Clinical History
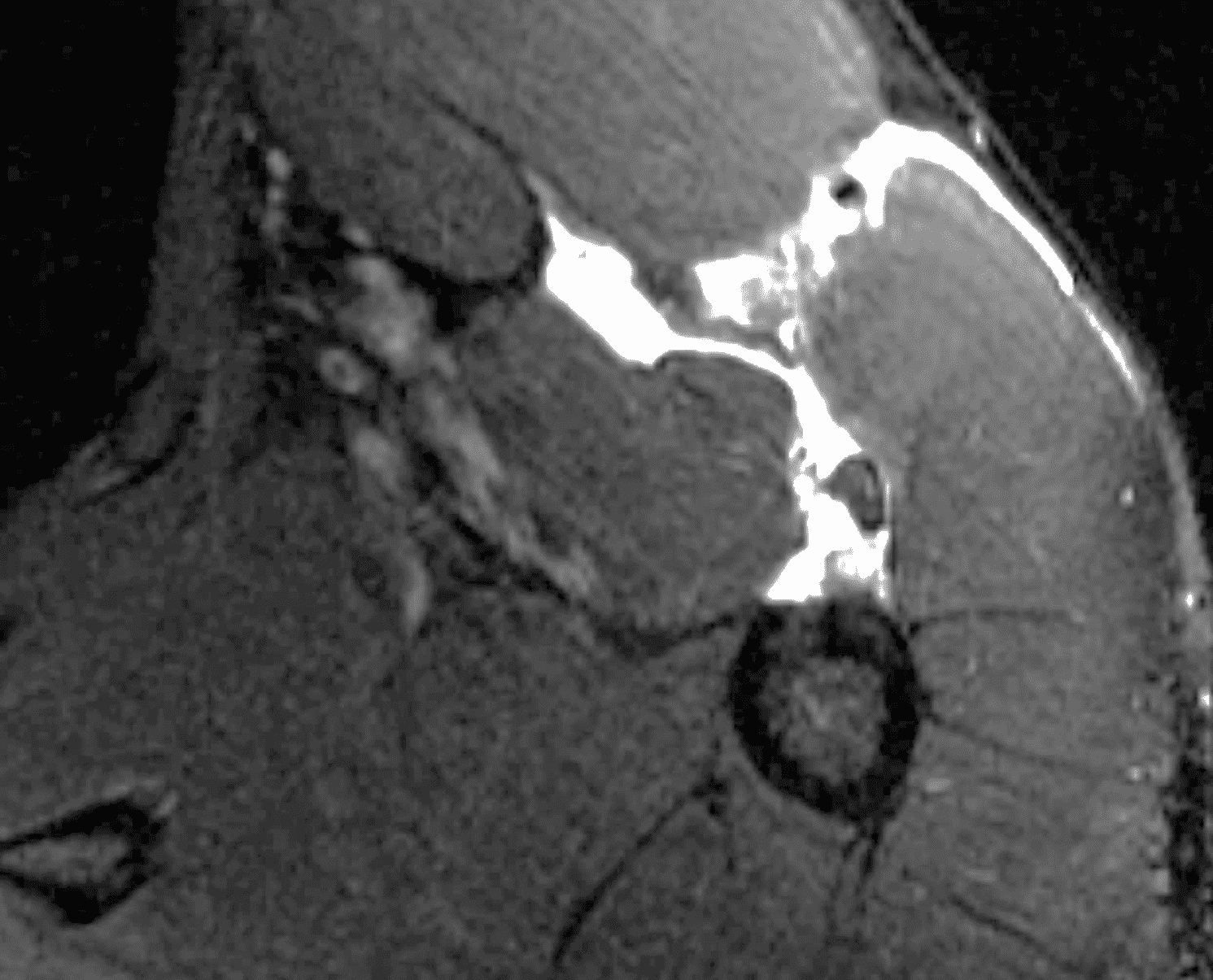
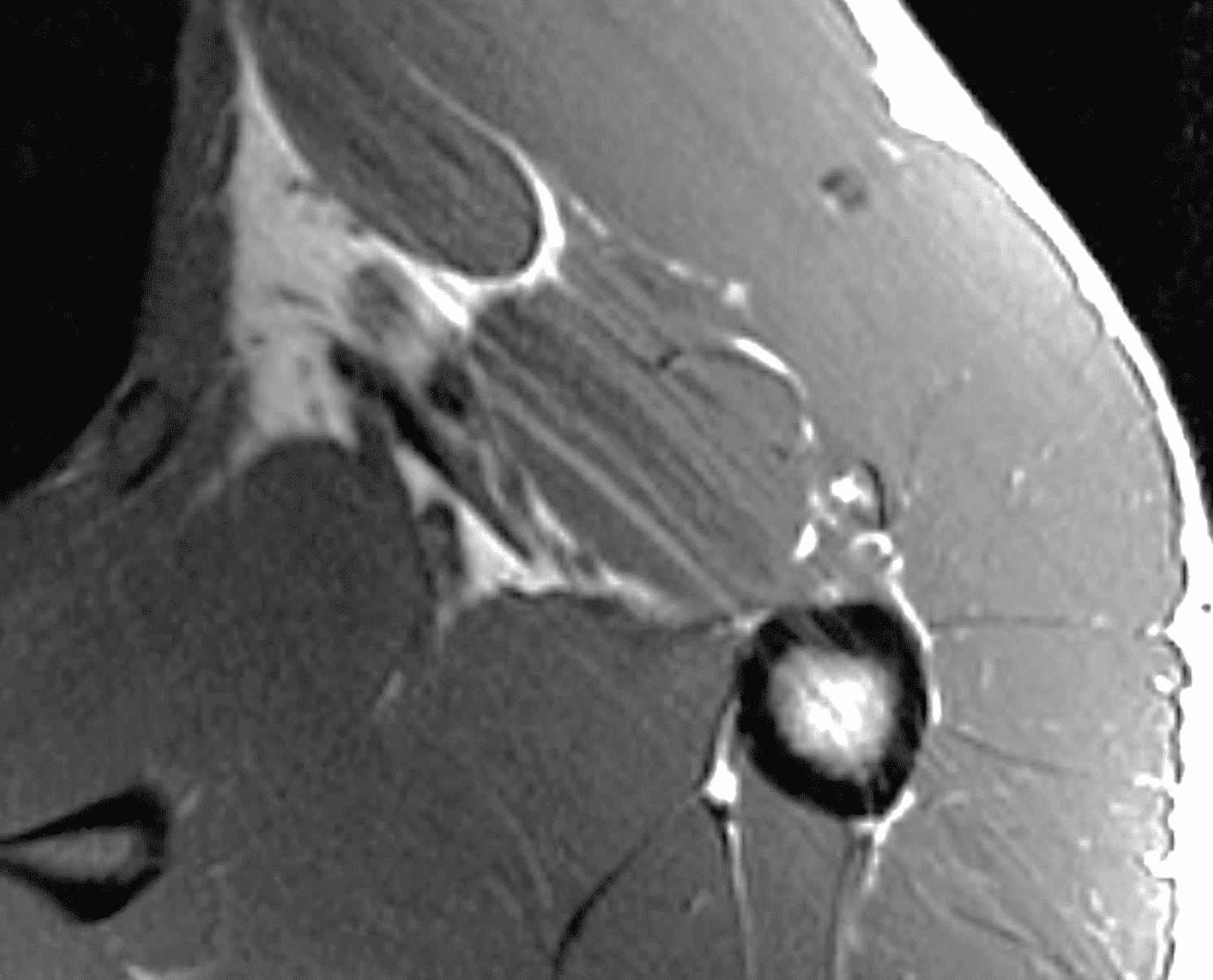
A 36-year-old male developed abrupt onset chest wall pain while bench pressing. Axial (1A) fat-suppressed T2-weighted, and (1B) T1-weighted images as well as a clinical photograph (1C) are provided. What are the findings? What is your diagnosis?

