Clinical History
A 19 year old college baseball pitcher heard a “pop” after throwing a ball. Axial fat-suppressed proton density-weighted (1A and 1B), coronal fat-suppressed T2-weighted images (1C), and a Grashey projection radiograph (1D) images are provided. What are the findings? What is your diagnosis?




Findings




Figure 2: (2A) An axial image at the level of the humeral lesser tuberosity (LT) shows an intact subscapularis tendon (arrowheads). (2B) More inferiorly at the level of the humeral neck (HN), the direct muscular attachment of subscapularis (yellow arrows) is avulsed from the humerus together with the anterior band of the inferior glenohumeral ligament (red arrow), representing humeral avulsion of the glenohumeral ligament, a HAGL lesion. (2C) A coronal image through the anterior humerus shows the avulsed direct muscular attachment of subscapularis (yellow arrows), and the retracted end of the torn anterior band of the inferior glenohumeral ligament (red arrow). (2D) The radiograph shows a small, avulsed bone fragment of the humerus (red arrow), making this injury a “bony” HAGL (BHAGL) lesion. He failed 3 weeks of conservative management, with persistent 7/10 shoulder pain and was managed operatively with a lesser tuberosity repair. 6 months later, after taking a hiatus from baseball, his pain was completely resolved.
Diagnosis
Anteroinferior glenohumeral capsular injury consisting of avulsion of the direct muscular attachment of subscapularis and “bony” humeral avulsion of the anterior band of the inferior glenohumeral ligament (BHAGL injury).
Introduction
Injuries to the anteroinferior shoulder capsule can result in shoulder instability, with anterior shoulder dislocations, trauma, and ball-throwing injuries being major causal etiologies. The shoulder joint capsule is an important structure required for shoulder stability, with the anterior band of the inferior glenohumeral ligament (IGHL) being a major passive stabilizer of the glenohumeral joint against anterior shoulder dislocations.
This Web Clinic highlights injuries to the shoulder capsule, including anterior and posterior humeral avulsion of the glenohumeral ligament (HAGL lesions), as well as a rarely recognized imaging finding often seen in conjunction HAGL lesions: injury to the direct muscular attachment of subscapularis. These muscle injuries do not typically require specific treatment but can be associated with extensive hemorrhage.
Relevant Anatomy
Inferior glenohumeral ligament (IGHL)
The IGHL is a hammock or sling-shaped structure along the inferior glenohumeral joint, connecting the glenolabral rim to the surgical neck of the humerus. It forms part of the joint capsule along with the middle and superior glenohumeral ligaments (MGHL and SGHL respectively).
The IGHL (Figures 3 and 4) is comprised of an anterior band, axillary pouch, and posterior band. These bands represent focal thickenings of the joint capsule rather than distinct ligaments separable from the joint capsule.1 Owing to this merged appearance of the ligaments with the capsule, the anterior and posterior bands may be difficult to identify on MRI, even on arthrographic images. The classic description of the anterior band indicates an origin directly from the anteroinferior labrum; however, a recent MRI analysis describes variants: the anterior band originating either directly from the labrum (type 1, 54%) or from the adjacent glenoid rim (type 2, 46%).2 The anterior and posterior bands both insert on the surgical neck of the humerus, immediately inferior to the humeral head articular surface. The axillary pouch connects the anterior and posterior bands and is the most caudal capsular segment, generally considered less important for shoulder instability compared to the anterior band.

Figure 3. Illustration of the sling-like morphology of the inferior glenohumeral ligament complex. The anterior band (arrowheads), axillary pouch, and posterior band form a “hammock” along the inferior half of the glenohumeral joint.






Figure 4: Normal anatomy of the inferior glenohumeral ligament (IGHL) complex. (4A-4C) Oblique coronal fat-suppressed MR arthrogram images from anterior to posterior show the anterior band (4A, red arrow), axillary pouch (4B, green arrow), and posterior band (4C, white arrow) of the IGHL. (4D-4F) Oblique sagittal fat-suppressed MR arthrogram images from medial to lateral show the anterior band (4D, red arrow), axillary pouch (4E, green arrow), and posterior band (4F, white arrow) of the IGHL. Note that the anterior band is thicker than the posterior band. These capsular ligaments are not always clearly visible, especially without joint distention, due to variations in shape and thickness, and their curved courses.
The thickness of the IGHL decreases from anteriorly to posteriorly (Figures 4 and 5), with the average thickness of the anterior band measuring 2.8 mm, and the posterior band measuring 1.7 mm, likely reflecting the greater stabilizing role of the anterior band in anterior shoulder dislocations as compared to uncommon posterior shoulder dislocations.3 In cadaveric studies, the anterior band of the IGHL has been reported as absent in approximately 10% of subjects, so its absence may be considered a normal variant.4

Figure 5: Normal anatomy of the inferior glenohumeral ligament (IGHL) complex. Axial fat-suppressed T1-weighted MR arthrogram image at the level of the inferior glenoid (G) shows the thick anterior (red arrow) and thin posterior (white arrow) bands of the IGHL. The axillary pouch is located more inferiorly. H = humerus.
It is important to not mistake the nearby MGHL for the anterior band. A way to differentiate these two structures in the axial and sagittal planes is to note that the MGHL parallels and then fuses with the deep aspect of the subscapularis tendon, whereas the anterior band of the IGHL never merges with the subscapularis (Figure 6).


