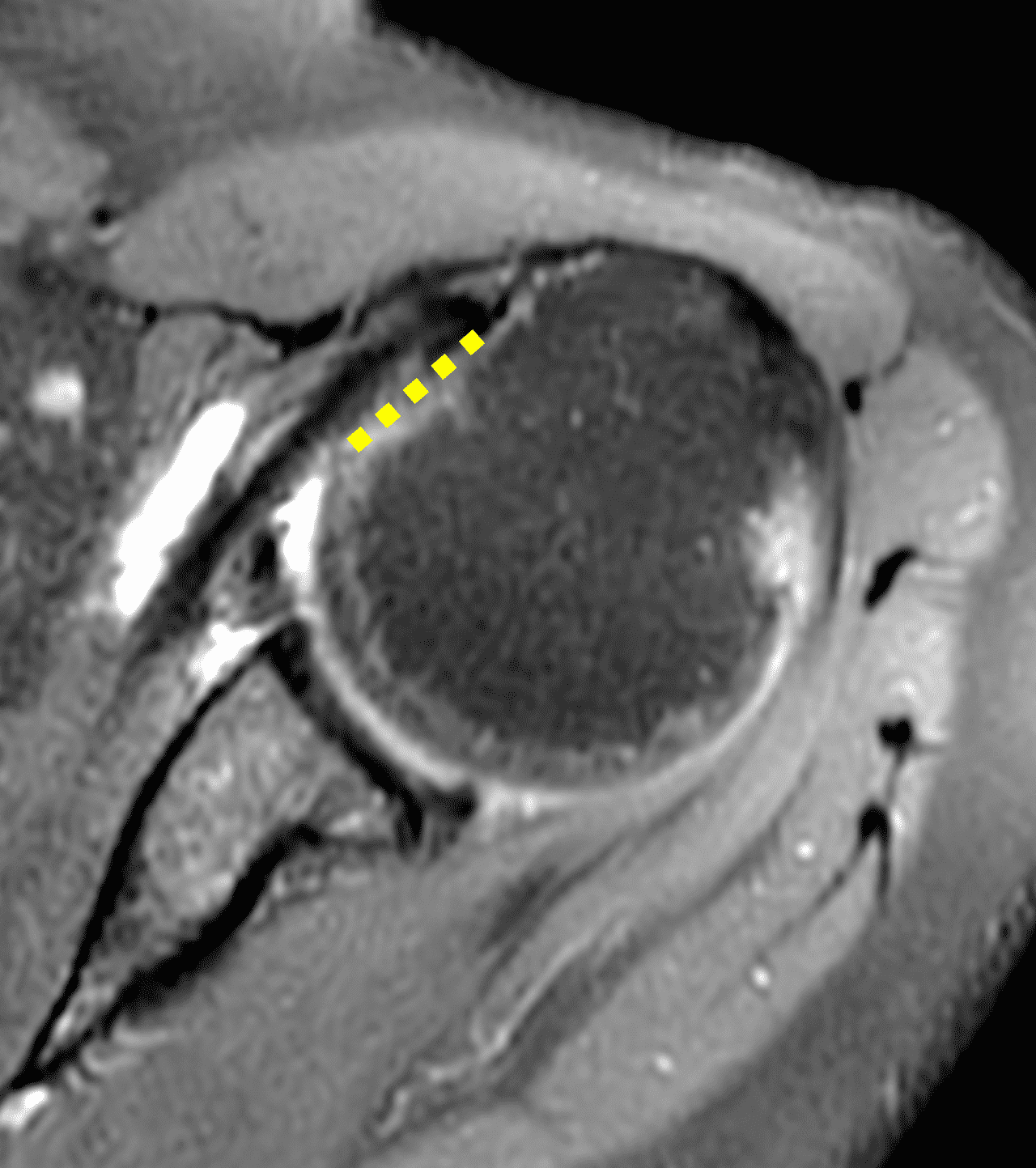

Figure 6: 44-year-old woman with 8-week history of shoulder pain and a labral tear (not shown). (6A) Sagittal T2-weighted image demonstrates the anterior osseous ridge (arrow) described by Yoo and Rhee,16 between the superior first lesser tuberosity facet (red arrowheads) and the more inferior and smaller second facet (black arrowhead). (6B and 6C) Axial proton density-weighted, fat suppressed images show the larger first facet (6B, dashed line) located cranial and lateral to the second, smaller facet (6C, solid line).