Findings
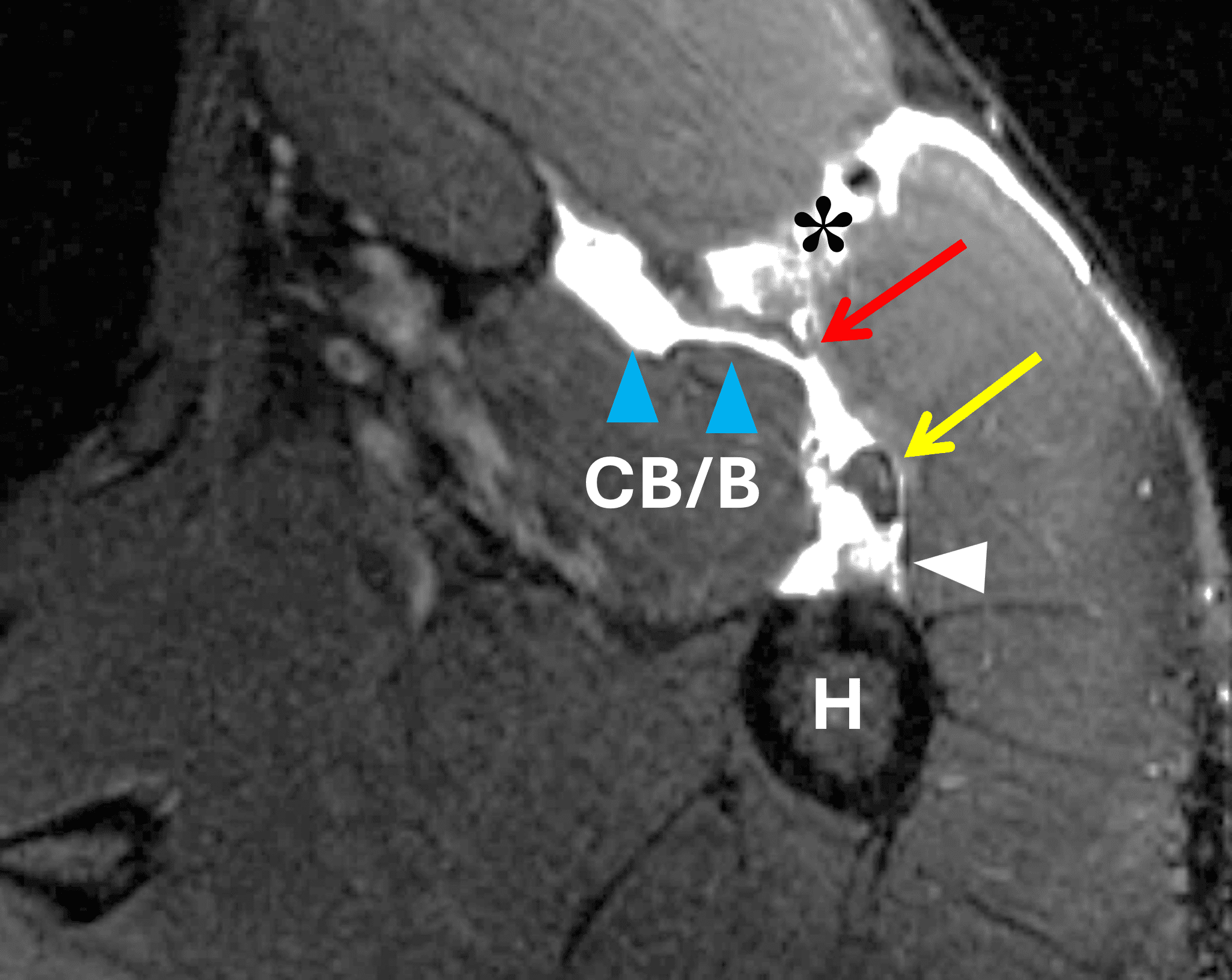


Figure 2: Complete pectoralis major tendon avulsion. H = humeral shaft, CB/B = coracobrachialis & short head biceps muscles. (2A) The long head biceps tendon (yellow arrow) is displaced anteriorly with high-signal intensity fluid (white arrowhead) anterior to the humerus. The torn pectoralis major tendon (red arrow) is retracted medially. Fluid along the anterior margin of the coracobrachialis muscle (blue arrowheads) contributes to the “smoke sign.” Edema and hemorrhage are present in the deltopectoral groove (asterisk). (2B) No intact tendon is visible at the humeral shaft (white arrow). (2C) Ecchymosis is visible in the anterior axilla corresponding to the edema in the deltopectoral groove in 2A. Bruising also extends down the proximal arm overlying the pectoralis tendon insertion site. A complete tendon avulsion was identified and repaired at surgery.
Diagnosis
Full-thickness, complete-width pectoralis major tendon tear at the humeral insertion.
Introduction
Prior to the twenty-first century, intricate knowledge of pectoralis major (PM) anatomy, biomechanics and tear patterns was limited by the low prevalence of injury in the general population. Injuries were typically associated with work or trauma-related mechanisms leading to tendon avulsions at the humeral attachment.1,2 In contrast, over the past quarter century, recreational and professional weightlifting has led to an increased number of partial tears at the myotendinous (MT) junction.3 Standardization of clinical evaluation, imaging interpretation and surgical classification has developed with the pectoralis muscle index, various primary and secondary imaging signs, and detailed surgical classification schemes. Treatment options for both acute and chronic tears are increasingly tailored to patient age and activity.4 Interpreting MR studies of PM injuries can be challenging due to the difficulty of resolving small anatomic structures in the setting of large, muscular patients and soft tissue edema. The aim of this Web Clinic is to provide an update on the primary and secondary MRI signs of PM injuries that help guide treatment decisions.
Anatomy and Function
The PM is a large, fan-shaped, multipennate muscle composed of clavicular, sternocostal and abdominal heads (Figure 3). The muscle has a broad origin from the clavicle, sternum, costal cartilages 1-6 and aponeurosis of the external oblique muscle.4 The sternocostal head (SH) is composed of 7 segments and analogous to an unfolded, articulated hand fan, with the superior muscle segments lying anterior to the more inferior segments (Figure 5).5 The deltopectoral groove, containing the cephalic vein, marks the border between the anterior deltoid muscle and the clavicular head (CH) of the pectoralis muscle, and is an important landmark during surgical exploration. A rare accessory head called the chondrocoracoideus muscle originates from the PM lateral border, runs deep to the PM tendon humeral insertion and joins the short of biceps tendon at the coracoid process, and is potentially a source of neurogenic thoracic outlet syndrome.6 Additional rare but recognized local muscle anomalies include unilateral congenital absence or hypoplasia of the PM major muscle (typically as a part of Poland syndrome), the sternalis muscle and the chondroepitochlearis muscle.7 The pectoralis minor muscle runs deep to the PM, originating from the ribs and inserting on the medial margin of the coracoid process.7 The SH seventh sternal segment is equated to the abdominal head by some authors.8 The CH is a single segment arising from the anterior margin of the medial clavicle. Cadaveric studies report a mean muscle fiber length of 15.0 cm +/- 0.8 cm for the CH, and 16.4 cm +/- 1.2 cm for the SH.3 The difference in muscle fiber length and pennation angle may influence the location of injury during specific activities or injury mechanisms.9,10
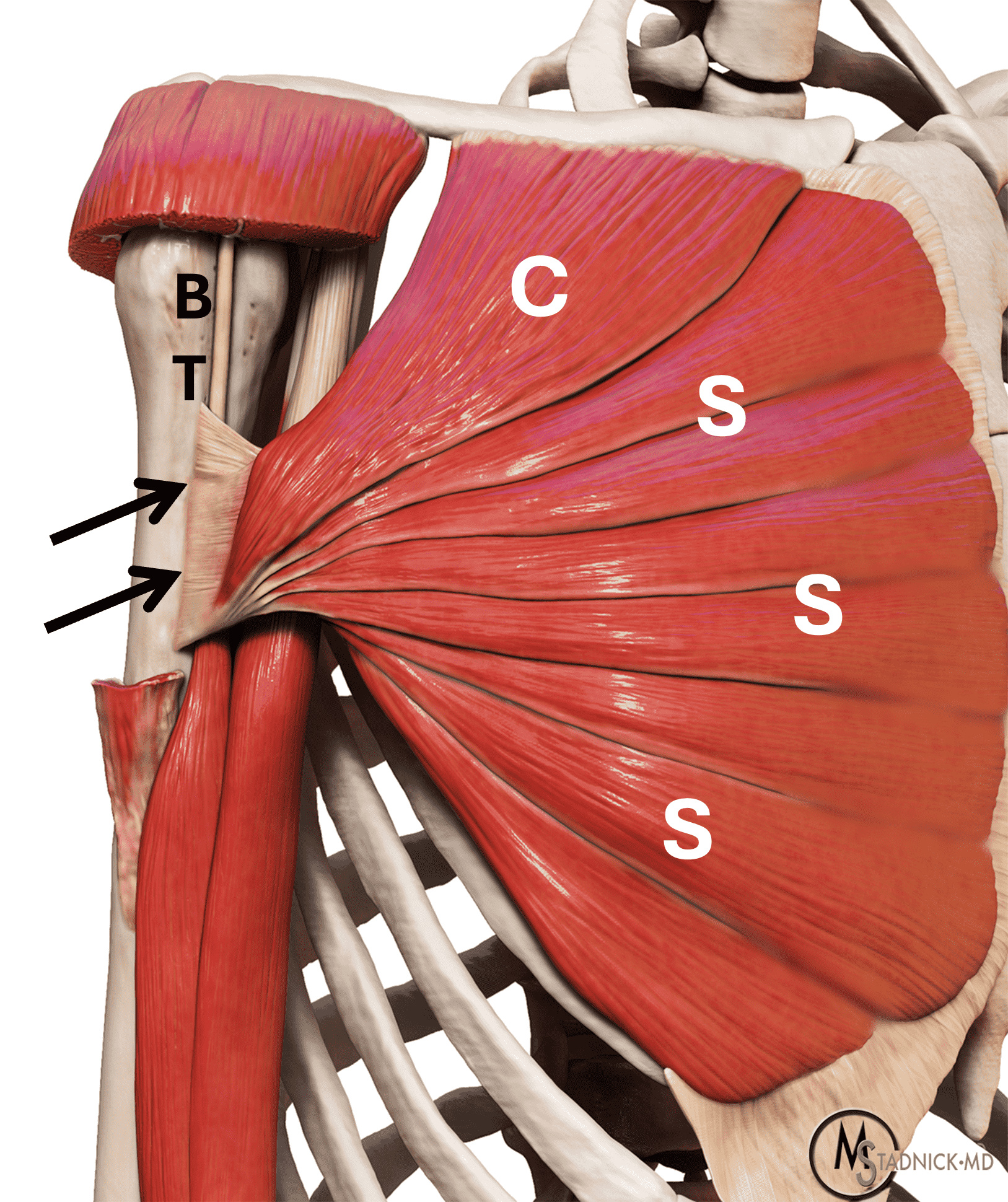
Figure 3: Pectoralis major anatomy. (3A) Photograph of an unfolded hand fan, a model for the muscle and tendon morphology. The dark brown portions are analogous to the muscle bellies, and the tan sticks represent the tendons, which overlap each other as they converge. (3B) Anatomic drawing showing the clavicular (C) and the seven sternocostal (S) muscle bellies leading to a broad, tendon composed of anterior and posterior layers that typically fuse before inserting on the humerus (arrows). The deltoid muscle has been partly cut away for exposure. BT = long head biceps tendon.
