Clinical History:
A 45 year old man fell through a plate glass window 6 months ago, lacerating the right wrist with subsequent diminished sensation in the right thumb, index and middle fingers. He now presents to the orthopaedist with an enlarging painful mass in the wrist at the site of injury. MRI of the wrist was obtained. Axial T1-weighted and inversion recovery (1A), sagittal T1-weighted (1B), and coronal GRE T2*-weighted and inversion recovery (1C) images are provided.
What are the findings? What is your diagnosis?

1a

1a

1a
Figure 1
Findings:
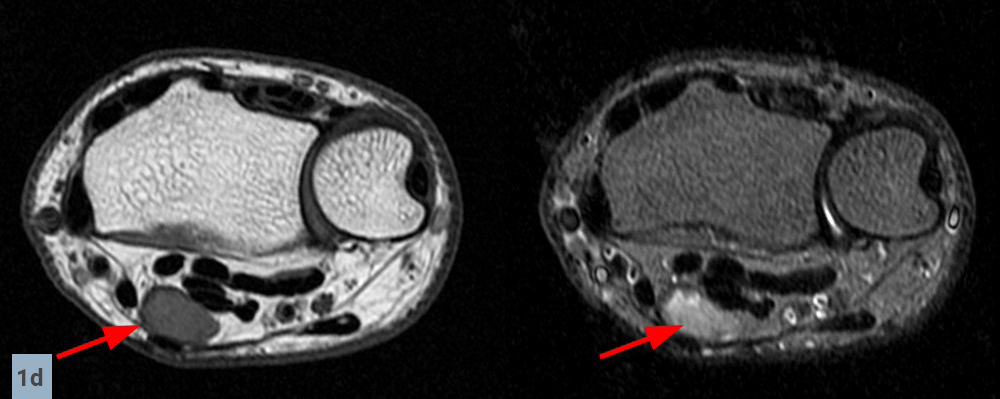
Axial images (1D) demonstrate a well-circumscribed mass (arrows) in the expected location of the median nerve, with smooth well-defined margins. Internal signal is mildly hyperintense to muscle on T1-weighted and inversion recovery sequences.