Clinical Findings
Symptoms in patients with subscapularis tears vary with severity, chronicity, and associated pathology. Patients typically present with dull, aching anterior shoulder pain aggravated by overhead movements and reaching across the body. Pain may be accompanied by weakness with internal rotation and difficulty lifting heavy objects, and with certain exercises including push-ups. Patients may present with an anterior clicking and popping sensation.8
A variety of clinical tests have been designed to evaluate the subscapularis, most commonly the lift-off test, internal rotation lag sign, belly-press test, and the bear hug test.6,18 For the lift-off test the shoulder is placed in internal rotation with the dorsal hand resting on the lower back. The patient is asked to actively raise the hand from back by further internally rotating the shoulder. An inability to do so is a positive test indicating subscapularis weakness.6 The examiner should be able to passively lift the patient’s hand off the back, which excludes adhesive capsulitis as a cause of a false positive test. The lift-off test has been shown to be the most specific clinical test for any subscapularis tear (100%), the most specific for differentiating a full thickness from a partial thickness tear (96.9%), and the most strongly correlated with fatty atrophy of the muscle on MR imaging.18
Imaging Findings
MRI is the imaging test of choice for evaluation of the rotator cuff. Ultrasound and CT arthrography should be considered in patients with a contraindication to MRI or artifact that obscures the rotator cuff tendon insertions. Assessment of the subscapularis can be challenging, especially if imaging is done with insufficient external rotation of the humerus. While Pfirrman reported a sensitivity of 91% and a specificity of 79-86% for 2 readers with arthroscopy as the gold standard,19 subsequent reports from Adams in 2010 and Foad in 2012 reported a sensitivity of 36-37.5% compared to arthroscopy.3,20 A thorough knowledge of the anatomy and common pitfalls together with a systematic approach to analyzing the MR images can improve the pre-operative assessment of subscapularis tears.7,9 A meta-analysis from 2023 revealed a pooled sensitivity of 71% and specificity of 93% for MRI and a sensitivity of 83% and specificity of 86% for MR arthrography in the diagnosis of subscapularis tears.21
Direct imaging findings of a subscapularis tear include discontinuity of the tendon, contrast entering the tendon, circumscribed signal alteration in the tendon, tendon caliber change, and uncovering of the lesser tuberosity with fluid/contrast/or deltoid muscle contacting the lesser tuberosity.10,19 Indirect imaging findings include fatty infiltration of the subscapularis muscle, medial dislocation or subluxation of the long head biceps tendon at the intertubercular groove (Figure 7), cystic change at the lesser tuberosity (Figure 8), and the comma sign.10,19,22,23


Figure 7: 51-year-old woman presents with several month history of lateral shoulder pain. (7A) Axial fat-suppressed proton-density-weighted image shows a tear of the coracohumeral ligament permitting medial dislocation of the long head biceps tendon (arrowhead) superficial to the subscapularis tendon, an empty bicipital groove (asterisk), and an additional interstitial tear at the superior subscapularis insertion (arrow). (7B) Oblique coronal fat-suppressed, proton-density-weighted image demonstrates the medially dislocated long head biceps tendon (arrowheads).