The tendons of the CH and SH course laterally and converge at a fusion point, forming a conjoint, bilaminar tendon with a U shape inferiorly (Figure 4).11 The bilaminar tendon inserts onto the humerus, specifically the lateral lip of the bicipital groove where a bony prominence can be found on the superior margin of the enthesis.12,13 Tendon fibers originating from sternal segments 5-7 form the posterior layer and insert onto the superior aspect of the humeral enthesis. The CH and upper SH segments form the anterior layer and insert onto the inferior margin of the humeral enthesis.5,14 The tendon may function as a kind of roof or retinaculum keeping the long head of biceps in place.15
Figure 4: Interactive series: Press and hold the left mouse button and drag left to view the layered anatomy of the pectoralis major muscle slips and tendon. The anterior tendon layer is derived from the clavicular and upper sternal segments, and posterior tendon layer from the inferior sternal and abdominal segments. Together they form a U-shape in cross-section.
Some controversy exists over whether the PM tendon consistently maintains a bilaminar morphology prior to the humeral insertion or displays more variation with some tendons being completely fused into one layer.5,13 A recent anatomic study reported a mean humeral footprint craniocaudal length of 80.8 mm (range, 70-90 mm), tendon thickness between 1-3 mm, and medial to lateral width of 6.1 mm.13 The mean distance between the farthest superior margin of the PM tendon footprint and the apex of the humeral head was found to be 59 mm.13 Another source of variation in anatomy between subjects is the length of the PM tendon in the medial to lateral dimension, ranging from 6 – 54 mm.12
The PM is innervated by the medial and lateral pectoral nerves, which arise from the C7 and T1 nerve roots and the lower trunk of the brachial plexus. PM contraction leads to three main effects on humeral motion: flexion, adduction, and internal rotation. Against a fixed humerus, the PM acts as a climbing muscle, pulling the thorax upward. It is also an accessory muscle of respiration when the shoulders are fixed in an elevated position.
Injury Mechanism and Classification
A typical patient is a muscular male between ages 20 and 40 who reports a pop with acute chest wall pain during bench pressing. Ecchymosis then develops in the anterior axilla and medial aspect of the upper arm. Non-athletic falling or lifting mechanisms can also injure the PM. Suspecting the injury based on physical exam alone can be challenging. The pectoralis major index test was developed to help standardize the clinical exam and improve clinical acumen. In this technique, the patient assumes a military press position with the arms in 90 degrees of abduction and external rotation, and the elbows in 90 degrees of flexion. The distance from the areola to the apex of the PM curvature at the anterior axillary line is measured and compared bilaterally. Injured muscles typically display some degree of muscle retraction and distortion, leading to a shorter line. If the length of the injured side is 90% or less of the normal PM side, then the test is positive for a PM tear.4
Injuries less than 6 weeks old are considered acute or subacute. After 6 weeks, a PM injury is considered chronic.4 Surgical classification uses a framework developed by ElMaraghy and Devereaux, based on earlier work by Tietjen.11,16 The system incorporates timing of injury, anatomic location (intramuscular, MT, intratendinous, humeral attachment, and bony avulsion), extent in thickness (i.e., one layer or two layers) and extent in width (i.e., the craniocaudal length of tendon involvement or specific number of muscle segments involved). Since the lateral to medial distance of the PM tendon is short and variable, the authors recommended collapsing injury location into 3 categories: Intramuscular (IM), myotendinous/tendinous or humeral attachment/bony avulsion (Figure 5).11 SH segments 5-7 constitute the posterior layer of the bilaminar tendon, while the CH and SH segments 1-4 form the anterior layer. Four distinct types of PM tendon tears can be described: 1. Partial thickness, incomplete width, 2. Partial thickness, complete width. 3. Full thickness, incomplete width, 4. Full thickness, complete width (Figure 6). Operative management is based on both location and tear degree. IM injuries are managed non-surgically, humeral attachment injuries are always operative, and management of MT injuries are patient specific.4,10
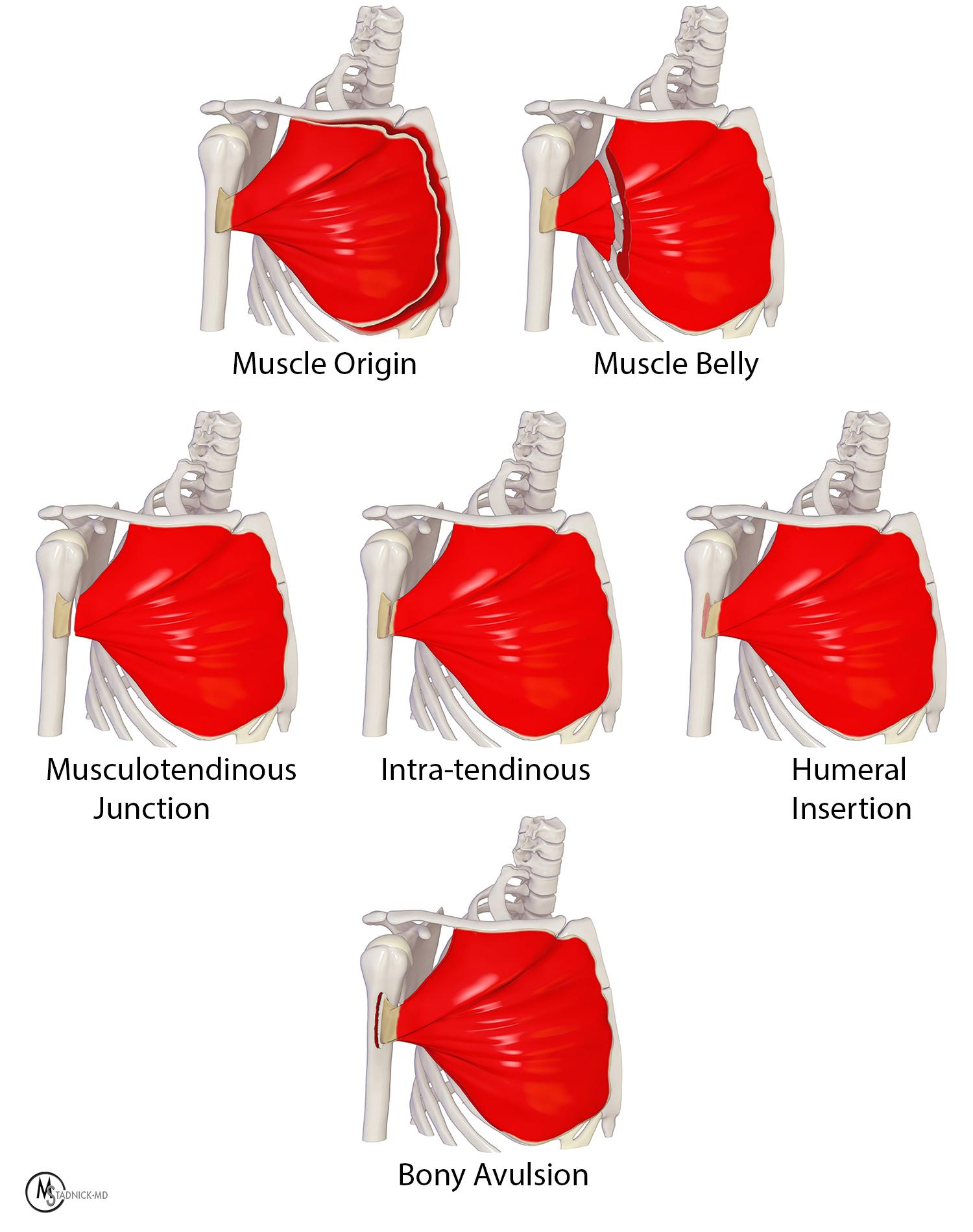
Figure 5: Illustration showing the potential anatomic locations of pectoralis muscle and tendon injuries.