Figure 6: Differentiating portions of the inferior glenohumeral ligament (IGHL) complex. (6A) Oblique sagittal fat-suppressed T2-weighted MR arthrogram image showing the anterior band of the IGHL (yellow arrows) extending inferior from the anterior glenoid margin. Note that the ligament remains separate from the subscapularis tendon (S) throughout its course. (6B) Oblique sagittal MR arthrogram image showing the middle glenohumeral ligament (red arrows), originating from the anterosuperior glenoid and extending inferiorly, paralleling and eventually fusing with the deep surface of the subscapularis tendon (S).
Direct muscular attachment of the subscapularis
The subscapularis muscle is a triangular-shaped rotator cuff muscle, originating from the anterior scapular surface. Its main function is an internal humeral rotator in conjunction with pectoralis major, latissimus dorsi, and teres major. It also has an additional stabilizing role particularly when the shoulder is in abduction and external rotation. The main insertion of the subscapularis is through a multipennate tendon to the lesser tuberosity of the humerus, which is at risk for tears as an isolated injury and in association with tears of the remainder of the rotator cuff tendons, as detailed in a recent Radsource Web Clinic. Additionally, the subscapularis has a lesser appreciated direct muscular insertion immediately inferior to the tendon attachment, along the surgical neck of the humerus. situated at the surgical neck of the humerus. The tendon has been estimated to originate from the superior 60% of the subscapularis muscle, whereas the direct muscular attachment of subscapularis originates from the lower 40% of the muscle (Figures 7 and 8).5 The close proximity of the direct humeral subscapularis attachment and the anterior band of the IGHL, predisposes to co-injury of both structures.

Figure 7: Anatomic drawing of the subscapularis showing the muscular (red) and tendinous (beige) components. Note the direct insertion of muscle fibers onto the humerus inferiorly.