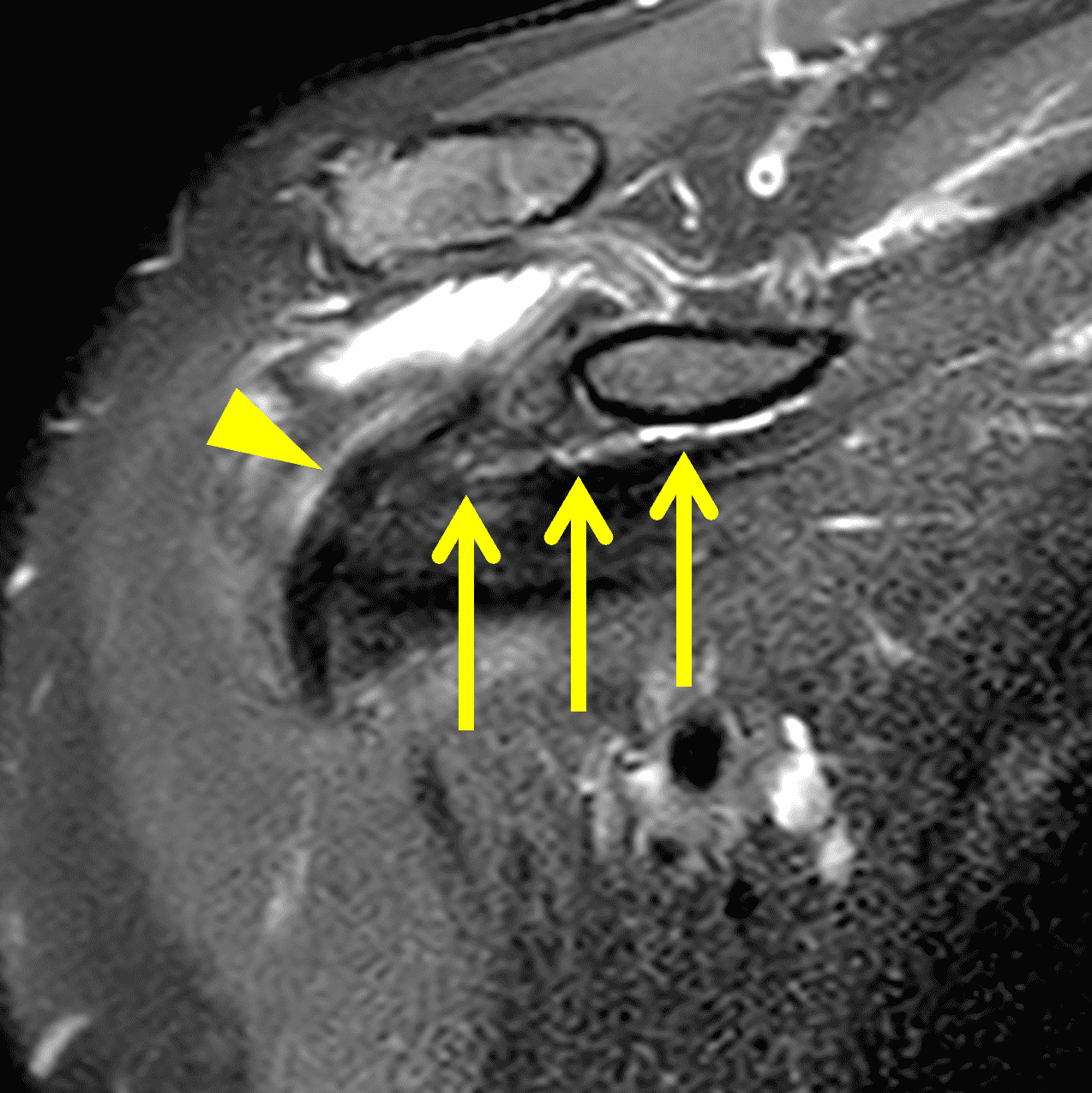

Figure 8: 54-year-old woman with shoulder pain and catching sensation. (8A) Axial fat-suppressed proton-density-weighted image shows a small interstitial tear at the superior subscapularis insertion (arrow) that permits mild medial subluxation of the long head biceps tendon (arrowhead). (8B) Oblique coronal fat-suppressed, T2-weighted image demonstrates medial subluxation of the long head biceps tendon (arrowhead) at the superior biceps groove. Note the position of the biceps tendon relative to the superior margin of the subscapularis tendon (arrows). (8C) On oblique sagittal T2-weighted image, cystic change (arrow) is present deep to the superior margin of the lesser tuberosity and biceps tendon (arrowhead).
