Clinical History
A 19-year-old collegiate baseball player sustained a twisting injury to the knee 3 weeks earlier. Sagittal (1A) proton density-weighted fat-suppressed image through the intercondylar notch, (1B and 1C) proton density-weighted images through the medial compartment, and (1D) fat-suppressed proton density image through the medial compartment are provided. What are the findings? What is your diagnosis?




Findings

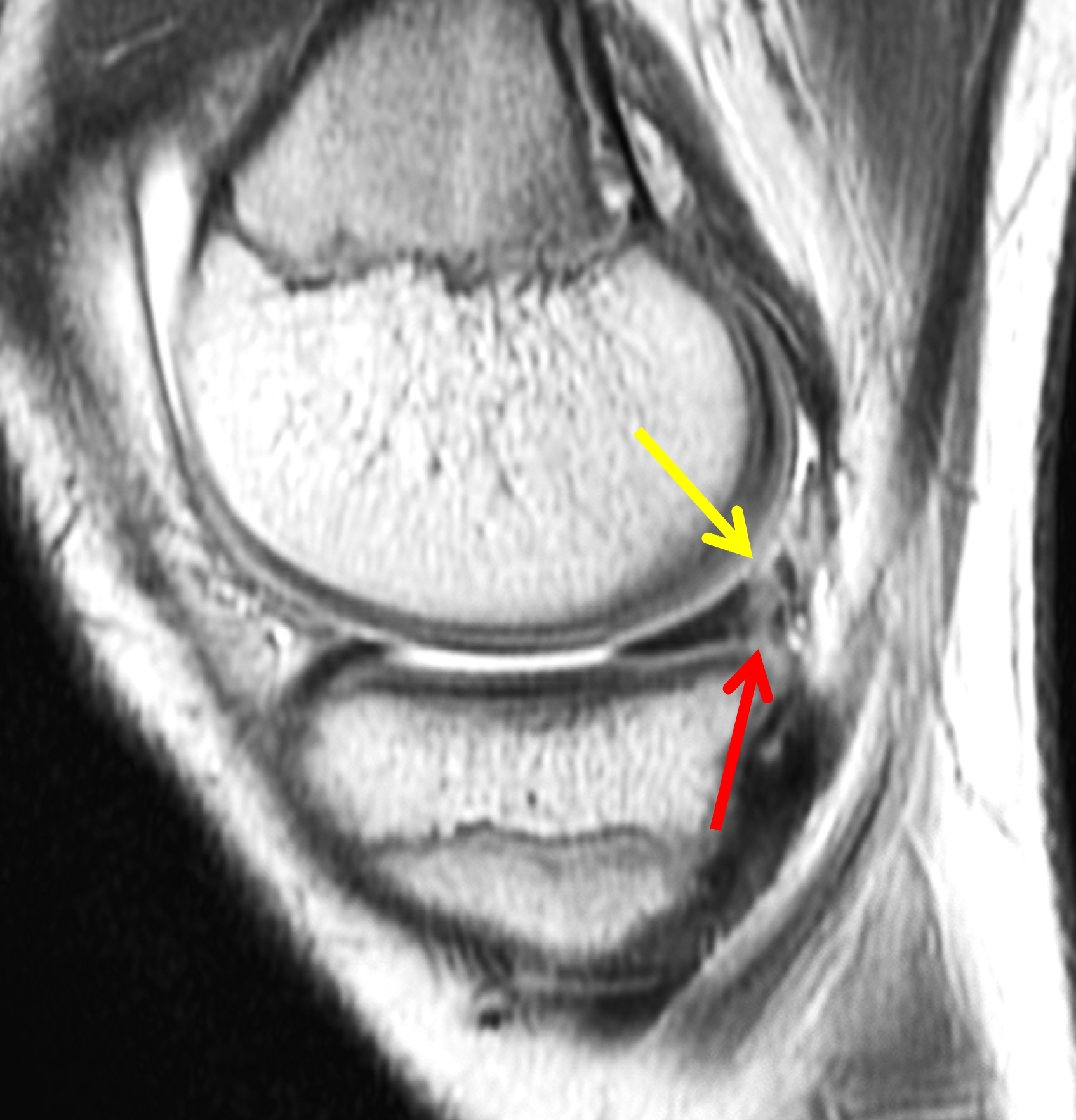
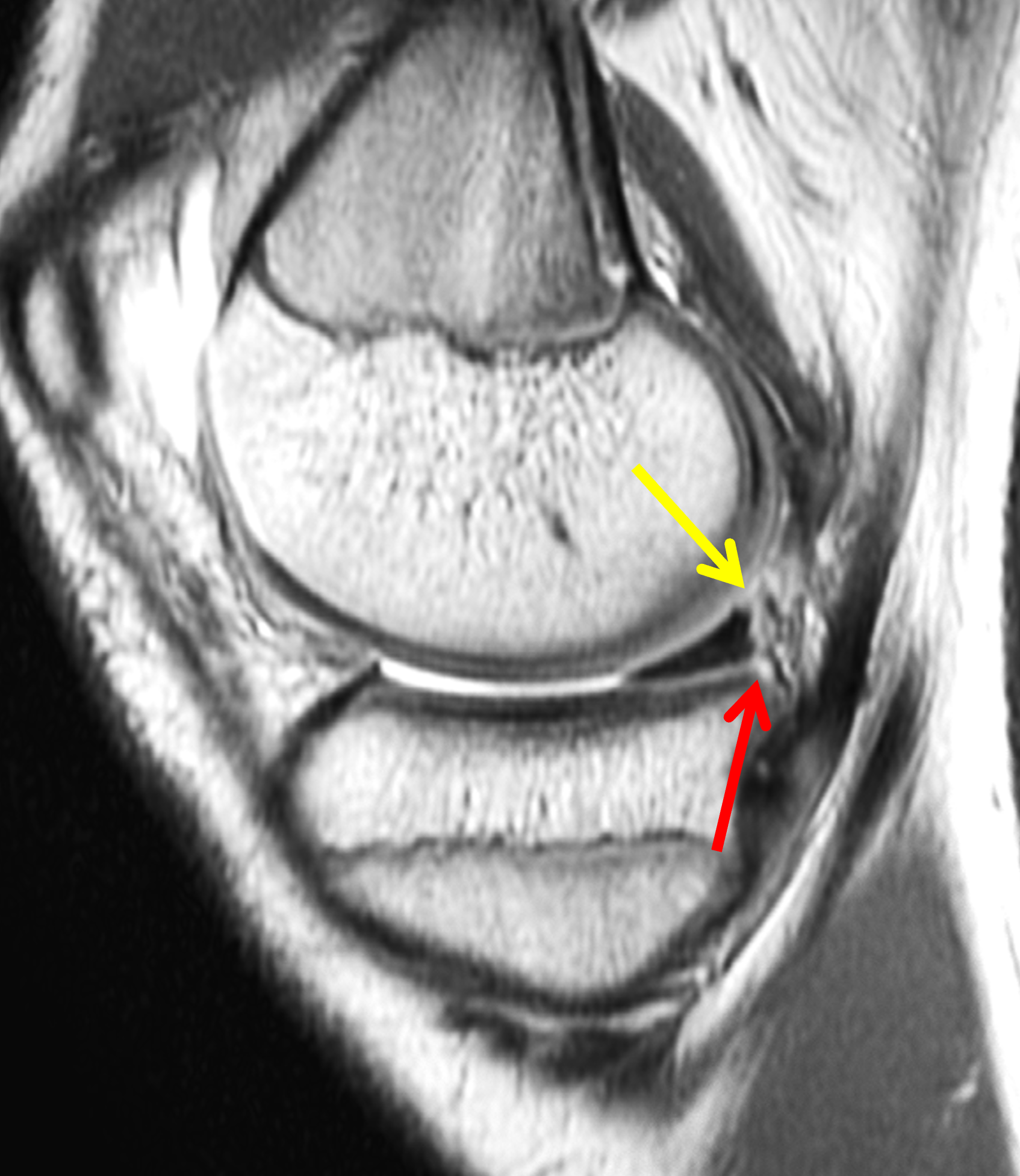

Figure 2: (2A) Sagittal image through the intercondylar notch shows a complete tear of the anterior cruciate ligament (arrowheads). (2B and 2C) Near the posterior meniscocapsular junction of the medial meniscus, there is disruption of the posterior meniscotibial ligament (red arrow) and irregularity of the posterior meniscocapsular ligament (yellow arrow). (2D) On the fluid-sensitive sequence, linear high signal intensity is interposed between the ligaments and the posterior horn of the medial meniscus (arrowheads).
Diagnosis
Anterior cruciate ligament tear with a medial meniscal ramp lesion.
Introduction
In the late 1980s, Strobel’s arthroscopy manual introduced the term “ramp” to describe peripheral tears at the posterior horn medial meniscus (PHMM) meniscocapsular junction in the setting of an anterior cruciate ligament tear.1 This term reflected the ramp-like appearance of the posterior horn when a meniscocapsular tear created a potential space behind its posterior edge. Subsequently, Bollen drew attention to posteromedial meniscocapsular injury as an under-recognized companion lesion in anterior cruciate ligament (ACL) tears.2 Since that time, several large arthroscopic series have reported between 9% and 42% of ACL injuries also have a ramp lesion, depending somewhat on patient demographics, age of injury, and the scrutiny of arthroscopic inspection.3,4,5,6,7
The growing body of evidence shows that ramp lesions increase anterior tibial translation and rotational instability in both ACL-deficient and ACL-reconstructed knees, and that meniscal repair can restore stability to near normal levels.8,9,10,11,12,13,14 At the same time, meta-analyses of several MRI studies show that routine imaging has only modest sensitivity in detecting ramp lesions.15,16,17,18 For radiologists, understanding the posteromedial meniscocapsular anatomy, the tear patterns that comprise ramp lesions, and the associated imaging findings and pitfalls will help guide diagnosis and appropriately alert our orthopedic colleagues to these potentially “hidden lesions.”
Anatomy of the Posteromedial Meniscocapsular Unit
The PHMM is a broad, wedge-shaped fibrocartilaginous structure comprised of type I collagen, glycosaminoglycans, and water. Collagen bundles in the peripheral portion of the PHMM are arranged in circumferential bundles that are enveloped by radially-oriented “tie fibers.”19 This circumferential fiber orientation accounts for the longitudinal tears frequently seen in the peripheral meniscus. The PHMM is anchored by the posterior root ligament at the tibial plateau, peripherally stabilized by the posterior meniscocapsular and meniscotibial ligaments, and indirectly stabilized by the capsular branch of semimembranosus tendon, which inserts on the posteromedial capsule.20 The peripheral PHMM and adjacent meniscocapsular tissue are well vascularized, and thus afford a high healing potential when injured.
