MRI technologists are balancing a lot right now. Packed schedules. Difficult positioning. Anxious patients. Pressure to keep exams moving.
But even in a high-volume environment, the technologist still plays one of the biggest roles in determining whether a study ends up truly diagnostic.
Because image quality is rarely about one big thing. It’s usually a series of small decisions that ...
The AMA’s warning about using AI for diagnosis and treatment decisions gets to the heart of a growing issue in healthcare: access to information is not the same thing as medical expertise.
AI tools can be helpful for simplifying terminology, organizing information, or helping patients prepare questions for their physician. But there is a major difference between gathering information and ...
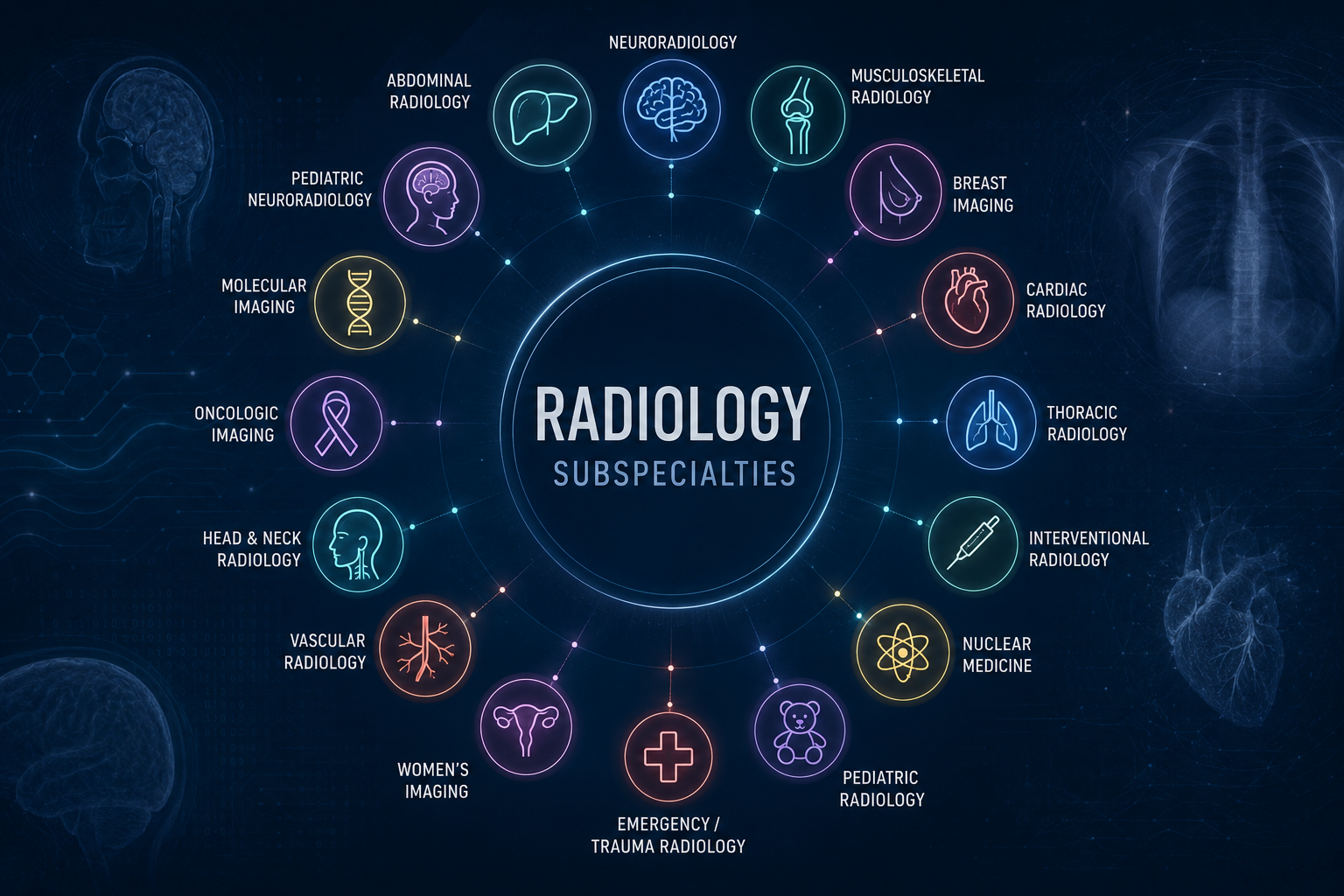
When an orthopedic surgeon orders an MRI, the assumption is that a radiologist will read it. What is rarely asked — and rarely specified in a teleradiology contract — is what kind of radiologist.
That distinction carries real clinical consequences, and the published literature is consistent on the point.
The Subspecialty Difference
Modern radiology encompasses more than a dozen ...
Most imaging centers track study volume. Most track revenue. Almost none track the one metric that most clearly reveals whether their teleradiology partner is actually performing: STAT utilization rate.
It is the percentage of your monthly read volume ordered as STAT rather than routine. And in our experience, most practices either do not track it, or have long since stopped questioning ...
Manual image sharing doesn’t usually show up as a line item on an invoice, but the costs add up all the same.
A technologist uploads a CD. A PACS admin fixes a mismatched study. A radiologist waits for prior imaging to arrive. None of these steps seem significant on their own, but together they create a steady drag on productivity.
The real cost shows up in time and ...