Knowledge of the potential pitfalls in the MRI diagnosis of subscapularis tears can improve one’s accuracy. The majority of subscapularis tears begin at the superolateral margin of the tendon insertion on the first facet of the lesser tuberosity.16 Volume averaging with the rotator interval and tendinosis may lead to an irregular appearance at the superior margin and result in overcalling tears, pitfalls that may be mitigated by assessment of the tendon on orthogonal images and confirmation of fluid-signal in the tear (Figure 8).9,16 Scar tissue contiguous with the torn subscapularis tendon and the fascia overlying the long head biceps tendon at the bicipital groove may be mistaken for an intact tendon, a pitfall that may be avoided by evaluating the tendon for focal caliber changes, medial retraction of the myotendinous junction, and fatty atrophy of the muscle (Figure 9).10,19 Finally, the distinction between interstitial tears, which are concealed at arthroscopy, and tears which extend to the articular surface can be challenging, necessitating careful assessment of the tendon margins.9


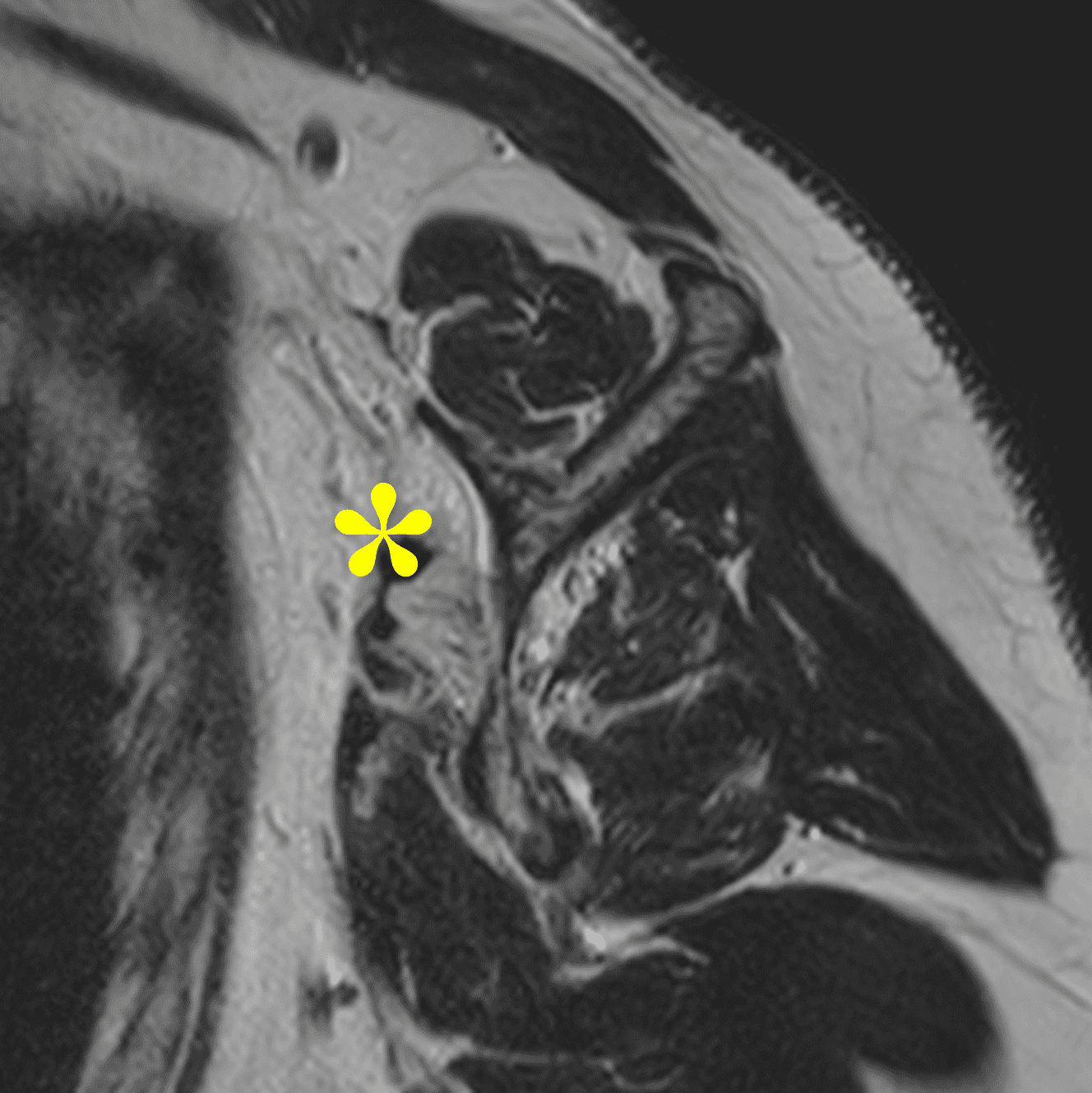
Figure 9: 68-year-old woman with progressive pain with activity, pain with range of motion, and decreased strength. (9A) Axial fat-suppressed, proton-density-weighted image demonstrates focal caliber change in the tendon with medial retraction of the myotendinous junction (arrowhead) and a thin band of fibrotic scar tissue extending to the lesser tuberosity (arrow). (9B and 9C) Oblique sagittal T2-weighted images show the thin band of scar tissue (arrow) superficial to the first and second facets of the lesser tuberosity. Severe fatty atrophy of the superior subscapularis muscle (asterisk) supports the diagnosis of a full-thickness subscapularis tendon tear with scar-in-continuity.
