Clinical History
Case 1:
13 year old male track and field athlete with constant back pain, increased with running.(1a,1b) Sagittal STIR image right and left of midline and (1c) axial T2 weighted images are provided. What are the findings? What is your diagnosis?

1a

1b

1c
Figure 1:
.(1a,1b) Sagittal STIR image right and left of midline and (1c) axial T2 weighted images
Case 2:
15 year old male basketball player with low back pain for two months; the patient remembers no specific injury.(2a,2b) Sagittal STIR images right and left of midline and a (2c) T1-weighted sagittal image right of midline are provided. What are the findings? What is your diagnosis?

2a

2b

2c
Figure 2:
(2a,2b) Sagittal STIR images right and left of midline and a (2c) T1-weighted sagittal image right of midline
Findings
Case 1:

3a

3b

3c
Figure 3:
All images demonstrate increased signal intensity in the pedicles and pars interarticularis of L5 bilaterally, consistent with marrow edema. Linear areas of low signal intensity within both L5 pedicles (arrows) begin at the medial and superior cortical borders but do not completely traverse the body of the pedicles. Lumbar alignment is normal.
Case 2:

4a

4b

4c
Figure 4:
(4a,4b) Sagittal STIR images show increased signal intensity within the pedicles and pars interarticularis of L3 (arrows), consistent with marrow edema. (4c) The sagittal T1-weighed image right of midline demonstrates a defect of the pars interarticularis of L3 (arrow), with disruption of cortical margins (note normal cortical margins of the pars at L4 in comparison). A similar appearance was present on the left (not shown). Low signal intensity is noted within visualized portions of the facets and pars, consistent with marrow edema. Lumbar alignment is normal.
Diagnosis
Case 1: Acute incomplete fractures of the pedicles of L5 with bilateral pars interarticularis stress reactions.
Case 2: Acute bilateral spondylolysis of L3 with bilateral pedicle stress reactions.
Introduction
Back pain is a common clinical complaint among adolescent athletes; it is estimated that approximately 30% of athletes ages 11-17 will experience lower back pain at some time during their participation in sports.1 Injuries of the neural arch in the lumbar spine are a common etiology of back pain in the young athlete, and can be missed in their earliest stages on routine imaging studies. The advent of MR has allowed more sensitive imaging that enables early diagnosis of these injuries, with significant implications in terms of clinical management and outcome.
Anatomy and pathophysiology
The posterior neural arch of the lumbar spine is composed of the superior and inferior articulating facets, the pars interarticularis, the laminae, and the pedicles. Several studies have identified the pars interarticularis, which connects the superior and inferior articulating facets, as the part of the neural arch that is most susceptible to stress injuries.2,3 Although the pedicle is the second most likely point of weakness in the neural arch, the shorter movement arm and greater intrinsic strength of the pedicle make it more resistant to cyclic shear forces and thus a less common site of isolated injury.2,4,5

5a
Figure 5:
3-dimensional views of a lumbar vertebral body viewed from the side (top) and from above (bottom) demonstrate key normal anatomical features. Illustration courtesy of Michael E. Stadnick, M.D.
Stress injuries of the neural arch are caused by repetitive spinal motion, particularly repeated lumbar flexion, extension, and rotation. Athletes involved in sports that involve these types of motion, such as football, gymnastics, wrestling, diving, soccer, and volleyball, have a high incidence of fracture or defect of the pars interarticularis (or spondylolysis).6 Spondylolysis is particularly common in the adolescent presenting for evaluation of back pain, with a prevalence reported to be as high as 47% in this cohort as opposed to only 5% of adults with similar clinical presentations.8,9
Pedicle stress injuries are most commonly seen in association with unilateral spondylolysis, most likely due to altered motion dynamics.7 However, isolated stress injuries of the pedicles without associated spondylolysis have been reported in young athletes and ballet dancers.5,15,16
Acute neural arch injuries are rare in patients over the age of 30. The increased incidence of neural arch injuries in adolescents as opposed to adults is believed to be due to a variety of factors, including increased involvement of younger people in rigorous sporting activities, increased elasticity of the intervertebral disc leading to greater transmission of shear force, and incomplete ossification of the neural arch. Associations with spina bifida occulta have been reported, as well as an increased likelihood of injury during the preadolescent growth spurt.2,8,10,11
Imaging technique
Prior to the advent of MR, CT and SPECT imaging were considered the gold standard for diagnosis of acute injuries of the neural arch. However, although SPECT is highly sensitive for detection of reactive marrow changes, it is not specific in distinguishing between acute stress reaction and complete or incomplete fracture, and is insensitive for detection of chronic non-union. CT is excellent for determining the presence or absence of fracture, as its high anatomic resolution enables accurate assessment of cortical margins, but is not sensitive for detection of stress reaction due to its inability to demonstrate cortical edema.13,17
MR has emerged as an excellent front-line test for the evaluation of back pain in adolescent athletes. Sequences that are highly sensitive for visualization of cortical edema have enabled early detection of stress injuries or incomplete fractures of the neural arch. The lack of ionizing radiation is desirable for young patients. In addition, MR can simultaneously evaluate other possible causes of back pain, including disc herniations and apophyseal injuries.12,13
In the adolescent presenting for imaging evaluation of back pain, MR sequences should be optimized for detection of marrow edema in the pars interarticularis and pedicles. In addition to routine T1 and T2 axial and sagittal images, sagittal short-inversion recovery time (STIR) and/or sagittal fat-saturated T2-weighted sequences should be performed.12 As the majority of neural arch injuries occur at the L5 level, followed by the L4 level17, contiguous T2-weighted axial images should be obtained from the L4 level through the sacrum, as well as through any other areas of interest identified on sagittal STIR or fat-saturated sequences.
Imaging findings and pitfalls
Increased signal intensity on T2-weighted, STIR and/or fat saturated T2-weighted images in the pars interarticularis and/or pedicles is consistent with marrow edema and, in the presence of intact cortical margins, indicates a neural arch stress injury or incomplete fracture. In general, lesions should be confirmed as isointense or hypointense on T1-weighted sequences, as reactive marrow changes due to previous injury or degenerative disease can mimic marrow edema on T2-weighted sequences18,19; this imaging pitfall again highlights the importance of the STIR and/or fat-saturated sequence in the evaluation of back pain. Fatty marrow within the pedicles can also mimic edema on routine T2-weighted sagittal images(6a,6b), though this pitfall should be avoidable as the region does not remain bright on fat-suppressed technique and fat will appear hyperintense on corresponding T1-weighted images.