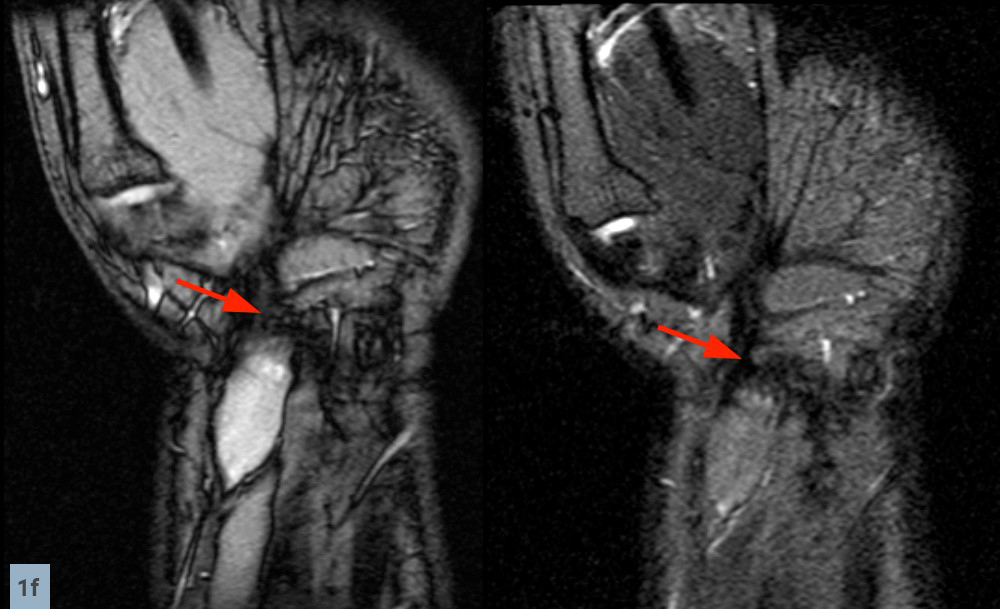
Sagittal (1E) and coronal (1F) images reveal that the mass terminates abruptly at an area of low signal fibrosis (arrows) over the proximal carpal row. The median nerve could not be identified in the area of fibrosis, and appears to terminate in the mass.
Diagnosis:
Traumatic neuroma originating from previously injured median nerve.
Anatomy and pathophysiology:
Peripheral nerves are composed of parallel unidirectional nerve axons surrounded by perineurium, a connective tissue sheath. Within the nerve, fibrous stroma divide the nerve into bundles of axons called fascicles.1
After focal traumatic injury, neural axonal tissue may attempt repair and display disordered proliferation at the site of trauma, resulting in a focal non-neoplastic area of enlargement called a traumatic neuroma, also known as stump neuroma or amputation neuroma.2 On histologic examination, these lesions demonstrate multidirectional tangled axonal tissue, Schwann cells, endoneurial and perineurial cells in a collagen matrix. Some remaining nerve fascicles may still be recognizable.1
Two types of traumatic neuromas have been described, spindle neuromas and terminal (also called lateral) neuromas. Spindle traumatic neuromas occur when the nerve trunk is injured but still intact, forming a focal fusiform area of swelling at the site of injury.3 Terminal traumatic neuromas develop from the proximal fragment at sites of avulsion or complete transection of a nerve, displaying a bulbous appearance at the end of the proximal fragment.4 Commonly reported sites include the lower extremity after amputation, the oral cavity after tooth extraction, the brachial plexus, and the radial nerve.5
Patients typically present between 1 month and 12 months after injury. Onset of symptoms has been reported as soon as 8 days, or as late as 40 years. 6 The most common presenting symptom is pain. Approximately 20% to 30% of all neuromas are painful; severity of pain ranges from mild to incapacitating.7 Physical examination may reveal a palpable mass at the site of previous trauma; percussion of the mass may elicit symptoms (Tinel’s sign).8 Temporary relief of symptoms with injection of local anesthetic supports the diagnosis of traumatic neuroma.9
MRI appearance:
On MR imaging, traumatic neuromas are intermediate signal on T1-weighted images, usually isointense or mildly hyperintense to muscle.10 They tend to be isointense to hyperintense compared to muscle on proton density- and T2-weighted images, often approaching the hyperintense signal intensity of the associated nerve. 11 Because intraneural fascicles may remain intact proximal to the injury site, traumatic neuromas often demonstrate clustered hypointense ring-like areas called the “fascicular sign” on T2-weighted images acquired perpendicular to the nerve, corresponding to nerve fascicles.1 (Case 3)

2a

2a

2a
Figure 2:
Case 2 – Tibial nerve traumatic (stump) neuroma (arrows) in a 52 year-old female, status post below knee amputation for diabetic ulcers and tibial fracture. Axial T1-weighted and fat-suppressed fast spin echo T2-weighted images (2A) demonstrate focal enlargement of the tibial nerve with well-defined margins. Internal signal approaches joint fluid intensity on the T2-weighted series, with a suggestion of internal fascicles on sagittal fat-suppressed fast spin echo T2-weighted images (2B), and coronal T1-weighted and fat-suppressed fast spin echo T2-weighted images (2C). Deformity of the proximal tibia is due to chronic healed fracture.

3a

3a

3a
Figure 3:
Case 3 – Fascicular sign in a tibial nerve stump neuroma. Patient is a 62 year-old male status post below knee amputation due to leg trauma, presenting with pain and swelling in the stump. Axial fast spin-echo inversion recovery images (3A) reveal enlargement of the tibial nerve with internal fine septations (arrows), corresponding to nerve fascicles. Note the extensive adventitial bursitis along the anterior stump (arrowheads), a likely etiology for the patient’s symptoms. Coronal (3B) and sagittal (3C) fast spin-echo inversion recovery images also visualize fascicles in the neuroma, parallel to the long axis of the nerve.
Traumatic neuromas should be contiguous with a peripheral nerve; however, they can arise from small branch nerves which are difficult to identify (Case 4), or there may be variant nerve anatomy (Case 5). Most reported cases measure between 1.0 to 3.5 cm in size.10 Terminal traumatic neuromas frequently display a “bulbous end” appearance on cross-sectional imaging.12(Cases 6, 7, 8) After intravenous contrast material, enhancement within traumatic neuromas is variable and nonspecific.9 (Case 9)

4a

4a

4a
Figure 4:
Case 4 – 32 year-old female status post below knee amputation for sarcoma. Coronal (4A) and axial (4B) fat-suppressed fast spin-echo proton density-weighted images reveal a hyperintense oblong mass in the peroneus longus muscle belly (arrows). The sagittal (4C) image demonstrates the lesion in continuity with the superficial peroneal nerve anterior to the fibula (arrowheads), consistent with a stump neuroma.

