Clinical History: A 15-year-old female presents with knee pain following a sports injury nine days prior. What is the acute finding? What is the underlying condition that supports the acute finding?

1a

1b

1c
Figure 1:
Successive axial proton-density fat-saturated MR images through the superior aspect of the patellofemoral joint.
Findings

2a

2b

2c
Figure 2:
Successive axial proton-density fat-saturated MR images through the proximal portion of the trochlea (beginning with the most superior axial section displaying trochlear cartilage) demonstrate edema at both the patellar and femoral attachments of the medial patellofemoral ligament (arrowheads), raising the possibility of a recent lateral patellar subluxation or dislocation. Supporting this diagnosis is the presence of an abnormally shallow trochlea, predisposing to lateral patellar subluxation or dislocation.
Diagnosis
Partial tear of the medial patellofemoral ligament, presumably from recent lateral subluxation or dislocation, in the setting of trochlear dysplasia.
Introduction
Trochlear dysplasia refers to a pathologic alteration in the shape of the femoral trochlea. Whereas a normal trochlea (also known as facies patellaris, intercondylar groove, or intercondylar sulcus) is sufficiently concave to guide and retain the patella throughout the normal range of movement, a dysplastic trochlea may be shallower than normal or even flat or convex, thus predisposing the patella to lateral subluxation or even dislocation.

3a
Figure 3:
In this more severe case of trochlear dysplasia, there has been recent lateral dislocation of the patella, with clear disruption of the medial patellar retinaculum and extensive surrounding fluid and edema. There are bone contusions involving the lateral aspect of the lateral femoral condyle and the medial aspect of the patella.
The study of trochlear dysplasia can be daunting, first because it deals with a three-dimensional surface whose biomechanics may not be self-evident. Second, in an attempt to quantify the complexities of this surface, researchers over the years have created a large number of metrics that may be difficult to remember. Finally, different authors have employed metrics that initially may seem identical but are not, related to variations in methodology that can significantly affect results.
To avoid compounding these challenges, this MRI Web Clinic does not delve deeply into other factors which may contribute to patellar instability, including patellofemoral congruence (i.e. tilt and lateral subluxation), tibial tuberosity–trochlear groove distance (with Q angle), and patella alta. Each of these is a topic of extensive research that has resulted in multiple measurements. A previous MRI Web Clinic (August 2010) has already addressed the many methodologies for quantifying patellar height.
To provide a proper background and context for the MRI evaluation of trochlear dysplasia, we will first establish the basic physiology necessary for understanding trochlear dysplasia and discuss how this condition was studied before the application of MRI. Moderate emphasis will be placed on the predominant classification system in current use—the Dejour classification.
Importance of the Proximal Trochlea
When the human knee is fully extended, especially if the quadriceps muscle is contracted, the patella does not articulate with the femoral trochlea; instead, it lies just superolateral to the most superior portion of the trochlea. On every cycle of knee flexion, at approximately 10° of flexion, the patella moves downward from this position to enter the trochlea.1
The most proximal extent of the trochlea (the portion encountered by the patella in early flexion) is the shallowest and therefore offers the least stability to the patella. While articulating with this portion of the trochlea, the patella is most susceptible to dislocation. Thus, even small abnormalities of this portion of the trochlea have a profound effect on patellar stability. As a corollary, it is for this reason that patellar dislocation often occurs in the presence of patella alta; compared to a normal patella, a patella that is superiorly located articulates with the proximal shallow portion of the trochlea for a longer time, with an increased risk for patellar dislocation.
As the patella moves distally with increasing flexion of the knee, the trochlear floor deepens and provides increased patellar stability. Thus, it is rare for the patella to dislocate from the distal, or more inferior, portions of the trochlear groove. Consequently, any trochlear measurements that are relevant to patellar stability must be made proximally, that is, in the early stages of knee flexion.1

4a

4b

4c
Figure 4:
Simplified schematics of patellar tracking. In these schematics, the curved femoral condyles are flattened into a planar surface. In a normal trochlea (a), the patella (sphere), guided by forces from the quadriceps tendon, patellar tendon, and medial and lateral supporting structures (red arrows), begins each cycle of knee flexion by entering the shallowest, most proximal portion of the trochlea (upper portion of diagram). In a dysplastic trochlea, the crucial proximal extent of the trochlea may be (b) flat or (c) convex, predisposing to patellar dislocation. Other factors contributing to patellar instability can similarly be conceptualized as alterations of the positions and forces illustrated in this figure.
Traditional Assessment of Trochlear Dysplasia
The importance of trochlear dysplasia first came to light in 1802, when the French surgeon Richerand noticed several cases of patellar dislocation in which the lateral femoral condyle was less prominent than usual.2 Early radiographic attempts to assess the morphology of the trochlea employed axial radiographs of the knee. However, the earliest techniques for axial radiography, starting with Settegast in 1921, were accomplished with the knee in deep flexion, a position that did not allow assessment of the crucial proximal portion of the trochlea.2,3 In the ensuing decades, authors proposed new techniques to study more proximal portions of the trochlea, culminating in the two early-flexion axial techniques that are used today, those of Merchant in 1974 (45° flexion; Figure 5a) and Laurin in 1978 (20° flexion; Figure 5b).4 ,5 With these views, trochlear morphology was gauged using measurements such as the sulcus angle, lateral inclination angle, and condylar heights2,6—metrics that would later be used in conjunction with cross-sectional imaging.