Figure 8: Normal anatomy of the subscapularis direct muscular attachment: (8A) Axial fat-suppressed T1-weighted image from an MR arthrogram at the level of the inferior glenoid (G) shows the inferior muscle fibers of the subscapularis (yellow arrows) inserting onto the surgical neck of the humerus (H). The anterior band of the inferior glenohumeral ligament (red arrow) is located deep to the subscapularis muscle insertion. (8B) Coronal T1-weighted MR arthrogram image shows the inferior subscapularis muscle fibers passing caudal to the joint capsule and directly attaching to the humeral neck (yellow arrows). Note the proximity to the anterior band of the inferior glenohumeral ligament (red arrows), which is located deep to the subscapularis with a less broad insertion.
The subscapularis muscle and tendon together act as both passive (without muscle contraction) and active (with muscle contraction) shoulder stabilizers. In an EMG study of throwers, the subscapularis muscle remained noncontractile in certain phases of the throwing motion but still played a role in joint stabilization.6 Cadaveric studies of arthroscopic tendon release found the tendon important for inhibiting anterior and inferior shoulder translation.7
Humeral avulsion of the glenohumeral Ligament (HAGL injuries)
Clinical Features
HAGL injuries are rare but clinically important injuries that can contribute to long-term shoulder instability and persistent pain. They should be considered as a potential missed cause of recurrent shoulder instability in patients with prior anterior shoulder dislocations who do not have a labral tear or glenoid bone loss.
HAGL is a general term that can describe an avulsion of any part of the IGHL complex – the anterior band, axillary pouch, and/or posterior band – from the humerus. The anterior band is the most commonly injured component, as it plays a major role in resisting hyperabduction and external rotation, and is subject to injury with anterior shoulder dislocations. In one case review, injuries to the anterior band comprised over 90% of identified IGHL injuries, whereas the remaining <10% cases involved the posterior band.8 While this case review did not identify isolated axillary pouch injuries and included them as co-injuries with tears of anterior and posterior bands, a separate publication describes axillary pouch HAGL injuries in female college volleyball players caused by repetitive microtrauma, describing 4 patients with surgically-proven isolated axillary pouch tears (with intact anterior and posterior bands) who underwent subsequent repair.9
In cadaveric studies of tensile strength, anterior band tears are estimated to occur with 40% frequency at the glenolabral attachment (GAGL lesion), 25% at the humeral insertion (HAGL), and 35% intrasubstance.3 It is however important to note that these cadaveric percentages may differ from the incidence encountered in clinical cases, where reports and imaging examples of pure GAGL injuries are rare.10 HAGL lesions have been estimated to have a prevalence of 1.6% on shoulder MRI examinations, and 9% on shoulder MRI examinations in patients with recurrent shoulder instability.11,12
Patients with a HAGL diagnosis are 94% male with average age of 25-30.13 HAGL injuries usually occur after an anterior shoulder dislocation, but can also occur in pitchers and other high-velocity throwing athletes as part of anteroinferior capsular injuries (Figures 1 and 2).9,14,15 HAGL injuries should be considered in patients with recurrent unexplained shoulder instability, especially if they have had previous anterior shoulder dislocation(s).
West Point Classification of IGHL/HAGL Injuries