5a

5a

5a

5a
Figure 5:
Case 5 – Variant nerve anatomy with postsurgical complication. A 68 year-old male underwent carpal tunnel release but did not experience any improvement in symptoms after surgery. He returned 5 months later with an enlarging mass in the area of surgery. Coronal T1-weighted and fast spin-echo inversion recovery images (5A) reveal a bifid median nerve, a normal anatomic variant. The ulnar side bundle is normal in signal and morphology (arrowheads). The radial side bundle (small arrows) is enlarged with a terminal bulbous dilatation (large arrows), consistent with a traumatic neuroma. Axial T1-weighted and fast spin-echo inversion recovery images (5B) through the dilated region of the radial bundle demonstrate a normal appearing ulnar bundle (arrowhead) adjacent to the neuroma in the radial bundle with fascicular sign (arrow). Axial images acquired just distal to the neuroma (5C) reveal the ulnar bundle in the carpal tunnel (arrowhead), but absence of the radial bundle. Axial images distal to the site of surgery (5D) visualize both bundles. Note denervation changes in the muscles of the thenar eminence (asterisks).

6a

6a
Figure 6:
Case 6 – 63 year-old male with previous above knee amputation for infected prosthesis, stump pain for 6 months. Sagittal (6A) and coronal (6B) fat-suppressed fast spin-echo T2-weighted images demonstrate the typical “bulbous end” appearance (arrows) of a terminal traumatic neuroma (stump neuroma) of the sciatic nerve.

7a

7a
Figure 7:
Case 7 – A 25 year old female status post below knee amputation for severe trauma 8 years ago reports stump pain. Coronal T1-weighted and fast spin-echo inversion recovery images (7A) along with sagittal T1-weighted and fast spin-echo inversion recovery images (7B) demonstrate the bulbous end appearance of a stump neuroma involving a branch of the tibial nerve (arrows), outlined by fat on the T1-weighted images.

8a

8a
Figure 8:
Case 8 – 85 year old female status post amputation of the ring finger for infection 10 months ago reports swelling at the site of surgery. Coronal T1-weighted and fast spin echo inversion recovery images (8A) along with an axial fast spin echo inversion recovery image (8B) demonstrate bulbous enlargement of the terminal end of the radial side palmar proper digital nerve of the ring finger (arrows), consistent with a stump neuroma.