5a

5b
Figure 5:
Techniques for axial radiography of the knee. When performed in shallow flexion, axial views of the knee can profile the proximal portion of the trochlea. (a) The Merchant view is taken with the knee in 45° of flexion, with the beam passing toward the patient's feet. (b) The Laurin view is taken with the knee in 20° of flexion, with the beam passing toward the patient's head. Although these views are useful, the use of axial radiographs to evaluate portions of the trochlea that are even further proximal is prohibited by physical constraints, such as the soft tissues of the thigh.
In the 1980s, Malghem and other investigators7,8 began to turn their interest away from axial radiographs in favor of lateral radiographs (Figure 6); this method set the stage for the Dejour classification system that is used today. The medical literature that relates to the “Dejour system,” however, may initially seem contradictory until it is recognized that the name Dejour applies to two separate classification systems that were developed by two separate French orthopaedic surgeons from the Lyon School of Knee Surgery: Henri Dejour, the late father, and David Henri Dejour, his son.

6a
Figure 6:
Schematic of a true lateral radiograph. Acquisition of axial images is limited with regard to the proximal extent of the trochlea that can be profiled. The lateral radiograph, however, allows the assessment of the entire trochlear floor (blue), proximal to distal, in a single image. Medial (green) and lateral (red) aspects of the knee can be distinguished by means of several characteristics labeled on the schematic.
In the late 1980s and early 1990s, Henri Dejour and his coworkers9 conducted a number of landmark studies identifying radiologic and anatomic characteristics of the knee in patients who had previously experienced one or more patellar dislocations. They identified four factors with statistical significance, still widely accepted as the primary contributors to patellar instability:
- Trochlear dysplasia (present in 85% of abnormal cases)
- Quadriceps dysplasia/patellar tilt (present in 83% of abnormal cases)
- Patella alta (present in 24% of abnormal cases)
- Tibial tuberosity–trochlear groove distance (increased in 56% of abnormal cases)
These four factors would subsequently form the basis for the Lyon School’s surgical strategy of “le menu à la carte”, in which each predisposing abnormality is corrected through its own operative technique. According to this strategy, a patient would receive individualized treatment suited to his situation, much like a diner might receive individual dinner items suited to his tastes.10
During the same series of investigations, working exclusively with true lateral radiographs, Henri Dejour et al.9 distilled trochlear dysplasia into three primary concepts:
- Crossing sign (present in 96% of abnormal cases). The most fundamental sign of trochlear dysplasia, the crossing sign is positive when the contours of the trochlear floor and of the lateral femoral condyle intersect at any level. This indicates that, at that level, the lateral side of the trochlea is flat or, equivalently, the trochlear floor is flush with the lateral condyle.
- Trochlear depth (shallow in 85% of abnormal cases). The trochlear depth is measured at a location in the proximal aspect of the trochlea that requires the construction of multiple lines (Figure 7a). Henri Dejour et al. considered this measurement to be pathologic at a value of 4 mm or less.
- Trochlear bump (present in 66% of abnormal cases). Not to be confused with the trochlear spur (discussed below), the trochlear bump measurement assesses the most anterior extent of the trochlear floor, measured relative to a line drawn along the most distal 10 cm of the anterior cortex of the femoral diaphysis (Figure7b). Protrusion of the trochlear floor anterior to this line is denoted with a positive value. Henri Dejour et al. considered this measurement to be pathologic at a value of +3 mm or greater.

7a

7b
Figure 7:
Trochlear measurements (methodology of Henri Dejour et al.). (a) The trochlear depth is measured from the true lateral radiograph at a location in the proximal aspect of the trochlea that requires the construction of multiple lines. First, a "vertical" line is drawn along the posterior cortex of the femoral diaphysis (dotted green line). Next, perpendicular to this line, a second "horizontal" line (dashed green line) is drawn at the vertical level of the most proximal point of the posterior contour of the femoral condyles (blue arrow), the inflection point where the concavity of the femoral metaphysis gives way to the convexity of the posterior femoral condyles. From the intersection of the first two lines, a third line is drawn anteroinferiorly, angled 15° from the "horizontal" line (solid green line). It is along this line that the distance between the osseous trochlear floor and lateral condyle is measured (red line). (b) The trochlear bump measurement assesses the most anterior extent of the trochlear floor, measured (red line) relative to a line (green line) drawn along the most distal 10 cm of the anterior cortex of the femoral diaphysis.
Henri Dejour et al.9 also discussed a few ancillary concepts:
- Trochlear beak/spur. Introduced initially only as an incidental note, the (supra)trochlear beak, or spur, refers to an angular projection of the most proximal portion of the trochlea.
- Trochlear angle (shallow in 65% of abnormal cases). The trochlear angle refers to the opening angle of the trochlea as visualized on a 30° flexion axial radiograph. In the study of Henri Dejour et al., a threshold of 145° successfully excluded all normal patients. However, this cutoff value allowed the identification of only 65% of cases of patellar instability (high specificity, low sensitivity), implying that the trochlear abnormality in many patients was located even more superiorly than the portion of the trochlea profiled in a 30° flexion view.
- Double contour sign. The double contour sign indicates that the contour of the medial femoral condyle is significantly smaller than that of the lateral femoral condyle.
Based on the location of the crossing sign and the presence or absence of the double contour sign, Henri Dejour et al.9 divided dysplastic trochleae into three types: I, II, and III. Unfortunately, a subsequent study by Rémy et al.11 in 1998 found that the system was poorly reproducible. Hence, in the same year, the same fundamental signs were reused by David Dejour et al.12,13 to create a revised system. This revision was found to be more reproducible and has generally supplanted its predecessor.14 Radiologists and clinicians should be aware that these two different systems exist and, for example, a “Type III dysplasia” (of H. Dejour) is not at all identical to a “Type C dysplasia” (of D. Dejour).
David Dejour et al.12,13,15 made several modifications to the work of Henri Dejour et al. First, these investigators elevated the status of the trochlear spur, promoting what was initially considered an ancillary finding to one of the three major discriminating signs of trochlear dysplasia. Second, they also de-emphasized quantitative measurements, such as the trochlear bump. Finally, despite his father’s pronouncement9 that CT “does not permit a repetitively reliable study of the trochlea,” David Dejour with his coworkers sought to correlate the four new types of dysplasia (as judged by lateral radiographs) with their appearances on axial CT scans or MRI images at a specific trochlear level (the most superior image demonstrating trochlear cartilage) (Figure 8).