A useful framework to understand injuries to the anterior band of the IGHL is the West Point classification system developed by Bui-Mansfeld et al (Figure 9).16 In this classification, humeral avulsions are categorized as HAGL lesions, BHAGL if a bony fragment accompanies the torn ligament, and a floating anterior band IGHL if tears occur at both the humeral attachment and along the ligament proper. This classification is similarly applied to the far less common posterior band injuries.
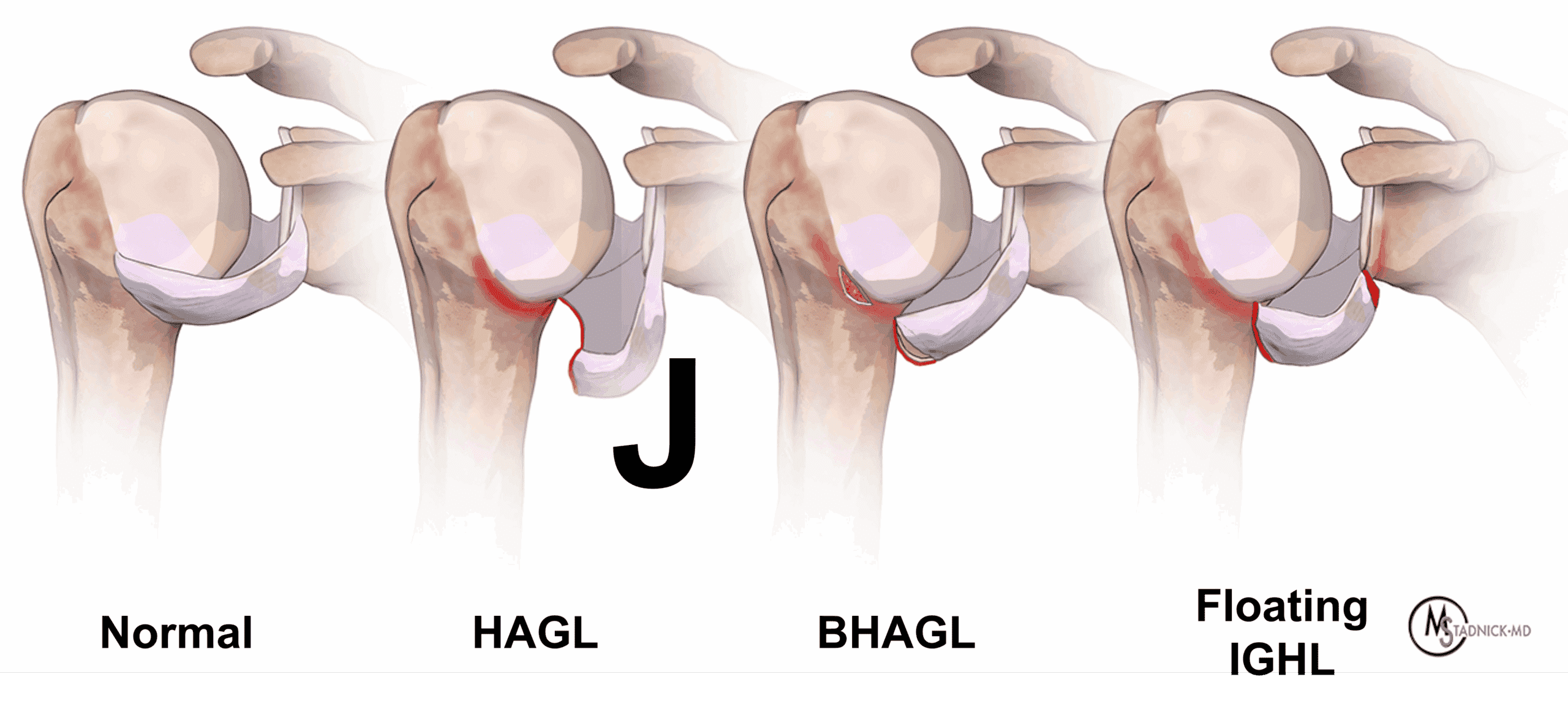
Figure 9 : West Point classification of injuries to the anterior band, inferior glenohumeral ligament (IGHL).16 From left to right, coronal drawings show a normal anterior band, classic HAGL lesion with the ligament torn from the humerus, forming a “J”-shape, BHAGL lesion with an avulsed fracture fragment attached to the ligament, and a floating IGHL injury with the ligament detached on both the humeral and glenoid sides.
The authors of the West Point Classification scheme reported percentages of the types of injuries they encountered in their population of MRI-diagnosed IGHL injuries. 55% were classic HAGL lesions, 17% were BHAGL lesions, and 21% were floating IGHL injuries. Only 7% were posterior band injuries. 62% of the reviewed HAGL diagnoses had concomitant shoulder injuries, most commonly (25%) labral tears.
MRI Diagnosis
MRI is required for diagnosis for noninvasive anteroinferior capsular injuries, with other modalities (CT, US, radiographs) playing a much more limited role. The literature describes the appearance of the torn anterior band of the IGHL as a “J” or “reverse-J” shape (depending on whether the humeral head is located on the right or left) on coronal images, and “U”-shaped when intact (Figure 9). In practice, however, the MRI pattern of such injuries is often complex and not characteristic, so these described shapes of injury should be used more as a paradigm of injury rather than as a commonly expected pattern of injury.
MR arthrography is more sensitive than conventional MRI for evaluating IGHL injuries, providing joint distention and contrast outlining the IGHL. However, caution should still be exercised diagnosing the exact location of IGHL injuries on MR arthrograms: a small case series of 4 MR arthrograms with preoperative diagnoses of HAGL injuries noted that none of the 4 patients had true HAGL lesions at arthroscopy despite suggestive MR findings.1 The authors noted that trauma to the IGHL outside the humeral attachment (axillary pouch, posterior band, labrum) could mimic the appearance of a HAGL lesion on MR arthrograms, and they proposed a more general description of ‘injury to the inferior glenohumeral complex’ rather than HAGL. MR arthrogram findings should be evaluated together with clinical symptoms such as recurrent unexplained shoulder instability or persisting pain when considering a diagnosis of HAGL or capsular injury. BHAGL injuries can be suspected on radiographs when a cortical avulsion fracture fragment is visible, but MRI is needed to confirm the diagnosis.
HAGL injuries can be difficult to diagnose in the acute phase of injury due to the prominent soft tissue and capsular edema, which can distort the typical appearance of the joint capsule, but should be suspected when the anterior band of the IGHL does not appear to insert on the humeral neck (Figure 10). Contrast extravasation inferiorly along the humeral neck after arthrography should increase suspicion of a HAGL lesion (Figure 11). On MR arthrograms, images obtained with the arm abducted and externally rotated (the ABER position), may be useful for subtle avulsions because the anterior band of the IGHL is placed under tension in this position (Figure 12).