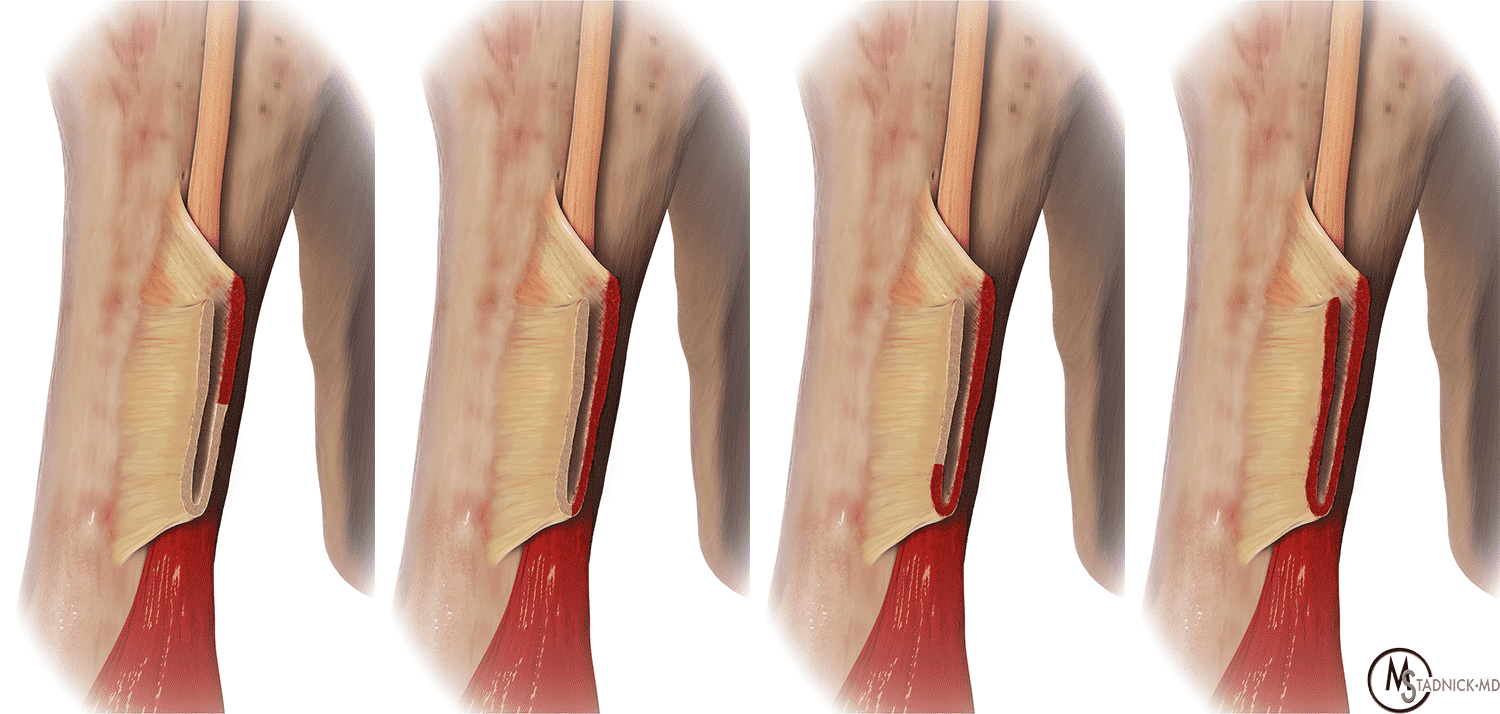
Figure 6: Tear progression and nomenclature. From left to right, pectoralis major tendon tears begin in the upper portion of the posterior layer as partial-thickness, incomplete width tears, then as force increases, progress inferiorly toward bottom of U (partial-thickness, complete width) before becoming complete tears involving both anterior and posterior layers (full-thickness, complete width).
Anatomic studies and retrospective case series in the surgical literature suggest that PM injuries in the general population most commonly involve the SH.10 In contrast, military paratrooper populations suffer bony avulsion or tendon ruptures from the humeral attachment due to a distinct mechanism where the arm gets caught in the static line, causing forcible arm abduction and external rotation.2 In the civilian, weightlifting population, a large single-surgeon case series found that PM injuries are most commonly partial tears involving the posterior layer at the MT junction or intratendinous location.3,10 Out of 104 surgical cases, 96% occurred at the MT junction or between the musculotendinous junction and humeral attachment. Partial thickness, complete width tears involving the posterior layer comprised 58% of the cases, and complete 2-layer tears comprised 42%.
An explanation for the relative abundance of MT injuries in weightlifters is provided by EMG studies that show PM muscle fiber activity is greatest at the beginning of the bench-pressing maneuver, when the elbow is flexed and the shoulder extended.10 In this position, the lower SH segments are stretched twice as much as upper SH and CH fibers due to their pennation angles and inherently shorter lengths.3,10 As repetitions and muscle fatigue increase, the ability to press the barbell upwards from the starting position decreases or stops, dubbed the “sticking point”, and is believed to represent a particularly susceptible moment for injury.9 According to ElMaraghy and Devereaux, the kinetics of PM tears follows a predictable pattern where the tears begin in the lower sternal segment posterior layer and superior humeral enthesis, progress inferiorly to the bottom of the U-shaped enthesis, then finally extend into anterior layers originating from the upper SH and CH (Figure 6).11
Imaging Modalities and MRI protocol
Imaging has an essential role in visualizing tear location and establishing surgical candidacy in both acute and chronic settings. To help characterize PM tears, various imaging modalities provide complementary information. Ultrasound offers high spatial resolution able to resolve the bilaminar tendon anatomy (Figure 7) and allows dynamic imaging and easy contralateral comparison. Radiographs are sensitive to subtle cortical avulsion fractures of the humeral enthesis. MRI allows imaging of the entire pectoralis muscle and tendons as well as the surrounding structures in the chest wall with very high contrast resolution.17 A recent large MRI-surgery correlation study established that MRI accuracy in predicting PM tear location is greater relative to prediction of tear thickness/number of layers involved.3
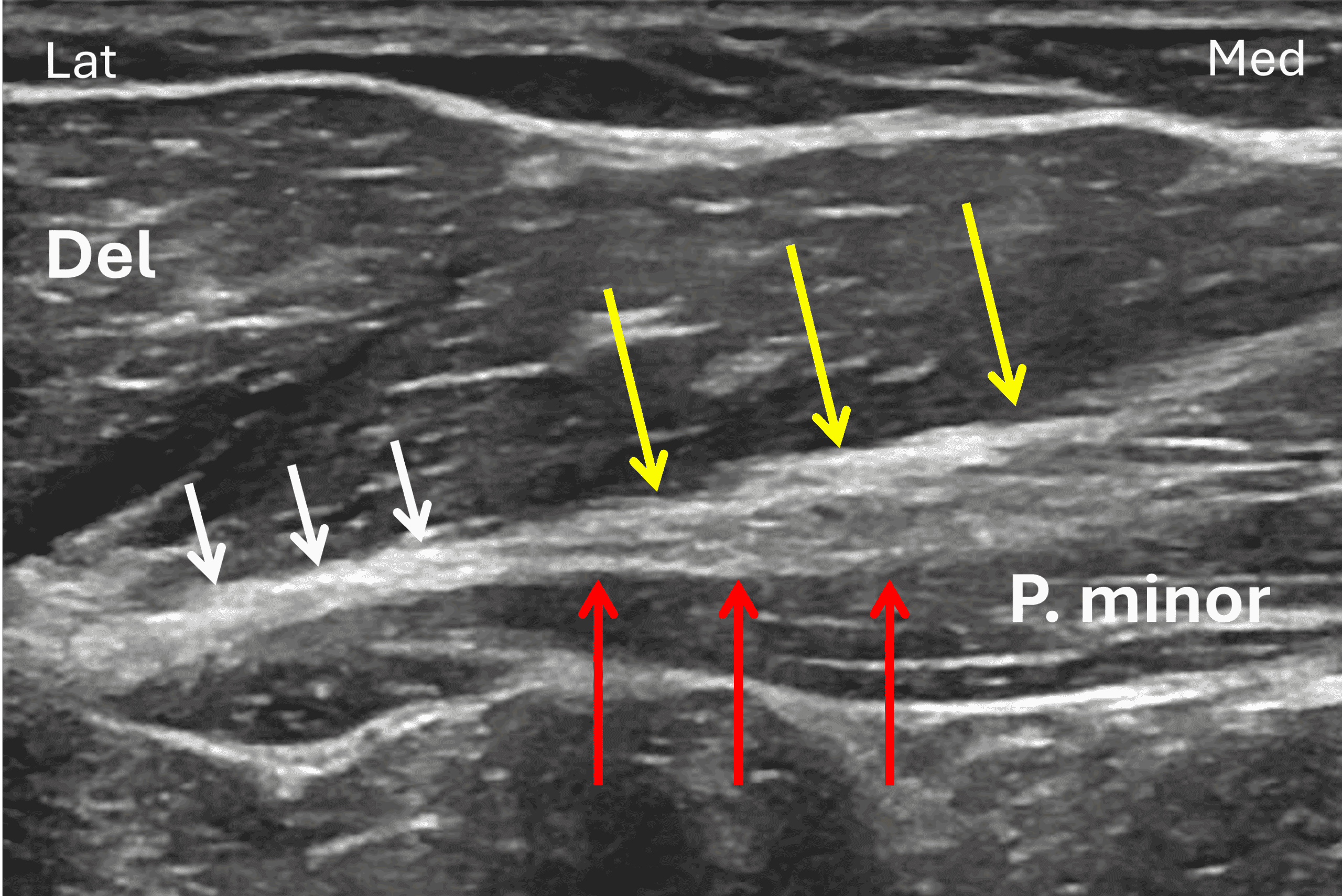
Figure 7: Transverse ultrasound of a normal pectoralis major tendon. Lat = lateral, M = medial. The clavicular head tendon (yellow arrows) contributes to the anterior tendon leaflet and is seen merging with a tendon of the sternal head (red arrows), forming a bi-layered structure (see Figure 4 and 6). In this subject, the two layers fuse (white arrows) before inserting on the humerus, located to the left of this image. P. minor = pectoralis minor muscle, Del = deltoid muscle.