6a

6b
Figure 6:
Sagittal T2- and T1-weighted images show hyperintensity within the pedicle of L4 on both sequences (arrows), consistent with fatty marrow replacement. This appearance can mimic a stress reaction on routine T2-weighted sequences alone and highlights the need for STIR and/or fat-saturated T2-weighted sequences to confirm the presence of true marrow edema.
Hollenberg et al have proposed a grading system for stress injuries of the pars interarticularis based on the MR appearance14:
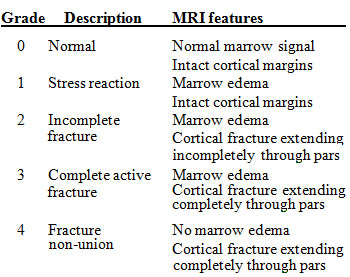
Several studies have found MR to be highly sensitive in confirmation and grading of grade 3 and 4 lesions, and in confirmation of a normal pars interarticularis (grade 0).12,13 When compared to SPECT, MR is equally sensitive and more specific in detecting stress injuries and incomplete fractures; in a study by Campbell et al, 98% of patients with pars injuries had an associated MR abnormality.13 Because of limitations in evaluating the cortical margins of the pars, MR is less accurate when compared with CT/SPECT in combination in distinguishing between stress injuries (grade 1) and incomplete fractures (grade 2). However, in terms of determining treatment and predicting outcome, the most important distinction that should be made by imaging is between a stress reaction or incomplete fracture (grade 1 or 2 injury) versus a complete fracture (grade 3 injury), and this distinction can be made using MR alone. In cases where treatment decisions would be altered by the presence of an incomplete fracture, limited non-contrast CT can be performed.12
Treatment and implications of early diagnosis

7a
Figure 7:
Sagittal fat-saturated T2-weighted (left) and routine T2-weighted images(middle) demonstrate hyperintensity within the pedicle of L5 with corresponding hypointensity on T1-weighted images (right), consistent with marrow edema (arrows). Cortical margins are intact. The appearance is consistent with an acute stress reaction.