The meniscocapsular and meniscotibial ligaments both arise from the posterior margin of the PHMM (Figures 3 and 4). The meniscocapsular ligament courses posterosuperiorly and blends into the capsule with a variable amount of meniscosynovial tissue covering its superior articular surface. The meniscotibial ligament travels posteroinferiorly and anchors to the posterior tibia several millimeters below the articular surface. The ligaments are comprised of type 1 collagen but are less compacted than typical ligamentous structures, with loose adipose and vascular tissue interposed between the two ligaments.8,21
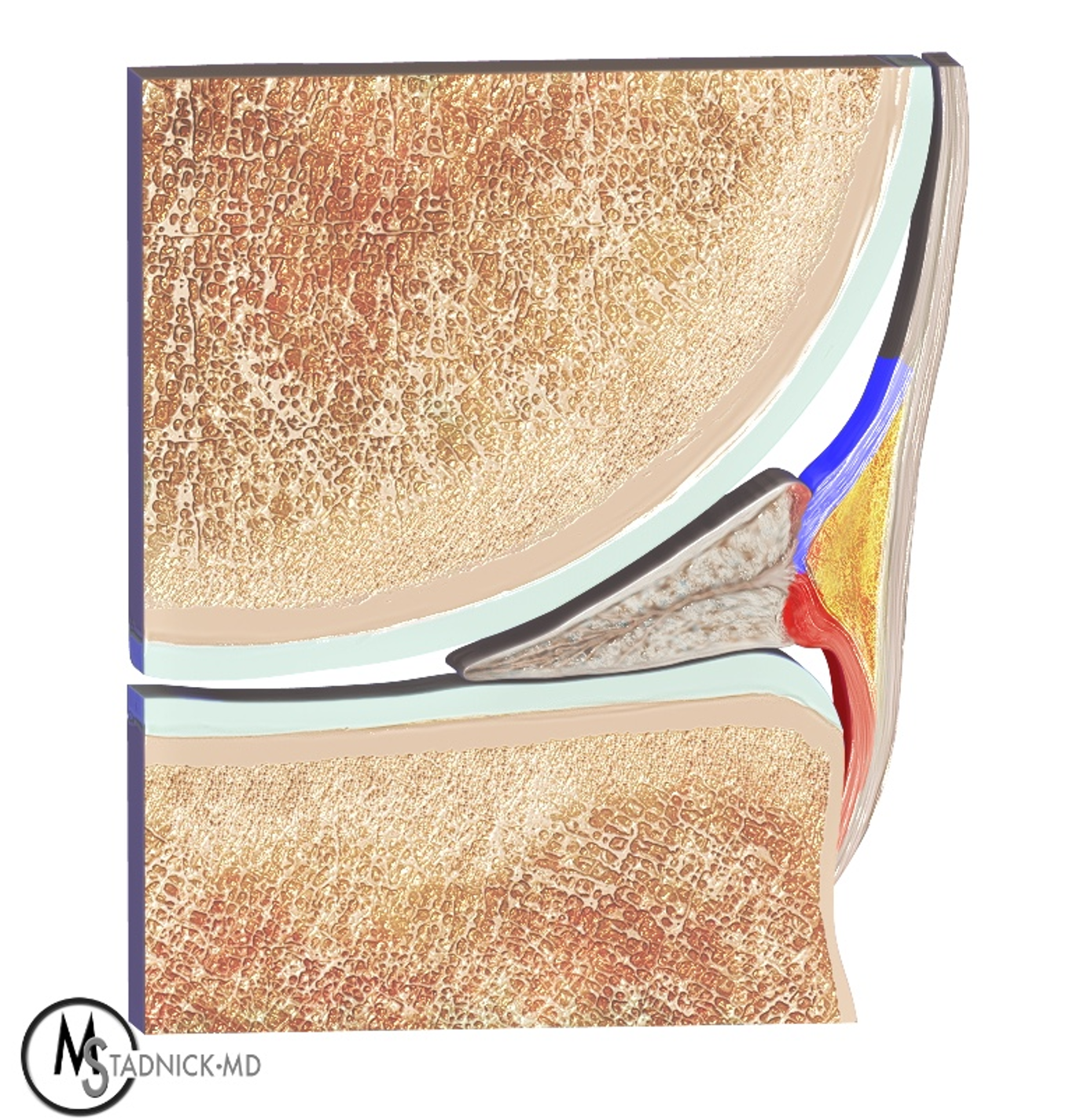
Figure 3: Anatomic drawing of the normal posterior medial meniscus attachments. The meniscocapsular (blue) and meniscotibial (red) ligaments share a common attachment point along the posterior margin of the PHMM. The meniscocapsular ligament blends with the posterior joint capsule and inserts on the femur. The meniscotibial ligament inserts on the posterior cortex of the tibia several millimeters caudal to the joint line. Vascularized adipose tissue (yellow) resides between the two ligaments.


Figure 4: Normal MRI anatomy of the posteromedial knee. (4A) Sagittal proton density-weighted image shows the meniscocapsular ligament (yellow arrow) and the meniscotibial ligament (red arrow) attached to the posterior horn of the medial meniscus. (4B) Fat-suppressed fluid-sensitive image demonstrates loose connective and adipose tissue (asterisk), which is hyperintense due to its inherent vascularity, between the posterior ligaments. Note the meniscotibial ligament insertion on the tibia several millimeters below the articular cartilage (arrowhead).
Anatomic descriptions of the relationship between the meniscocapsular and meniscotibial ligaments at their PHMM attachment sites are inconsistent. In a small cadaveric series, DePhillipo et al. described a common shared attachment site of both the meniscocapsular and meniscotibial ligaments located at approximately one third of the PHMM height,8 whereas a subsequent small series discovered that the meniscocapsular and meniscotibial ligaments attach to the respective superior and inferior borders of the PHMM.21 These variations in the literature contribute to challenges imaging and treating these lesions, especially with respect to surgical repair techniques that target an arthroscopically-hidden inferior meniscotibial ligament lesion.
Biomechanics and Pathophysiology of Ramp Lesions
The medial meniscus is a key secondary stabilizer of the ACL-deficient knee. When the ACL is torn, the intact PHMM offers additional resistance to anterior tibial translation and internal rotation. Following ACL reconstruction, Papageorgiou et al. showed a strong interdependence between the ACL graft and the medial meniscus, underscoring the stabilizing role of the medial meniscal complex, particularly in resisting anterior tibial translation post-operatively. Indeed, resection or compromise of the medial meniscus increased forces on the ACL graft by 33-50%, illustrating how the intact meniscus normally protects the ligament from excessive load.10
Furthermore, studies specifically targeting the ramp region demonstrate similar results. Selective sectioning of the meniscocapsular and meniscotibial ligaments in cadaveric specimens increases anterior translation and rotational instability in both ACL-deficient and ACL-reconstructed knees. In these studies, rotational instability was not restored with isolated ACL reconstruction, but only returned to normal with ramp lesion repair.9,12 However, a few human cadaveric and porcine models have failed to demonstrate a direct protective effect of ramp lesion repair on ACL reconstruction grafts.22,23 Although the evidence is evolving, these studies suggest that treating ramp lesions may be important in restoring normal knee kinematics and mitigating ACL graft overload.
Ramp lesions occur either during an acute ACL injury or from repetitive translational trauma in a chronic ACL-deficient knee. Several mechanisms have been proposed, but the most common suggests that the PHMM becomes entrapped between the femur and tibia during anterior tibial translation. In addition, reflexive contraction of the semimembranosus during translational injury may distract the capsule due to the semimembranosus tendon slip attaching to the posterior capsule (Figure 5).24

Figure 5: Anatomic drawing illustrating the dynamic forces hypothesized to create ramp lesions. Anterior subluxation of the tibia due to a torn ACL results in relative posterior translation of the medial femoral condyle (MFC), which compresses and anchors the bulk of the PMHH in place (arrow) while also pushing the periphery of the meniscus posteriorly. At the same time, contraction of the semimembranosus acts on its capsular tendon branch (SM), which pulls the meniscal periphery posteriorly. The result is tearing of the posterior margin of the meniscus and/or the attached ligaments (arrowhead).