9a

9a
Figure 9:
Case 9 – 33 year-old female status post partial hand amputation 1 year ago for a vascular tumor. Axial T1-weighted and fat-suppressed postcontrast T1-weighted images (9A), along with coronal fast spin-echo T2-weighted and fat-suppressed postcontrast T1-weighted images (9B) reveal a diffusely enhancing mass at the terminal end of the truncated median nerve (arrows), consistent with a stump neuroma. The flexor pollicis longus tendon courses along the deep margin of the neuroma.
Clinical management:
After extremity amputation, stump pain is a common complication with over 50% prevalence in most reported series.13 Traumatic neuromas account for 10% to 25% of chronic post-amputation pain.14 Many patients report persistent symptoms despite conservative therapy.13
Conservative treatment may include acupuncture, physical therapy, and neuromodulation 15 with transcutaneous and direct nerve stimulation. Systemic medications such as opioids, antidepressants, and anticonvulsants may also be utilized.13 Minimally invasive treatment with direct injection of corticosteroid medication16, 17 or sclerosing agents such as phenol 18,19,20 into traumatic neuromas has been reported with improvement of symptoms. RF ablation 21, coblation22, cryoablation23, and extracorporeal shock wave therapy24 have also been utilized.
Surgical treatment of symptomatic stump neuromas is generally reserved for refractory cases not responding to conservative treatment. Excision of the neuroma and repair of the nerve with direct anastomosis, graft, or conduit is preferred if possible.25 Traction neurectomy has historically been performed by many surgeons as the most straightforward and least invasive surgical technique in amputees; however, this has been recently reported to have a high failure rate of 42%.26 Resection of the neuroma and coverage with a vascularized flap7, centrocentral nerve coaptation 27,28, implantation into muscle 29,30 implantation into a vein 31,32,33, targeted nerve reimplantation34, and transposition into a location which is protected from mechanical stimulation have been advocated in the recent surgical literature.25,26
Conclusion:
Traumatic neuromas are a well-known complication of injury to peripheral nerves. A painful mass developing at a site of previous trauma or amputation should prompt further workup. Definitive diagnosis of traumatic neuroma can often be made by MRI. Post-amputation patients may have multiple etiologies for pain, such as infection or adventitial bursitis, and such abnormalities are also well characterized with MRI.
References
- Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple HT. From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. Radiographics. 1999 Sep-Oct;19(5):1253-80. ↩
- Donnal JF, Blinder RA, Coblentz CL, Moylan JA, Fitzpatrick KP. MR imaging of stump neuroma. J Comput Assist Tomogr. 1990 Jul-Aug;14(4):656-7. ↩
- Provost N, Bonaldi VM, Sarazin L, Cho KH, Chhem RK. Amputation stump neuroma: ultrasound features. J Clin Ultrasound. 1997 Feb;25(2):85-9. ↩
- Boutin RD, Pathria MN, Resnick D. Disorders in the stumps of amputee patients: MR imaging. AJR Am J Roentgenol. 1998 Aug;171(2):497-501. ↩
- Duzcu S, Ilaslan H, Joyce MJ, Sundaram M. Stump Neuroma. orthopaedics. 2015 Dec;38(12):720, 769-70. ↩
- Kitcat M, Hunter JE, Malata CM. Sciatic neuroma presenting forty years after above-knee amputation. Open Orthop J. 2009 Dec 30;3:125-7. ↩
- Krishnan KG, Pinzer T, Schackert G. Coverage of painful peripheral nerve neuromas with vascularized soft tissue: method and results. Neurosurgery. 2005 Apr;56(2 Suppl):369-78; discussion 369-78. ↩
- Watson J, Gonzalez M, Romero A, Kerns J. Neuromas of the hand and upper extremity. J Hand Surg Am. 2010 Mar;35(3):499-510. ↩
- Henrot P, Stines J, Walter F, Martinet N, Paysant J, Blum A. Imaging of the painful lower limb stump. Radiographics. 2000 Oct;20 Spec No:S219-35. ↩
- Singson RD, Feldman F, Staron R, Fechtner D, Gonzalez E, Stein J. MRI of postamputation neuromas. Skeletal Radiol. 1990;19(4):259-62. ↩
- Beggs I. Pictorial review: imaging of peripheral nerve tumours. Clin Radiol. 1997 Jan;52(1):8-17. (Case 2) ↩