Figure 10: 20-year-old man with HAGL injury. (10A) Fluoroscopic image from MR arthrogram injection shows injected contrast extravasating past of the inferior joint capsule along the proximal humeral shaft (arrow). (10B) Coronal fat-suppressed T1-weighted image from an MR arthrogram shows the anterior band of the inferior glenohumeral ligament torn and retracted (yellow arrow) from its insertion site on the humerus (asterisk). The muscular insertion of the subscapularis also appears avulsed (red arrow). Compare to Figure 8B. The torn structures allow injected contrast to extravasate into the fascia inferior to the axillary pouch (arrowheads).



Figure 11: Acute HAGL in a 24-year-old with multidirectional instability. (11A) Fluoroscopic image from arthrogram injection showing contrast extravasating inferior to the joint capsule along the humeral neck (arrow), raising suspicion for a capsular tear. (11B) Coronal fat-suppressed T2-weighted MR arthrogram image shows a torn anterior band, inferior glenohumeral ligament (red arrow) creating a “J” sign. Inferior contrast extravasation (yellow arrow) corresponds to the fluoroscopic image (11A). (11C) Sagittal fat-suppressed T2-weighted MR arthrogram image shows the full extent of the tear, which involves nearly the entire inferior joint capsule, with torn anterior band, axillary pouch, and possibly posterior band (between arrows).


Figure 12: 16-year-old female volleyball player with repetitive injury and a HAGL lesion involving the axillary pouch. (12A) Coronal fat-suppressed T1-weighted image from an MR arthrogram image shows the axillary pouch fibers of the inferior glenohumeral ligament (arrows) avulsed from the insertion site on the humerus (asterisk). (12B) ABER T2-weighted image shows the IGHL (arrows) originating from the tip of the anteroinferior glenoid labrum and coursing anterior to the humeral head (H) but not inserting on the humeral neck (asterisk). G = glenoid. The HAGL lesion was confirmed at arthroscopy and the patient underwent capsular repair.
The posterior band of the IGHL resists posterior shoulder translation. It is injured far less frequently than the anterior band, with less than 10% of cases of HAGL involving the posterior band.17 Football players (typically lineman) are susceptible to posterior HAGL (PHAGL) injuries due to traumatic force pushing the humeral head posteriorly during blocking. The torn posterior band is usually easiest to see on axial images posterior to the humerus, or on coronal images through the posterior glenohumeral joint, where a “J” or “reverse J” appearance can be created (Figures 13 – 15).

Figure 13: PHAGL in a patient with shoulder pain. Axial fat-suppressed proton-density weighted image at the level of the inferior glenoid shows the posterior band of the inferior glenohumeral ligament (arrows) originating from the posterior labrum and coursing dorsal to the humeral head. The ligament is avulsed from its insertion site on the humerus (asterisk) and appears lax.