Subscapularis tears can be classified by the location, size, and associated secondary findings. The Pfirrman classification is based on tear size.19 Grade 1 tears involve less than 25% of the craniocaudal dimension of the tendon. Grade 2 tears involve >25% of the tendon without complete detachment. Grade 3 tears are distinguished by complete detachment of the tendon from the lesser tuberosity. The Lafosse classification has the advantage of incorporating partial thickness tears and guiding surgical treatment.6,24 Type 1 tears are partial thickness tears of the superior third of the tendon. Type 2 tears are complete tears limited to the superior third of the tendon. Type 3 tears are complete tears involving up to two thirds of the cranio-caudal dimension. Type 4 tears are complete tendon tears with fatty atrophy of the muscle less than or equal to Goutallier stage 3. Type 5 tears are complete tears with an eccentric position of the humeral head, coracoid impingement, and muscle atrophy greater than or equal to Goutallier stage 3.24 The Yoo and Rhee classification is based on the footprint anatomy.16 Type 1 tears encompass fraying or longitudinal splitting of the leading edge of the tendon. Type 2A tears involve less than 50% detachment at the first facet. Type 2B tears greater than 50% detachment at the first facet. Type 3 tears involve the entire first facet with disruption of the lateral band, full thickness tear of the upper third of the tendon. Type 4 tears extend into the second facet and involve up to two thirds of the entire footprint or the entire tendinous insertion. Type 5 tears involve the entire tendinous insertion and extend into the muscular insertion.
Treatment
Partial tears of the subscapularis are often managed conservatively due to the low risk of progression.8,16 The goals of conservative treatment are to provide symptom relief, promote healing, and restore function through a combination of rest, physical therapy, medication and lifestyle modification.8 The decision to operate is multi-factorial based on patient age, arm dominance arm, activity level, symptoms, tear size, and associated injuries. Chronic subscapularis tears may be surgically repaired after a failure of conservative treatment.6,10 Acute traumatic tears are best treated with early operative intervention.6,10 Preoperative identification of the comma sign may be useful in operative planning – assisting the surgeon in finding and securing the leading edge of the subscapularis.2,15,25
Summary
The subscapularis tendon plays an important role in both active and passive stabilization of the shoulder. Subscapularis tears are challenging to diagnose clinically. MR imaging is the best noninvasive exam to assess subscapularis tendon tears. Tears typically begin at the superolateral insertion and are associated with tears of the supraspinatus, termed the anterosuperior tear. Imaging interpretation is optimized by a thorough understanding of the anatomy, systematic assessment of the MR images in all planes, and knowledge of the potential pitfalls.
References
- Kellam P, Kahn T, Tashjian RZ. Anatomy of the Subscapularis: A Review. J Shoulder Elb Arthroplast. 2019;3. ↩
- Atinga A, Dwyer T, Theodoropoulos JS, Dekirmendjian K, Naraghi AM, White LM. Preoperative Magnetic Resonance Imaging Accurately Detects the Arthroscopic Comma Sign in Subscapularis Tears. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2021;37(10):3062-3069. ↩
- Foad A, Wijdicks CA. The accuracy of magnetic resonance imaging and magnetic resonance arthrogram versus arthroscopy in the diagnosis of subscapularis tendon injury. Arthroscopy. 2012;28(5):636-641. ↩
- McKean D, Teh J. Imaging of the Long Head of Biceps Tendon and Rotator Interval. Semin Musculoskelet Radiol. 2022;26(5):566-576. ↩