Epidemiology and Risk Factors
Several large arthroscopic series have characterized the prevalence and risk factors for ramp lesions in ACL-injured knees. Reported prevalence varies widely in the literature, likely reflecting challenges in diagnosing ramp lesions arthroscopically. However, a few studies with larger sample sizes are noteworthy. Liu et al. looked at a cohort of 868 patients with ACL tears and reported that an arthroscopic ramp lesion was present in nearly 17% of patients.3 Thaunat et al. analyzed 2,156 ACL reconstructions and classified ramp subtypes, again demonstrating an overall prevalence around 16% but also showing that certain subtypes are more often associated with chronic injuries and high-grade instability.5 An additional study of 3,214 ACL reconstructions found a similar prevalence of around 24%.4
Various risk factors have been reported, and a 2021 meta-analysis by Kunze et al. confirmed strong associations with complete ACL tears, male sex, younger age, posteromedial tibial edema, and concomitant lateral meniscal tears.25 Other researchers have identified that ramp lesions are more likely to occur in contact injuries, emphasizing the role of high-energy trauma, which may also account for the association of concomitant lateral meniscal tears.6,7 Interestingly, several anatomic features may also predispose patients to ramp injuries, including an increased lateral femoral condyle ratio, steeper medial tibial slope, and steeper medial meniscal slope.26,27
On MRI, the presence of any of these risk factors in a knee with a torn ACL should direct attention to the periphery of the PHMM. In particular, bone contusions in the posterior medial tibia are highly associated with injuries to the PMHH, both peripheral longitudinal tears and ramp lesions (Figure 6).28,29,30
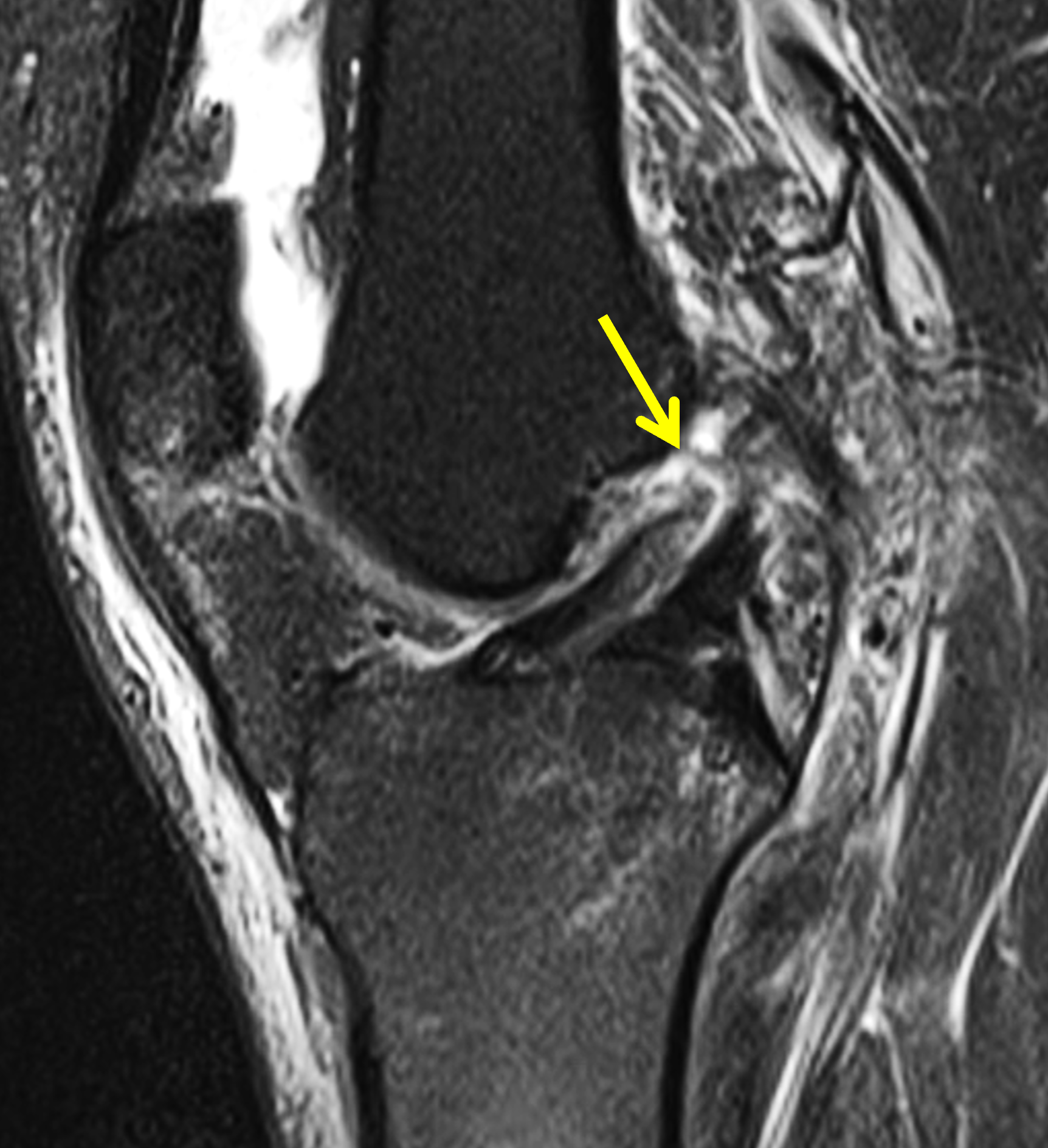
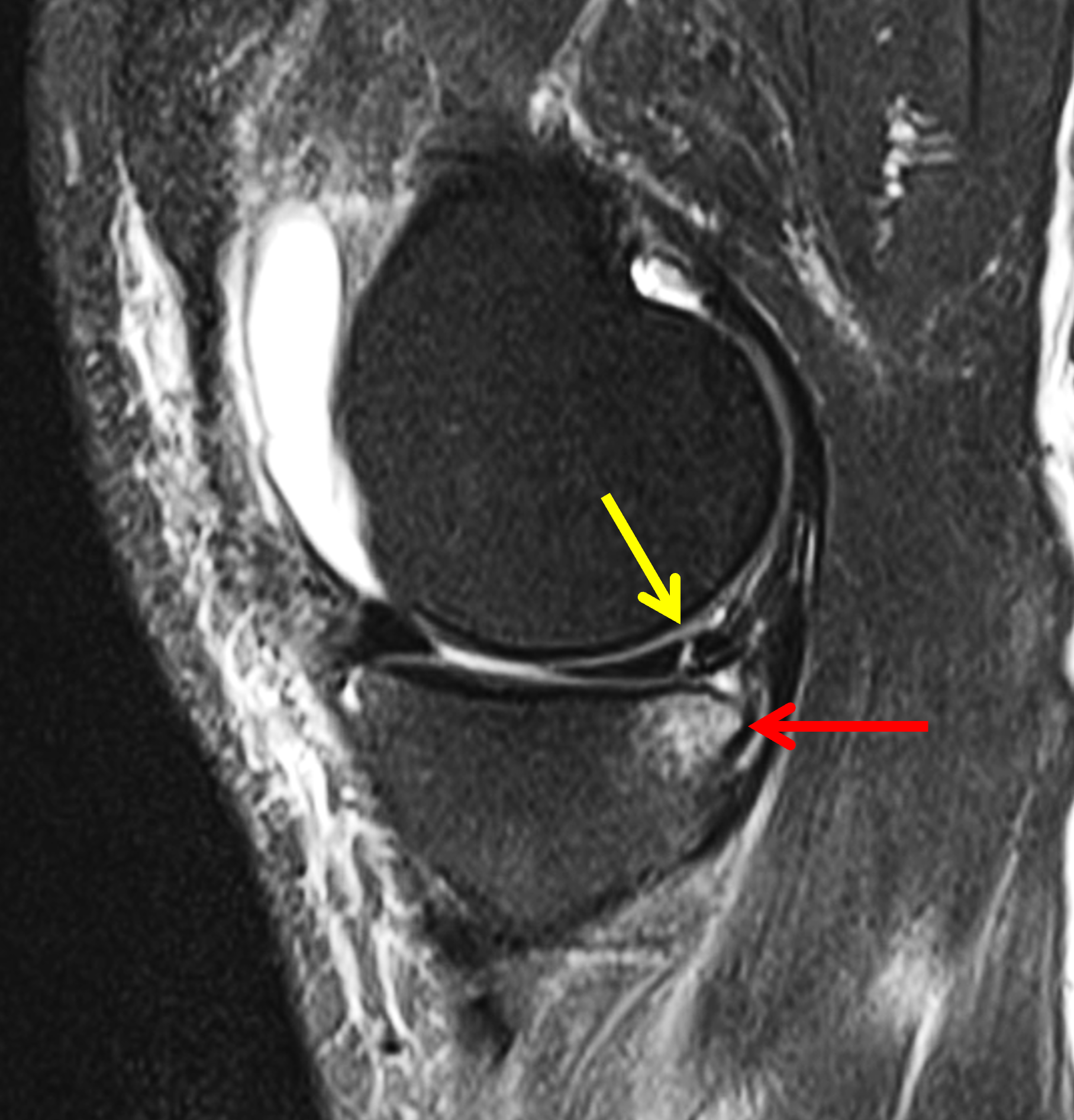
Figure 6: ACL tear associated with peripheral PHMM injury. (6A) Sagittal fat-suppressed fluid-sensitive image through the intercondylar notch shows a complete, acute proximal ACL tear (arrow). (6B) Sagittal fat-suppressed fluid-sensitive image through the medial compartment shows a peripheral longitudinal tear PHMM tear (yellow arrow). Note the subjacent posterior medial tibial bone contusion (red arrow), which should alert the radiologist to a likely injury to the meniscus or meniscocapsular junction.
Definitions, Concepts, and Classification
Originally, a ramp lesion was described as a tear of the peripheral meniscocapsular attachment of the PHMM in the setting of an ACL tear. Over time, this definition has expanded to include lesions involving the meniscotibial surface as well as peripheral longitudinal tears in the red–red zone of the PHMM that are within 3 mm of the capsule. Many investigators feel that these peripheral PHMM tears have similar biomechanical consequences as purely posterior ligamentous lesions and share similar healing potential. Debate on the definition of a ramp lesion persists, however, with the European Society for Sport Traumatology, Knee Surgery, and Arthroscopy issuing a consensus statement in 2019 that ramp lesions should remain distinct from meniscal tears.31
Several classification systems have been created to facilitate communication and provide a framework for developing treatment algorithms. Thaunat et al. initially proposed an arthroscopic classification that subdivided ramp lesions into multiple types based on location, tear thickness, and the presence of double longitudinal tears.5 This classification assumes that the meniscocapsular and meniscotibial ligaments attach to the peripheral margins of the PHMM.
Using MRI findings, Greif et al. expanded Thaunat’s original classification to include additional subtypes differentiating between peripheral PHMM tears and lesions involving the ligaments together with their meniscal attachments.32 Additionally, Greif’s descriptions reference a common attachment of the meniscocapsular and meniscotibial ligaments to the meniscus (Figure 7). This classification system remains the only imaging-based classification to date (Table).