Figure 14: PHAGL in a 16-year-old football lineman after injury. (14A) Axial fat-suppressed T1-weighted image from an MR arthrogram shows the posterior band of the IGHL (arrows) avulsed from the humerus. (14B) Coronal fat-suppressed T1-weighted MR arthrogram image through the posterior aspect of the glenohumeral joint shows the avulsed posterior band (arrows) forming a “J” shape.
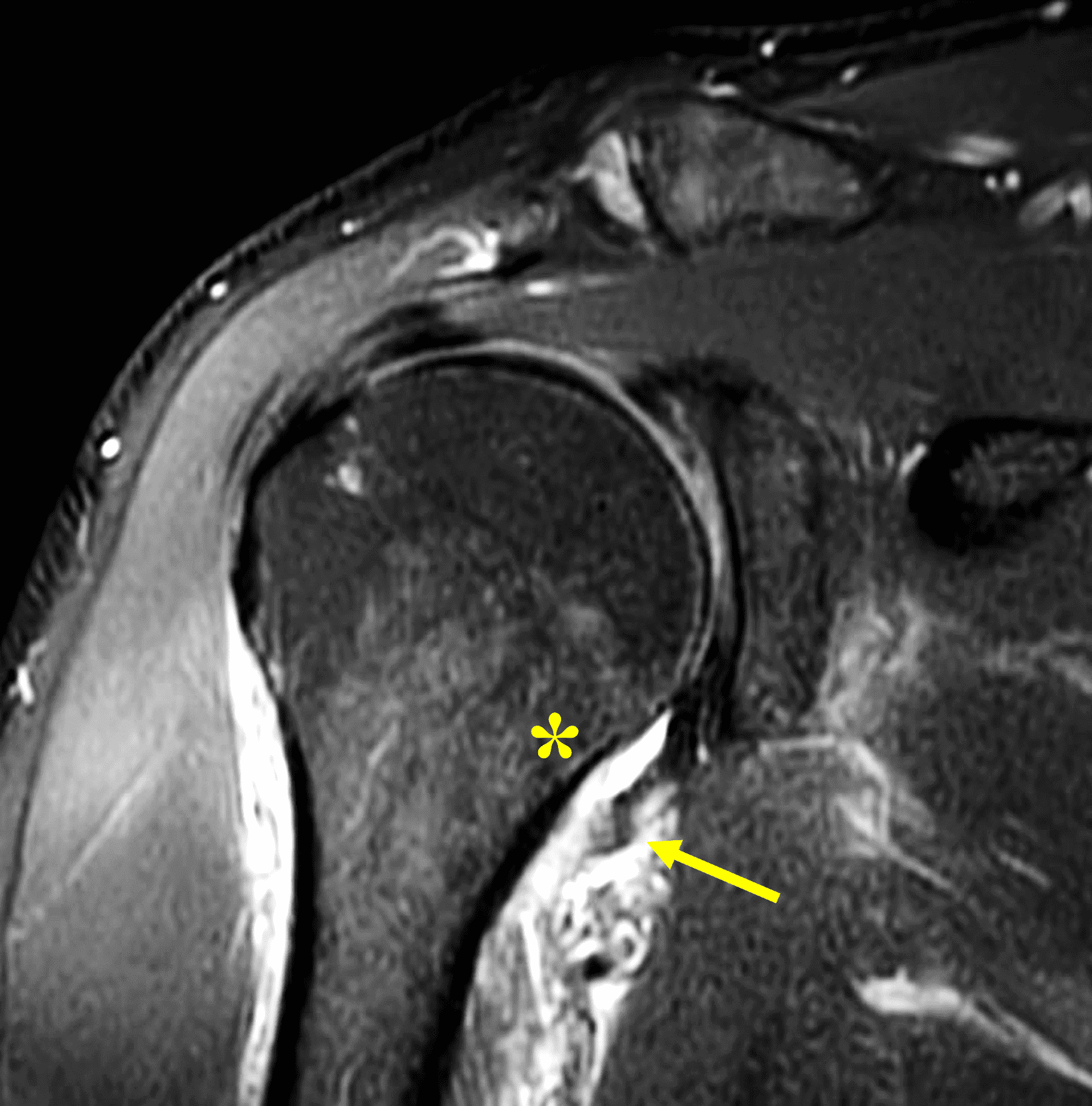
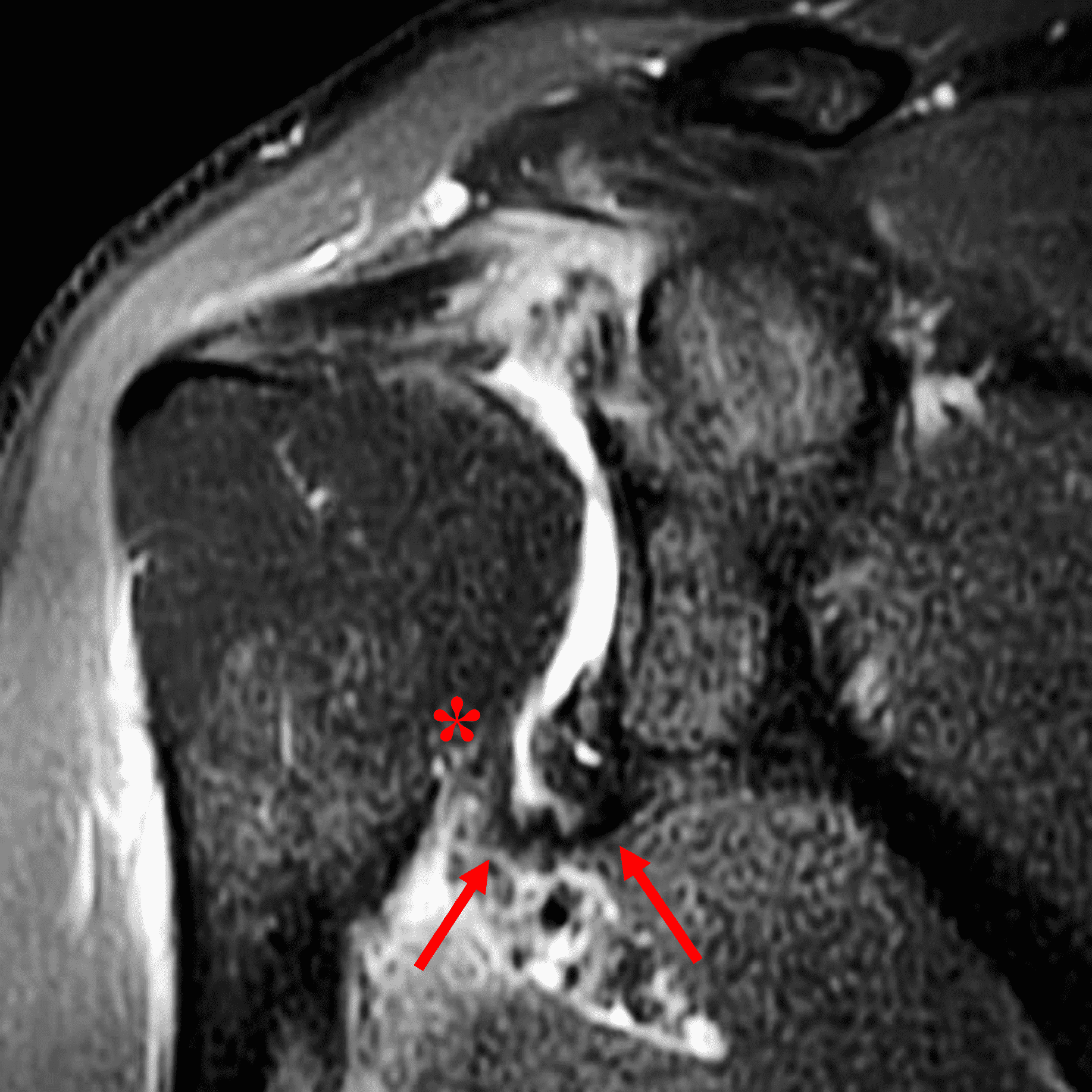
Figure 15: PHAGL injury 1 week after a mountain bike accident. (15A) Coronal fat-suppressed proton-density weighted image through the posterior glenoid shows the posterior band of the IGHL (arrow) avulsed from its humeral insertion (asterisk), with surrounding soft tissue edema. (15B) For comparison in the same patient, a coronal image through the anterior glenoid shows an intact anterior band of the IGHL (arrows) inserting on the humerus (asterisk).
HAGL/IGHL injuries vs. contrast extravasation on MR arthrography
A challenge in the diagnosis of HAGL/IGHL injuries with MR arthrography is differentiating iatrogenic contrast extravasation from extravasation through a true capsular tear. The location of the contrast in both can overlap, and thus criteria have been developed to help distinguish between the two conditions.
A study performed in 2014 by Maldjian et al.18 investigated 12 arthroscopically proven HAGL lesions and found that contrast extravasation into an extra-articular anatomical space, specifically, along the proximal humeral diaphysis, or into the quadrilateral space or other paramuscular location, was present in 10 of 12 of their cases. Extravasation into known bursal spaces such as the subacromial subdeltoid bursa or subcoracoid region did not predict capsular tears. Subsequently in 2018, a review of 1740 MR arthrograms was performed by Wang et al.19 to identify MR arthrogram features to distinguish between IGHL tears and extravasation. In 16 cases of arthroscopically proven true IGHL tears, the presence of a torn anterior IGHL band, thick ligament, reversed-tapered ligament caliber (thicker at the torn distal end and thinner proximally), and scarring of the torn margin were found to be 100% specific (Figure 16). In contrast, isolated disruption of the posterior axillary pouch (the thinnest portion of the IGHL) but with preserved anterior and posterior bands was found to be 100% specific for iatrogenic extravasation.