8a

8a

8a

8a
Figure 8:
The David Dejour classification. All four types, starting with the mildest David Dejour Type A, exhibit the positive crossing sign. (a) In a David Dejour Type A trochlea, only this one sign, the crossing sign, is present. When Type A trochleae are examined by axial CT at the reference level, they appear shallow, but not flat. Although the presence of a crossing sign in Type A dysplasia indicates that the trochlea is indeed flat at one level, the location of the flatness is typically proximal to the axial section that is used as a reference. (b) In Type B, there is an additional trochlear spur. On axial images these trochleae appear flat. (c) In Type C, there is no trochlear spur, but instead, there is a double contour sign. On axial images, these trochleae appear convex, with a hypoplastic medial condyle. (d) In Type D all three signs are present: the double contour sign, the crossing sign, and the trochlear spur. On axial images, these trochleae have a sharp convex "cliff" separating the medial and lateral facets.
The four trochlear types of David Dejour et al. are summarized, with comparison to the three types of Henri Dejour et al., in Table 1.
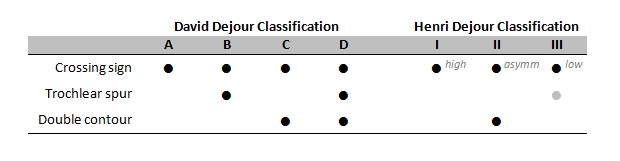
Table 1. Comparison of the classifications of David and Henri Dejour. In the Henri Dejour classification system, dysplastic trochleae were classified by the proximodistal level of the crossing sign: high, asymmetric, or low. In trochleae with a low (distal) crossing sign, a trochlear spur was not consistently observed; hence, spurs were considered an ancillary finding and irrelevant to the classification of dysplastic trochleae. In the subsequent David Dejour classification, the trochlear spur was promoted to one of the three major discriminating signs of trochlear dysplasia.
MRI Assessment of Trochlear Dysplasia
In 2000, remarking that true lateral radiographs are rare and, also, that patients routinely undergo MRI examinations without comparison radiographs, the Swiss radiologist Pfirrmann and his coworkers16 published one of the earliest sets of criteria for diagnosing trochlear dysplasia by MRI. Pfirrmann et al. studied which MRI criteria allowed the most reliable diagnosis of trochlear dysplasia according to the gold standard provided by the Henri Dejour criteria. Patients were included in the study group if and only if their lateral radiographs demonstrated all three primary Henri Dejour criteria. Subsequent authors have generally preferred to select their study groups according to clinical and not radiological criteria. The methodologies and results of various other investigations—Carrillon et al.,17 Escala et al.,18 van Huyssteen et al.,19 Biedert et al,20 Ali et al.,21 Salzmann et al,22 and Charles et al.23—are compared in Table 2.
MRI investigations typically rely on a limited number of observations using a mid-sagittal image, defined as the image that best depicts the trochlear floor. The analysis of Pfirrmann et al.16 included the following:
- Ventral trochlear prominence. This metric is analogous to Henri Dejour’s “trochlear bump,” except that it is the cartilaginous (and not the osseous) floor of the trochlea that is measured. Adopting a threshold of 8 mm yielded a sensitivity of 75% and a specificity of 83% for identifying patients in the study group, that is, patients whose lateral radiographs demonstrated all three primary Henri Dejour criteria. (For comparison, Henri Dejour et al.9 had previously established an osseous measurement of 3 mm.) Several other authors18,21 also used a similar metric.
- Nipple height. This metric assesses the prominence of the Dejour (supra)trochlear spur, if such a spur is present. The reference for this measurement is not the distal diaphyseal cortex (as is the case for ventral trochlear prominence), but the subchondral bone of the proximal trochlea immediately distal to the spur. This measurement is not commonly studied; it does not appear in any of the other MRI investigations reviewed in this MRI Web Clinic.
As in most MRI investigations, the majority of the data of Pfirrmann et al.16 is collected not from sagittal images, but from axial images. For such axial images, selecting an accurate and reproducible reference level is a decision of prime importance. Although Pfirrmann et al. identified some statistically significant results 1 cm and 2 cm above the femorotibial joint line, they recommended the axial image that yielded the best discrimination between normal and dysplastic trochleae, one that is located 3 cm above the joint line. The use of such an absolute measurement is unusual. Although the 3 cm reference image localizes roughly to the proximal aspect of the trochlea, the exact level varies in knees of different sizes. Subsequent authors have preferred anatomic landmarks that are adaptable to knees of different sizes, such as the first axial image that displays any trochlear cartilage,17 the first axial image that displays full chondral coverage of the trochlea,18,19,20,22,23 the axial image that contains the greatest ventral trochlear prominence,21 or the axial image with the most symmetrical “Roman arch” appearance of the posterior intercondylar fossa.18
In the study of Pfirrmann et al.,16 two axial measurements achieved statistical significance:
- Facet asymmetry. A concept adapted from axial radiographs, facet asymmetry indicates the ratio of facet lengths, medial to lateral (Figure 9). Adopting a threshold of 40% yielded a sensitivity of 100% and a specificity of 96% for identifying patients in their study group. A similar metric was reported by Charles et al.,23 but with this ratio inverted