- Kang Y, Lee JW, Ahn JM, Lee E, Kang HS. Instability of the long head of the biceps tendon in patients with rotator cuff tear: evaluation on magnetic resonance arthrography of the shoulder with arthroscopic correlation. Skeletal Radiol. 2017;46(10):1335-1342. ↩
- Lee J, Shukla DR, Sánchez-Sotelo J. Subscapularis tears: hidden and forgotten no more. JSES Open Access. 2018;2(1):74-83. ↩
- Adams CR, Brady PC, Koo SS, et al. A systematic approach for diagnosing subscapularis tendon tears with preoperative magnetic resonance imaging scans. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2012;28(11):1592-1600. ↩
- Garg AK, Meena A, Farinelli L, D’Ambrosi R, Tapasvi S, Braun S. Partial subscapularis tear: State-of-the-art. J ISAKOS. 2024;9(6):100290. ↩
- Gyftopoulos S, O’ Donnell J, Shah NP, Goss J, Babb J, Recht MP. Correlation of MRI with arthroscopy for the evaluation of the subscapularis tendon: a musculoskeletal division’s experience. Skeletal Radiol. 2013;42(9):1269-1275. ↩
- Morag Y, Jamadar DA, Miller B, Dong Q, Jacobson JA. The subscapularis: anatomy, injury, and imaging. Skeletal Radiol. 2011;40(3):255-269. ↩
- Giaroli EL, Major NM, Lemley DE, Lee J. Coracohumeral interval imaging in subcoracoid impingement syndrome on MRI. AJR Am J Roentgenol. 2006;186(1):242-246. doi:10.2214/AJR.04.0830 ↩
- Nové-Josserand L, Boulahia A, Levigne C, Noel E, Walch G. Coraco-humeral space and rotator cuff tears. Rev Chir Orthop Reparatrice Appar Mot. 1999;85(7):677-683. ↩
- Yoon SH, Seo JB, Kim MG, Yoo JS. The anterior translation of the humeral head leads to a decrease in the coracohumeral distance in subscapularis tear. J Orthop. 2020;22:535-538. ↩
- Lo IKY, Burkhart SS. The comma sign: An arthroscopic guide to the torn subscapularis tendon. Arthroscopy. 2003;19(3):334-337. ↩
- Zappia M, Ascione F, Romano AM, et al. Comma sign of subscapularis tear: diagnostic performance and magnetic resonance imaging appearance. J Shoulder Elbow Surg. 2021;30(5):1107-1116. ↩
- Yoo JC, Rhee YG, Shin SJ, et al. Subscapularis tendon tear classification based on 3-dimensional anatomic footprint: a cadaveric and prospective clinical observational study. Arthroscopy. 2015;31(1):19-28. ↩
- Ahn TR, Yoon YC, Yoo JC, Kim HS, Lee JH. Diagnostic performance of conventional magnetic resonance imaging for detection and grading of subscapularis tendon tear according to Yoo and Rhee classification system in patients underwent arthroscopic rotator cuff surgery. Skeletal Radiol. 2022;51(3):659-668. ↩
- Yoon JP, Chung SW, Kim SH, Oh JH. Diagnostic value of four clinical tests for the evaluation of subscapularis integrity. J Shoulder Elbow Surg. 2013;22(9):1186-1192. ↩
- Pfirrmann CW, Zanetti M, Weishaupt D, Gerber C, Hodler J. Subscapularis tendon tears: detection and grading at MR arthrography. Radiology. 1999;213(3):709-714. ↩
- Adams CR, Schoolfield JD, Burkhart SS. Accuracy of preoperative magnetic resonance imaging in predicting a subscapularis tendon tear based on arthroscopy. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2010;26(11):1427-1433. ↩
- Saremi H, Seifrabiei M. Subscapularis tendon tear classification and diagnosis: A systemic review and meta-analysis. Front Surg. 2023;10:916694. ↩
- Studler U, Pfirrmann CWA, Jost B, Rousson V, Hodler J, Zanetti M. Abnormalities of the lesser tuberosity on radiography and MRI: association with subscapularis tendon lesions. AJR Am J Roentgenol. 2008;191(1):100-106. ↩
- Wissman RD, Ingalls J, Hendry D, Gorman D, Kenter K. Cysts within and adjacent to the lesser tuberosity: correlation with shoulder arthroscopy. Skeletal Radiol. 2012;41(9):1105-1110. ↩
- Lafosse L, Jost B, Reiland Y, Audebert S, Toussaint B, Gobezie R. Structural integrity and clinical outcomes after arthroscopic repair of isolated subscapularis tears. J Bone Joint Surg Am. 2007;89(6):1184-1193. ↩
- Solomon DJ. Editorial Commentary: Magnetic Resonance Imaging Identifies the Comma Sign Seen During Arthroscopy for Subscapularis Tears. Arthroscopy. 2021;37(10):3070-3071. ↩