Figure 16: Acute HAGL lesion in a 36 year old. Coronal fat-suppressed T2-weighted image from an MR arthrogram shows contrast extravasation from the inferior glenohumeral joint (yellow arrow). The presence of the thick, edematous, torn anterior band of the IGHL (red arrows) is highly specific for a HAGL lesion rather than iatrogenic contrast extravasation.
Injuries of the direct subscapularis muscular attachment
Clinical Features
Injury to the direct muscular attachment of subscapularis can coexist with a HAGL lesion given the close proximity of the subscapularis muscle insertion to the anterior band of the IGHL (Figure 8). Etiologies of direct subscapularis muscular attachment injuries are not clearly described in the literature; however, these are assumed to overlap those of HAGL injuries, which include anterior shoulder dislocation, trauma, and pitching/ball-throwing. Injuries to the subscapularis tendon can also occur in conjunction with injuries to the direct muscular attachment (Figure 17).



Figure 17: Injury involving both the muscle and tendon insertions of the subscapularis. (17A) Axial fat-suppressed proton-density weighted image shows a high-grade strain and interstitial tearing of the direct subscapularis muscular attachment (red arrow). (17B) On an axial image cranial to 17A, the subscapularis tendon is completely torn from the lesser tuberosity (yellow arrow). (17C) Coronal fat-suppressed T2-weighted image demonstrates a low-grade sprain of the nearby anterior band of the inferior glenohumeral ligament (white arrow).
A pattern of injury has recently been described in pitchers and forceful ball throwers, who can injure the inferior subscapularis with sparing of the upper subscapularis muscle and tendon, like in the test case (Figures 1 and 2).20 A retrospective review of MRI scans from a Major League Baseball organization over a 5 year period identified 11 of 133 MRIs with subscapularis injury, 10 of which showed injuries occurring in the inferior half of subscapularis at the myotendinous junction, with sparing of the tendon.21 These inferior myotendinous injuries can extend to involve the direct muscular attachment at the humerus.
On MRI, injuries to the direct muscular attachment can manifest with edema and hemorrhage within the muscle and surrounding soft tissues, and/or avulsion of the muscle from the humerus. The lower signal intensity of the anterior band of the IGHL allows it to be distinguished from the direct muscular attachment of subscapularis, which can be important if the anterior band is torn and retracted (Figure 18). In these cases, the muscle tissue should not be mistaken for an intact IGHL. Hematomas may occur with injuries of the direct muscular attachment and can become quite large as they expand within the axillary soft tissues (Figure 19).



Figure 18: Injuries to direct muscular insertion of the subscapularis and HAGL lesion following recent shoulder dislocation (18A) Coronal fat-suppressed proton-density weighted shows a high-grade strain and partial-thickness interstitial tearing of the direct subscapularis muscular attachment (yellow arrows). The torn and retracted inferior glenohumeral ligament is not visible on this image. (18B) Coronal image just posterior to 18A shows a torn anterior band of the IGHL (red arrows) forming a “J” sign. (18C) Axial fat-suppressed proton-density weighted image shows both the strained muscle attachment of the subscapularis (yellow arrow) and the torn anterior band of the inferior glenohumeral ligament (red arrow).
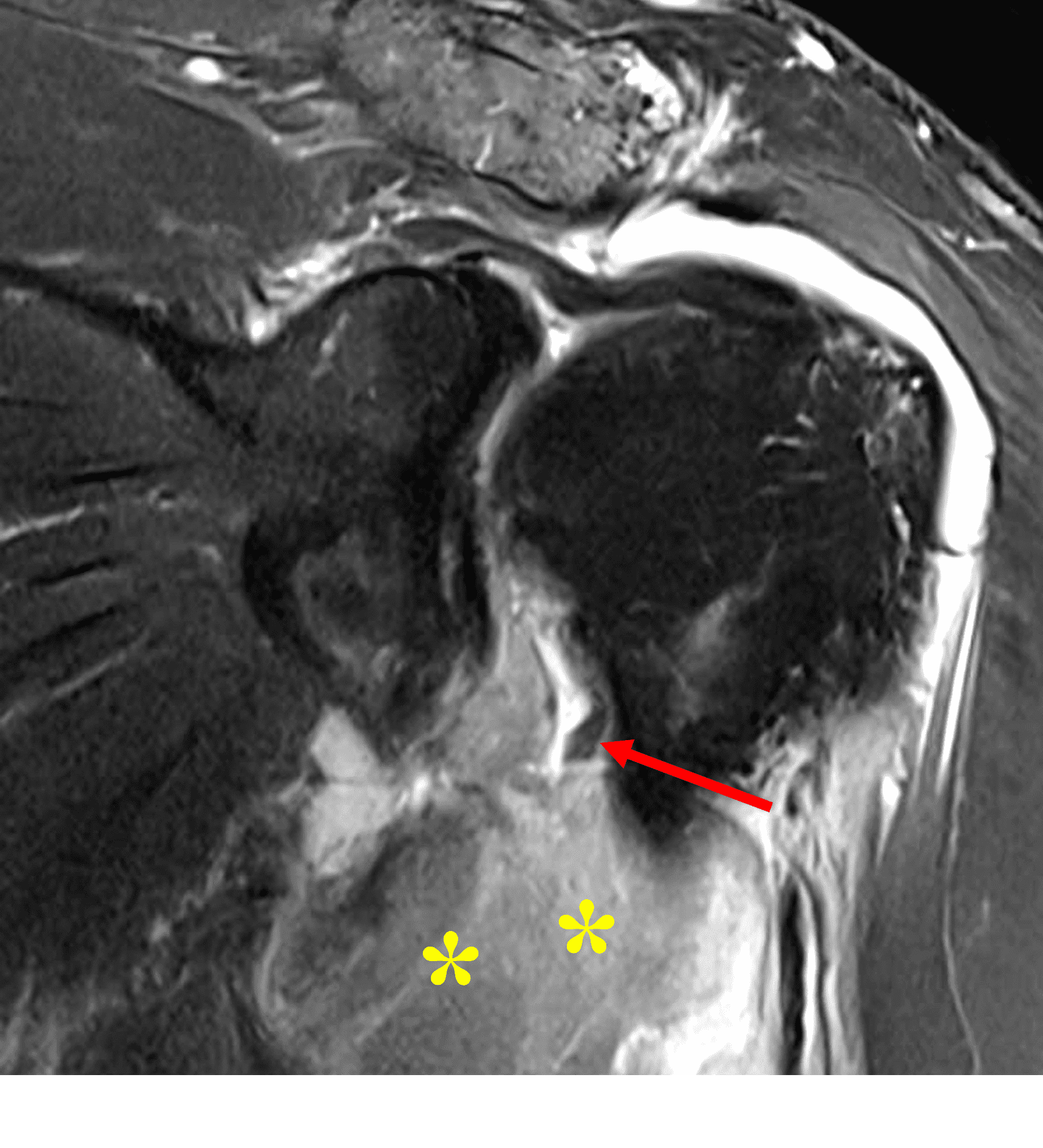