9a

9b
Figure 9:
Facet asymmetry. Facet asymmetry indicates the ratio of facet lengths. (a) Pfirrmann et al. reported this value as the medial facet measurement (red) divided by the lateral facet measurement (blue); Charles et al. instead reported the reciprocal (lateral divided by medial). (b) Applying the measurement of Pfirrmann et al. to the appropriate cross-section of our introductory case yields a ratio of 39%, which is abnormally small.
- Trochlear depth. For this popular metric, Pfirrmann et al. employed a somewhat uncommon methodology. First, the tangent to the posterior aspect of both condyles is drawn as a reference baseline. Perpendicular to this baseline, measurements are made to the most anterior points of the medial and lateral facets, as well as to the trochlear floor. To compute the final metric, the floor measurement is subtracted from the average of the two facet measurements (Figure 10). Adopting a threshold of 3 mm yielded a sensitivity of 100% and a specificity of 96% for identifying patients in the study group. (For comparison, Henri Dejour et al.9 had previously established an osseous threshold of 4 mm.) Other authors’ methodologies are mentioned below.

10a

10b
Figure 10:
Trochlear depth (methodology of Pfirrmann et al.). (a) To make this measurement, the tangent to the posterior aspect of both condyles (green line) is first drawn as a reference baseline. Perpendicular to this baseline, measurements are made to the most anterior points of the medial and lateral facets (red lines), as well as to the trochlear floor (blue line). To compute the final metric, the floor measurement is subtracted from the average of the two facet measurements. The average of the two facet measurements may be interpreted as the length of a line parallel to and equidistant from the two facet measurements (red dotted line). (b) Applying these measurements to the appropriate cross-section of our introductory case yields a trochlear depth of (61.3+63.6)/2 − 61.0 = 1.4 mm, which is abnormally small.
In practice, attempts to use the trochlear depth threshold of Pfirrmann et al16 are often erroneous for two reasons.
- First, the measurement should be made relative to the cartilaginous (not osseous) surface of the trochlea. Pfirrmann et al. emphasized that their MRI methodology was meant to assess the real geometry of the joint. Incorrectly choosing the osseous contour overestimates the trochlear depth and therefore leads to underdiagnosis of trochlear dysplasia. Most subsequent MRI studies18,23 were based similarly on the true cartilaginous contour.
- Second, the methodology of Pfirrmann et al. is often simplified into a model that is not mathematically equivalent. In this simplified variant, the most anterior points of the medial and lateral facets are connected with a line, and from this line a measurement line is extended to the floor of the trochlea (Figure 11a,b). This variant is mathematically equivalent to the original methodology only if (1) the floor of the trochlea is positioned exactly halfway between the anterior points (red dotted line in Figure 10) and (2) the final measurement is made perpendicular to the posterior baseline. Other authors such as Ali et al.21 and Charles et al.,23 however, have adopted this simpler technique as their official methodology. Using yet another methodology, Escala et al.18 calculated the trochlear depth as a purely anteroposterior measurement relative to the most anterior aspect of the lateral facet (Figure 11c,d), a methodology that is theoretically most analogous to a measurement derived from a lateral radiograph.