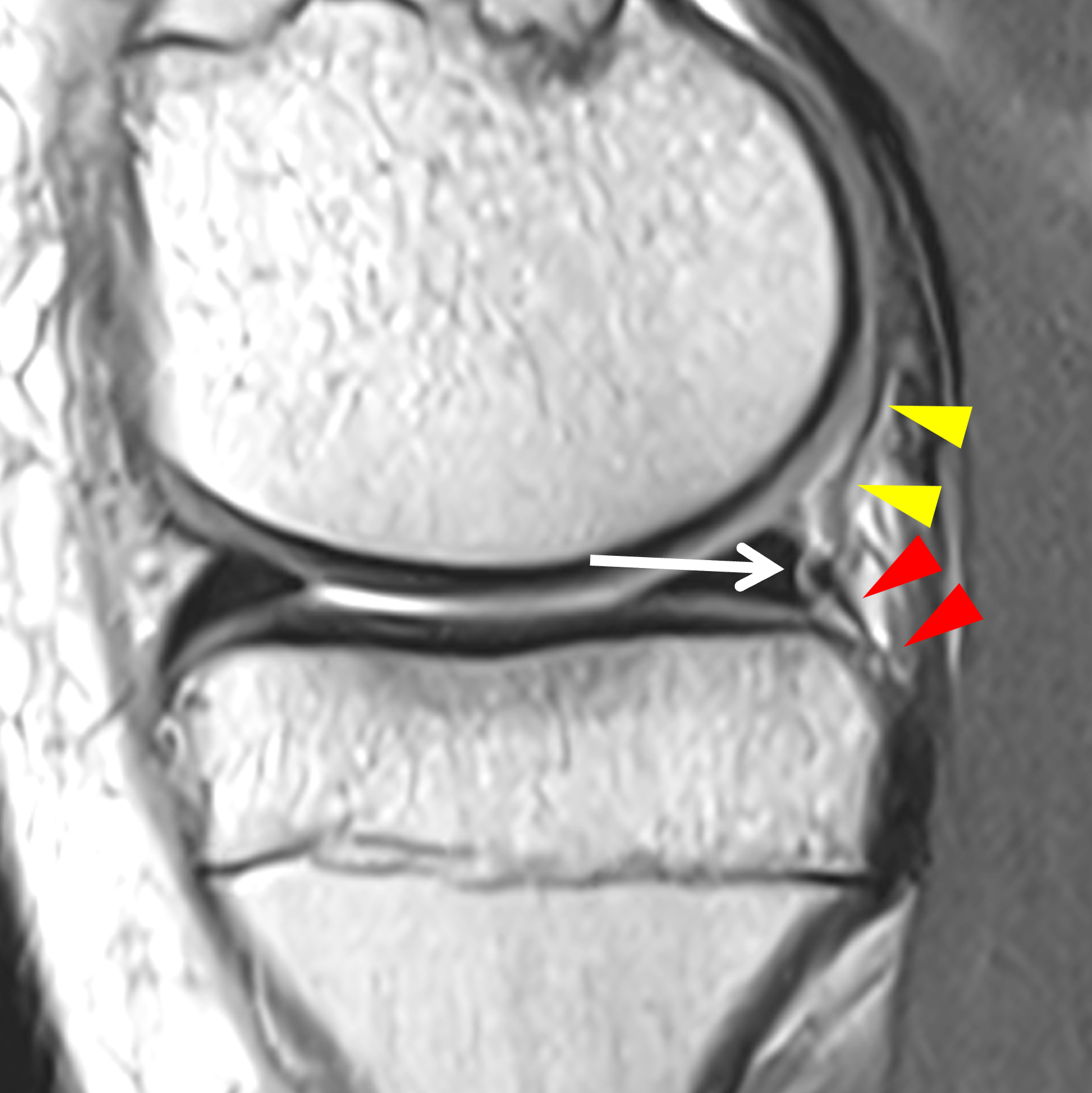

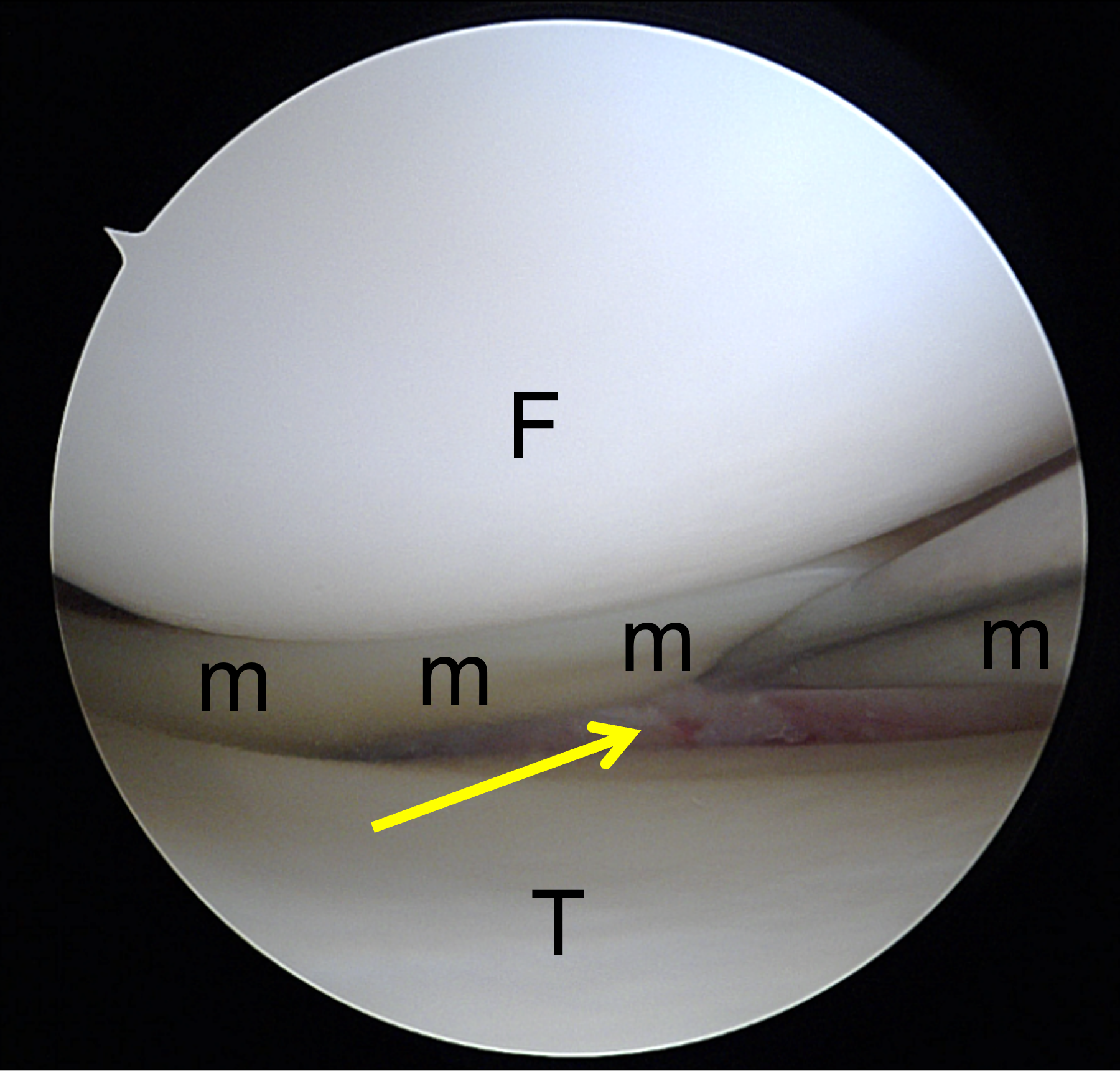
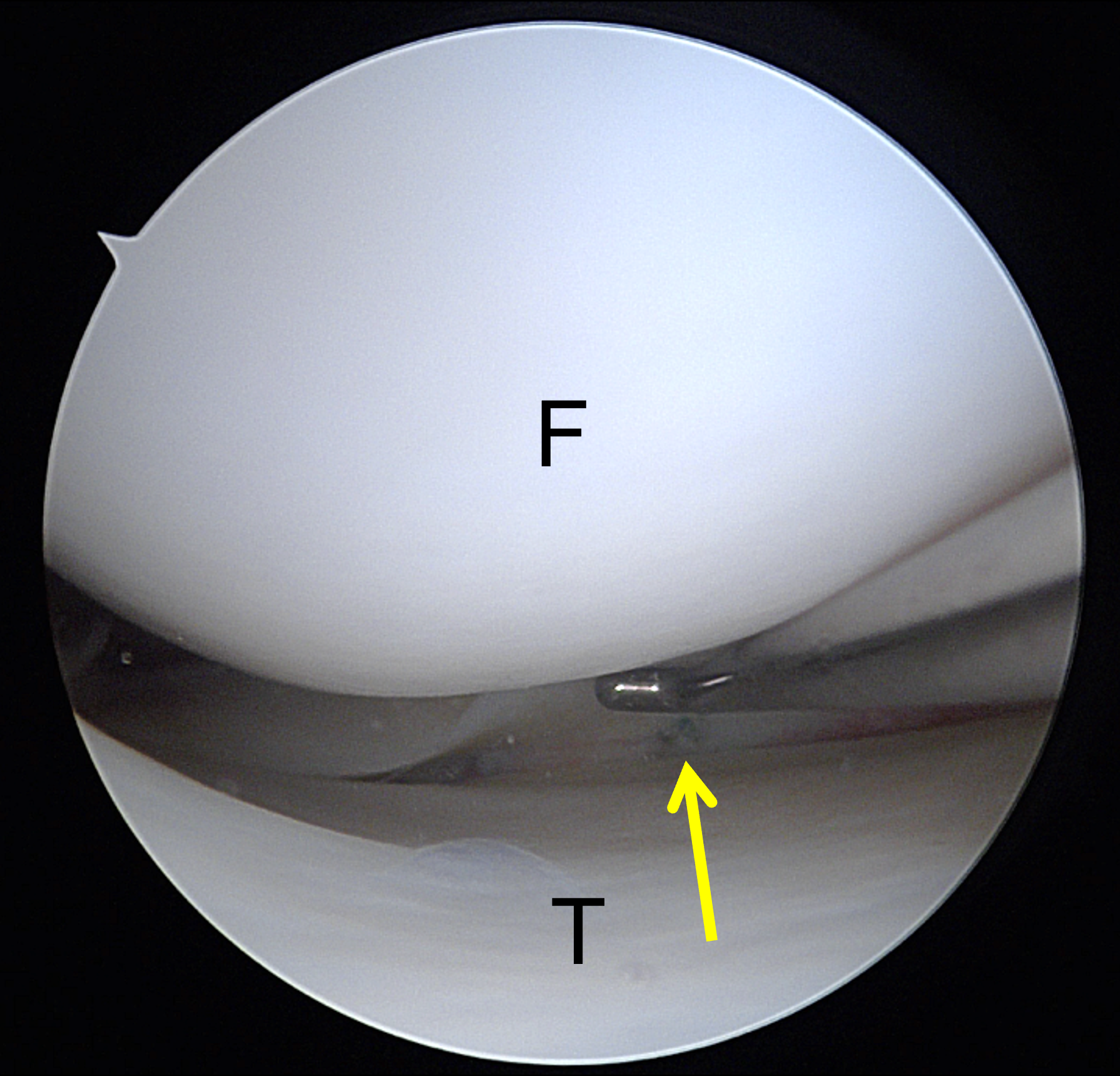
Figure 7: Greif Type 4B ramp lesion in a 15-year-old boy injured playing football. The ACL was torn (not shown). (7A) Sagittal proton-density weighted image shows the meniscocapsular (yellow arrowheads) and meniscotibial (red arrowheads) ligaments converging to a single common structure (arrow) that has torn from the PHMM. (7B) Sagittal fat-suppressed fluid-sensitive image demonstrates a linear fluid collection (arrow) between the avulsed common ligament attachment and the PHMM. (7C) Arthroscopic photograph showing a probe elevating the meniscus (m) away from the tibia, reflecting injury to the meniscotibial ligament (arrow). (7D) Arthroscopic photograph following repair using a FAST-FIX device shows a vertical mattress suture (arrow) securing the torn structures. F = femur, T = tibia.

Additional surgical classification systems have been proposed that factor the length of the lesion, expand subtypes of tear patterns, and/or reflect surgical stability with anatomical consideration.33,34,35 Arthroscopic classifications typically include lesion stability because it impacts surgical management of ramp lesions, whereas stability is more difficult to ascertain with MRI. Thus, there may not be a direct correlation between arthroscopic and imaging classification systems. Nevertheless, it is important to recognize which specific anatomic structures may be involved in a ramp lesion to best communicate these findings to the orthopedic surgeon.