As with all MRI imaging, protocols vary substantially between facilities but nearly always include a patient-specific FOV that includes the entire PM muscle from sternal origin to humeral insertion. A combination of fluid sensitive and T1-weighted sequences are acquired in three planes. The axial (transverse) plane images usually provide the most diagnostic information, while coronal and sagittal images are useful in depicting which specific muscle segments are involved (Figure 8). Some institutions angle oblique sagittal and coronal sequences guided by the anterior to posterior angulation of the PM, while others simply acquire images orthogonal to the axial plane. Large body habitus, hematomas and patient motion limit MRI study quality in many cases. Imaging the humeral attachment with the arm in the ABER (abduction and external rotation) position has been described during ultrasound assessment as a method to improve tendon stump visualization.18 ABER position in an MRI gantry may be difficult due to patient size or pain and subsequent motion.



Figure 8: Complete 2-layer pectoralis major tendon tear at humeral attachment. (8A) Axial T2-weighted image with fat suppression shows the torn tendon stump retracted to the myotendinous junction (red arrow). Edema contacting the anterior humeral cortex (yellow arrow) and anterior displacement of the long head of biceps tendon (black arrow) are secondary signs of a tendon avulsion at the humeral attachment rather than myotendinous junction injury. (8B) Coronal T2-weighted image with fat suppression demonstrates completely torn sternal and clavicular head tendon fibers (arrows). (8C) Oblique sagittal T2-weighted image shows full thickness and full width (2-layer) tear involving both sternal and clavicular heads (arrows) with retracted, irregular fibers across the full craniocaudal extent of the pectoralis major tendon complex.
If implants, patient discomfort or claustrophobia limit scan time, then small FOV axial images focused on the humeral enthesis and MT junction should be prioritized as most injuries occur at these sites.10 Although the timing of injury may be known by history, comparing T1-weighted images with fat-suppressed fluid sensitive sequences may help differentiate between acute, chronic or acute-on-chronic injuries (Figure 9). The stigmata of chronic injury such as thick and irregular tendon margins and muscle atrophy may be difficult to appreciate without at least one non-fat suppressed pulse sequence.

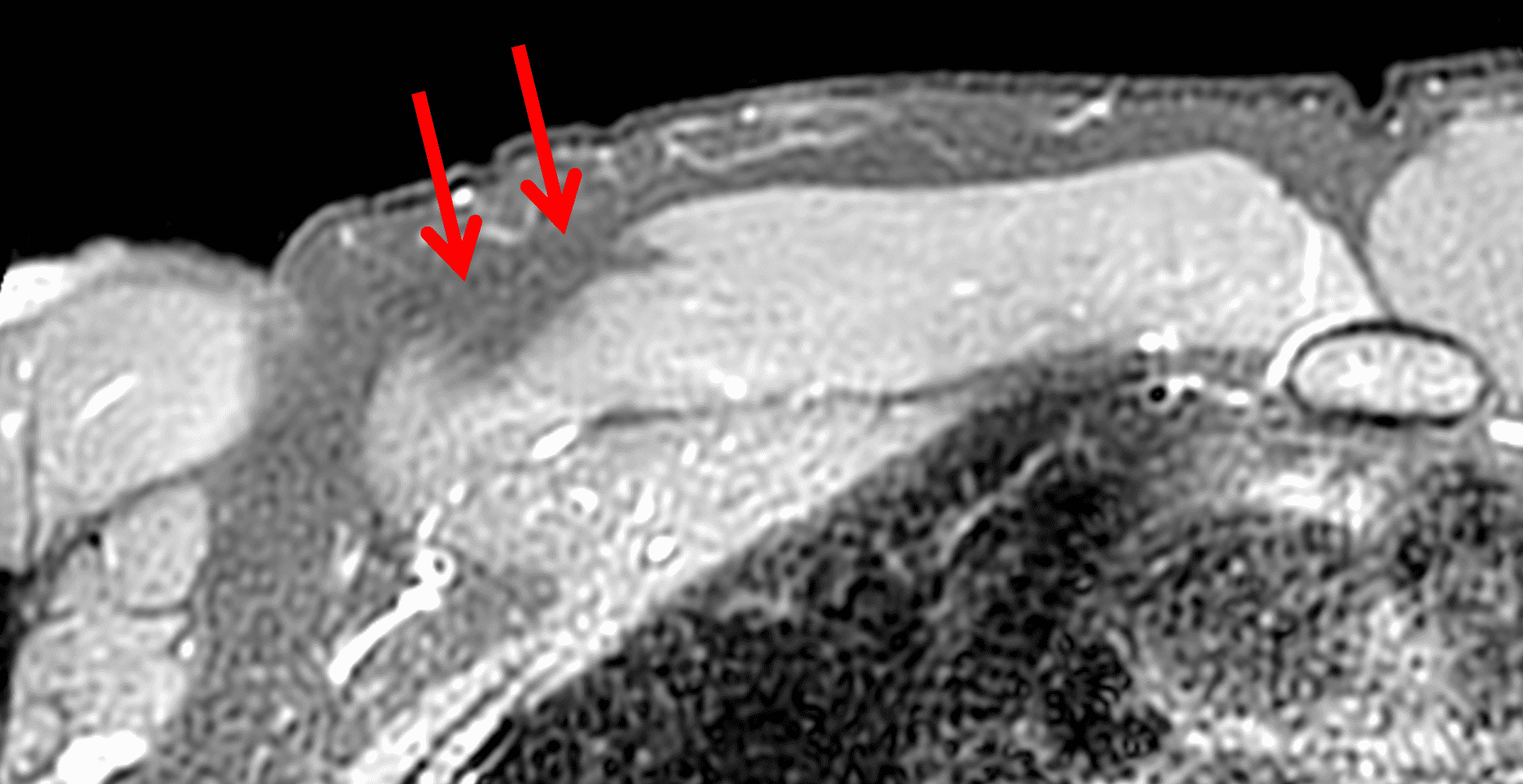
Figure 9: Chronic pectoralis major myotendinous injury. (9A) Axial T1-weighted image shows focal fatty atrophy of the sternal head muscle and mild fibrotic scarring (arrows). (9B) On the axial fat-suppressed T2-weighted image, the scar tissue is not visible and the muscle atrophy is harder to appreciate (arrows) due to the suppressed fat signal and lack of edema in the chronic injury.
MRI Signs and Accuracy
Only a handful of retrospective series have evaluated the accuracy of MRI in characterizing PM tears using operative findings as a reference standard. Some of the studies have focused on the accuracy of primary MRI signs in predicting tear thickness and location, while others have focused on the utility of secondary MRI signs distinguishing between humeral attachment from MT injuries. One consistent finding is that MRI readers are more accurate in characterizing complete tears from the humeral attachment as compared to partial tears at any location. In a recent MRI-surgery correlation series of 102 subjects, agreement between operative and MRI findings was 83.9% for complete tears and 62.5% for partial tears. Higher agreement was found with complete tears of the SH (81.4%) compared to complete tears of both SH and CH layers (46.2%). Agreement was found in 53.8% of cases with partial single-layer SH tears, and 0% of partial two-layer SH and CH tears. As a function of location, agreement was noted in 80% of complete tears at the humeral insertion, and 70% of complete tears at the MT junction. Overall, there was 83% agreement based on tear location, 78.9% on tear thickness, and 80.2% on muscle head involvement.3
Primary imaging signs of PM injury include absence of the tendon at the humeral attachment (Figure 2B), tendon laxity, direct visualization of gaps in the tendon or a retracted tendon stump (Figures 2A and 8A). Of the primary signs, Baker et al. found lack of tendon visualization was the most accurate in isolation.19 The normal PM tendon should be visible on multiple continuous axial images through the proximal humeral shaft (Figure 10).