11a

11b

11c

11d
Figure 11:
Alternative methodologies for measuring trochlear depth. (a) In the methodology of Ali et al., the most anterior points of the medial and lateral facets are connected with a line (green line), and from this line a perpendicular measurement line (red line) is extended to the floor of the trochlea. Ali et al. used the subchondral bony contour, while Charles et al. used the cartilaginous contour. (b) Applying the cartilaginous measurement of Charles et al. to the appropriate cross-section of our introductory case yields a measurement of 0.7 mm, which is abnormally small. The measurement of Ali et al. at its appropriate cross-section is also abnormal (not depicted). (c) Escala et al. calculated the trochlear depth as a purely anteroposterior measurement (red line) relative to the most anterior aspect of the lateral facet (uppermost green line). (d) Applying the measurement of Escala et al. to the appropriate cross-section of our introductory case yields a measurement of 63.6−61.0 = 2.6 mm, which is abnormally small.
In subsequent years, other authors have described additional measurements that can be made on axial MRI scans.
- Carrillon et al.17 (2000) validated an MRI version of lateral trochlear inclination. Originally employed on axial radiographs,6 this metric aims to detect the reduced prominence of a dysplastic lateral condyle by the abnormally shallow slope of its lateral trochlear facet. With Carrillon’s methodology, on the most superior axial slice containing any trochlear cartilage, both the lateral trochlear line and the posterior condylar reference line are drawn with respect only to the subchondral bone (not to the cartilage); the angle between the lines is measured (Figure 12). Carrillon et al. proposed a diagnosis of trochlear dysplasia when the angle measures 11° or less.

12a

12b
Figure 12:
Lateral trochlear inclination. (a) Both the lateral trochlear line (red) and the posterior condylar reference line (green) are drawn with respect only to the subchondral bone (not to the cartilage); the angle between the lines is measured. (b) Applying the measurement of Carrillon et al. to the appropriate cross-section of our introductory case yields a measurement of 9-10°, which is abnormally small.
- Biedert and Bachmann20 (2009) studied the anterior extent of the femoral condyles, which they termed anterior–posterior trochlear measurements, with respect to the posterior condylar reference line. With their methodology, on the most superior axial image with complete trochlear cartilage coverage, the posterior condylar reference line is drawn tangent to the subchondral bone; the anterior measurements, however, take into account the cartilaginous contour of the trochlea (Figure 13). Using these data, Biedert and Bachmann attempted to answer whether the reduced prominence of the lateral facet in trochlear dysplasia originates from depression of the lateral facet or elevation of the trochlear floor. Though their results suggested both types exist, the overwhelming majority of cases appeared to have an elevation of the floor. This conclusion agrees with the observation of Henri Dejour et al9 that an increased “trochlear bump” is present in most cases of trochlear dysplasia. Other studies, however, have not confirmed this result.16,18,23