8a
Figure 8:
Repeat images 4 months after conservative treatment show resolution of hyperintensity within the pedicle on fat-saturated T2-weighted images (arrow, first image), consistent with healed stress injury. Note the small area of hyperintensity within the inferior margin of the pedicle on routine T2-weighted and T1-weighted images (arrows, second and third images), indicating development of a small area of fatty marrow replacement. This is a common finding following stress injury and should not be mistaken for true marrow edema.
Conservative treatment is the standard for stress injuries or incomplete fractures of the neural arch. Pain reduction and cessation of sports for 4-6 weeks along with modification of daily activities is effective in the majority of cases. In patients with lack of symptomatic improvement or in the case of a complete active fracture, bracing may be indicated.
Continued, unlimited activity can cause progression of stress injuries or incomplete fractures to complete fractures and chronic non-union, significantly increasing the likelihood of surgery and leading to long-term complications such as spondylolisthesis, chronic back pain, degenerative disease, or additional stress injuries due to altered motion dynamics. For this reason, early detection and treatment of acute neural arch injuries is critical.11,20,21
As the primary goal of treatment is pain relief and return to normal activities, reimaging of neural arch injuries is not routinely indicated. However, there is a strong correlation between normalization of imaging findings and cessation of symptoms. Persistent marrow edema on MRI may reflect non-compliance, but in some cases, continuing stress response despite adequate treatment may be an indicator of increased risk for re-injury.12
Conclusion
Acute injuries of the lumbar neural arch are a common cause of back pain in the adolescent athlete. MR is an excellent first-line test for the evaluation of neural arch injuries due to its high sensitivity for the detection of cortical edema, its lack of ionizing radiation, and its ability to simultaneously evaluate for other causes of back pain. Early diagnosis and treatment of neural arch injuries leads to excellent outcomes and can obviate the need for surgery and/or eliminate long-term complications. As MR is limited in distinguishing between stress reactions and incomplete fractures, non-contrast CT can be performed in cases where treatment would be altered. However, in most cases, the information provided by MR is adequate for diagnosis and treatment without further testing.
References and recommended reading
1 Olsen TL, Anderson RL, Dearwater SR, Kriska AM, Cauley JA, Aaron DJ, et al. The epidemiology of low back pain in an adolescent population. Am J Public Health, Apr 1992; 82(4):606-608.
2 Cyron BM, Hutton WC. The fatigue strength of the lumbar neural arch in spondylolysis. J Bone Joint Surg Br, 1978; 60:234-238.
3 Dietrich M, Kurowski P. The importance of mechanical factors in the etiology of spondylolysis. A model analysis of loads and stresses in human lumbar spine. Spine, Jul – Aug 1985; 10(6): 532-542.
4 Robertson PA, Grobler LJ. Stress fracture of the pedicle: a late complication of posterolateral lumbar fusion. Spine, 1993; 18: 930-932.
5 Amari R, Sakai T, Katoh S, Sairyo K, Higashino K, Tachibana K, Yasui N. Fresh stress fractures of lumbar pedicles in an adolescent male ballet dancer: Case report and literature review. Arch Orthop Trauma Surg, 2009; 129:397-401.
6 Garry JP, McShane J. Lumbar spondylolysis in adolescent athletes. J Fam Pract, Aug 1998; 47(2): 145-149.
7 Vialle R, Mary P, de Carvalho A, Ducou le Pointe H, Damsin JP, Filipe G. Acute L5 pedicle fracture and contralateral spondylolysis in a 12 year old boy: a case report. Eur Spine J, 2007;16(Suppl 3):S316-S317.
8 Malanga, GA, Tung, DL, Kim, N, Perez, C. Pars Interarticularis Injury. emedicine.medscape.com, Dec 2009.
9 Micheli LJ, Wood R. Back pain in young athletes. Significant differences from adults in causes and patterns. Arch Pediatr Adolesc Med, Jan 1995;149(1): 15-18.
10 Roche MA, Rowe GG. The incidence of separate neural arch and coincident bone variations: A survey of 4200 skeletons. Anat Rec, 1951;109-233-252.
11 Smith JA, Hu SS. Management of spondylolysis and spondylolisthesis in the pediatric and adolescent population. Orthop Clin North Am, Jul 1999;30(3): 487-499.
12 Dunn A, Campbell RSD, Mayor P, Rees D. Radiological findings and healing patterns of incomplete stress fractures of the pars interarticularis. Skeletal Radiol, 2008;37: 443-450.
13 Campbell RSD, Grainger AJ, Hide IG, Papastefanou S, Greenough C. Juvenile spondylolysis: comparative imaging of CT, SPECT and MRI. Skeletal Radiol, 2005;34(2):63-73.
14 Hollenberg GM, Beattie PF, Meyers SP, Weinberg EP, Adams MJ. Stress reactions of the lumbar pars interarticularis: the development of a new MRI classification system. Spine, 2002;27(2): 181-186.
15 Ireland ML, Micheli LJ. Bilateral stress fractures of the lumbar pedicles in a ballet dancer. A case report. J Bone Joint Surg Am, 1987;69:140-142.
16 Parvateneti HK, Nicholas SJ, McCance SE. Bilateral pedicle stress fractures in a female athlete: case report and review of the literature. Spine, Jan 2004;29(2):E19-21.
17 Pennell RG, Maurer AH, Bonakdarpour A. Stress Injuries of the Pars Interarticularis: Radiologic Classification and Indications for Scintigraphy. AJR Am J Roentgenol, 1985;145:763-742.
18 Ulmer JL, Elster AD, Mathews VP, Allen AM. Lumbar spondylolysis: reactive marrow changes seen in adjacent pedicles on MR images. AJR Am J Roentgenol, 1995;164(2):429-433.
19 Morrison JL, Kaplan PA, Dussault RG, Anderson MW. Pedicle marrow signal intensity changes in the lumbar spine: a manifestation of facet degenerative joint disease. Skeletal Radiol, 2000;29:703-707.
20 Seitsalo S, Osterman K, Hyvarinen H, et al. Progression of spondylolisthesis in children and adolescents: A long term follow up of 272 patients. Spine, Apr. 1991;16(4):417-421.
21 Herman MJ, Pizzutillo PD, Cavalier R. Spondylolysis and spondylolisthesis in the child and adolescent athlete. Orthop Clin N Am, 2003;34:461-467.