Figure 10: Normal pectoralis major tendon. Axial T1-weighted image shows an intact low signal intensity tendon extending to the anterior humerus, without laxity of discontinuity. Compare to Figure 2B.
Secondary signs include hematoma, edema contacting the anterior humeral surface and anterior displacement of the long head of biceps tendon (LHBT) due to loss of the overlying retinacular function of the torn PM tendon (Figure 8A).15,19 In a series of 26 subjects, Godoy et al. found LHBT displacement of 4.5 mm or greater from the floor of the bicipital groove provided 86% sensitivity and 75% specificity for complete, 2-layer PM tendon tears from the humeral attachment.15 Baker et al, found edema contacting the anterior margin of the humerus helped improve radiologist’s ability to accurately distinguish tendon avulsions from MT injuries in the acute or subacute setting.19 Occasionally, if a PM injuries is unsuspected clinically, a shoulder joint MRI may be requested rather than a chest wall examination. Subtle findings suggesting a PM injury may be visible on shoulder images. The “smoke sign” was recently proposed to help identify PM injuries – especially humeral avulsions – in this scenario.20 The appearance of smoke billowing from a distant horizon is created by edema lateral (on coronal images) and anterior (on sagittal and axial images) to the short head biceps and coracobrachialis, with a relatively sharp margin (Figure 11). The sharp demarcation provided by these tendons constitutes the horizon of the smoke sign. The sign is not intended to be used as a method of distinguishing between humeral attachment and MT injuries. Of the group of 38 test subjects, the smoke sign was present in 24/24 humeral avulsions, 4/4 intratendinous injuries, 4/8 MT injuries and 0/2 intramuscular injuries.20

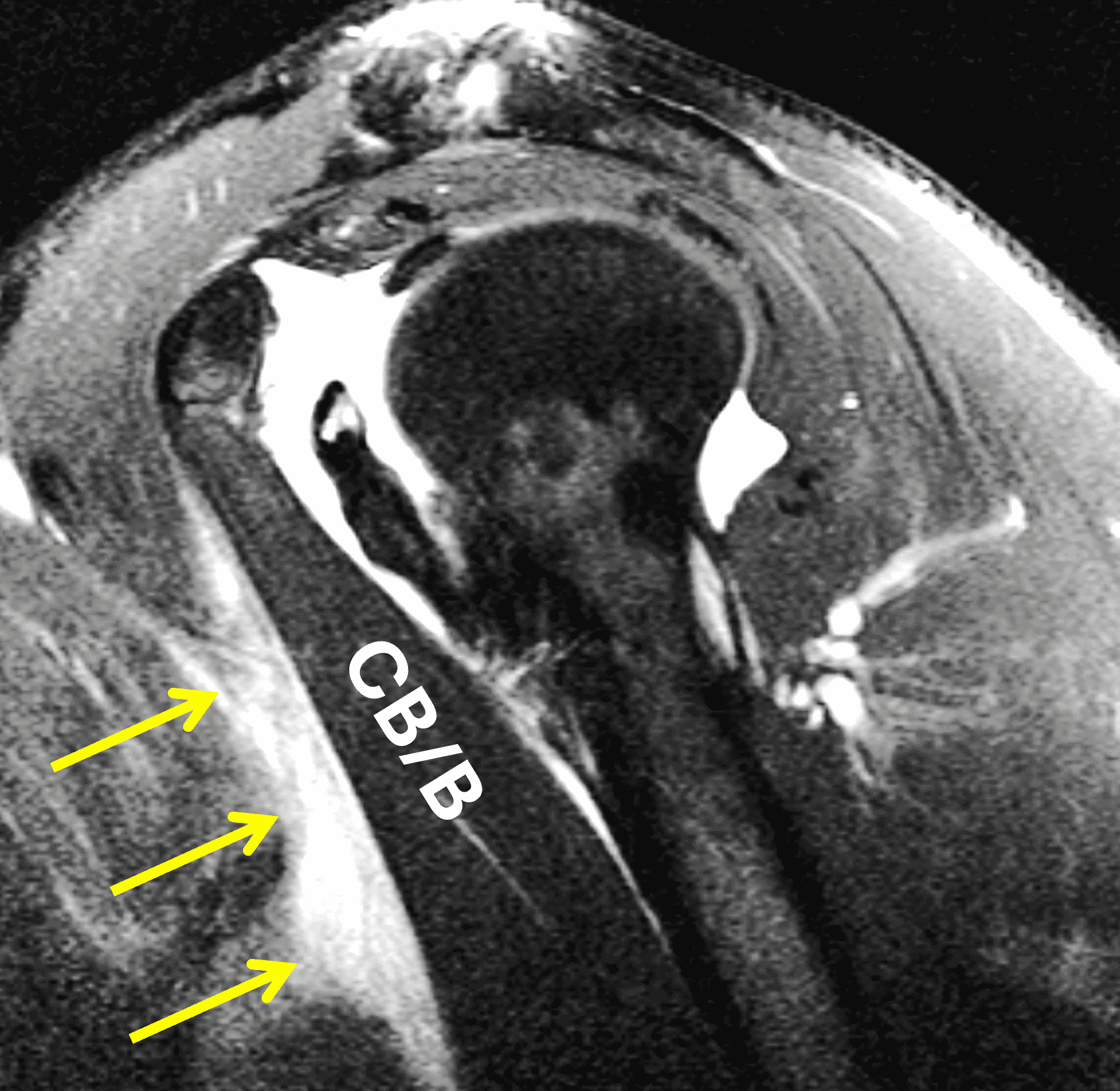
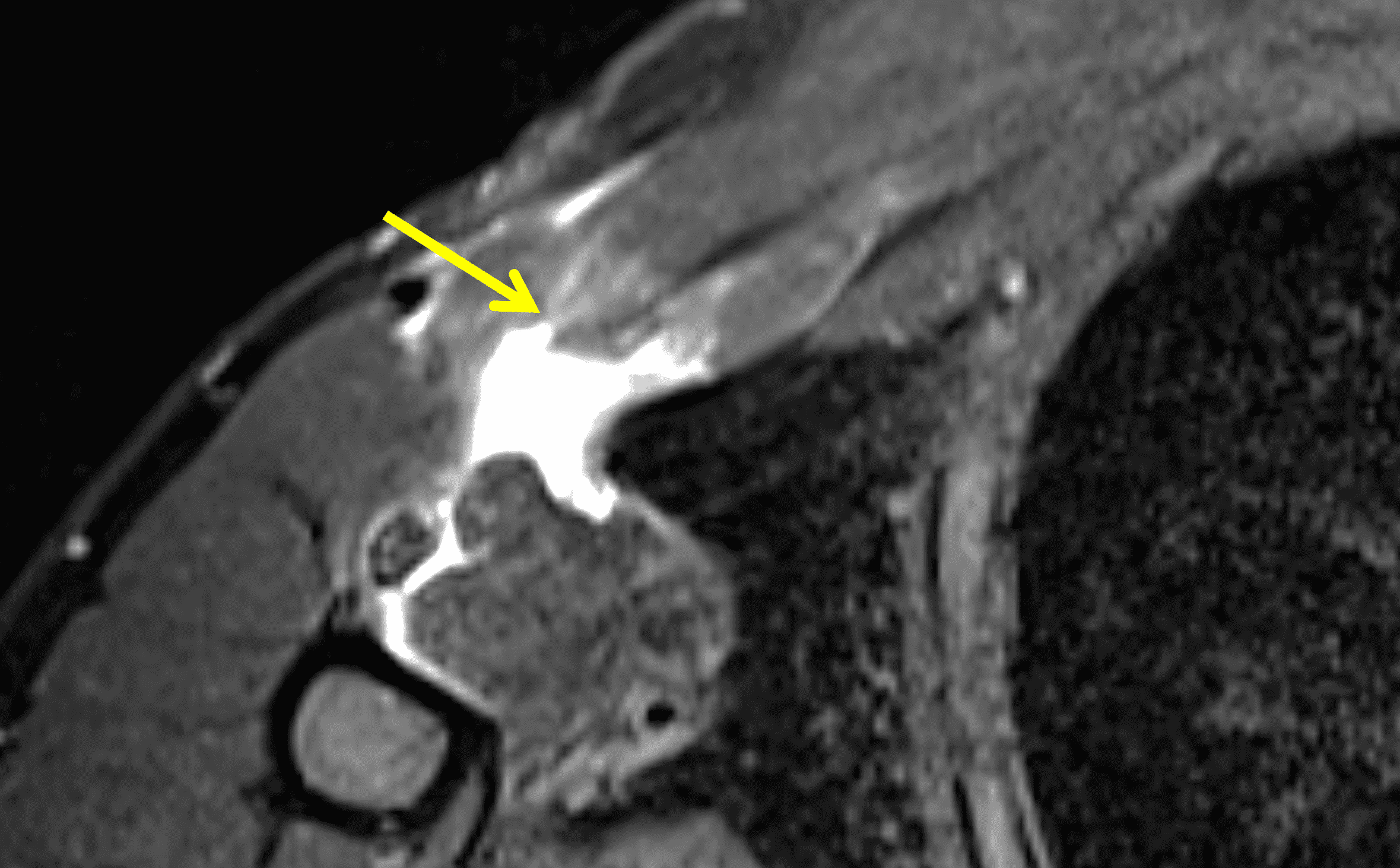
Figure 11: “Smoke sign” as a clue to a pectoralis major injury on shoulder MRI. (11A) Axial T2-weighted image from a shoulder MRI does not extend distally to include the pectoralis major tendon but shows edema along the anterior margin of the coracobrachialis muscle (arrows), the “smoke sign.” (11B) Sagittal T2-weighted image from a shoulder MRI shows a sharp posterior margin of the edema along the muscles (arrows). CB/B = coracobrachialis/short head biceps muscle bellies. (11C) Because of the findings on the shoulder images, the patient returned two days later for a dedicated chest wall MRI, with a fat-suppressed axial T2-weighted image from that study confirming a completely torn, retracted pectoralis major tendon (arrow).