13a
Figure 13:
Anterior–posterior trochlear measurements. The anterior extent of the femoral condyles and also of the trochlear floor (three red lines) is measured with respect to the posterior condylar reference line (green).
Some of the most common MRI metrics are compared in Table 2. It is crucial to note the reference level at which different authors’ axial measurements have been validated, as well as other methodological details (e.g. selection of the cartilaginous or osseous contour).
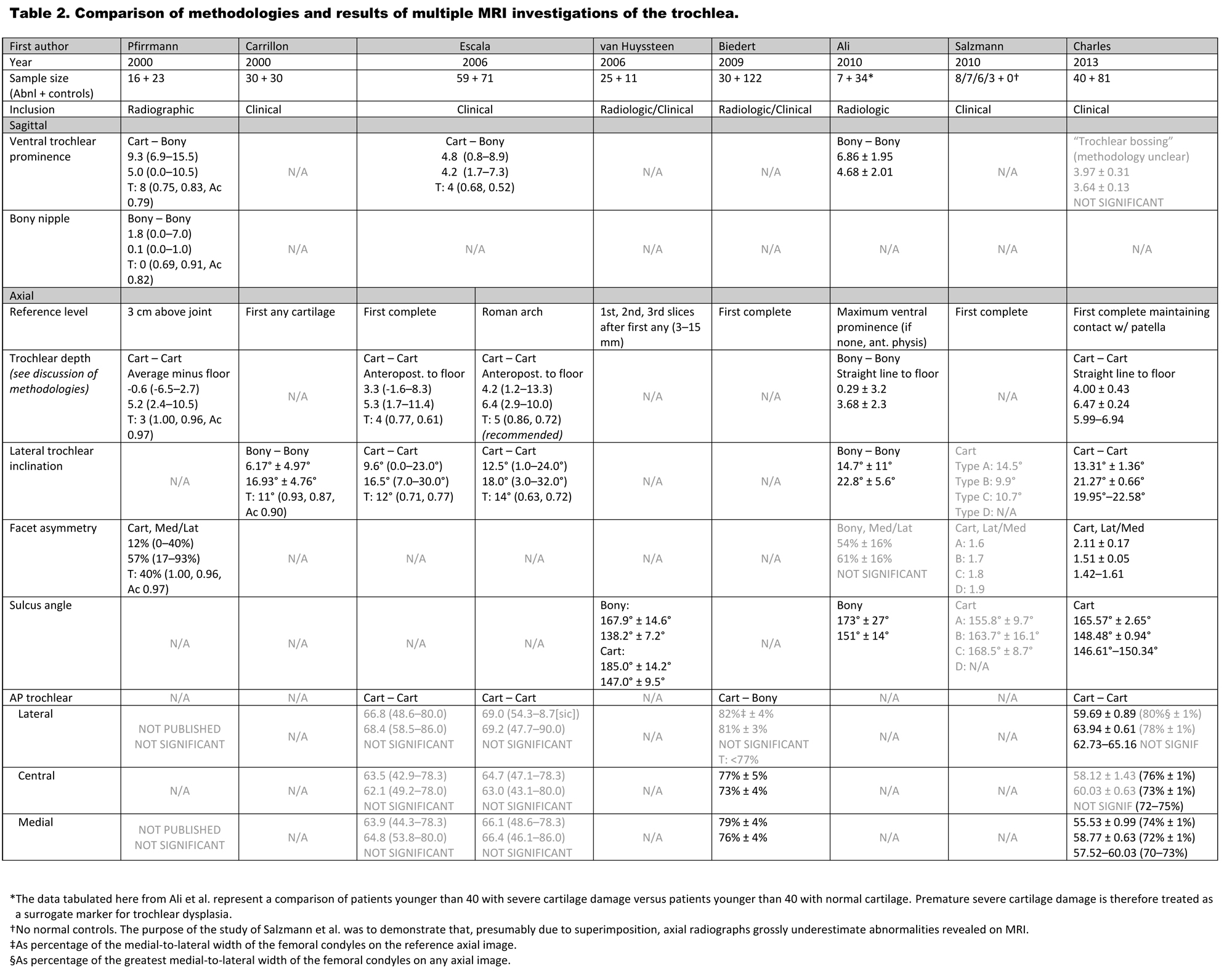
Table 2. Lines in each measurement entry represent the following: abbreviated methodology (including choice of cartilaginous or subchondral bony contour); pathologic mean ± standard deviation (or range if unavailable); normal mean ± SD (or range if unavailable); T: published threshold (with sensitivity, specificity, and other measures) or 95% confidence interval of normal, if any. Values are in mm unless otherwise specified. If a metric is reported as “NOT SIGNIFICANT,” usually no further information is given. Entries in gray denote results that are not significant or not applicable.
Characteristics of the Ideal Metric
The above methodologies have various strengths and weaknesses when compared to what we believe are characteristics of an ideal metric of trochlear morphology:
- Use of cartilaginous contour. An ideal MRI metric should assess the true geometry of the femoral trochlea, that is, its cartilaginous contour. Because the cartilaginous contour of the trochlea differs significantly from its osseous contour,19 measurements based on these bone contours are valuable primarily for correlation with historical studies in which measurements were derived from axial radiographs or CT scans. Otherwise, osseous measurements such as the lateral trochlear inclination of Carrillon et al.17 should be avoided.
- Simplicity. The ideal measurement should be simple, involving as little drawing and measuring as is feasible, with convenient numerical thresholds. In this respect, measurements such as anterior–posterior trochlear measurements—which require drawing at least four lines, then making three measurements, each with its own 95% confidence interval—face an uphill battle in gaining clinical acceptance.
- Use of reproducible, accurate reference level. It is sometimes difficult to identify the cross-section at which trochlear cartilage coverage first transitions from partial to complete or when the best “Roman arch” is seen. Of the landmark-based reference levels, therefore, the most reproducible level seems to be the most proximal image that displays any trochlear cartilage. However, while it seems logical to choose a reference image that is adaptable to knees of different sizes, it is not certain that the current landmark-based reference levels are necessarily more accurate than the absolute offset of Pfirrmann et al.16 (3 cm above the joint line). It is conceivable that trochlear dysplasia may alter not only the contour of the trochlea but also the craniocaudal level at which cartilage coverage begins. For optimal functional analysis of patellar tracking, we speculate whether even more accurate results might be obtained by using a reference level related to the craniocaudal level of the patella in full knee extension.
- Theoretical soundness. In the absence of prior surgical overcorrection, it is very rare for the patella to dislocate medially.1 The use of the medial femoral condyle was helpful in studies based on axial radiography, in which it was impractical to establish a posterior condylar reference line.2,5,22 When cross-sectional images are available, however, continued analysis of the medial condyle may introduce unnecessary complexity and variability into determining the likelihood of lateral patellar dislocation. This rationale would argue against measurements such as the trochlear depths of Pfirrmann et al.,16 Ali et al.,21 or Charles et al.23 or the sulcus angle, instead arguing in favor of measurements such as lateral trochlear inclination or the trochlear depth of Escala et al.18
Lateral or Axial? Qualitative or Quantitative?
Though the David Dejour system of trochlear classification remains the most commonly used, it does not describe the trochlea completely. In their criticism of the earlier Henry Dejour classification system, Rémy et al.11 noted that in addition to its poor reproducibility, a description of the trochlea should include, at the very least, a measurement of the trochlear prominence, as it may affect the choice of corrective surgery. In their reassessment of the revised classification of David Dejour, Rémy et al.14 acknowledged an improvement in intra-observer reproducibility, but repeated the criticism that the new classification system still lacked a measure of trochlear depth or prominence.
Moreover, the David Dejour system, with its largely qualitative assessments derived from lateral radiographs, does not seem to reconcile well with qualitative metrics derived primarily from axial MRI images. A 2014 study showed that, of many common metrics (including lateral trochlear inclination, trochlear facet asymmetry, and trochlear groove depth), none correlated well with the four types of David Dejour, and the three metrics specified above correlated better only after types B, C, and D were collapsed into one single “high-grade” category.24 Even a paper from 2012 co-written by David Dejour25 reported that participants reading lateral radiographs were rarely able to assign the same trochlear type as those reading the corresponding MRI images, and that in comparing lateral radiographs and axial MRI, the axial MRI images gave the impression of more severe dysplasia. Again, reproducibility improved only after an aggregate “Dejour B–D” category was created.
Surgical Treatment of Trochlear Dysplasia
Trochlear dysplasia can be corrected using surgery. The earliest operative technique that enjoyed widespread adoption was described in 1915 by Albee,26 who performed a coronally-oriented opening osteotomy of the lateral femoral condyle to steepen the inclination of the lateral trochlea without changing the trochlear floor (Figure 14). This approach seems to disregard the apparent cause of most cases of trochlear dysplasia—namely, that it is the trochlear floor that is too elevated, not the condyles that are too flat. Because the procedure tends to lift the patella further away from the femur, narrowing the angle between the vectors of the quadriceps and patellar tendons, it elevates contact pressures and predisposes to cartilage damage.27