MRI Evaluation
MRI is the primary imaging modality for detecting ramp lesions, yet it remains imperfect. Many arthroscopic case series have reported only modest MRI sensitivity on preoperative imaging. A meta-analysis of MRI performance by Koo et al., revealed a pooled sensitivity of 71% and specificity of 94% in the diagnostic ability to detect arthroscopic-proven ramp lesions in knees with ACL injuries.17 Moreira et al., in another systematic review, showed similar findings but emphasized the heterogeneity in MRI protocols, magnet strengths, and diagnostic criteria across the analyzed studies.18
The most sensitive direct signs of a ramp lesion include a fluid-signal cleft between the PHMM and the meniscocapsular unit, a step-off or contour irregularity of the peripheral PHMM, and focal discontinuity of the peripheral fibers (Figure 8).16,36,37 Posteromedial tibial plateau bone marrow edema, anterior displacement of the PHMM, and focal capsular edema serve as important indirect clues.14,25

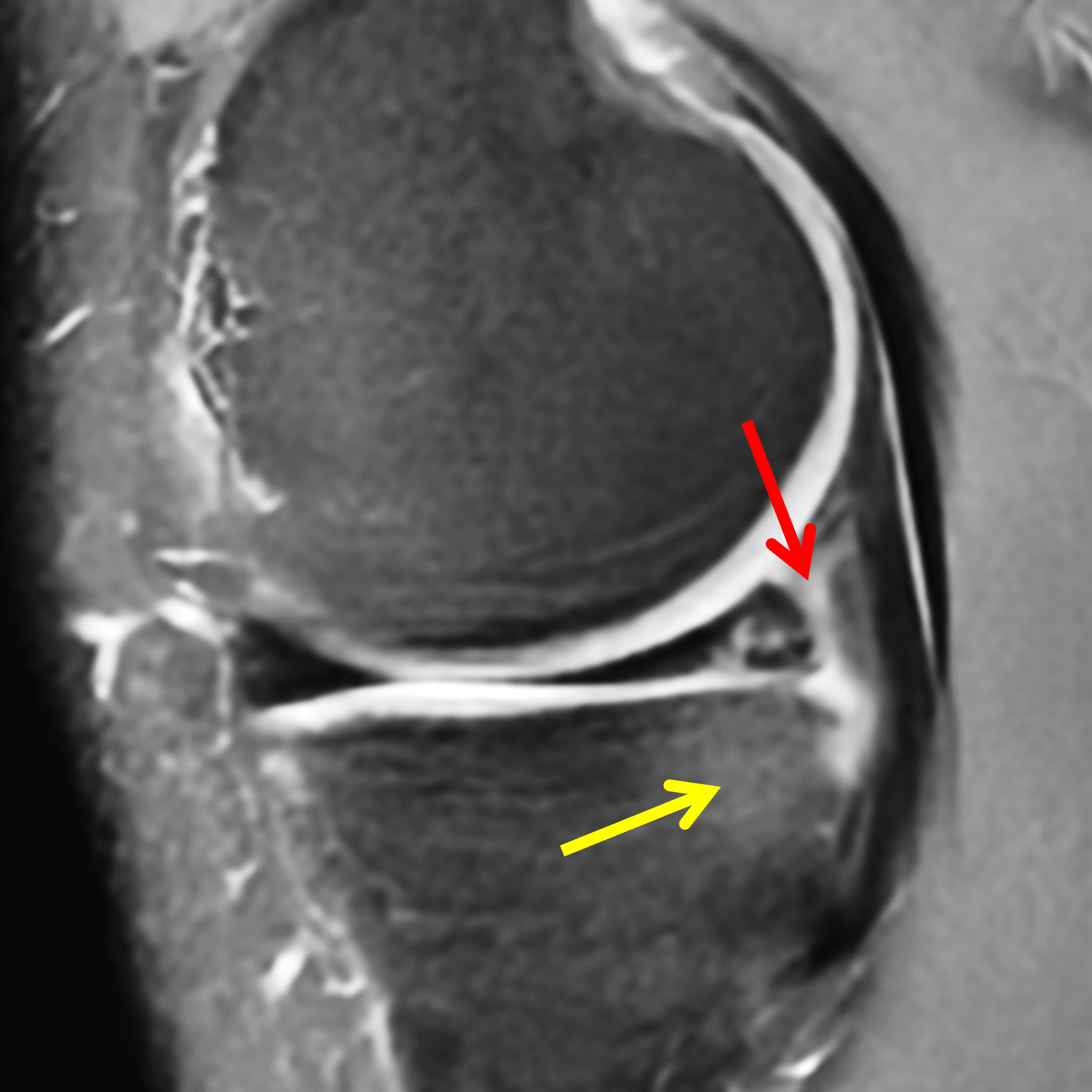
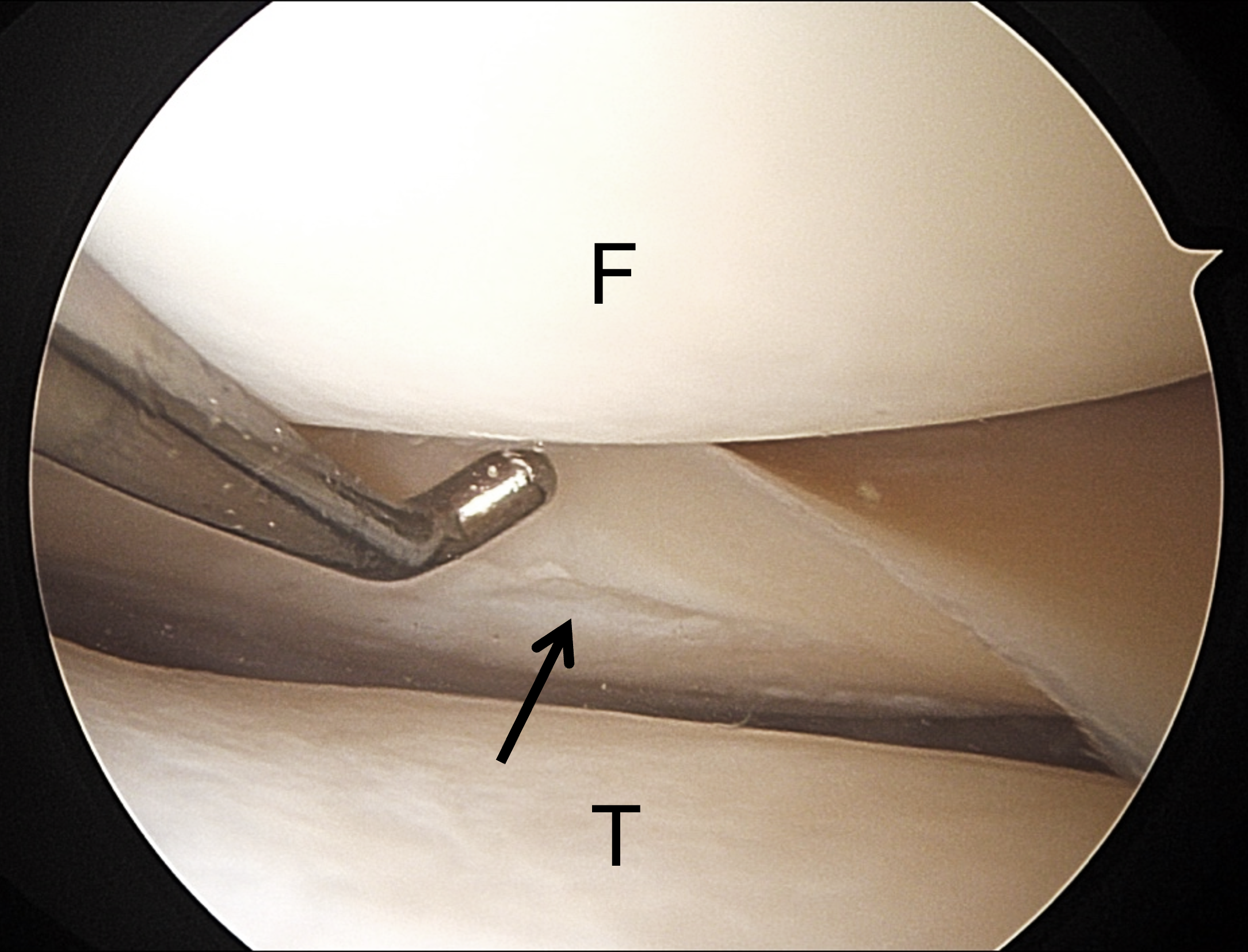
Figure 8: Grief Type 3A ramp lesion in a 22 year-old man who sustained a twisting injury to the knee playing soccer. The ACL and lateral meniscus were also torn (not shown). (8A) Sagittal proton density-weighted image shows an incomplete peripheral tear of the PHMM extending to the tibial surface (arrow). A well-defined meniscotibial ligament is not visible (arrowhead). Compare to Figure 7A. (8B) Sagittal fat-suppressed, fluid-sensitive image shows high signal edema along the posterior margin of the meniscus (red arrow) and a small bone contusion in the posteromedial proximal tibia (yellow arrow), findings often associated with a ramp lesion. (8C) Arthroscopic photograph confirming the peripheral inferior surface PHMM longitudinal tear (arrow). These injuries are sometimes referred to as “hidden lesions” because they may not be visible with standard arthroscopic portals. F = femur, T = tibia.
Intuitively, higher field strength MR imaging should provide better anatomic resolution and improve detection of ramp lesions. One study found sensitivity for ramp lesions of 83% with a 3-T MRI scanner compared to 68% for a 1.5-T scanner.38 Positional changes may also improve sensitivity, although this is of limited availability in routine outpatient imaging. Okazaki et al. showed that open MRI performed with the knee flexed improved visualization of meniscocapsular separation and increased diagnostic performance, likely because flexion accentuates gapping at the tear site.15
Diagnostic mimics of ramp lesions include a normal PHMM superior meniscocapsular recess, non-linear meniscocapsular fluid, posterior root tears, meniscal contusions, and longitudinal tears greater than 3 mm from the meniscocapsular junction (Figure 9). Additionally, acute stable ramp lesions may undergo healing in the interval between imaging and surgical exploration, given the robust vascularity and healing potential of the region (Figure 10).