In summary, MRI may not be highly accurate in determining exact degree of PM tear thickness or width but appears to be excellent in predicting tear location, and it is location more than degree of tearing that guides management decisions regarding surgical or conservative treatment. Many radiologists use complete or partial as descriptors of tear degree rather than the surgical classification using the terms thickness and width. Another potential method of describing PM tendon injuries would be to use the terms anterior layer and/or posterior layer involvement. A potential interpretation checklist would include the following steps:
- Is the injury acute or chronic based on history? If history is not available, can scar tissue be visualized on T1-weighted sequences?
- Assess the primary signs of tears by looking at insertion and fiber discontinuity. If tendon tears are not directly visible at insertion, look for tendon laxity and medial retraction into the MT junction.
- Determine if tear is complete 2-layer or partial, 1-layer by looking at extent of edema into muscle fibers on coronal and sagittal sequences and analyzing visible torn and intact tendon leaflets (Figures 12, 13, and 14).
- Determine Location: humeral avulsion, intratendinous, MT or intramuscular (Figures 8 and 13, and 14). Use secondary signs to distinguish between avulsion/intratendinous vs MT injuries.

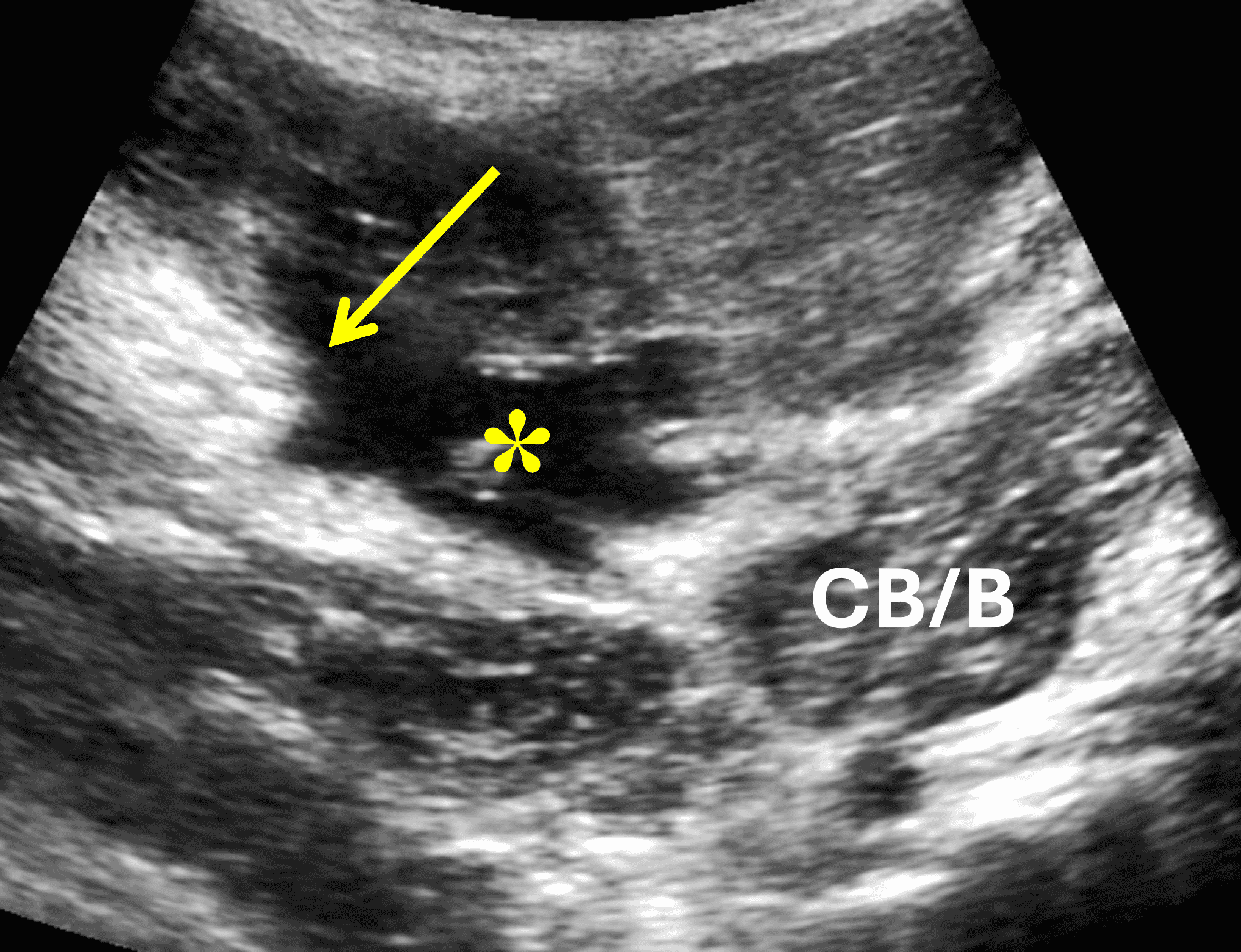

Figure 12: Partial-thickness, full-width (1-layer) tear of pectoralis major tendon at the humeral attachment. (12A) Axial T2-weighted image shows an intact tendon (anterior leaflet) inserting on the humerus (red arrows), approximately half the thickness of the normal tendon. The torn, retracted stump of the deep leaflet is visible (yellow arrow) medial to the hematoma. (12B and 12C) Transverse ultrasound images confirm the retracted torn deep tendon layer (yellow arrow) medial to the hematoma (asterisk), as well as the intact anterior tendon layer (red arrows). H = humerus, CB/B = coracobrachialis/short head biceps muscle bellies.