14a
Figure 14:
Albee trochleoplasty. A coronally-oriented opening osteotomy of the lateral femoral condyle is performed to steepen the inclination of the lateral trochlea. Note that in the postsurgical state, the lateral facet of the trochlea is more anterior than that of a normal trochlea (dotted line).
The next major procedure, the deepening trochleoplasty, was described by Masse28 in 1978 and modified by Henri Dejour in 1987.10,13 The preferred surgery of the Lyon School, this procedure involves removing a near full-width coronal slab of cancellous bone from the anterior femur and then bluntly depressing the central trochlear surface into the surgical defect to create the new trochlear floor (Figure 15). A procedure described by Bereiter et al.29 is similar but involves a thinner flap of the trochlear surface.

15a
Figure 15:
Deepening trochleoplasty. A near full-width coronal slab of cancellous bone is removed from the anterior femur, and the central trochlear surface is then bluntly depressed into the surgical defect to create the new trochlear floor. Note that the contour of the postsurgical trochlea roughly approximates that of a normal trochlea (dotted line).
Finally, for those trochleae that contain a prominent bump, Goutallier et al.30 described an operative procedure known as a wedge recession trochleoplasty, in which a wedge of cancellous bone (as seen in the sagittal plane) is removed from the anterior femur, and the superior aspect of the trochlea is tilted posteriorly into the surgical defect to make it flush with the anterior diaphyseal cortex (Figure 16). This procedure has the advantage of tilting but not otherwise distorting the shape of the trochlear groove, preserving any patellofemoral congruence and reducing the procedure’s technical complexity.