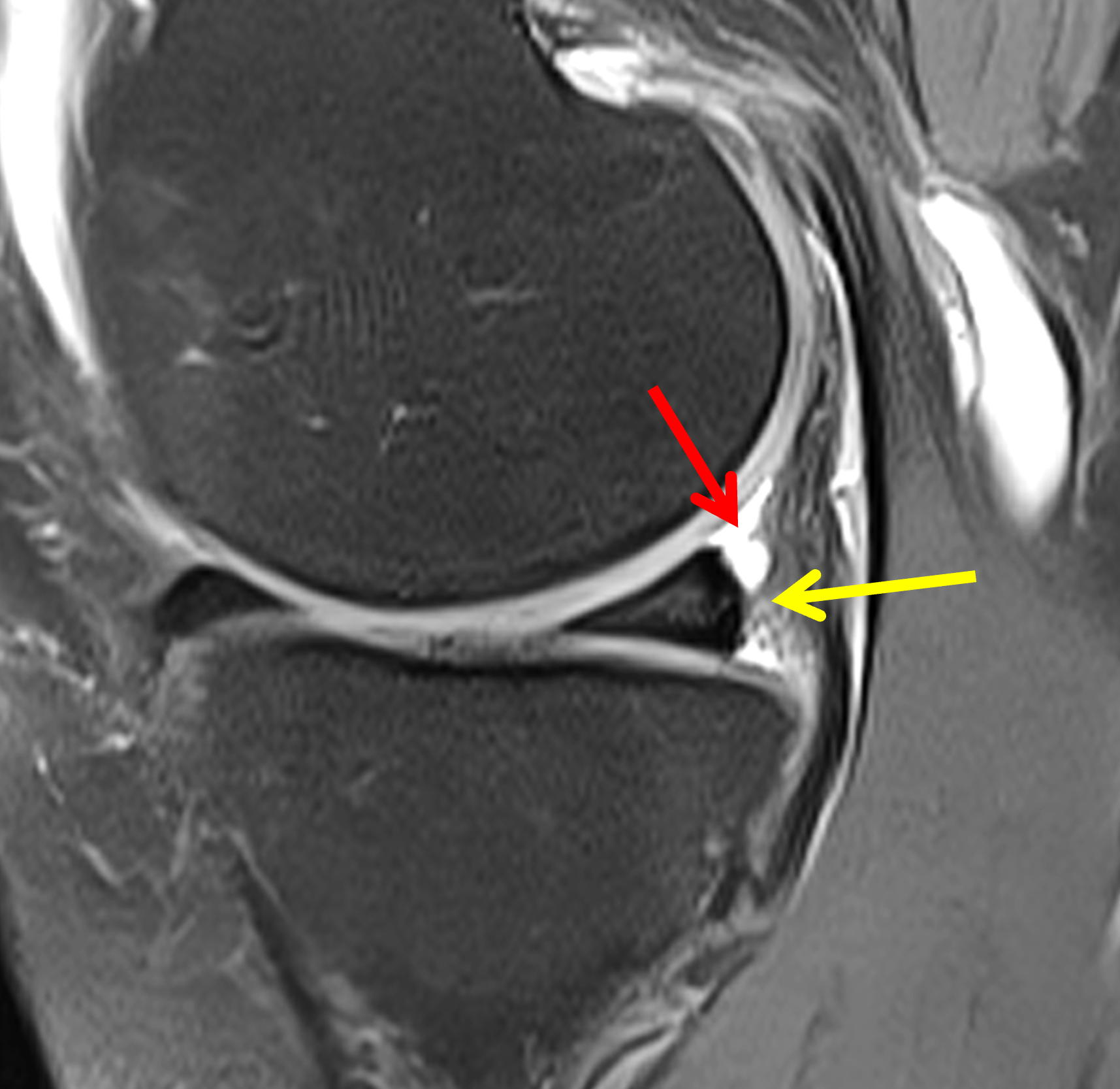

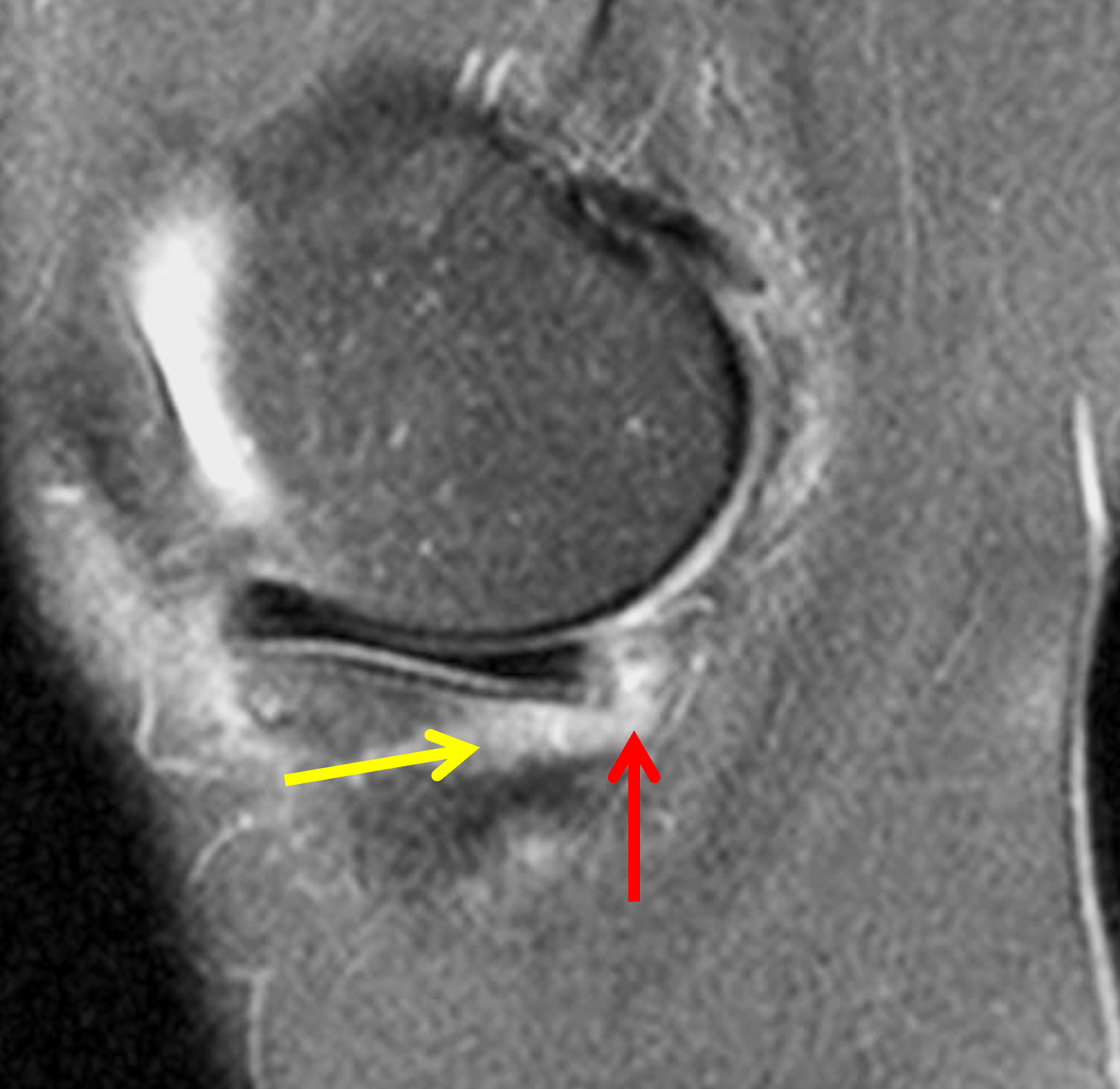
Figure 9: Pitfalls in the diagnosis of ramp lesions. (9A) Superior meniscocapsular recess. Sagittal fat-suppressed, fluid-sensitive image shows fluid in the recess (red arrow), which is round rather than linear in shape. Note the intact common insertion of the meniscocapsular and meniscotibial ligaments (yellow arrow). (9B) Non red-zone longitudinal PHMM tear. Sagittal proton density-weighted image shows a longitudinal meniscal tear (arrow) located more than 3 mm from the posterior meniscal margin. (9C) Medial meniscal contusion. Fat-suppressed fluid-sensitive image shows ill-defined high signal in the vascularized meniscal periphery (red arrow) overlying a bone contusion (yellow arrow) in a knee with an acute ACL tear. At subsequent arthroscopy, resolving hyperemia was present in the meniscal periphery but no tear or ramp lesion.

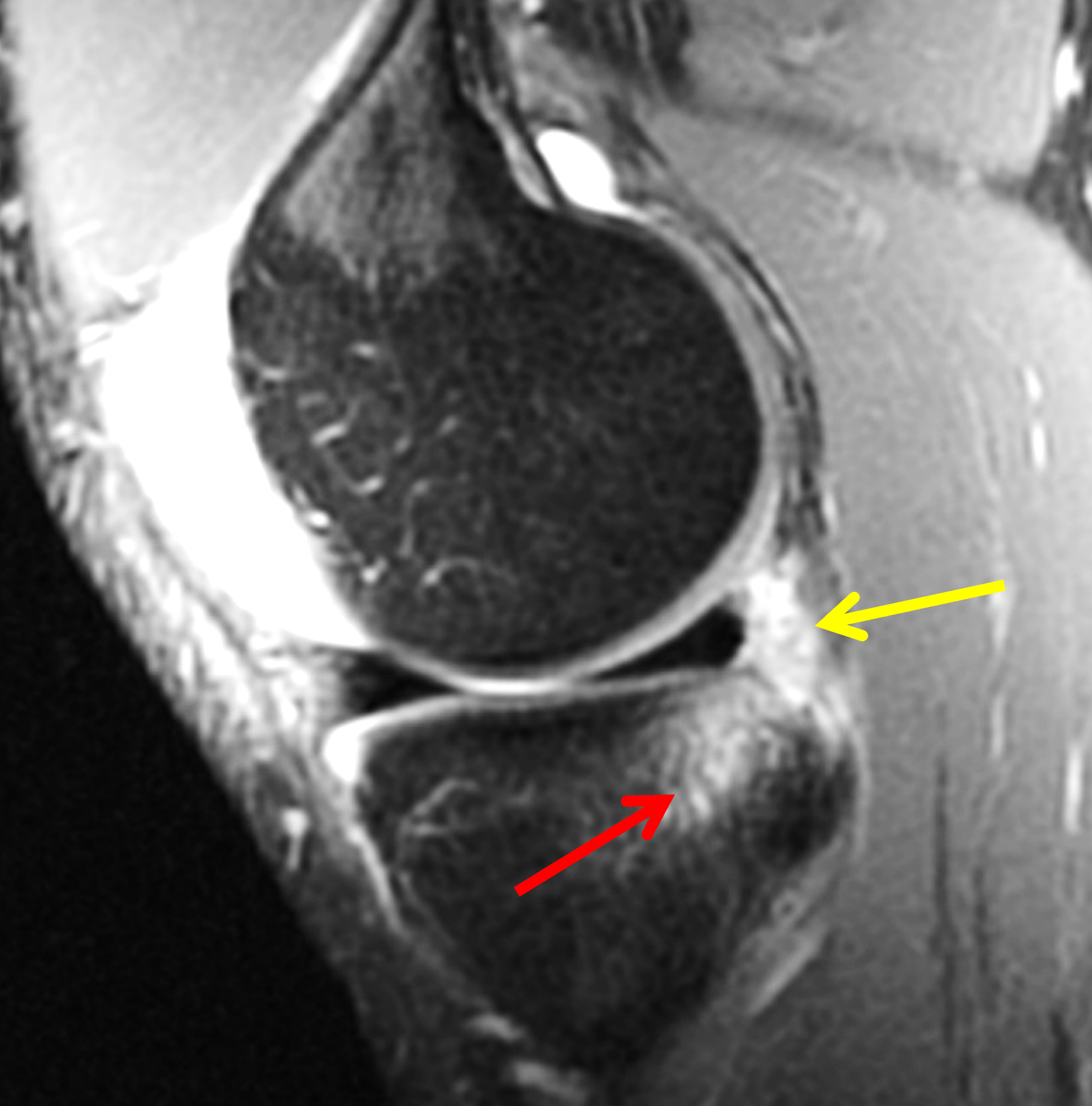
Figure 10. Potential spontaneous healing of a ramp lesion in a 17-year-old boy following a basketball injury. (10A) Sagittal fat-suppressed, fluid-sensitive image through the intercondylar notch shows an acute, complete ACL tear (arrow). (10B) Sagittal fat-suppressed, fluid-sensitive image through the medial compartment shows edema along the posterior meniscal margin (yellow arrow) suggesting a ramp lesion, and a posterior medial tibial bone contusion (red arrow). At arthroscopy 4 weeks later, the posterior meniscocapsular junction was stable to probing and normal in appearance. The MRI appearance may represent a meniscal contusion or a stable ramp lesion that healed.