- Abreu E, Aubert S, Wavreille G, Gheno R, Canella C, Cotten A. Peripheral tumor and tumor-like neurogenic lesions. Eur J Radiol. 2013 Jan;82(1):38-50. ↩
- Hsu E, Cohen SP. Postamputation pain: epidemiology, mechanisms, and treatment. J Pain Res. 2013;6:121-36. ↩
- Ducic I, Mesbahi AN, Attinger CE, Graw K. The role of peripheral nerve surgery in the treatment of chronic pain associated with amputation stumps. Plast Reconstr Surg. 2008 Mar;121(3):908-14; discussion 915-7. ↩
- Soin A, Fang ZP, Velasco J. Peripheral Neuromodulation to Treat Postamputation Pain. Prog Neurol Surg. 2015;29:158-67. ↩
- Chen PJ, Liang HW, Chang KV, Wang TG. Ultrasound-guided injection of steroid in multiple postamputation neuromas. J Clin Ultrasound. 2013 Feb;41(2):122-4. ↩
- Kesikburun S, Yaşar E, Dede I, Göktepe S, Tan AK. Ultrasound-guided steroid injection in the treatment of stump neuroma: pilot study. J Back Musculoskelet Rehabil. 2014;27(3):275-9. ↩
- Lim KB, Kim YS, Kim JA. Sonographically guided alcohol injection in painful stump neuroma. Ann Rehabil Med. 2012 Jun;36(3):404-8. ↩
- Gruber H, Kovacs P, Peer S, Frischhut B, Bodner G. Sonographically guided phenol injection in painful stump neuroma. AJR Am J Roentgenol. 2004 Apr;182(4):952-4. ↩
- Gruber H, Glodny B, Kopf H, Bendix N, Galiano K, Strasak A, Peer S. Practical experience with sonographically guided phenol instillation of stump neuroma: predictors of effects, success, and outcome. AJR Am J Roentgenol. 2008 May;190(5):1263-9. ↩
- Restrepo-Garces CE, Marinov A, McHardy P, Faclier G, Avila A. Pulsed radiofrequency under ultrasound guidance for persistent stump-neuroma pain. Pain Pract. 2011 Jan-Feb;11(1):98-102. ↩
- Zeng Y, Wang X, Guo Y, He L, Ni J. Coblation of Femoral and Sciatic Nerve for Stump Pain and Phantom Limb Pain: A Case Report. Pain Pract. 2016 Feb;16(2):E35-41. ↩
- Cazzato RL, Garnon J, Ramamurthy N, Tsoumakidou G, Caudrelier J, Thenint MA, Rao P, Koch G, Gangi A. Percutaneous MR-Guided Cryoablation of Morton’s Neuroma: Rationale and Technical Details After the First 20 Patients. Cardiovasc Intervent Radiol. 2016 May 17. ↩
- Jung YJ, Park WY, Jeon JH, Mun JH, Cho YS, Jun AY, Jang KU, Seo CH. Outcomes of ultrasound-guided extracorporeal shock wave therapy for painful stump neuroma. Ann Rehabil Med. 2014 Aug;38(4):523-33. ↩
- Thomsen L, Bellemere P, Loubersac T, Gaisne E, Poirier P, Chaise F. Treatment by collagen conduit of painful post-traumatic neuromas of the sensitive digital nerve: a retrospective study of 10 cases. Chir Main. 2010 Sep;29(4):255-62. ↩
- Pet MA, Ko JH, Friedly JL, Smith DG. Traction Neurectomy for Treatment of Painful Residual Limb Neuroma in Lower Extremity Amputees. J Orthop Trauma. 2015 Sep;29(9):e321-5. ↩
- Shapira Y, Midha R. Centrocentral Short Circuiting for Management of Stump Neuroma Pain in Amputees. World Neurosurg. 2016 Feb;86:59-60. ↩
- Barberá J, Albert-Pampló R. Centrocentral anastomosis of the proximal nerve stump in the treatment of painful amputation neuromas of major nerves. J Neurosurg. 1993 Sep;79(3):331-4. ↩
- Rungprai C, Cychosz CC, Phruetthiphat O, Femino JE, Amendola A, Phisitkul P. Simple Neurectomy Versus Neurectomy With Intramuscular Implantation for Interdigital Neuroma: A Comparative Study. Foot Ankle Int. 2015 Dec;36(12):1412-24. ↩
- Otfinowski J, Pawelec A, Kałuza J. Implantation of peripheral neural stump into muscle and its effect on the development of posttraumatic neuroma. Pol J Pathol. 1994;45(3):195-202. ↩
- Balcin H, Erba P, Wettstein R, Schaefer DJ, Pierer G, Kalbermatten DF. A comparative study of two methods of surgical treatment for painful neuroma. J Bone Joint Surg Br. 2009 Jun;91(6):803-8. ↩
- Koch H, Haas F, Hubmer M, Rappl T, Scharnagl E. Treatment of painful neuroma by resection and nerve stump transplantation into a vein. Ann Plast Surg. 2003 Jul;51(1):45-50. ↩
- Kakinoki R, Ikeguchi R, Matsumoto T, Shimizu M, Nakamura T. Treatment of painful peripheral neuromas by vein implantation. Int Orthop. 2003;27(1):60-4. ↩
- Pet MA, Ko JH, Friedly JL, Mourad PD, Smith DG. Does targeted nerve implantation reduce neuroma pain in amputees? Clin Orthop Relat Res. 2014 Oct;472(10):2991-3001. ↩