16a
Figure 16:
Wedge resection trochleoplasty. A wedge of cancellous bone (as seen in the sagittal plane) is removed from the anterior femur, and the superior aspect of the trochlea is tilted posteriorly into the surgical defect to make it flush with the anterior diaphyseal cortex.
Summary
Radiography (especially lateral) and multiplanar cross-sectional imaging both contribute to a fuller understanding of the anatomic abnormalities that accompany trochlear dysplasia. Careful analysis of lateral radiographs may reveal findings including the crossing sign that support the diagnosis of a dysplastic trochlea. With axial images provided by CT or MRI, trochlear dysplasia can be confirmed in the presence of a variety of abnormal measurements: the lateral trochlear inclination may be decreased, the sulcus angle increased, the lateral facet asymmetrically widened, or the central trochlear anteroposterior measurement increased. Although current methods that attempt to characterize trochlear dysplasia are not without flaws, radiologists can play an important role in identifying risk factors that promote patellar dislocation.
References
- Fulkerson JP. Disorders of the Patellofemoral Joint. 4th ed. Philadelphia, PA: Lippincott, Williams, & Wilkins; 2004. ↩
- Brattström H. Shape of the intercondylar groove normally and in recurrent dislocation of patella: a clinical and X-ray anatomical investigation. Acta Orthop Scand 1964;68(suppl):1–148. ↩
- Settegast H. Typische Röntgenbilder von normalen Menschen. Lehmanns medizinische Atlanten 1921;5:211. German. ↩
- Merchant AC, Mercer RL, Jacobsen RH, Cool CR. Roentgenographic analysis of patellofemoral congruence. J Bone Joint Surg Am. 1974 Oct;56(7):1391–6. ↩
- Laurin CA, Dussault R, Levesque HP. The tangential x-ray investigation of the patellofemoral joint: x-ray technique, diagnostic criteria and their interpretation. Clin Orthop Relat Res. 1979 Oct;(144):16–26. ↩
- Bernageau J, Goutallier D, Larde D, Guérin L. (The obliquity of the external facet of the femoral trochlea.)Encyclop Med Chir. 1981; 30:39–42. French. ↩
- Malghem J, Maldague B. (Profile of the knee. Differential radiologic anatomy of the articular surfaces). J Radiol. 1986 Oct;67(10):725–35. French. ↩
- Malghem J, Maldague B. Depth insufficiency of the proximal trochlear groove on lateral radiographs of the knee: relation to patellar dislocation. Radiology. 1989 Feb;170(2):507–10. ↩
- Dejour H, Walch G, Nove-Josserand L, Guier C. Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc. 1994;2(1):19–26. ↩
- Dejour DH. The patellofemoral joint and its historical roots: the Lyon School of Knee Surgery. Knee Surg Sports Traumatol Arthrosc. 2013 Jul;21(7):1482–94. ↩
- Rémy F, Chantelot C, Fontaine C, Demondion X, Migaud H, Gougeon F. Inter- and intraobserver reproducibility in radiographic diagnosis and classification of femoral trochlear dysplasia. Surg Radiol Anat. 1998;20(4):285–9. ↩
- Dejour D, Reynaud P, Lecoultre B. Douleurs et instabilite rotulienne: Essai de classification. Med Hyg. 1998; 56:1466–1471. ↩
- Dejour D, Saggin P. The sulcus deepening trochleoplasty—the Lyon’s procedure. Int Orthop. 2010 Feb;34(2):311–6. ↩
- Rémy F, Gougeon F, Ala Eddine T, Migaud H, Fontaine C, Duquennoy A. Reproducibility of the new classification of femoral trochlear dysplasia proposed by Dejour: predictive value for severity of femoropatellar instability in 47 knees. Orthopaedic Proceedings (Société Française de Chirurgie Orthopédique et Traumatologique). 2002 Mar;84-B:43. ↩
- Zaffagnini S, Dejour D, Arendt EA, editors. Patellofemoral pain, instability, and arthritis: clinical presentation, imaging, and treatment. Berlin: Springer-Verlag; 2010. ↩
- Pfirrmann CW, Zanetti M, Romero J, Hodler J. Femoral trochlear dysplasia: MR findings. Radiology. 2000 Sep;216(3):858–64. ↩
- Carrillon Y, Abidi H, Dejour D, Fantino O, Moyen B, Tran-Minh VA. Patellar instability: assessment on MR images by measuring the lateral trochlear inclination-initial experience. Radiology. 2000 Aug;216(2):582–5. ↩
- Escala JS, Mellado JM, Olona M, Giné J, Saurí A, Neyret P. Objective patellar instability: MR-based quantitative assessment of potentially associated anatomical features. Knee Surg Sports Traumatol Arthrosc. 2006 Mar;14(3):264–72. ↩
- van Huyssteen AL, Hendrix MR, Barnett AJ, Wakeley CJ, Eldridge JD. Cartilage-bone mismatch in the dysplastic trochlea. An MRI study. J Bone Joint Surg Br. 2006 May;88(5):688–91. ↩
- Biedert RM, Bachmann M. Anterior-posterior trochlear measurements of normal and dysplastic trochlea by axial magnetic resonance imaging. Knee Surg Sports Traumatol Arthrosc. 2009 Oct;17(10):1225–30. ↩
- Ali SA, Helmer R, Terk MR. Analysis of the patellofemoral region on MRI: association of abnormal trochlear morphology with severe cartilage defects. AJR Am J Roentgenol. 2010 Mar;194(3):721–7. ↩
- Salzmann GM, Weber TS, Spang JT, Imhoff AB, Schöttle PB. Comparison of native axial radiographs with axial MR imaging for determination of the trochlear morphology in patients with trochlear dysplasia. Arch Orthop Trauma Surg. 2010 Mar;130(3):335–40. ↩
- Charles MD, Haloman S, Chen L, Ward SR, Fithian D, Afra R. Magnetic resonance imaging-based topographical differences between control and recurrent patellofemoral instability patients. Am J Sports Med. 2013 Feb;41(2):374–84. ↩
- Nelitz M, Lippacher S, Reichel H, Dornacher D. Evaluation of trochlear dysplasia using MRI: correlation between the classification system of Dejour and objective parameters of trochlear dysplasia. Knee Surg Sports Traumatol Arthrosc. 2014 Jan;22(1):120–7. ↩
- Lippacher S, Dejour D, Elsharkawi M, Dornacher D, Ring C, Dreyhaupt J, Reichel H, Nelitz M. Observer agreement on the Dejour trochlear dysplasia classification: a comparison of true lateral radiographs and axial magnetic resonance images. Am J Sports Med. 2012 Apr;40(4):837–43. ↩
- Albee FH. The bone graft wedge in the treatment of habitual dislocation of the patella. Med Rec. 1915;88:257–259. ↩
- Arendt EA, Dejour D. Patella instability: building bridges across the ocean a historic review. Knee Surg Sports Traumatol Arthrosc. 2013 Feb;21(2):279–93. ↩
- Masse Y. (Trochleoplasty. Restoration of the intercondylar groove in subluxations and dislocations of the patella). Rev Chir Orthop Reparatrice Appar Mot. 1978 Jan-Feb;64(1):3–17. French. ↩
- Bereiter H, Gautier E. (Trochleoplasty as surgical approach for the treatment of recurrent patella instability in patients with trochlear dysplasia of the femur.) Arthroskopie. 1994;7:281–286. German. ↩
- Goutallier D, Raou D, Van Driessche S. (Retro-trochlear wedge reduction trochleoplasty for the treatment of painful patella syndrome with protruding trochleae. Technical note and early results). Rev Chir Orthop Reparatrice Appar Mot. 2002 Nov;88(7):678–85. French. ↩