Arthroscopic Correlation
Standard anterior viewing portals are often insufficient to identify ramp lesions due to limited visualization of the peripheral PHMM, especially along its tibial surface. Sonnery-Cottet et al. highlighted the concept of these “hidden lesions,” and showed that a systematic arthroscopic exploration of the concealed portion of the posterior horn via trans-notch or posteromedial portals dramatically increased detection of ramp lesions compared with standard anterior portals.39 Kim et al. also demonstrated that a sequential arthroscopic approach that included posteromedial evaluation improved diagnostic accuracy for ramp lesions.40
Because trans-notch and/or posteromedial portals may not be routinely employed by all surgeons, MRI may meaningfully influence whether the posterior meniscocapsular unit is explored in detail. Even a cautiously worded suggestion of a possible ramp lesion (particularly in high-risk patients) can prompt surgeons to inspect this region more thoroughly.
Treatment and Outcomes
Stable ramp lesions, particularly short peripheral tears, appear to have substantial healing potential in acute injuries with subsequent ACL reconstruction. Historical work by Yagishita and colleagues showed that some meniscal tears could heal without direct repair, particularly in the vascularized red zone.41 More recent studies have specifically focused on ramp lesions. Arthroscopic “refreshing” procedures with abrasion and trephination for smaller, stable ramp injuries combined with ACL reconstruction have shown good clinical outcomes, suggesting that biological stimulation without suturing may be sufficient in select cases.42,43 Indeed, a systematic review by Moreira et al. found no clear difference in outcomes between suture repair and abrasion/trephination alone for stable ramp lesions measuring less than 1.5 cm in length.18
Unstable and chronic lesions are generally treated with repair. Failing to repair an unstable ramp lesion could leave the knee biomechanically compromised even after an otherwise anatomic ACL reconstruction. As noted earlier, the repair of meniscocapsular and meniscotibial lesions reduces abnormal translation and rotation and decreases forces on the ACL graft. Following repair, patients have improved Lysholm and IKDC scores with durable stability documented by second-look arthroscopy.44,45,46 No single operative approach or fixation technique has been established with clear superiority, with both all-inside and inside-out techniques performed according to surgeon preference.
For radiologists, the key implication is not to decide whether a lesion should be repaired, but to describe features that may correlate with instability: tear length, degree of separation, involvement of the ligamentous attachments to the meniscus, and associated markers of high energy or chronicity. Such descriptions can help surgeons stratify which lesions might be managed expectantly versus those that are likely to warrant repair.
Future Directions
Although our understanding of ramp lesions has grown substantially, several important questions remain. Biomechanically, further work is needed to delineate the relative contributions of the posterior meniscocapsular unit to overall stability, and to define more precise thresholds of “instability” that may warrant repair. Prospective clinical studies directly comparing repair versus non-repair of stable lesions and the various surgical techniques, with standardized rehabilitation and objective measurements of laxity and cartilage health, are needed to refine treatment algorithms.
On the imaging side, advanced techniques such as 3D isotropic sequences, higher field strengths, flexion or weight-bearing MRI, and meniscal mapping may improve detection of subtle ramp lesions and permit assessment of healing.15-18,47
Conclusion
Medial meniscal ramp lesions are common, biomechanically important injuries in ACL-deficient knees. They occur in the vascularized portions of the peripheral PHMM and the posterior ligamentous attachments to the meniscus, and contribute to increased anterior tibial translation, rotational instability, and potentially elevated ACL graft forces. Large arthroscopic series and biomechanical experiments highlight that unstable ramp lesions can leave patients with residual instability even after a technically successful ACL reconstruction. MRI is specific but only moderately sensitive for their detection, making a systematic, anatomy-driven interpretation approach essential.
For radiologists, understanding the nuances of the posterior meniscocapsular unit anatomy, recognizing direct and indirect MRI signs, and integrating epidemiologic and biomechanical insights into everyday reporting can impact surgical decision-making and long-term outcomes for patients with ACL injuries.
References
- Strobel MJ. Knee joint – special part. In: Strobel MJ, editor. Manual of Arthroscopic Surgery. Berlin, Germany: Springer; 2002 ↩
- Bollen SR. Posteromedial meniscocapsular injury associated with rupture of the anterior cruciate ligament: a previously unrecognised association. J Bone Joint Surg Br. 2010;92(2):222–223. doi:10.1302/0301-620X.92B2.22974 ↩
- Liu X, Feng H, Zhang H, Hong L, Wang XS, Zhang J. Arthroscopic prevalence of ramp lesion in 868 patients with anterior cruciate ligament injury. Am J Sports Med. 2011;39(4):832–837. doi:10.1177/0363546510388933 ↩
- Sonnery-Cottet B, Praz C, Rosenstiel N, Blakeney WG, Ouanezar H, Kandhari V, et al. Epidemiological Evaluation of Meniscal Ramp Lesions in 3214 Anterior Cruciate Ligament-Injured Knees From the SANTI Study Group Database: A Risk Factor Analysis and Study of Secondary Meniscectomy Rates Following 769 Ramp Repairs. Am J Sports Med. 2018;46(13):3189–3197. doi:10.1177/0363546518800717 ↩
- Thaunat M, Ingale P, Penet A, Kacem S, Haidar I, Bauwens PH, et al. Ramp Lesion Subtypes: Prevalence, Imaging, and Arthroscopic Findings in 2156 Anterior Cruciate Ligament Reconstructions. Am J Sports Med. 2021;49(7):1813–1821. doi:10.1177/03635465211006103 ↩
- Balazs GC, Greditzer HGt, Wang D, Marom N, Potter HG, Marx RG, et al. Ramp Lesions of the Medial Meniscus in Patients Undergoing Primary and Revision ACL Reconstruction: Prevalence and Risk Factors. Orthop J Sports Med. 2019;7(5):2325967119843509. doi:10.1177/2325967119843509 ↩
- Seil R, Mouton C, Coquay J, Hoffmann A, Nuhrenborger C, Pape D, et al. Ramp lesions associated with ACL injuries are more likely to be present in contact injuries and complete ACL tears. Knee Surg Sports Traumatol Arthrosc. 2018;26(4):1080–1085. doi:10.1007/s00167-017-4598-3 ↩
- DePhillipo NN, Moatshe G, Chahla J, Aman ZS, Storaci HW, Morris ER, et al. Quantitative and Qualitative Assessment of the Posterior Medial Meniscus Anatomy: Defining Meniscal Ramp Lesions. Am J Sports Med. 2019;47(2):372–378. doi:10.1177/0363546518814258 ↩
- DePhillipo NN, Moatshe G, Brady A, Chahla J, Aman ZS, Dornan GJ, et al. Effect of Meniscocapsular and Meniscotibial Lesions in ACL-Deficient and ACL-Reconstructed Knees: A Biomechanical Study. Am J Sports Med. 2018;46(10):2422–2431. doi:10.1177/0363546518774315 ↩
- Papageorgiou CD, Gil JE, Kanamori A, Fenwick JA, Woo SL, Fu FH. The biomechanical interdependence between the anterior cruciate ligament replacement graft and the medial meniscus. Am J Sports Med. 2001;29(2):226–231. doi:10.1177/03635465010290021801 ↩
- Guegan B, Drouineau M, Common H, Robert H. All the menisco-ligamentary structures of the medial plane play a significant role in controlling anterior tibial translation and tibial rotation of the knee. Cadaveric study of 29 knees with the Dyneelax(R) laximeter. J Exp Orthop. 2024;11(3):e12038. doi:10.1002/jeo2.12038 ↩
- Stephen JM, Halewood C, Kittl C, Bollen SR, Williams A, Amis AA. Posteromedial Meniscocapsular Lesions Increase Tibiofemoral Joint Laxity With Anterior Cruciate Ligament Deficiency, and Their Repair Reduces Laxity. Am J Sports Med. 2016;44(2):400–408. doi:10.1177/0363546515617454 ↩
- Edgar C, Kumar N, Ware JK, Ziegler C, Reed DN, DiVenere J, et al. Incidence of Posteromedial Meniscocapsular Separation and the Biomechanical Implications on the Anterior Cruciate Ligament. J Am Acad Orthop Surg. 2019;27(4):e184–e192. doi:10.5435/JAAOS-D-17-00327 ↩
- Willinger L, Balendra G, Pai V, Lee J, Mitchell A, Jones M, et al. Medial meniscal ramp lesions in ACL-injured elite athletes are strongly associated with medial collateral ligament injuries and medial tibial bone bruising on MRI. Knee Surg Sports Traumatol Arthrosc. 2022;30(5):1502–1510. doi:10.1007/s00167-021-06671-z ↩