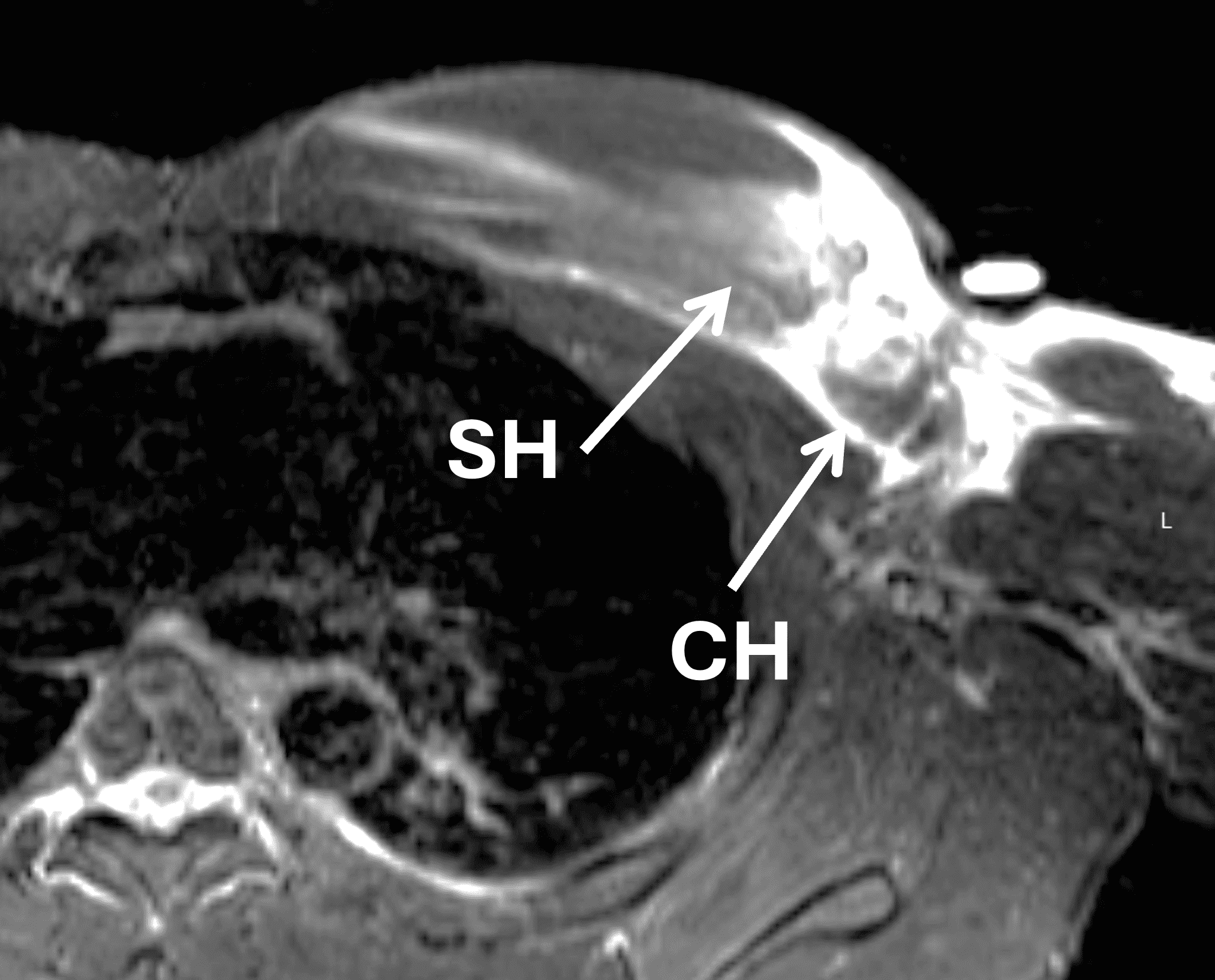

Figure 13: Complete (2-layer) pectoralis major tear at the myotendinous junction. (13A) Coronal STIR image shows complete fiber disruption at the myotendinous junction (arrows) in the medial lip of the axilla. (13B) Axial fat-suppressed T2-weighted image confirms involvement of both the sternal head (SH) and clavicular head (CH). (13C) Axial T1-weighted image shows the intact tendon insertion on the humerus (arrows).
Management
Treatment recommendations are generally informed by injury location, patient age and activity level (Figure 5). Surgical repair is encouraged in most patients with tendinous or myotendinous injuries, as it is correlated with improved patient satisfaction, cosmesis and shorter return to play. Non operative management is considered in elderly patients and muscle belly injuries. While partial tears can be repaired, the decision is generally patient specific. The location of the tear determines the surgical technique, with injuries at the humeral tendo-osseous junction repaired with transosseous sutures, suture anchors and cortical button fixation techniques. Chronic tears or injuries centered at the musculotendinous junction often require reconstruction techniques which weave various types of allografts or autografts into the injured MT junction.4
Conclusion
Recent surgical studies have shown PM injuries are very commonly located between the humeral attachment and MT junction and are frequently partial thickness tears involving the SH-derived posterior layer. MRI appears to be more accurate in predicting complete 2-layer tears at or near the humeral attachment and less accurate for injuries at the MT junction, injuries involving the CH and chronic injuries. Although MRI accuracy may be limited in these scenarios, MRI remains essential in classifying injury location and helping determine the type and clinical appropriateness of surgical intervention.
References
- Li WWL, De Jonge MC, Goslings C, Haverlag R, Ponsen KJ. Complete avulsion of the pectoralis major tendon: A case report. European Journal of Trauma and Emergency Surgery. 2007;33(5):553-556. doi:10.1007/s00068-007-6103-z. ↩
- Synovec J, Shaw KA, Hattaway J, Wilson AM, Chabak M, Parada SA. Magnetic Resonance Imaging of Pectoralis Major Injuries in an Active Duty Military Cohort: Mechanism Affects Tear Location. Orthop J Sports Med. 2020;8(6). doi:10.1177/2325967120925019. ↩
- Carlos NBT, Drain NP, Fatora GC, et al. Myotendinous junction tears of the pectoralis major are occurring more frequently and discrepancies exist between intraoperative and radiographic assessments. JSES Int. 2023;7(6):2311-2315. doi:10.1016/j.jseint.2023.06.019. ↩
- Long MK, Ward T, DiVella M, Enders T, Ruotolo C. Injuries of the Pectoralis Major: Diagnosis and Management. Orthop Rev (Pavia). 2022 Nov 30;14(4):36984. doi: 10.52965/001c.36984. ↩
- Fung L, Wong B, Ravichandiran K, Rindlisbacher T, Elmaraghy A. Three-dimensional study of pectoralis major muscle and tendon architecture†. Clinical Anatomy. 2009;22(4):500-508. ↩
- Zielinska N, Karauda P, Węgiel A, Szewczyk B, Olewnik Ł. A very rare case of a thoracobrachialis muscle. Surgical and Radiologic Anatomy. 2023;45(11):1493-1496. doi:10.1007/s00276-023-03240-6. ↩
- Shekhawat D, Kumar D, Tubbs RS. Bilateral Sternalis Muscle With the Absence of Unilateral Sternocostal Part of the Pectoralis Major and Variation of Pectoralis Minor Muscles. Cureus. 2023;15(7):e41653. doi: 10.7759/cureus.41653. ↩
- Chadwick N, Weaver JS, Shultz C, Morag Y, Patel A, Taljanovic MS. High-resolution ultrasound and MRI in the evaluation of pectoralis major injuries. J Ultrason. 2023;23(95):e202-e213. doi: 10.15557/jou.2023.0029. ↩
- van den Tillaar R, Ettema G. The “sticking period” in a maximum bench press. J Sports Sci. 2010;28(5):529-535. ↩
- Kowalczuk M, Rubinger L, Elmaraghy AW. Pectoralis Major Ruptures: Tear Patterns and Patient Demographic Characteristics. Orthop J Sports Med. 2020;8(12). doi:10.1177/2325967120969424. ↩
- ElMaraghy A, Devereaux M. A systematic review and comprehensive classification of pectoralis major tears. Journal of Elbow and Shoulder Surgery. 2012;210(3):412-422. doi:10.1016/j.jse.2011.04.035. ↩
- Bois AJ, Lo IKY. Surgical anatomy of the pectoralis major tendon insertion revisited: relationship to nearby structures and the pectoral eminence for defining the anatomic footprint. JSES Int. 2020;4(2):324-332. doi:10.1016/j.jseint.2020.02.010. ↩
- de Figueiredo EA, Terra BB, Cohen C, et al. The pectoralis major footprint: An anatomical study. Revista Brasileira de Ortopedia (English Edition). 2013;48(6):519-523. doi:10.1016/j.rboe.2013.12.009. ↩
- Guiu R, Lefort H, Mihai I, Ernouf C, Domanski L. Regarding “A systematic review and comprehensive classification of pectoralis major tears.” J Shoulder Elbow Surg. 2013;22(2). doi:10.1016/j.jse.2012.10.030. ↩
- Godoy IRB, Martinez-Salazar EL, Simeone FJ, Bredella MA, Palmer WE, Torriani M. MRI of pectoralis major tears: association between ancillary findings and tear severity. Skeletal Radiol. 2018;47(8):1127-1135. doi:10.1007/s00256-018-2893-9. ↩
- Tietjen R. Closed injuries of the pectoralis major muscle. J Trauma. 1980;20(3):262-264. ↩
- Chiavaras MM, Jacobson JA, Smith J, Dahm DL. Pectoralis major tears: Anatomy, classification, and diagnosis with ultrasound and MR imaging. Skeletal Radiol. 2014;44(2):157-164. doi:10.1007/s00256-014-1990-7. ↩
- Rehman A, Robinson P. Sonographic evaluation of injuries to the pectoralis muscles. AJR Am J Roentgenol. 2005;184(4):1205-11. doi: 10.2214/ajr.184.4.01841205. ↩
- Baker JC, Pacheco RA, Bansal D, Shah VA, Rubin DA. The diagnostic performance of MRI signs to distinguish Pectoralis major tendon avulsions from Myotendinous injuries. Skeletal Radiol. 2021;50:2395-2404. doi:10.1007/s00256-021-03794-9. ↩
- Petchprapa CN, Vaswani D, Garwood E, Samim M, Bencardino JT. The smoke sign: a secondary sign of unsuspected acute pectoralis major tendon injury on routine shoulder MRI. Skeletal Radiol. 2021;50(9):1873-1880. doi: 10.1007/s00256-021-03759-y. ↩