Figure 19: Ruptured subscapularis muscle insertion and associated hematoma in a 54-year-old man after a fall. (19A) Coronal fat-suppressed T2-weighted image shows a large hematoma (asterisks) in the area of a ruptured direct attachment of subscapularis to the humeral neck. Also visible is a tear of the anterior band, inferior glenohumeral ligament with small remnant stump (arrow). (19B). Axial fat-suppressed proton-density-weighted image shows the extent of the hematoma (asterisks).
Treatment
HAGL lesions presenting with instability typically require surgical capsular repair, with nonoperative treatment reserved for patients without shoulder instability.22 A 2017 literature review of surgical treatments and outcomes for HAGL injuries found both arthroscopic and open repair highly effective, with most patients returning to play at their previous levels, including Olympic and professional athletes.13 Arthroscopic HAGL repair is currently the favored technique.23 ,24 A posterior arthroscopic viewing portal is used to evaluate the rotator cuff, capsulolabral complex, cartilage, and biceps tendon as additional injuries are common, and then the HAGL lesion is addressed. The humeral neck is debrided and suture anchors placed anteriorly and posteriorly around the capsular tear, followed by a repair suture placed through the IGHL for reattachment to the humeral neck. A second suture anchor can be placed posterolaterally to help restore full tension to the IGHL complex. Postoperative rehabilitation includes limited passive range of motion for 3 weeks, 3 weeks of full passive range of motion, and active and active-assisted range of motion at 6 weeks. Full recovery to activities typically requires 3 months.
Tears and injuries to the direct subscapularis attachment to the humerus are typically managed conservatively and heal without surgery. Operative management is indicated for tears of the subscapularis tendon rather than the direct muscle attachment, usually considered after failure of conservative treatment or following acute high-grade traumatic tendon tears.
Conclusion
HAGL is a rare injury that most frequently occurs in young male patients, usually involving the anterior band of the IGHL. Most cases are due to anterior shoulder dislocation or throwing injuries. An untreated HAGL can lead to shoulder instability in addition to pain, and undiagnosed HAGL/capsular tears are potentially overlooked source of chronic/recurrent shoulder pain and instability. MRI and MR arthrogram are the best imaging studies for diagnosis, but findings such as inferior contrast extravasation can be nonspecific. Identification of the torn elements of the IGHL is the key finding. Arthroscopic repair is recommended for HAGL injuries with shoulder instability.
Injury to the subscapularis direct muscular attachment can accompany HAGL lesions due to the proximity of these structures, and isolated injuries to the inferior subscapularis muscle have been reported, most frequently in throwing athletes. The muscle attachment of the subscapularis can be identified along the anteroinferior aspect of the glenohumeral joint, superficial to the thinner anterior band of the IGHL. Most injuries of the subscapularis muscle attachment are managed conservatively, although concomitant unstable HAGL injuries and subscapularis tendon tears may require surgery.
References
- Melvin JS, Mackenzie JD, Nacke E, Sennett BJ, Wells L. MRI of HAGL lesions: four arthroscopically confirmed cases of false-positive diagnosis. AJR Am J Roentgenol. 2008;191(3):730–734. doi:10.2214/AJR.07.3631 ↩
- Simao MN, Kobayashi MJ, Hernandes MA, Nogueira-Barbosa MH. Evaluation of variations of the glenoid attachment of the inferior glenohumeral ligament by magnetic resonance arthrography. Radiol Bras. 2021;54(3):148–154. doi:10.1590/0100-3984.2020.0043 ↩
- Ticker JB, Flatow EL, Pawluk RJ, Soslowsky LJ, Ratcliffe A, Arnoczky SP, et al. The inferior glenohumeral ligament: a correlative investigation. J Shoulder Elbow Surg. 2006;15(6):665–674. doi:10.1016/j.jse.2005.11.006 ↩
- Ide J, Maeda S, Takagi K. Normal variations of the glenohumeral ligament complex: an anatomic study for arthroscopic Bankart repair. Arthroscopy. 2004;20(2):164–168. doi:10.1016/j.arthro.2003.11.005 ↩
- Arciero RA, Cordasco FA, Provencher MT. Shoulder and Elbow Injuries in Athletes: Elsevier; 2018. ↩
- Jobe FW, Tibone JE, Perry J, Moynes D. An EMG analysis of the shoulder in throwing and pitching. A preliminary report. Am J Sports Med. 1983;11(1):3–5. doi:10.1177/036354658301100102 ↩
- Marquardt B, Garmann S, Hurschler C, Pötzl W, Steens W, Witt KA, et al. The influence of arthroscopic subscapularis tendon and anterior capsular release on glenohumeral translation: a biomechanical model. J Shoulder Elbow Surg. 2006;15(4):502–508. doi:10.1016/j.jse.2005.09.018 ↩
- Bui-Mansfield LT, Taylor DC, Uhorchak JM, Tenuta JJ. Humeral avulsions of the glenohumeral ligament: imaging features and a review of the literature. AJR Am J Roentgenol. 2002;179(3):649–655. doi:10.2214/ajr.179.3.1790649 ↩
- Taljanovic MS, Nisbet JK, Hunter TB, Cohen RP, Rogers LF. Humeral avulsion of the inferior glenohumeral ligament in college female volleyball players caused by repetitive microtrauma. Am J Sports Med. 2011;39(5):1067–1076. doi:10.1177/0363546510391155 ↩
- Mannem R, DuBois M, Koeberl M, Kosempa D, Erickson S. Glenoid avulsion of the glenohumeral ligament (GAGL): a case report and review of the anatomy. Skeletal Radiol. 2016;45(10):1443–1448. doi:10.1007/s00256-016-2449-9 ↩
- Wolf EM, Cheng JC, Dickson K. Humeral avulsion of glenohumeral ligaments as a cause of anterior shoulder instability. Arthroscopy. 1995;11(5):600–607. doi:10.1016/0749-8063(95)90139-6 ↩
- Tirman PF, Steinbach LS, Feller JF, Stauffer AE. Humeral avulsion of the anterior shoulder stabilizing structures after anterior shoulder dislocation: demonstration by MRI and MR arthrography. Skeletal Radiol. 1996;25(8):743–748. doi:10.1007/s002560050172 ↩
- Bozzo A, Oitment C, Thornley P, Yan J, Habib A, Hoppe DJ, et al. Humeral Avulsion of the Glenohumeral Ligament: Indications for Surgical Treatment and Outcomes-A Systematic Review. Orthop J Sports Med. 2017;5(8):2325967117723329. doi:10.1177/2325967117723329 ↩
- Ahmad C. Glenohumeral Capsule Tears in Baseball Pitchers 2018 [Available from: foreonline.org/wp-content/uploads/2018/11/9.-Ahmad-Glenohumeral-Capsule-Tears.pdf. ↩
- Gehrmann RM, DeLuca PF, Bartolozzi AR. Humeral avulsion of the glenohumeral ligament caused by microtrauma to the anterior capsule in an overhand throwing athlete: a case report. Am J Sports Med. 2003;31(4):617–619. doi:10.1177/03635465030310042401 ↩
- Bui-Mansfield LT, Banks KP, Taylor DC. Humeral avulsion of the glenohumeral ligaments: the HAGL lesion. Am J Sports Med. 2007;35(11):1960–1966. doi:10.1177/0363546507301081 ↩
- Bigliani LU, Pollock RG, Soslowsky LJ, Flatow EL, Pawluk RJ, Mow VC. Tensile properties of the inferior glenohumeral ligament. J Orthop Res. 1992;10(2):187–197. doi:10.1002/jor.1100100205 ↩
- Maldjian C, Khanna V, Bradley J, Adam R. Evaluation of Contrast Extravasation as a Diagnostic Criterion in the Evaluation of Arthroscopically Proven HAGL/pHAGL Lesions. Radiol Res Pract. 2014;2014283575. doi:10.1155/2014/283575 ↩
- Wang W, Huang BK, Sharp M, Wan L, Shojaeiadib N, Du J, et al. MR Arthrogram Features That Can Be Used to Distinguish Between True Inferior Glenohumeral Ligament Complex Tears and Iatrogenic Extravasation. AJR Am J Roentgenol. 2019;212(2):411–417. doi:10.2214/ajr.18.20090 ↩
- Seroyer ST, Nho SJ, Bach BR, Jr., Bush-Joseph CA, Nicholson GP, Romeo AA. Shoulder pain in the overhead throwing athlete. Sports Health. 2009;1(2):108–120. doi:10.1177/1941738108331199 ↩
- Polster JM, Lynch TS, Bullen JA, Soloff L, Ilaslan H, Subhas N, et al. Throwing-related injuries of the subscapularis in professional baseball players. Skeletal Radiol. 2016;45(1):41–47. doi:10.1007/s00256-015-2239-9 ↩
- Nelson C, Reiter C, Cyrus J, Satalich J, O’Connell R, Vap A. Indications, management, and outcomes of humeral avulsions of the glenohumeral ligament: a systematic review. Orthop Rev (Pavia). 2022;14(3):37830. doi:10.52965/001c.37830 ↩
- Fritz EM, Pogorzelski J, Hussain ZB, Godin JA, Millett PJ. Arthroscopic Repair of Humeral Avulsion of the Glenohumeral Ligament Lesion. Arthrosc Tech. 2017;6(4):e1195–e1200. doi:10.1016/j.eats.2017.04.008 ↩
- Parameswaran AD, Provencher MT, Bach BR, Jr., Verma N, Romeo AA. Humeral avulsion of the glenohumeral ligament: injury pattern and arthroscopic repair techniques. Orthopedics. 2008;31(8):773–779. doi:10.3928/01477447-20080801-21 ↩