- Okazaki Y, Furumatsu T, Okamoto S, Hiranaka T, Kintaka K, Miyazawa S, et al. Diagnostic performance of open MRI in the flexed knee position for the detection of medial meniscus ramp lesions. Skeletal Radiol. 2020;49(11):1781–1788. doi:10.1007/s00256-020-03480-2 ↩
- DePhillipo NN, Cinque ME, Chahla J, Geeslin AG, Engebretsen L, LaPrade RF. Incidence and Detection of Meniscal Ramp Lesions on Magnetic Resonance Imaging in Patients With Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2017;45(10):2233–2237. doi:10.1177/0363546517704426 ↩
- Koo B, Lee SH, Yun SJ, Song JG. Diagnostic Performance of Magnetic Resonance Imaging for Detecting Meniscal Ramp Lesions in Patients With Anterior Cruciate Ligament Tears: A Systematic Review and Meta-analysis. Am J Sports Med. 2020;48(8):2051–2059. doi:10.1177/0363546519880528 ↩
- Moreira J, Almeida M, Lunet N, Gutierres M. Ramp lesions: a systematic review of MRI diagnostic accuracy and treatment efficacy. J Exp Orthop. 2020;7(1):71. doi:10.1186/s40634-020-00287-x ↩
- Andrews SH, Rattner JB, Abusara Z, Adesida A, Shrive NG, Ronsky JL. Tie-fibre structure and organization in the knee menisci. J Anat. 2014;224(5):531–537. doi:10.1111/joa.12170 ↩
- Kittl C, Becker DK, Raschke MJ, Muller M, Wierer G, Domnick C, et al. Dynamic Restraints of the Medial Side of the Knee: The Semimembranosus Corner Revisited. Am J Sports Med. 2019;47(4):863–869. doi:10.1177/0363546519829384 ↩
- Cavaignac E, Sylvie R, Teulières M, Fernandez A, Frosch KH, Gomez-Brouchet A, et al. What Is the Relationship Between the Distal Semimembranosus Tendon and the Medial Meniscus? A Gross and Microscopic Analysis From the SANTI Study Group. Am J Sports Med. 2021;49(2):459–466. doi:10.1177/0363546520980076 ↩
- Naendrup JH, Pfeiffer TR, Chan C, Nagai K, Novaretti JV, Sheean AJ, et al. Effect of Meniscal Ramp Lesion Repair on Knee Kinematics, Bony Contact Forces, and In Situ Forces in the Anterior Cruciate Ligament. Am J Sports Med. 2019;47(13):3195–3202. doi:10.1177/0363546519872964 ↩
- Matsumoto Y, Takahashi T, Hatayama K, Kubo T, Higuchi H, Kimura M, et al. Medial Meniscal Ramp Lesion Repair Concomitant With Anterior Cruciate Ligament Reconstruction Did Not Contribute to Better Anterior Knee Stability and Structural Properties After Cyclic Loading: A Porcine Model. Arthrosc Sports Med Rehabil. 2021;3(6):e1967–e1973. doi:10.1016/j.asmr.2021.09.019 ↩
- Vieira TD, Pioger C, Frank F, Saithna A, Cavaignac E, Thaunat M, et al. Arthroscopic Dissection of the Distal Semimembranosus Tendon: An Anatomical Perspective on Posteromedial Instability and Ramp Lesions. Arthrosc Tech. 2019;8(9):e987–e991. doi:10.1016/j.eats.2019.05.008 ↩
- Kunze KN, Wright-Chisem J, Polce EM, DePhillipo NN, LaPrade RF, Chahla J. Risk Factors for Ramp Lesions of the Medial Meniscus: A Systematic Review and Meta-analysis. Am J Sports Med. 2021;49(13):3749–3757. doi:10.1177/0363546520986817 ↩
- Kim SH, Park YB, Won YS. An Increased Lateral Femoral Condyle Ratio Is an Important Risk Factor for a Medial Meniscus Ramp Lesion Including Red-Red Zone Tear. Arthroscopy. 2021;37(10):3159–3165. doi:10.1016/j.arthro.2021.03.078 ↩
- Kim SH, Seo HJ, Seo DW, Kim KI, Lee SH. Analysis of Risk Factors for Ramp Lesions Associated With Anterior Cruciate Ligament Injury. Am J Sports Med. 2020;48(7):1673–1681. doi:10.1177/0363546520918207 ↩
- Kaplan PA, Gehl RH, Dussault RG, Anderson MW, Diduch DR. Bone contusions of the posterior lip of the medial tibial plateau (contrecoup injury) and associated internal derangements of the knee at MR imaging. Radiology. 1999;211(3):747–753. doi:10.1148/radiology.211.3.r99jn30747 ↩
- Calvo-Gurry M, Hurley ET, Withers D, Vioreanu M, Moran R. Posterior tibial bone bruising associated with posterior-medial meniscal tear in patients with acute anterior cruciate ligament injury. Knee Surg Sports Traumatol Arthrosc. 2019;27(11):3633–3637. doi:10.1007/s00167-019-05490-7 ↩
- Beel W, Mouton C, Tradati D, Nührenbörger C, Seil R. Ramp lesions are six times more likely to be observed in the presence of a posterior medial tibial bone bruise in ACL-injured patients. Knee Surg Sports Traumatol Arthrosc. 2022;30(1):184–191. doi:10.1007/s00167-021-06520-z ↩
- Kopf S, Beaufils P, Hirschmann MT, Rotigliano N, Ollivier M, Pereira H, et al. Management of traumatic meniscus tears: the 2019 ESSKA meniscus consensus. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1177–1194. doi:10.1007/s00167-020-05847-3 ↩
- Greif DN, Baraga MG, Rizzo MG, Mohile NV, Silva FD, Fox T, et al. MRI appearance of the different meniscal ramp lesion types, with clinical and arthroscopic correlation. Skeletal Radiol. 2020;49(5):677–689. doi:10.1007/s00256-020-03381-4 ↩
- Seil R, Hoffmann A, Scheffler S, Theisen D, Mouton C, Pape D. Ramp lesions : Tips and tricks in diagnostics and therapy. Orthopade. 2017;46(10):846–854. doi:10.1007/s00132-017-3461-z ↩
- Keyhani S, Mirahmadi A, Maleki A, Vosoughi F, Verdonk R, LaPrade RF, et al. Approaching ramp lesions from the different world of posterior knee compartment: A review of evidence with a proposal of a new classification and treatment. J Exp Orthop. 2024;11(4):e70018. doi:10.1002/jeo2.70018 ↩
- Tollefson LV, Tapasvi S, Seil R, Slette EL, LaPrade CM, LaPrade RF. Medial Meniscal Ramp Tears in Patients With Anterior Cruciate Ligament Tears Undergoing Reconstruction: A Surgically Relevant Classification System Based on Tear Morphology. Arthroscopy. 2025;41(10):4103–4111. doi:10.1016/j.arthro.2025.03.015 ↩
- Yeo Y, Ahn JM, Kim H, Kang Y, Lee E, Lee JW, et al. MR evaluation of the meniscal ramp lesion in patients with anterior cruciate ligament tear. Skeletal Radiol. 2018;47(12):1683–1689. doi:10.1007/s00256-018-3007-4 ↩
- Laurens M, Cavaignac E, Fayolle H, Sylvie R, Lapegue F, Sans N, et al. The accuracy of MRI for the diagnosis of ramp lesions. Skeletal Radiol. 2022;51(3):525–533. doi:10.1007/s00256-021-03858-w ↩
- Hatayama K, Terauchi M, Saito K, Aoki J, Nonaka S, Higuchi H. Magnetic Resonance Imaging Diagnosis of Medial Meniscal Ramp Lesions in Patients With Anterior Cruciate Ligament Injuries. Arthroscopy. 2018;34(5):1631–1637. doi:10.1016/j.arthro.2017.12.022 ↩
- Sonnery-Cottet B, Conteduca J, Thaunat M, Gunepin FX, Seil R. Hidden lesions of the posterior horn of the medial meniscus: a systematic arthroscopic exploration of the concealed portion of the knee. Am J Sports Med. 2014;42(4):921–926. doi:10.1177/0363546514522394 ↩
- Kim SH, Lee SH, Kim KI, Yang JW. Diagnostic Accuracy of Sequential Arthroscopic Approach for Ramp Lesions of the Posterior Horn of the Medial Meniscus in Anterior Cruciate Ligament-Deficient Knee. Arthroscopy. 2018;34(5):1582–1589. doi:10.1016/j.arthro.2017.12.008 ↩
- Yagishita K, Muneta T, Ogiuchi T, Sekiya I, Shinomiya K. Healing potential of meniscal tears without repair in knees with anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32(8):1953–1961. doi:10.1177/0363546504263702 ↩
- Yang J, Guan K, Wang JZ. Clinical study on the arthroscopic refreshing treatment of anterior cruciate ligament injury combined with stable medial meniscus ramp injury. J Musculoskelet Neuronal Interact. 2017;17(2):108–113. ↩
- Liu X, Zhang H, Feng H, Hong L, Wang XS, Song GY. Is It Necessary to Repair Stable Ramp Lesions of the Medial Meniscus During Anterior Cruciate Ligament Reconstruction? A Prospective Randomized Controlled Trial. Am J Sports Med. 2017;45(5):1004–1011. doi:10.1177/0363546516682493 ↩
- DePhillipo NN, Dornan GJ, Dekker TJ, Aman ZS, Engebretsen L, LaPrade RF. Clinical Characteristics and Outcomes After Primary ACL Reconstruction and Meniscus Ramp Repair. Orthop J Sports Med. 2020;8(4):2325967120912427. doi:10.1177/2325967120912427 ↩
- Ahn JH, Wang JH, Yoo JC. Arthroscopic all-inside suture repair of medial meniscus lesion in anterior cruciate ligament–deficient knees: results of second-look arthroscopies in 39 cases. Arthroscopy. 2004;20(9):936–945. doi:10.1016/j.arthro.2004.06.038 ↩
- Bumberger A, Koller U, Hofbauer M, Tiefenboeck TM, Hajdu S, Windhager R, et al. Ramp lesions are frequently missed in ACL-deficient knees and should be repaired in case of instability. Knee Surg Sports Traumatol Arthrosc. 2020;28(3):840–854. doi:10.1007/s00167-019-05521-3 ↩
- Severyns M, Zot F, Harika-Germaneau G, Germaneau A, Herpe G, Naudin M, et al. Extrusion and meniscal mobility evaluation in case of ramp lesion injury: a biomechanical feasibility study by 7T magnetic resonance imaging and digital volume correlation. Front Bioeng Biotechnol. 2023;111289290. doi:10.3389/fbioe.2023.1289290 ↩
